
Comparison of Glucose Lowering Efficacy of Human GLP-1 Agonist in Taiwan Type 2 Diabetes Patients after Switching from DPP-4 Inhibitor Use or Non-Use

Abstract
:1. Introduction
2. Methods
2.1. Data Source
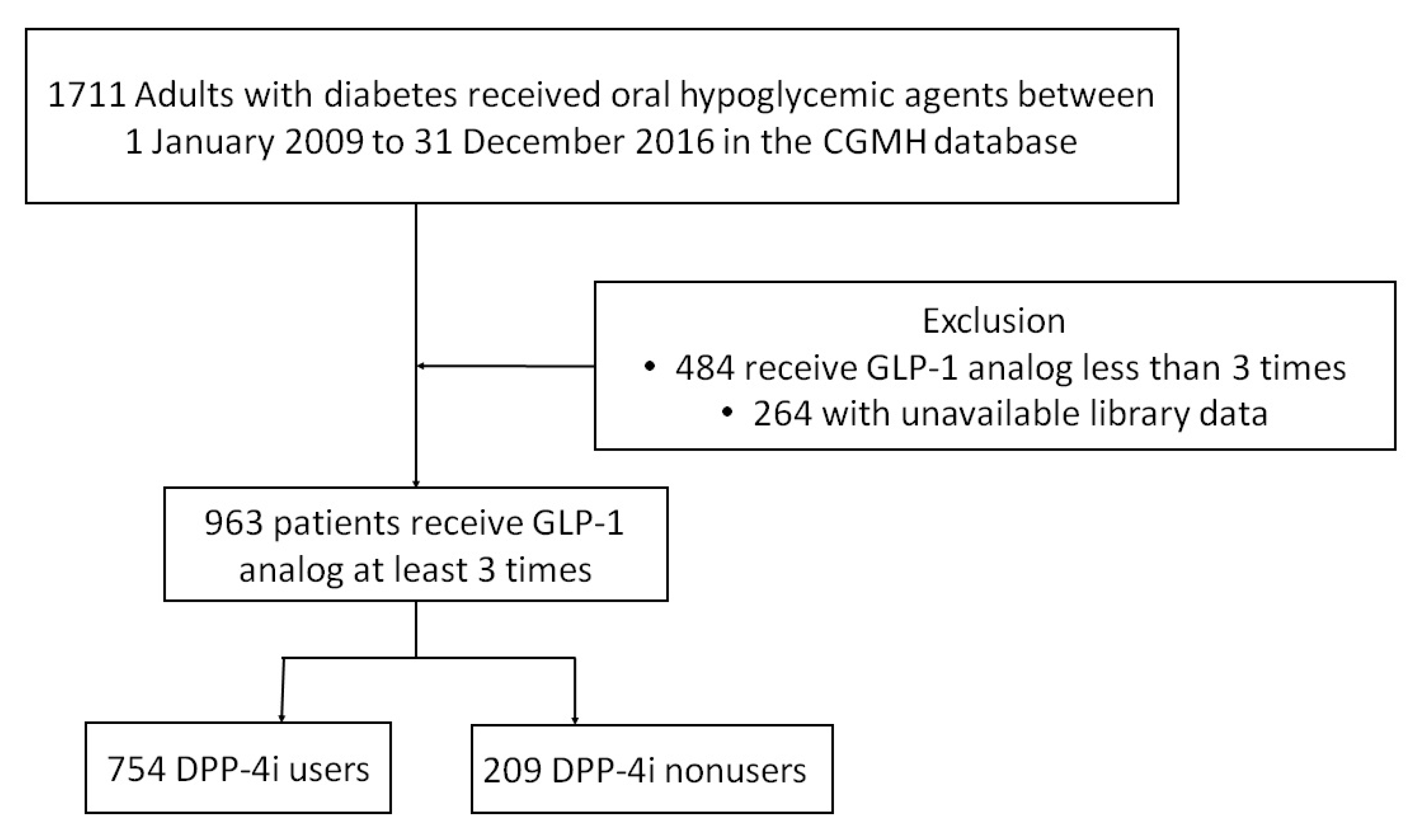
2.2. Study Population
2.3. Statistical Analyses
3. Results
3.1. Characteristics of the Study Population
3.2. Glucose Control Efficacy of Switching to GLP-1 RAs
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Care ADAJD. 9. Pharmacologic Approaches to Glycemic Treatment: Standards of Medical Care in Diabetes—2020. Diabetes Care 2020, 43, S98–S110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garber, A.J.; Handelsman, Y.; Grunberger, G.; Einhorn, D.; Abrahamson, M.J.; Barzilay, J.I.; Blonde, L.; Bush, M.A.; DeFronzo, R.A.; Garber, J.R.; et al. Consensus statement by the American Association of Clinical Endocrinologists and American College of Endocrinology on the comprehensive type 2 diabetes management algorithm–2020 executive summary. Endocr. Pract. 2020, 26, 107–139. [Google Scholar] [CrossRef] [PubMed]
- Thorens BJPotNAoS. Expression cloning of the pancreatic beta cell receptor for the gluco-incretin hormone glucagon-like peptide 1. Proc. Natl. Acad. Sci. USA 1992, 89, 8641–8645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, J.B.; Bethel, M.A.; Armstrong, P.W.; Buse, J.B.; Engel, S.S.; Garg, J.; Josse, R.; Kaufman, K.D.; Koglin, J.; Korn, S.; et al. Effect of sitagliptin on cardiovascular outcomes in type 2 diabetes. N. Engl. J. Med. 2015, 373, 232–242. [Google Scholar] [CrossRef] [Green Version]
- Scirica, B.M.; Bhatt, D.L.; Braunwald, E.; Steg, P.G.; Davidson, J.; Hirshberg, B.; Ohman, P.; Frederich, R.; Wiviott, S.D.; Hoffman, E.B.; et al. Saxagliptin and cardiovascular outcomes in patients with type 2 diabetes mellitus. N. Engl. J. Med. 2013, 369, 1317–1326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White, W.B.; Bakris, G.L.; Bergenstal, R.M.; Cannon, C.P.; Cushman, W.C.; Fleck, P.; Heller, S.; Mehta, C.; Nissen, S.E.; Perez, A.; et al. EXamination of cArdiovascular outcoMes with alogliptIN versus standard of carE in patients with type 2 diabetes mellitus and acute coronary syndrome (EXAMINE): A cardiovascular safety study of the dipeptidyl peptidase 4 inhibitor alogliptin in patients with type 2 diabetes with acute coronary syndrome. Am. Heart J. 2011, 162, 620–626.e621. [Google Scholar]
- Marso, S.P.; Daniels, G.H.; Brown-Frandsen, K.; Kristensen, P.; Mann, J.F.E.; Nauck, M.A.; Nissen, S.E.; Pocock, S.; Poulter, N.R.; Ravn, L.S.; et al. Liraglutide and cardiovascular outcomes in type 2 diabetes. N. Engl. J. Med. 2016, 375, 311–322. [Google Scholar] [CrossRef] [Green Version]
- Marso, S.P.; Bain, S.C.; Consoli, A.; Eliaschewitz, F.G.; Jódar, E.; Leiter, L.A.; Lingvay, I.; Rosenstock, J.; Seufert, J.; Warren, M.L.; et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N. Engl. J. Med. 2016, 375, 1834–1844. [Google Scholar] [CrossRef] [Green Version]
- Gerstein, H.C.; Colhoun, H.M.; Dagenais, G.R.; Diaz, R.; Lakshmanan, M.; Pais, P.; Probstfield, J.; Riesmeyer, J.S.; Riddle, M.C.; Rydén, L.; et al. Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND): A double-blind, randomised placebo-controlled trial. Lancet 2019, 394, 121–130. [Google Scholar] [CrossRef]
- Berra, C.C.; Resi, V.; Mirani, M.; Folini, L.; Rossi, A.; Solerte, S.B.; Fiorina, P. Clinical efficacy and predictors of response to dulaglutide in type-2 diabetes. Pharmacol. Res. 2020, 159, 104996. [Google Scholar] [CrossRef]
- Mirani, M.; Favacchio, G.; Serone, E.; Lucisano, G.; Rossi, M.C.; Berra, C.C. Liraglutide and cardiovascular outcomes in a real world type 2 diabetes cohort. Pharmacol. Res. 2018, 137, 270–279. [Google Scholar] [CrossRef] [PubMed]
- Lazzaroni, E.; Ben Nasr, M.; Loretelli, C.; Pastore, I.; Plebani, L.; Lunati, M.E.; Vallone, L.; Bolla, A.M.; Rossi, A.; Montefusco, L.; et al. Anti-diabetic drugs and weight loss in patients with type 2 diabetes. Pharmacol. Res. 2021, 171, 105782. [Google Scholar] [CrossRef] [PubMed]
- Rask, E.; Olsson, T.; Söderberg, S.; Holst, J.J.; Tura, A.; Pacini, G.; Ahrén, B. Insulin secretion and incretin hormones after oral glucose in non-obese subjects with impaired glucose tolerance. Metabolism 2004, 53, 624–631. [Google Scholar] [CrossRef] [PubMed]
- DeFronzo, R.A.; Okerson, T.; Viswanathan, P.; Guan, X.; Holcombe, J.H.; MacConell, L. Effects of exenatide versus sitagliptin on postprandial glucose, insulin and glucagon secretion, gastric emptying, and caloric intake: A randomized, cross-over study. Curr. Med Res. Opin. 2008, 24, 2943–2952. [Google Scholar] [CrossRef] [PubMed]
- Pratley, R.E.; Nauck, M.; Bailey, T.; Montanya, E.; Cuddihy, R.; Filetti, S.; Thomsen, A.B.; Søndergaard, R.E.; Davies, M. Liraglutide versus sitagliptin for patients with type 2 diabetes who did not have adequate glycaemic control with metformin: A 26-week, randomised, parallel-group, open-label trial. Lancet 2010, 375, 1447–1456. [Google Scholar] [CrossRef]
- Laakso, M.; Zilinskaite, J.; Hansen, T.; Boesgaard, T.W.; Vänttinen, M.; Stančáková, A.; Jansson, P.-A.; Pellmé, F.; Holst, J.J.; Kuulasmaa, T.; et al. Insulin sensitivity, insulin release and glucagon-like peptide-1 levels in persons with impaired fasting glucose and/or impaired glucose tolerance in the EUGENE2 study. Diabetologia 2008, 51, 502–511. [Google Scholar] [CrossRef]
- Fritsche, A.; Stefan, N.; Hardt, E.; Häring, H.; Stumvoll, M. Characterisation of beta-cell dysfunction of impaired glucose tolerance: Evidence for impairment of incretin-induced insulin secretion. Diabetologia 2000, 43, 852–858. [Google Scholar] [CrossRef] [Green Version]
- Bock, G.; Dalla Man, C.; Campioni, M.; Chittilapilly, E.; Basu, R.; Toffolo, G.; Cobelli, C.; Rizza, R. Pathogenesis of pre-diabetes: Mechanisms of fasting and postprandial hyperglycemia in people with impaired fasting glucose and/or impaired glucose tolerance. Diabetes 2006, 55, 3536–3549. [Google Scholar] [CrossRef] [Green Version]
- Ahmann, A.J.; Capehorn, M.; Charpentier, G.; Dotta, F.; Henkel, E.; Lingvay, I.; Holst, A.G.; Annett, M.P.; Aroda, V.R. Efficacy and safety of once-weekly semaglutide versus exenatide ER in subjects with type 2 diabetes (SUSTAIN 3): A 56-week, open-label, randomized clinical trial. Diabetes Care 2018, 41, 258–266. [Google Scholar] [CrossRef] [Green Version]
- DeFronzo, R.A.; Ratner, R.E.; Han, J.; Kim, D.D.; Fineman, M.S.; Baron, A.D. Effects of exenatide (exendin-4) on glycemic control and weight over 30 weeks in metformin-treated patients with type 2 diabetes. Diabetes Care 2005, 28, 1092–1100. [Google Scholar] [CrossRef] [Green Version]
- Buse, J.B.; Henry, R.R.; Han, J.; Kim, D.D.; Fineman, M.S.; Baron, A.D. Effects of exenatide (exendin-4) on glycemic control over 30 weeks in sulfonylurea-treated patients with type 2 diabetes. Diabetes Care 2004, 27, 2628–2635. [Google Scholar] [CrossRef] [PubMed]
- Kendall, D.M.; Riddle, M.C.; Rosenstock, J.; Zhuang, D.; Kim, D.D.; Fineman, M.S.; Baron, A.D. Effects of exenatide (exendin-4) on glycemic control over 30 weeks in patients with type 2 diabetes treated with metformin and a sulfonylurea. Diabetes Care 2005, 28, 1083–1091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahrén, B.; Masmiquel, L.; Kumar, H.; Sargin, M.; Karsbøl, J.D.; Jacobsen, S.H.; Chow, F. Efficacy and safety of once-weekly semaglutide versus once-daily sitagliptin as an add-on to metformin, thiazolidinediones, or both, in patients with type 2 diabetes (SUSTAIN 2): A 56-week, double-blind, phase 3a, randomised trial. Lancet Diabetes Endocrinol. 2017, 5, 341–354. [Google Scholar] [CrossRef]
- Pratley, R.E.; Nauck, M.A.; Bailey, T.; Montanya, E.; Filetti, S.; Garber, A.J.; Thomsen, A.B.; Furber, S.; Davies, M. Efficacy and safety of switching from the DPP-4 inhibitor sitagliptin to the human GLP-1 analog liraglutide after 52 weeks in metformin-treated patients with type 2 diabetes: A randomized, open-label trial. Diabetes Care 2012, 35, 1986–1993. [Google Scholar] [CrossRef] [Green Version]
- Wysham, C.; Bergenstal, R.; Malloy, J.; Yan, P.; Walsh, B.; Malone, J.; Taylor, K. DURATION-2, efficacy and safety of switching from maximum daily sitagliptin or pioglitazone to once-weekly exenatide. Diabet. Med. 2011, 28, 705–714. [Google Scholar] [CrossRef] [Green Version]
- Bihan, H.; Ng, W.L.; Magliano, D.J.; Shaw, J.E. Predictors of efficacy of GLP-1 agonists and DPP-4 inhibitors: A systematic review. Diabetes research and clinical practice. Diabetes Res. Clin. Pract. 2016, 121, 27–34. [Google Scholar] [CrossRef]
- Degn, K.B.; Juhl, C.B.; Sturis, J.; Jakobsen, G.; Brock, B.; Chandramouli, V.; Rungby, J.; Landau, B.R.; Schmitz, O. One week’s treatment with the long-acting glucagon-like peptide 1 derivative liraglutide (NN2211) markedly improves 24-h glycemia and alpha- and beta-cell function and reduces endogenous glucose release in patients with type 2 diabetes. Diabetes 2004, 53, 1187–1194. [Google Scholar] [CrossRef] [Green Version]
- Aschner, P.; Kipnes, M.S.; Lunceford, J.K.; Sanchez, M.; Mickel, C.; Williams-Herman, D.E. Effect of the dipeptidyl peptidase-4 inhibitor sitagliptin as monotherapy on glycemic control in patients with type 2 diabetes. Diabetes Care 2006, 29, 2632–2637. [Google Scholar] [CrossRef] [Green Version]
- Kahn, S.E.; Haffner, S.M.; Heise, M.A.; Herman, W.H.; Holman, R.R.; Jones, N.P.; Kravitz, B.G.; Lachin, J.M.; O’Neill, M.C.; Zinman, B.; et al. Glycemic durability of rosiglitazone, metformin, or glyburide monotherapy. N. Engl. J. Med. 2006, 355, 2427–2443. [Google Scholar] [CrossRef] [Green Version]
- Sherifali, D.; Nerenberg, K.; Pullenayegum, E.; Cheng, J.E.; Gerstein, H.C. The effect of oral antidiabetic agents on A1C levels: A systematic review and meta-analysis. Diabetes Care 2010, 33, 1859–1864. [Google Scholar] [CrossRef] [Green Version]
- Shao, S.C.; Chan, Y.Y.; Yang, Y.K.; Lin, S.; Hung, M.; Chien, R.; Lai, C.; Lai, E.C. The Chang Gung Research Database—A multi-institutional electronic medical records database for real-world epidemiological studies in Taiwan. Pharmacoepidemiol. Drug Saf. 2019, 28, 593–600. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| DPP4-i Users | DPP4-i Nonusers | p Value | |
|---|---|---|---|
| (n = 754) | (n = 209) | ||
| Age (years) | 51.7 (11.5) | 50.9 (12.1) | 0.369 |
| Sex: male (%) | 336 (44.5%) | 95 (45.5%) | 0.818 |
| Height (cm) | 163.1 (8.7) | 162.4 (9.6) | 0.302 |
| Weight (kg) | 83.4 (17.8) | 84.6 (20.9) | 0.452 |
| Body mass index (kg/m2) | 31.3 (5.6) | 31.9 (6.3) | 0.300 |
| HbA1c (%) | 9.3 (1.5) | 9.3 (1.4) | 0.873 |
| Total cholesterol (mg/dL) | 174.6 (33.9) | 183.6 (38.0) | 0.001 |
| Triglycerides (mg/dL) | 194.8 (148.9) | 194.5 (144.52) | 0.981 |
| HDL-cholesterol (mg/dL) | 43.7 (11.1) | 45.2 (10.1) | 0.087 |
| LDL-cholesterol (mg/dL) | 97.6 (26.2) | 106.6 (29.6) | <0.001 |
| GPT (U/L) | 40.2 (29.3) | 42.5 (35.0) | 0.414 |
| Creatinine (mg/dL) | 0.93 (0.78) | 0.83 (0.30) | 0.010 |
| Number of oral anti-hyperglycemia agents | |||
| Metformin | 740 (98.1%) | 170 (81.3%) | <0.001 |
| Sulfonylurea | 700 (92.8%) | 134 (64.1%) | <0.001 |
| Glinides | 80 (10.6%) | 10 (4.8%) | 0.01 |
| Thiazolidinedione | 367 (48.7%) | 56 (26.8%) | <0.001 |
| α-glucosidase inhibitors | 338 (44.8) | 44 (21.1%) | <0.001 |
| SGLT2 inhibitors | 2 (0.3%) | 0 (0.0%) | 1.000 |
| Insulin regimen | |||
| Basal insulin | 284 (37.7%) | 60 (28.7%) | 0.017 |
| Rapid-acting insulin | 46 (6.1%) | 18 (8.61%) | 0.197 |
| Premix insulin | 203 (26.9%) | 55 (26.3%) | 0.861 |
| DPP-4 i Users | DPP-4 I Nonusers | DPP4-i Users | DPP4-i Nonusers | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Before GLP-1 RAs | After GLP-1 RAs | Before GLP-1 RAs | After GLP-1 RAs | Change from baseline | Change from baseline | ||||||
| Glycemic outcome | N | HbA1c | HbA1c | p-value | N | HbA1c | HbA1c | p-value | HbA1c | HbA1c | p-value |
| 754 | 9.34 (±1.48) | 8.92 (±1.42) | <0.001 | 209 | 9.32 (±1.40) | 8.34 (±1.55) | <0.001 | −0.42 (±2.04) | −0.99 (±2.06) | <0.001 | |
| Number of diabetes medications | |||||||||||
| 0 | 5 [0.66%] | 8.36 (±1.26) | 7.80 (±1.27) | 0.312 | 25 [11.96%] | 9.11 (±1.31) | 8.13 (±1.62) | 0.007 | −0.56 (±1.08) | −0.98 (±1.67) | 0.594 |
| 1 | 5 [0.66%] | 9.56 (±0.91) | 9.02 (±1.09) | 0.363 | 30 [14.35%] | 9.25 (±1.35) | 7.55 (±1.13) | <0.001 | −0.54 (±1.18) | −1.69 (±1.80) | 0.178 |
| 2 | 24 [3.18%] | 9.18 (±1.32) | 8.43 (±1.31) | 0.064 | 57 [27.27%] | 9.45 (±1.40) | 8.25 (±1.38) | <0.001 | −0.75 (±1.88) | −1.20 (±2.08) | 0.360 |
| 3 | 158 [20.95%] | 9.46 (±1.58) | 8.55 (±1.36) | <0.001 | 56 [26.79%] | 9.18 (±1.44) | 8.39 (±1.62) | 0.013 | −0.91 (±2.22) | −0.79 (±2.31) | 0.743 |
| ≥4 | 562 [74.53%] | 9.32 (±1.46) | 9.05 (±1.42) | 0.001 | 41 [19.61%] | 9.52 (±1.46) | 9.08 (±1.64) | 0.157 | −0.27 (±1.99) | −0.44 (±1.97) | 0.586 |
| Group by level of HbA1c | |||||||||||
| <7 | 23 [3.05%] | 6.49 (±0.38) | 8.93 (±1.41) | <0.001 | 5 [2.39%] | 6.44 (±0.50) | 7.36 (±0.81) | 0.081 | 2.44 (±1.40) | 0.92 (±0.89) | 0.029 |
| 7~9 | 298 [39.52%] | 8.13 (±0.52) | 9.00 (±1.44) | <0.001 | 78 [37.32%] | 8.11 (±0.54) | 8.33 (±1.49) | 0.200 | 0.87 (±1.53) | 0.22 (±1.51) | 0.001 |
| ≧9 | 433 [57.42%] | 10.33 (±1.08) | 8.87 (±1.41) | <0.001 | 126 [60.28%] | 10.19 (±1.04) | 8.38 (±1.60) | <0.001 | −1.46 (±1.70) | −1.81 (±1.98) | 0.052 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsai, C.-J.; Tsao, C.-F. Comparison of Glucose Lowering Efficacy of Human GLP-1 Agonist in Taiwan Type 2 Diabetes Patients after Switching from DPP-4 Inhibitor Use or Non-Use. J. Pers. Med. 2022, 12, 1915. https://doi.org/10.3390/jpm12111915
Tsai C-J, Tsao C-F. Comparison of Glucose Lowering Efficacy of Human GLP-1 Agonist in Taiwan Type 2 Diabetes Patients after Switching from DPP-4 Inhibitor Use or Non-Use. Journal of Personalized Medicine. 2022; 12(11):1915. https://doi.org/10.3390/jpm12111915
Chicago/Turabian StyleTsai, Chia-Jen, and Cheng-Feng Tsao. 2022. "Comparison of Glucose Lowering Efficacy of Human GLP-1 Agonist in Taiwan Type 2 Diabetes Patients after Switching from DPP-4 Inhibitor Use or Non-Use" Journal of Personalized Medicine 12, no. 11: 1915. https://doi.org/10.3390/jpm12111915