
Adoption of a Digital Patient Health Passport as Part of a Primary Healthcare Service Delivery: Systematic Review
 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Method
2.1. Protocol and Registration
2.2. Research Question
2.3. Search Strategy
2.4. Identification
2.5. Screening
2.5.1. Study Selection and Extraction
2.5.2. Eligibility Criteria
2.5.3. Assessment of Quality
2.6. Data Extraction and Data Analysis
3. Results
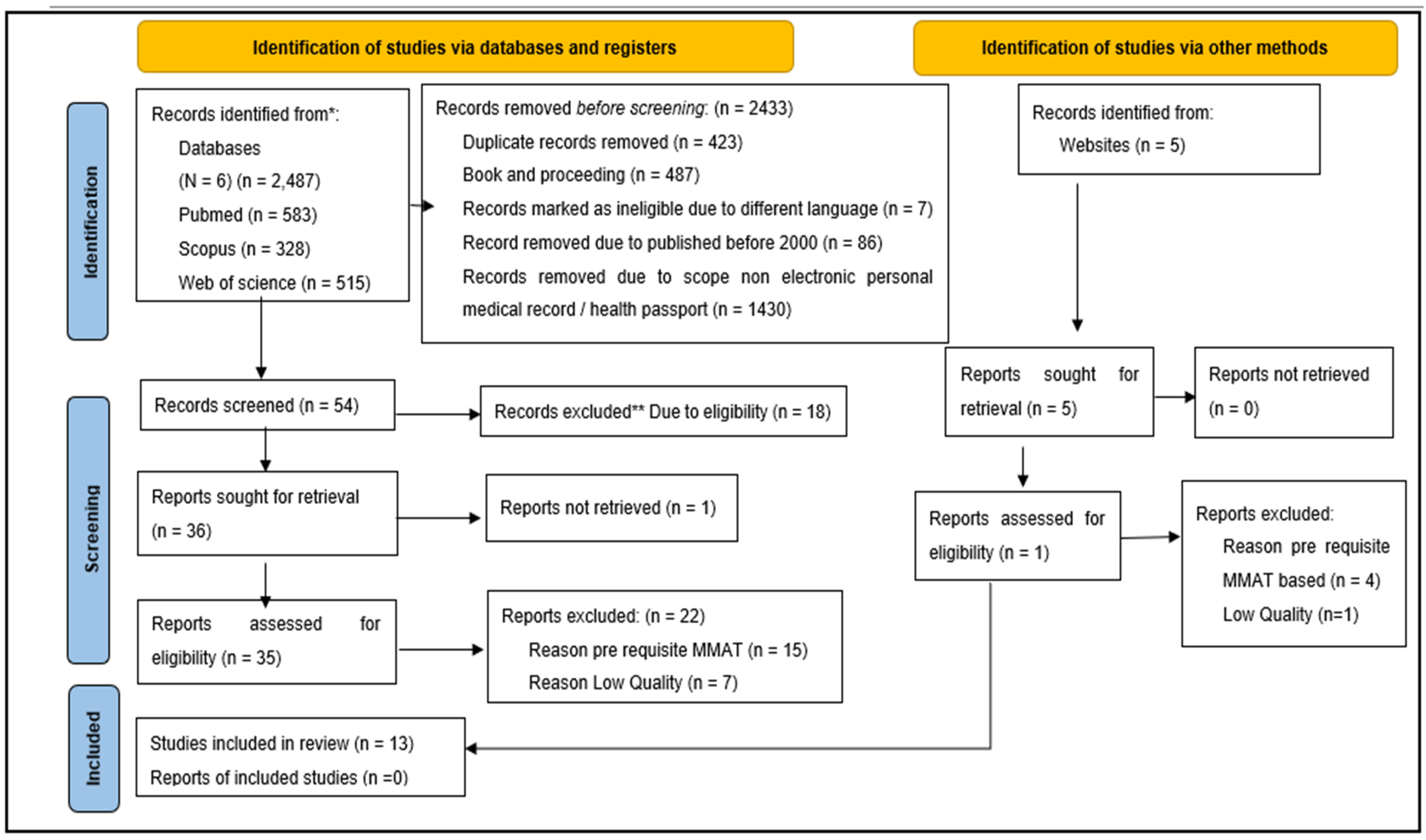
3.1. Study Selection
3.2. Developed Themes
3.3. Empowerment
3.4. Help in Communication
3.5. Improve Relationship
3.6. Improve Quality of Care
3.7. Maintaining Health Records
3.8. Records Sharing
3.9. Time Saving
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A. Searching Systematic Review
| Population/problem/patient | Intervention | Comparison/context | Outcome |
| Primary care User | Using the Digital health passport | Not using the Digital health passport | Benefit |
- Synonym
- Related term
- Variation
| Population/problem/patient | Intervention | Comparison | Outcome | |
| PICO | Primary care User | Using the Digital health passport | Not using the mobile health app | Benefit |
| Primary care Operator | Digital Personal Health Record(s) | Acceptable | ||
| Primary care Worker | Digital Personal Health Information(s), | Efficiency | ||
| Primary care Patient | Digital Personal Medical Record(s) | Success | ||
| Primary healthcare Operator | Digital Personal Dental Record(s) | Usefulness | ||
| Primary healthcare Worker | Personal Health Record(s) | Efficacy | ||
| Primary Healthcare Patient(s) | Personal Health Information(s), | Use | ||
| Primary Healthcare providers | Personal Medical Record(s) | Effectiveness | ||
| Healthcare providers | Personal Dental Record(s) | Helpful | ||
| Healthcare professional | Digital Mobile health app | Value | ||
| Primary Healthcare professional | Digital mobile dental app | Usability | ||
| Primary health care Operator | Digital health passport usage | Inefficient | ||
| Patient(s) | Ineffective | |||
| Doctor(s) | useless | |||
| Nurse(s) | Advantage | |||
| dental therapies | ||||
| dental hygienist(s) | ||||
| midwife |
- I.
- PubMed
- II.
- Scopus
- III.
- EBSCO
- IV.
- Web of Science
- V.
- Google Scholar
Appendix B. Searching Strategy Result
- I.
- PubMed:
| No. | Concept | Search String: PubMed | Number |
| #1 | Benefit/Advantage | ((((((((((((((((((advantage s[MeSH Terms]) OR (analysis, cost benefit[MeSH Terms])) OR (analysis, cost benefit[MeSH Terms])) OR (usage[MeSH Terms])) OR (acceptance(s)[MeSH Terms])) OR (acceptable[MeSH Terms])) OR (acceptability[MeSH Terms])) OR (efficiency[MeSH Terms])) OR (success[MeSH Terms])) OR (usefull[MeSH Terms])) OR (efficacy[MeSH Terms])) OR (use[MeSH Terms])) OR (effectiveness[MeSH Terms])) OR (helpfull[MeSH Terms])) OR (value[MeSH Terms])) OR (usability[MeSH Terms])) OR (adaptation[MeSH Terms])) OR (adaptable[MeSH Terms])) OR (adaptability[MeSH Terms]) | 278,496 |
| #2 | Digital Health passport usage | (((((((((((Digital health passport[MeSH Terms]) OR (Digital Personal Health Record(s)[MeSH Terms])) OR (Digital Personal Health Information(s)[MeSH Terms])) OR (Digital Personal Medical Record(s)[MeSH Terms])) OR (Digital Personal Dental Record(s)[MeSH Terms])) OR (Personal Health Record(s)[MeSH Terms])) OR (Personal Health Information(s)[MeSH Terms])) OR (Personal Medical Record(s)[MeSH Terms])) OR (Personal Dental Record(s)[MeSH Terms])) OR (Digital Mobile health app[MeSH Terms])) OR (Digital mobile dental app[MeSH Terms])) OR (Digital health passport usage[MeSH Terms]) | 17,223 |
| #3 | Potential User | ((((((((((((((((((((((Primary care User[MeSH Terms]) OR (Primary care Operator[MeSH Terms])) OR (Primary care Worker[MeSH Terms])) OR (Primary care Patient[MeSH Terms])) OR (Primary healthcare Operator[MeSH Terms])) OR (Primary healthcare Worker[MeSH Terms])) OR (Primary Healthcare Patient(s)[MeSH Terms])) OR (Primary Healthcare provider(s)[MeSH Terms])) OR (Healthcare provider(s)[MeSH Terms])) OR (Healthcare professional[MeSH Terms])) OR (Primary Healthcare professional(s)[MeSH Terms])) OR (Primary health care Operator(s)[MeSH Terms])) OR (out patients[MeSH Terms])) OR (Doctors[MeSH Terms])) OR (nurses[MeSH Terms])) OR (dental nurse(s)[MeSH Terms])) OR (dental therapist[MeSH Terms])) OR (dental hygienist[MeSH Terms])) OR (dental hygienists[MeSH Terms])) OR (medical assistance[MeSH Terms])) OR (nurse midwife[MeSH Terms])) OR (midwife[MeSH Terms])) OR (health care provider[MeSH Terms]) | 847,494 |
| Total | (#1 AND #2 AND #3) | 583 |
- II.
- SCOPUS:
| No. | Concept | Search String: SCOPUS | Number |
| #1 | Benefit | (advantage* OR cost benefit OR usage OR acceptance* OR acceptable OR acceptability OR efficiency OR success OR useful OR efficacy OR use OR effectiveness OR helpful OR value OR usability OR adaptation OR adaptable OR adaptability) | 1,932,408 |
| #2 | Digital Health passport usage | (Digital health passport* OR Digital Personal Health Record* OR Digital Personal Health Information* OR Digital Personal Medical Record* OR Digital Personal Dental Record* OR Personal Health Record* OR Personal Health Information* OR Personal Medical Record* OR Personal Dental Record* OR Digital Mobile health app* OR Digital mobile dental app* OR Digital health passport usage) | 3449 |
| #3 | Potential User | (“Primary care User*” OR “Primary care Operator*” OR “Primary care Worker” OR “Primary care Patient*” OR “Primary healthcare Operator*” OR “Primary healthcare Worker*” OR “Primary Healthcare Patient*” OR “Primary Healthcare provider*” OR “Healthcare provider*” OR “Healthcare professional” OR “Primary Healthcare professional*” OR “Primary health care Operator*” OR out*patient* OR Doctors OR nurse* OR “dental nurse*” OR “dental therapist*” OR “dental hygienist*” OR dentist* OR “medical assistance” OR “nurse midwife” OR midwife OR “health care provider*”) | 1,314,396 |
| Total | (#1 AND #2 AND #3) | 328 |
- III.
- EBSCO:
| No. | Concept | Search String: EBSCO | Number |
| #1 | Benefit | advantage* OR “cost benefit” OR usage OR acceptance* OR acceptable OR acceptability OR efficiency OR success OR useful OR efficacy OR use OR effectiveness OR helpful OR value OR usability OR adaptation OR adaptable OR adaptability | 6,951,959 |
| #2 | Digital Health passport usage | “Digital health passport*” OR “Digital Personal Health Record*” OR “Digital Personal Health Information*” OR “Digital Personal Medical Record*” OR “Digital Personal Dental Record*” OR “Personal Health Record*” OR “Personal Health Information*” OR “Personal Medical Record*” OR “Personal Dental Record*” OR “Digital Mobile health app*” OR “Digital mobile dental app*” OR “Digital health passport usage” | 1381 |
| #3 | Potential User | “Primary care User*” OR “Primary care Operator*” OR “Primary care Worker*” OR “Primary care Patient*” OR “Primary healthcare Operator*” OR “Primary healthcare Worker*” OR “Primary Healthcare Patient*” OR “Primary Healthcare provider*” OR “Healthcare provider*” OR “Healthcare professional*” OR “Primary Healthcare professional*” OR “Primary health care Operator*” OR “out*patient*” OR doctor* OR nurse* OR “dental nurse*” OR “dental therapist*” OR “dental hygienist*” OR “dentist*” OR “medical assistance*” OR “nurse midwife” OR “midwife” OR “health care provider*” | 588,313 |
| Total | (#1 AND #2 AND #3) | 231 |
- IV.
- Web of Sciences
| No. | Concept | Search String: Web of Sciences | Number |
| #1 | Benefit | (ALL = ((advantage* OR “cost benefit” OR usage OR acceptance* OR acceptable OR acceptability OR efficiency OR success OR useful OR efficacy OR use OR effectiveness OR helpful OR value OR usability OR adaptation OR adaptable OR adaptability))) | 27,747,961 |
| #2 | Digital Health passport usage | ALL = ((“Digital health passport*” OR “Digital Personal Health Record*” OR “Digital Personal Health Information*” OR “Digital Personal Medical Record*” OR “Digital Personal Dental Record*” OR “Personal Health Record*” OR “Personal Health Information*” OR “Personal Medical Record*” OR “Personal Dental Record*” OR “Digital Mobile health app*” OR “Digital mobile dental app*” OR “Digital health passport usage”)) | 2633 |
| #3 | Potential User | ALL = ((“Primary care User*” OR “Primary care Operator*” OR “Primary care Worker*” OR “Primary care Patient*” OR “Primary healthcare Operator*” OR “Primary healthcare Worker*” OR “Primary Healthcare Patient*” OR “Primary Healthcare provider*” OR “Healthcare provider*” OR “Healthcare professional*” OR “Primary Healthcare professional*” OR “Primary health care Operator*” OR “out*patient*” OR doctor* OR nurse* OR “dental nurse*” OR “dental therapist*” OR “dental hygienist*” OR “dentist*” OR “medical assistance*” OR “nurse midwife” OR “midwife” OR “health care provider*”)) | 1,258,928 |
| #4 | Total | (#1 AND #2 AND #3) | 515 |
- V.
- Google Scholar
- Using engine
- URL: https://harzing.com/resources/publish-or-perish (accessed on 1 August 2021)
- Search String
- advantage* OR “cost benefit” OR usage OR acceptance* OR acceptable OR acceptability OR efficiency OR success OR useful OR efficacy OR use OR effectiveness OR helpful OR value OR usability OR adaptation OR adaptable OR adaptability AND “Digital health passport*” OR “Digital Personal Health Record*” OR “Digital Personal Health Information*” OR “Digital Personal Medical Record*” OR “Digital Personal Dental Record*” OR “Personal Health Record*” OR “Personal Health Information*” OR “Personal Medical Record*” OR “Personal Dental Record*” OR “Digital Mobile health app*” OR “Digital mobile dental app*” OR “Digital health passport usage” AND “Primary care User*” OR “Primary care Operator*” OR “Primary care Worker*” OR “Primary care Patient*” OR “Primary healthcare Operator*” OR “Primary healthcare Worker*” OR “Primary Healthcare Patient*” OR “Primary Healthcare provider*” OR “Healthcare provider*” OR “Healthcare professional*” OR “Primary Healthcare professional*” OR “Primary health care Operator*” OR “out*patient*” OR doctor* OR nurse* OR “dental nurse*” OR “dental therapist*” OR “dental hygienist*” OR “dentist*” OR “medical assistance*” OR “nurse midwife” OR “midwife” OR “health care provider*”

- 4.
- Filter
- 5.
- Save to endnote
- 6.
- Create a folder for Google Scholar

Appendix C. The Criteria Used to Determine the Rigour of the Methodology and Analysis Used in the Selected Articles

{kind=link}
{kind=link}
{kind=link}
| Research Design | Assessment Criteria |
|---|---|
| Qualitative | QA1—Is the qualitative approach appropriate to answer the research question? QA2—Are the qualitative data collection methods adequate to address the research question? QA3—Are the findings adequately derived from the data? QA4—Is the interpretation of results sufficiently substantiated by data? QA5—Is there coherence between qualitative data sources, collection, analysis and interpretation? |
| Quantitative (descriptive) | QA1—Is the sampling strategy relevant to address the research question? QA2—Is the sample representative of the target population? QA3—Are the measurements appropriate? QA4—Is the risk of nonresponse bias low? QA5—Is the statistical analysis appropriate to answer the research question? |
| Quantitative (non-randomised) | QA1—Are the participants representative of the target population? QA2—Are measurements appropriate regarding both the outcome and intervention (or exposure)? QA3—Are there complete outcome data? QA4—Are the confounders accounted for in the design and analysis? QA5—During the study period, is the intervention administered (or exposure occurred) as intended? |
| Mixed methods | QA1—Is there an adequate rationale for using a mixed methods design to address the research question? QA2—Are the different components of the study effectively integrated to answer the research question? QA3—Are the outputs of the integration of qualitative and quantitative components adequately interpreted? QA4—Are divergences and inconsistencies between quantitative and qualitative results adequately addressed? QA5—Do the different components of the study adhere to the quality criteria of each tradition of the methods involved? |
References
- Mort, M.; Smith, A. Beyond information: Intimate relations in sociotechnical practice. Sociology 2009, 43, 215–231. [Google Scholar] [CrossRef]
- Mort, M.; Finch, T.; May, C. Making and unmaking telepatients: Identity and governance in new health technologies. Sci. Technol. Hum. Values 2009, 34, 9–33. [Google Scholar] [CrossRef] [Green Version]
- Kumar, S.; Bauer, K. The business case for implementing electronic health records in primary care settings in the United States. J. Revenue Pricing Manag. 2011, 10, 119–131. [Google Scholar] [CrossRef]
- Noraziani, K.; Nurul’Ain, A.; Azhim, M.; Eslami, S.R.; Drak, B.; Sharifa Ezat, W.; Siti Nurul Akma, A. An overview of electronic medical record implementation in healthcare system: Lesson to learn. World Appl. Sci. J. 2013, 25, 323–332. [Google Scholar]
- Mohd, H.; Mohamad, S.M.S. Acceptance Model Electronic Medical Record EMR. J. Adv. Inf. Manag. Stud. 2005, 2, 16. [Google Scholar]
- Almeida, F.L. Benefits, challenges and tools of big data management. J. Syst. Integr. 2017, 8, 12–20. [Google Scholar]
- Zhang, Z.; Yan, C.; Mesa, D.A.; Sun, J.; Malin, B.A. Ensuring electronic medical record simulation through better training, modeling, and evaluation. J. Am. Med. Inform. Assoc. 2019, 27, 99–108. [Google Scholar] [CrossRef]
- Park, H.S.; Cho, H.; Kim, H.S. Development of a multi-agent m-health application based on various protocols for chronic disease self-management. J. Med. Syst. 2016, 40, 36. [Google Scholar] [CrossRef]
- Ahmadi, M.; Jeddi, F.R.; Gohari, M.R.; Sadoughi, F. A review of the personal health records in selected countries and Iran. J. Med. Syst. 2012, 36, 371–382. [Google Scholar] [CrossRef] [PubMed]
- Lane, L. Healthy start for South African health passport. Biom. Technol. Today 2009, 2009, 2–3. [Google Scholar]
- Chen, H.-M.; Liou, Y.-Z. Performance evaluation of continuity of care records (CCRs): Parsing models in a mobile health management system. J. Med. Syst. 2014, 38, 117. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Chou, J.; Wang, F. Integrative analysis of patient health records and neuroimages via memory-based graph convolutional network. In Proceedings of the 2018 IEEE International Conference on Data Mining (ICDM), Singapore, 17–20 November 2018. [Google Scholar]
- Pretlow, R.; Stock, C.; Allison, S.; Roeger, L. Treatment of child/adolescent obesity using the addiction model: A smartphone app pilot study. Child Obes. 2015, 11, 248–259. [Google Scholar] [CrossRef]
- Ahmadi, M.; Shahrokhi, S.N.; Khavaninzadeh, M.; Alipour, J. Development of a Mobile-Based Self-care Application for Patients with Breast Cancer-Related Lymphedema in Iran. Appl. Clin. Inform. 2022, 13, 935–948. [Google Scholar] [CrossRef] [PubMed]
- Subramani Parasuraman, A.T.S.; Yee, S.W.K.; Chuon, B.L.C.; Ren, L.Y. Smartphone usage and increased risk of mobile phone addiction: A concurrent study. Int. J. Pharm. Investig. 2017, 7, 125. [Google Scholar] [CrossRef] [PubMed]
- Cabana, M.D.; Jee, S.H. Does continuity of care improve patient outcomes. J. Fam. Pract. 2004, 53, 974–980. [Google Scholar]
- Karazivan, P.; Dumez, V.; Flora, L.; Pomey, M.-P.; Del Grande, C.; Ghadiri, D.P.; Fernandez, N.; Jouet, E.; Las Vergnas, O.; Lebel, P. The patient-as-partner approach in health care: A conceptual framework for a necessary transition. Acad. Med. 2015, 90, 437–441. [Google Scholar] [CrossRef]
- Hirsh, D.A.; Ogur, B.; Thibault, G.E.; Cox, M. “Continuity” as an organizing principle for clinical education reform. N. Engl. J. Med. 2007, 356, 858. [Google Scholar] [CrossRef] [Green Version]
- Singh, K.; Landman, A.B. Mobile health. In Key Advances in Clinical Informatics; Elsevier: Amsterdam, The Netherlands, 2017; pp. 183–196. [Google Scholar]
- Maraolo, A.E. Una bussola per le revisioni sistematiche: La versione italiana della nuova edizione del PRISMA statement. BMJ 2021, 372, n71. [Google Scholar]
- Kraus, S.; Breier, M.; Dasí-Rodríguez, S. The art of crafting a systematic literature review in entrepreneurship research. Int. Entrep. Manag. J. 2020, 16, 1023–1042. [Google Scholar] [CrossRef] [Green Version]
- Hong, Q.N.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.-P.; Griffiths, F.; Nicolau, B.; O’Cathain, A. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Educ. Inf. 2018, 34, 285–291. [Google Scholar] [CrossRef] [Green Version]
- Matthew, J.P.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 89. [Google Scholar]
- Petticrew, M.; Roberts, H. Systematic Reviews in the Social Sciences: A Practical Guide; Blackwell: Malden, MA, USA, 2006; Volume 6, pp. 304–305. [Google Scholar]
- Braun, V.; Clarke, V. Reflecting on reflexive thematic analysis. Qual. Res. Sport Exerc. Health 2019, 11, 589–597. [Google Scholar] [CrossRef]
- Flemming, K.; Booth, A.; Garside, R.; Tunçalp, Ö.; Noyes, J. Qualitative evidence synthesis for complex interventions and guideline development: Clarification of the purpose, designs and relevant methods. BMJ Glob. Health 2019, 4, e000882. [Google Scholar] [CrossRef] [Green Version]
- Kiger, M.E.; Varpio, L. Thematic analysis of qualitative data: AMEE Guide No. 131. Med. Teach. 2020, 42, 846–854. [Google Scholar] [CrossRef]
- Wynia, M.K.; Torres, G.W.; Lemieux, J. Many Physicians Are Willing To Use Patients’ Electronic Personal Health Records, But Doctors Differ By Location, Gender, And Practice. Health Aff. 2011, 30, 266–273. [Google Scholar] [CrossRef] [PubMed]
- Tawara, S.; Yonemochi, Y.; Kosaka, T.; Kouzaki, Y.; Takita, T.; Tsuruta, T. Use of patients’ mobile phones to store and share personal health information: Results of a questionnaire survey. Intern. Med. 2013, 52, 751–756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruiz, J.G.; Andrade, A.D.; Hogue, C.; Karanam, C.; Akkineni, S.; Cevallos, D.; Anam, R.; Sharit, J. The Association of Graph Literacy With Use of and Skills Using an Online Personal Health Record in Outpatient Veterans. J. Health Commun. 2016, 21, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Petrou, M.A.; Santamaria, R.M.; Romasew, A.; Splieth, C.H. Dissemination and use of the children’s dental pass in Germany. Oral Health Prev. Dent. 2015, 13, 129–134. [Google Scholar] [CrossRef]
- Marchak, J.G.; Cherven, B.; Williamson Lewis, R.; Edwards, P.; Meacham, L.R.; Palgon, M.; Escoffery, C.; Mertens, A.C. User-centered design and enhancement of an electronic personal health record to support survivors of pediatric cancers. Support. Care Cancer 2020, 28, 3905–3914. [Google Scholar] [CrossRef]
- Lopez Segui, F.; Pratdepadua Bufill, C.; Abdon Gimenez, N.; Martinez Roldan, J.; Garcia Cuyas, F. The Prescription of Mobile Apps by Primary Care Teams: A Pilot Project in Catalonia. JMIR Mhealth Uhealth 2018, 6, e10701. [Google Scholar] [CrossRef]
- Hanna, L.; Gill, S.D.; Newstead, L.; Hawkins, M.; Osborne, R.H. Patient perspectives on a personally controlled electronic health record used in regional Australia: ‘I can be like my own doctor’. Health Inf. Manag. J. 2017, 46, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Druss, B.G.; Ji, X.; Glick, G.; von Esenwein, S.A. Randomized trial of an electronic personal health record for patients with serious mental illnesses. Am. J. Psychiatry 2014, 171, 360–368. [Google Scholar] [CrossRef] [PubMed]
- Dontje, K.; Corser, W.D.; Holzman, G. Understanding patient perceptions of the electronic personal health record. J. Nurse Pract. 2014, 10, 824–828. [Google Scholar] [CrossRef]
- Donovan, D.J.; Macciola, D.; Paul, E.A.; Rama, G.; Krishnan, U.; Starc, T.J.; Weller, R.J.; Glickstein, J.S. Design and implementation of a patient passport in a pediatric cardiology clinic. Prog. Pediatr. Cardiol. 2020, 59, 101208. [Google Scholar] [CrossRef]
- Davis, S.; MacKay, L. Moving Beyond the Rhetoric of Shared Decision-Making: Designing Personal Health Record Technology With Young Adults With Type 1 Diabetes. Can. J. Diabetes 2020, 44, 434–441. [Google Scholar] [CrossRef]
- Aston, M.; Sweet, K.; McAfee, E.; Price, S.; Sheriko, J.; Monaghan, J.; Filliter, J.; Walls, C.; McGrath, P.; Vanderlee, E.; et al. Snap shot: Achieving better care through a one-page personal health profile. J. Intellect. Disabil. 2021, 25, 230–241. [Google Scholar] [CrossRef]
- Abelson, J.S.; Kaufman, E.; Symer, M.; Peters, A.; Charlson, M.; Yeo, H. Barriers and benefits to using mobile health technology after operation: A qualitative study. Surgery 2017, 162, 605–611. [Google Scholar] [CrossRef]
- Chandrashekar, P. Do mental health mobile apps work: Evidence and recommendations for designing high-efficacy mental health mobile apps. Mhealth 2018, 4, 6. [Google Scholar] [CrossRef] [Green Version]
- Marshall, J.M.; Dunstan, D.A.; Bartik, W. Effectiveness of using mental health mobile apps as digital antidepressants for reducing anxiety and depression: Protocol for a multiple baseline across-individuals design. JMIR Res. Protoc. 2020, 9, e17159. [Google Scholar] [CrossRef]
- Alkhalifah, J.M.; Seddiq, W.; Alshehri, B.F.; Alhaluli, A.H.; Alessa, M.M.; Alsulais, N.M. The role of the COVID-19 pandemic in expediting digital health-care transformation: Saudi Arabia’s experience. Inform. Med. Unlocked 2022, 33, 101097. [Google Scholar] [CrossRef]
- Chatzimarkakis, J. Why patients should be more empowered: A European perspective on lessons learned in the management of diabetes. J. Diabetes Sci. Technol. 2010, 4, 1570–1573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filip, R.; Puscaselu, R.G.; Anchidin-Norocel, L.; Dimian, M.; Savage, W.K. Global Challenges to Public Health Care Systems during the COVID-19 Pandemic: A Review of Pandemic Measures and Problems. J. Pers. Med. 2022, 12, 1295. [Google Scholar] [CrossRef]
- Rahman, N.; Nathwani, S.; Kandiah, T. Teledentistry from a patient perspective during the coronavirus pandemic. Br. Dent. J. 2020, 229, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Punhani, R.; Saini, S.; Varun, N.; Rustagi, R. mHealth: A Resolution in Improving Global Health. In Diagnostic Applications of Health Intelligence and Surveillance Systems; PennsylvaniaIGI Global: Hershey, PA, USA, 2021; pp. 86–105. [Google Scholar]
- Kafaei-Atrian, M.; Sadat, Z.; Nasiri, S.; Izadi-Avanji, F.S. The Effect of Self-care Education Based on Self-efficacy Theory, Individual Empowerment Model, and Their Integration on Quality of Life among Menopausal Women. Int. J. Community Based Nurs. Midwifery 2022, 10, 54. [Google Scholar] [PubMed]
- Yildirim Duman, J.G. Self-management of chronic diseases: A descriptive phenomenological study. Soc. Work. Public Health 2021, 36, 300–310. [Google Scholar] [CrossRef] [PubMed]
- Hariton, E.; Locascio, J.J. Randomised controlled trials—The gold standard for effectiveness research. BJOG Int. J. Obstet. Gynaecol. 2018, 125, 1716. [Google Scholar] [CrossRef] [Green Version]
- Anderson, N.; Sridharan, S.; Megson, M.; Evans, A.; Vallance, J.; Singh, S.; Shukla, R.; Patel, V. Preventing chronic disease in people with mental health problems: The HEALTH Passport approach. Psychiatrist 2012, 36, 208–213. [Google Scholar] [CrossRef]
- Leung, L. Validity, reliability, and generalizability in qualitative research. J. Fam. Med. Prim. Care 2015, 4, 324. [Google Scholar] [CrossRef]
- McKim, C.A. The value of mixed methods research: A mixed methods study. J. Mix. Methods Res. 2017, 11, 202–222. [Google Scholar] [CrossRef] [Green Version]
- Smith, J.; Noble, H. Bias in research. Evid. Based Nurs. 2014, 17, 100–101. [Google Scholar] [CrossRef] [Green Version]
- Choy, L.T. The strengths and weaknesses of research methodology: Comparison and complimentary between qualitative and quantitative approaches. IOSR J. Humanit. Soc. Sci. 2014, 19, 99–104. [Google Scholar] [CrossRef]
- Stoll, K.; Kubendran, S.; Cohen, S.A. The past, present and future of service delivery in genetic counseling: Keeping up in the era of precision medicine. Am. J. Med. Genet. Part C Semin. Med. Genet. 2018, 178, 24–37. [Google Scholar] [CrossRef] [PubMed]
- Bali, A.; Bali, D.; Iyer, N.; Iyer, M. Management of medical records: Facts and figures for surgeons. J. Maxillofac. Oral Surg. 2011, 10, 199–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martel, N.; Franco-Lopez, H.; Snyder, E.; Cheskey, S.; Fruchter, L.; Ahrari, A.; Farren-Dai, L.; Gruner, D.; Pottie, K. The refugee health passport: A portable medical history tool that facilitates communication for newly arrived refugees in interpretation-limited, acute care settings. Ann. Glob. Health 2015, 81, 115. [Google Scholar] [CrossRef]
- Wang, X.; Cheng, Z. Cross-sectional studies: Strengths, weaknesses, and recommendations. Chest 2020, 158, S65–S71. [Google Scholar] [CrossRef]
- Creswell, J.W.; Shope, R.; Plano Clark, V.L.; Green, D.O. How interpretive qualitative research extends mixed methods research. Res. Sch. 2006, 13, 1–11. [Google Scholar]
- Robinson, O.C. Sampling in interview-based qualitative research: A theoretical and practical guide. Qual. Res. Psychol. 2014, 11, 25–41. [Google Scholar] [CrossRef] [Green Version]
- Delgado, G.V.; de Carvalho, R.B.; Choo, C.W.; Leite, R.S.; de Castro, J.M. Patient empowerment through mobile health: Case study with a Brazilian application for pregnancy support. In Proceedings of the Association for Information Science and Technology, Online, 22 October–1 November 2020; Volume 57, p. e221. [Google Scholar]
- Gusenbauer, M.; Haddaway, N.R. Which academic search systems are suitable for systematic reviews or meta-analyses? Evaluating retrieval qualities of Google Scholar, PubMed, and 26 other resources. Res. Synth. Methods 2020, 11, 181–217. [Google Scholar] [CrossRef]
- Shaffril, H.A.M.; Samah, A.A.; Samsuddin, S.F. Guidelines for developing a systematic literature review for studies related to climate change adaptation. Environ. Sci. Pollut. Res. 2021, 28, 22265–22277. [Google Scholar] [CrossRef]

| No | Title | Author | Type of Study | Country | Sample | Type of Sample |
|---|---|---|---|---|---|---|
| 1 | Many Physicians Are Willing to Use Patients’ Electronic Personal Health Records, But Doctors Differ by Location, Gender, And Practice | [28] | Cross sectional | United States | physicians—856 responds | random-sample |
| 2 | Use of patients’ mobile phones to store and share personal health information: results of a questionnaire survey | [29] | A cross-sectional questionnaire survey | Japan | 193 patients | Convenience sampling—consecutive outpatients who visited our weekday clinic between 1 March and 30 May 2012 |
| 3 | The Association of Graph Literacy with Use of and Skills Using an Online Personal Health Record in Outpatient Veterans | [30] | cross-sectional survey | United States | 600 veterans We conducted a cross-sectional survey of veterans receiving outpatient care | conveniently recruited |
| 4 | Dissemination and use of the children’s dental pass in Germany | [31] | Cross sectional self-administered mail questionnaire | Germany | 1086 Dental officers | Convenient |
| 5 | User-centred design and enhancement of an electronic personal health record to support survivors of paediatric cancers | [32] | Focus groups and structured interviews | United States | Paediatric cancer (n = 3), parents (n = 11), and healthcare providers (n = 14) | purposive sampling |
| 6 | The Prescription of Mobile Apps by Primary Care Teams: A Pilot Project in Catalonia | [33] | focus groups | Spain (Catalonia) | 32 doctors and 79 patients per professional | purposive sampling |
| 7 | Patient perspectives on a personally controlled electronic health record used in regional Australia: ‘I can be like my own doctor’ | [34] | semi-structured telephone interviews | Australia | 12 patients | Random All Medenotes registered patients (n = 154) were emailed once and invited to participate in a telephone interview. |
| 8 | Randomized trial of an electronic personal health record for patients with serious mental illnesses | [35] | Randomized trial | United States | 170 individuals | with a serious mental disorder and a comorbid medical condition treated in a community mental health center |
| 9 | Understanding patient perceptions of the electronic personal health record | [36] | qualitative study | United States | 21 adults reporting an average age of about 64 years | purposive sampling—Identified |
| 10 | Design and implementation of a patient passport in a pediatric cardiology clinic | [37] | prospective survey—Qualitative | United States (New York) | 100 patients | A total of 100 patients were enrolled in the study between October 2016 and November 2018. |
| 11 | Moving Beyond the Rhetoric of Shared Decision-Making: Designing Personal Health Record Technology with Young Adults with Type 1 Diabetes | [38] | Cross sectional Mixed method | Canada | 22 participants took part, comprising 7 young adults with T1D and 15 care providers. | The two study groups were patients (young adults with T1D, aged 18–24 years) and healthcare providers of the patient population (specialist dieticians and nurses). |
| 12 | Snap shot: Achieving better care through a one-page personal health profile | [39] | qualitative descriptive approach | Canada | 13 participants. | Participant self-identify as having a child with an ID who required additional support |
| 13 | Barriers and benefits to using mobile health technology after operation: A qualitative study | [40] | Qualitative | New York | 800 participants and 25 individuals | 800 participants from national surveys—randomly 25 individuals—telephones with 2 open ended question by phone. |
| Theme (Benefit) | Sub-Themes | Articles |
|---|---|---|
| Empower patient | Awareness to patient about their health | [29,34,38] |
| Improve health literacy | [32,35] | |
| Empower patient to selfcare | [28,34] | |
| Improve knowledge | [32,36,37,38,39,40] | |
| Help in Communication | Improve doctor—patient Communication | [33,34,37,39,40] |
| Improve Communication among providers | [31,34,37,39] | |
| Improve consultation behaviour of parent/patient | [31,39] | |
| Receive alert notification from provider | [30,33] | |
| Improve Relationship | Improve Dr-Patient relationship | [28,33,39,40] |
| Improve quality of care | Improve quality of care | [28,34,35,39,40] |
| Support patient management | [36,38,39] | |
| Support Decision making during consultation | [33,34,38,39], | |
| Improve type of treatment with prevention | [31,35,40] | |
| Patient monitoring | [40] | |
| Improve Health status | [34,35,40] | |
| Improve oral health status | [31] | |
| Improve children behaviour | [31,39] | |
| Continuity of care | [37,39] | |
| Maintain Health Records | Patient own medical records | [39] |
| Improve record documentation | [28] | |
| Improve records accuracy | [28] | |
| Document health state | [31] | |
| Accessing health records | [30,33,38,39] | |
| Records sharing | Sharing Health record with providers | [29,32,33,34,36,37] |
| Sharing health record with family | [29,39] | |
| Time saving | Save time to see doctor | [28,40] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tuan Soh, T.Y.; Nik Mohd Rosdy, N.M.M.; Mohd Yusof, M.Y.P.; Azhar Hilmy, S.H.; Md Sabri, B.A. Adoption of a Digital Patient Health Passport as Part of a Primary Healthcare Service Delivery: Systematic Review. J. Pers. Med. 2022, 12, 1814. https://doi.org/10.3390/jpm12111814
Tuan Soh TY, Nik Mohd Rosdy NMM, Mohd Yusof MYP, Azhar Hilmy SH, Md Sabri BA. Adoption of a Digital Patient Health Passport as Part of a Primary Healthcare Service Delivery: Systematic Review. Journal of Personalized Medicine. 2022; 12(11):1814. https://doi.org/10.3390/jpm12111814
Chicago/Turabian StyleTuan Soh, Tuan Yuswana, Nik Mohd Mazuan Nik Mohd Rosdy, Mohd Yusmiaidil Putera Mohd Yusof, Syathirah Hanim Azhar Hilmy, and Budi Aslinie Md Sabri. 2022. "Adoption of a Digital Patient Health Passport as Part of a Primary Healthcare Service Delivery: Systematic Review" Journal of Personalized Medicine 12, no. 11: 1814. https://doi.org/10.3390/jpm12111814