
Local Infiltrations in Patients with Radiculopathy or Chronic Low Back Pain Due to Segment Degeneration—Only A Diagnostic Value?
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Ethical Approval
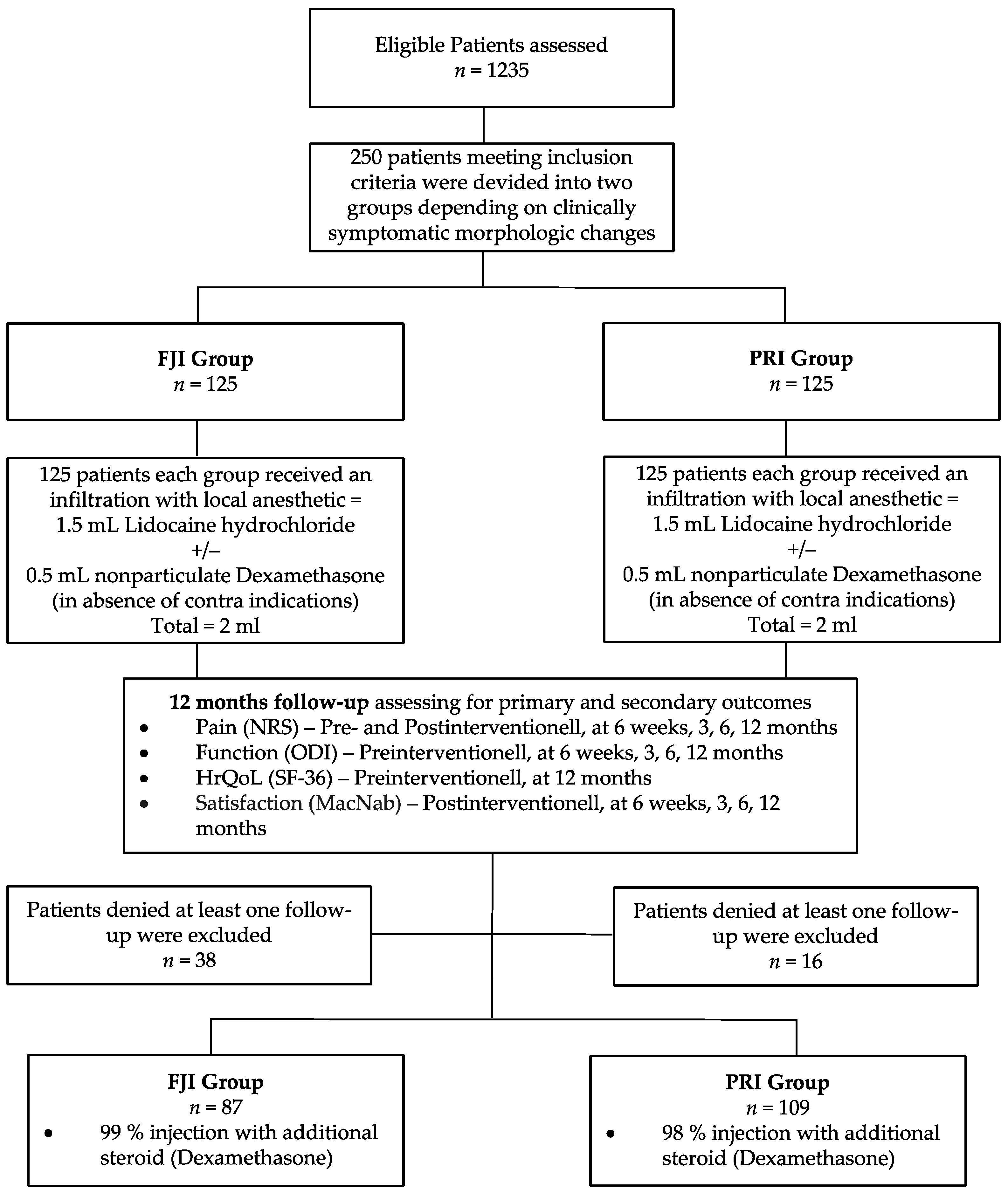
2.3. Patients and Groups
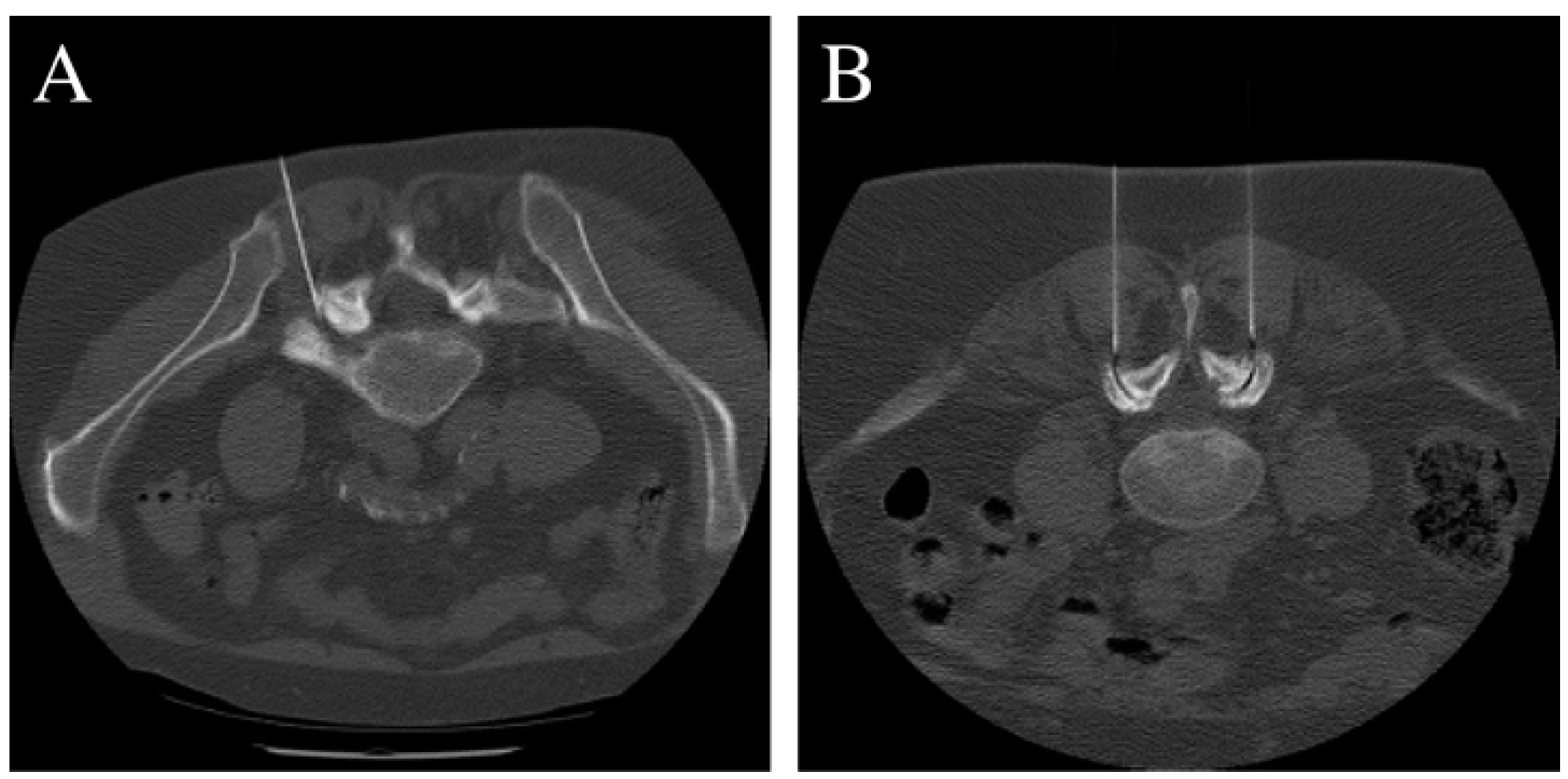
2.4. Intervention
2.5. Epidemiological and Clinical Data
2.6. Analysis of the Therapeutic Value
2.7. Statistics
3. Results
3.1. Baseline Demographics
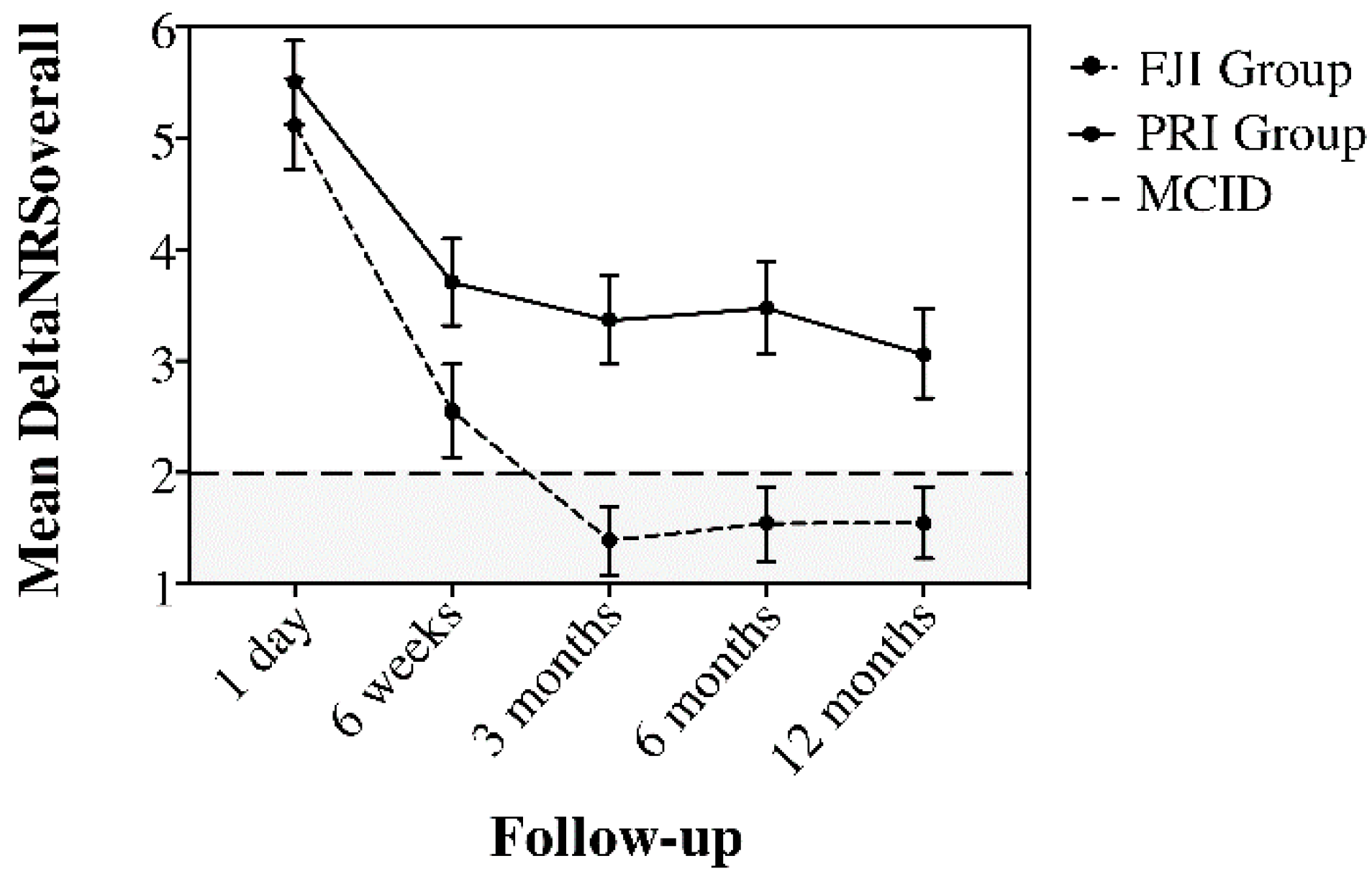
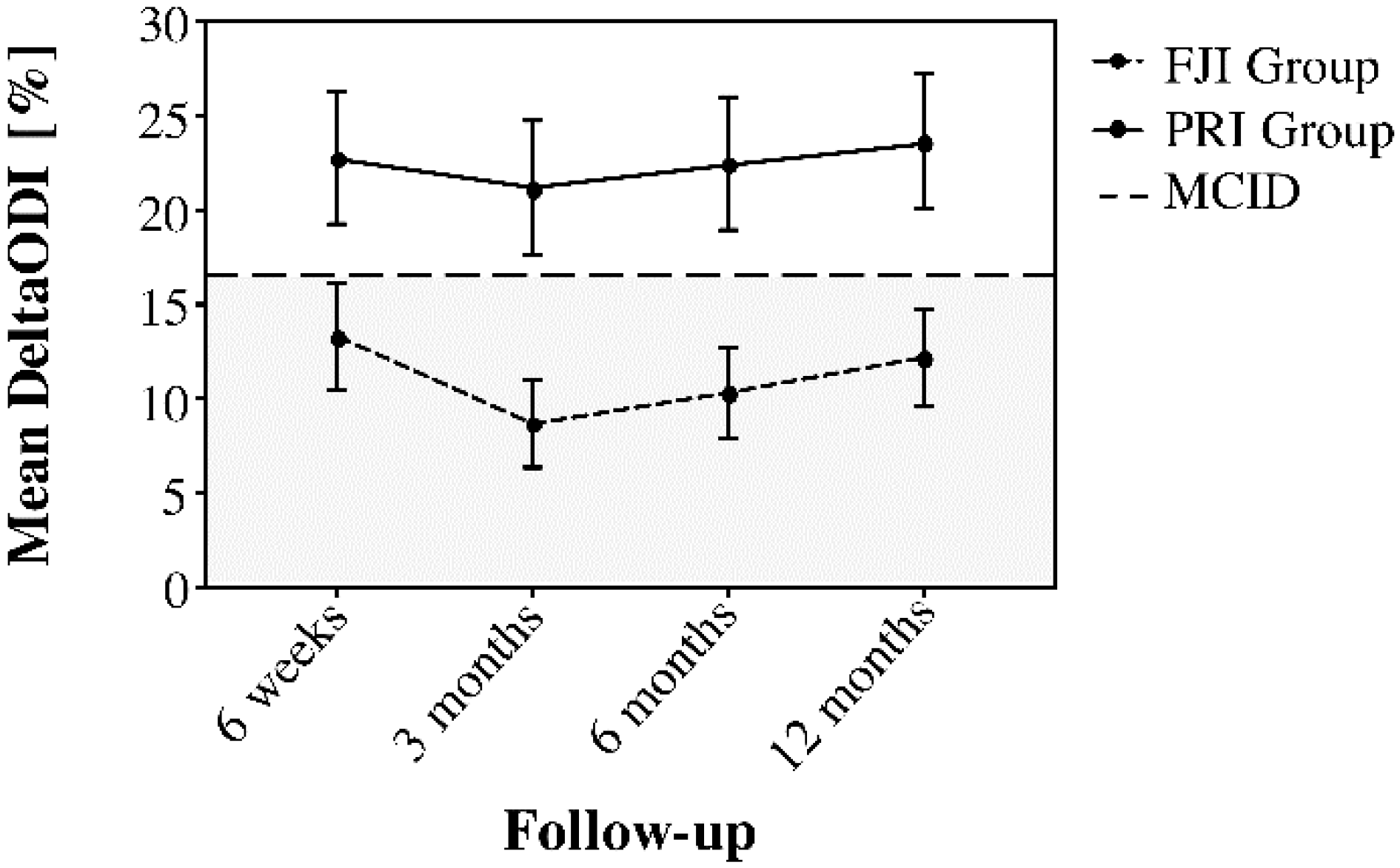
3.2. Results of Pain and Functional Improvement
3.3. Results Regarding the Therapeutic Value
3.4. Health-Related Quality of Life and Patient Satisfaction
3.5. Adverse Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bachmann, S.; Oesch, P.; Knusel, O.; De Bie, R.; Van den Brandt, P.; Kool, J. Costs of long term disability in patients with non-specific low back pain; A randomized study. Ann. Rheum. Dis. 2006, 65, 609. [Google Scholar]
- Manchikanti, L.; Boswell, M.V.; Singh, V.; Benyamin, R.M.; Fellows, B.; Abdi, S.; Buenaventura, R.M.; Conn, A.; Datta, S.; Derby, R.; et al. Comprehensive Evidence-Based Guidelines for Interventional Techniques in the Management of Chronic Spinal Pain. Pain Physician 2009, 12, 699–802. [Google Scholar] [CrossRef] [PubMed]
- Martin, B.I.; Deyo, R.A.; Mirza, S.K.; Turner, J.A.; Comstock, B.A.; Hollingworth, W.; Sullivan, S.D. Expenditures and health status among adults with back and neck problems. JAMA 2008, 299, 656–664. [Google Scholar] [CrossRef] [Green Version]
- Heliovaara, M.; Sievers, K.; Impivaara, O.; Maatela, J.; Knekt, P.; Makela, M.; Aromaa, A. Descriptive epidemiology and public-health aspects of low-back pain. Ann. Med. 1989, 21, 327–333. [Google Scholar] [CrossRef]
- Lamers, L.M.; Meerding, W.J.; Severens, J.L.; Brouwer, W.B.F. The relationship between productivity and health-related quality of life: An empirical exploration in persons with low back pain. Qual. Life Res. 2005, 14, 805–813. [Google Scholar] [CrossRef]
- Benny, B.; Azari, P. The efficacy of lumbosacral transforaminal epidural steroid injections: A comprehensive literature review. J. Back Musculoskelet. Rehabil. 2011, 24, 67–76. [Google Scholar] [CrossRef] [PubMed]
- Falco, F.J.E.; Manchikanti, L.; Datta, S.; Sehgal, N.; Geffert, S.; Onyewu, O.; Singh, V.; Bryce, D.A.; Benyamin, R.M.; Simopoulos, T.T.; et al. An Update of the Systematic Assessment of the Diagnostic Accuracy of Lumbar Facet Joint Nerve Blocks. Pain Physician 2012, 15, E869–E907. [Google Scholar] [CrossRef]
- Johansson, A.; Hao, J.; Sjolund, B. Local corticosteroid application blocks transmission in normal nociceptive c-fibers. Acta Anaesthesiol. Scand. 1990, 34, 335–338. [Google Scholar] [CrossRef]
- Filippiadis, D.K.; Kelekis, A. A review of percutaneous techniques for low back pain and neuralgia: Current trends in epidural infiltrations, intervertebral disk and facet joint therapies. Br. J. Radiol. 2016, 89, 10. [Google Scholar] [CrossRef] [Green Version]
- Kelekis, A.D.; Somon, T.; Yilmaz, H.; Bize, P.; Brountzos, E.N.; Lovblad, K.; Ruefenacht, D.; Martin, J.B. Interventional spine procedures. Eur. J. Radiol. 2005, 55, 362–383. [Google Scholar] [CrossRef]
- Lee, K.S.; Lin, C.L.; Hwang, S.L.; Howng, S.L.; Wang, C.K. Transforaminal periradicular infiltration guided by CT for unilateral sciatica—an outcome study. Clin. Imaging 2005, 29, 211–214. [Google Scholar] [CrossRef] [PubMed]
- Santiago, F.R.; Kelekis, A.; Alvarez, L.G.; Filippiadis, D.K. Interventional Procedures of the Spine. Semin. Musculoskelet. Radiol. 2014, 18, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Leonardi, M.; Pfirrmann, C.W.; Boos, N. Injection studies in spinal disorders. Clin. Orthop. Rel. Res. 2006, 443, 168–182. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, A.; Tamai, K.; Yamato, M.; An, H.S.; Yoshida, H.; Saotome, K.; Kurihashi, A. The relationship between facet joint osteoarthritis and disc degeneration of the lumbar spine: An MRI study. Eur. Spine J. 1999, 8, 396–401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fairbank, J.C. Why are there different versions of the Oswestry Disability Index? J. Neurosurg. Spine 2014, 20, 83–86. [Google Scholar] [CrossRef] [Green Version]
- Stewart, A.L.; Greenfield, S.; Hays, R.D.; Wells, K.; Rogers, W.H.; Berry, S.D.; McGlynn, E.A.; Ware, J.E., Jr. Functional status and well-being of patients with chronic conditions. Results from the Medical Outcomes Study. JAMA 1989, 262, 907–913. [Google Scholar] [CrossRef]
- Stewart, A.L.; Hays, R.D.; Ware, J.E., Jr. The MOS short-form general health survey. Reliability and validity in a patient population. Med. Care 1988, 26, 724–735. [Google Scholar] [CrossRef]
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef]
- Macnab, I. Negative disc exploration. An analysis of the causes of nerve-root involvement in sixty-eight patients. JBJS 1971, 53, 891–903. [Google Scholar] [CrossRef]
- Hagg, O.; Fritzell, P.; Nordwall, A.; Swedish Lumbar Spine Study, G. The clinical importance of changes in outcome scores after treatment for chronic low back pain. Eur. Spine J. 2003, 12, 12–20. [Google Scholar] [CrossRef]
- Farrar, J.T.; Young, J.P., Jr.; LaMoreaux, L.; Werth, J.L.; Poole, R.M. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain 2001, 94, 149–158. [Google Scholar] [CrossRef]
- Suarez-Almazor, M.E.; Kendall, C.; Johnson, J.A.; Skeith, K.; Vincent, D. Use of health status measures in patients with low back pain in clinical settings. Comparison of specific, generic and preference-based instruments. Rheumatology 2000, 39, 783–790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, S.J.; Taylor, A.E.; Foy, M.A.; Fogg, A.J. Responsiveness of common outcome measures for patients with low back pain. Spine 1999, 24, 1805–1812. [Google Scholar] [CrossRef] [PubMed]
- Hepper, C.T.; Halvorson, J.J.; Duncan, S.T.; Gregory, A.J.; Dunn, W.R.; Spindler, K.P. The efficacy and duration of intra-articular corticosteroid injection for knee osteoarthritis: A systematic review of level I studies. J. Am. Acad. Orthop. Surg. 2009, 17, 638–646. [Google Scholar] [CrossRef] [Green Version]
- McCabe, P.S.; Maricar, N.; Parkes, M.J.; Felson, D.T.; O’Neill, T.W. The efficacy of intra-articular steroids in hip osteoarthritis: A systematic review. Osteoarthr. Cartil. 2016, 24, 1509–1517. [Google Scholar] [CrossRef] [Green Version]
- Dietrich, C.L.; Smith, C.E. Epidural granuloma and intracranial hypotension resulting from cervical epidural steroid injection. Anesthesiology 2004, 100, 445–447. [Google Scholar] [CrossRef]
- Manchikanti, L. Role of neuraxial steroids in interventional pain management. Pain Physician 2002, 5, 182–199. [Google Scholar] [CrossRef]
- Kim, N.R.; Lee, J.W.; Jun, S.R.; Lee, I.J.; Lim, S.D.; Yeom, J.S.; Koo, K.H.; Jin, W.; Kang, H.S. Effects of epidural TNF-alpha inhibitor injection: Analysis of the pathological changes in a rat model of chronic compression of the dorsal root ganglion. Skeletal Radiol. 2012, 41, 539–545. [Google Scholar] [CrossRef]
- Benoist, M. The natural history of lumbar disc herniation and radiculopathy. Joint Bone Spine 2002, 69, 155–160. [Google Scholar] [CrossRef]
- Delgado-Lopez, P.D.; Rodriguez-Salazar, A.; Martin-Alonso, J.; Martin-Velasco, V. Lumbar disc herniation: Natural history, role of physical examination, timing of surgery, treatment options and conflicts of interests. Neurocirugia 2017, 28, 124–134. [Google Scholar] [CrossRef]
- Ribeiro, L.H.; Furtado, R.N.; Konai, M.S.; Andreo, A.B.; Rosenfeld, A.; Natour, J. Effect of facet joint injection versus systemic steroids in low back pain: A randomized controlled trial. Spine 2013, 38, 1995–2002. [Google Scholar] [CrossRef] [PubMed]
- Schulte, T.L.; Pietila, T.A.; Heidenreich, J.; Brock, M.; Stendel, R. Injection therapy of lumbar facet syndrome: A prospective study. Acta Neurochir. 2006, 148, 1165–1172; discussion 1172. [Google Scholar] [CrossRef] [PubMed]
- Lilius, G.; Laasonen, E.M.; Myllynen, P.; Harilainen, A.; Gronlund, G. Lumbar facet joint syndrome. A randomised clinical trial. J. Bone Joint Surg. Br. 1989, 71, 681–684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carette, S.; Marcoux, S.; Truchon, R.; Grondin, C.; Gagnon, J.; Allard, Y.; Latulippe, M. A controlled trial of corticosteroid injections into facet joints for chronic low back pain. N. Engl. J. Med. 1991, 325, 1002–1007. [Google Scholar] [CrossRef]
- Kawu, A.A.; Olawepo, A.; Salami, A.O. Facet joints infiltration: A viable alternative treatment to physiotherapy in patients with low back pain due to facet joint arthropathy. Niger J. Clin. Pract. 2011, 14, 219–222. [Google Scholar] [CrossRef] [Green Version]
- Cohen, S.P.; Raja, S.N. Pathogenesis, diagnosis, and treatment of lumbar zygapophysial (facet) joint pain. Anesthesiology 2007, 106, 591–614. [Google Scholar] [CrossRef]
- Fairbank, J.C.; Park, W.M.; McCall, I.W.; O’Brien, J.P. Apophyseal injection of local anesthetic as a diagnostic aid in primary low-back pain syndromes. Spine 1981, 6, 598–605. [Google Scholar] [CrossRef]
- Karppinen, J.; Malmivaara, A.; Kurunlahti, M.; Kyllonen, E.; Pienimaki, T.; Nieminen, P.; Ohinmaa, A.; Tervonen, O.; Vanharanta, H. Periradicular infiltration for sciatica: A randomized controlled trial. Spine 2001, 26, 1059–1067. [Google Scholar] [CrossRef]
- Riew, K.D.; Yin, Y.; Gilula, L.; Bridwell, K.H.; Lenke, L.G.; Lauryssen, C.; Goette, K. The effect of nerve-root injections on the need for operative treatment of lumbar radicular pain. A prospective, randomized, controlled, double-blind study. J. Bone Joint. Surg. Am. 2000, 82, 1589–1593. [Google Scholar] [CrossRef]
- Celik, B.; Er, U.; Simsek, S.; Altug, T.; Bavbek, M. Effectiveness of lumbar zygapophysial joint blockage for low back pain. Turk. Neurosurg. 2011, 21, 467–470. [Google Scholar] [CrossRef]
- Buenaventura, R.M.; Datta, S.; Abdi, S.; Smith, H.S. Systematic review of therapeutic lumbar transforaminal epidural steroid injections. Pain Physician 2009, 12, 233–251. [Google Scholar] [CrossRef] [PubMed]
- Carette, S.; Leclaire, R.; Marcoux, S.; Morin, F.; Blaise, G.A.; St-Pierre, A.; Truchon, R.; Parent, F.; Levesque, J.; Bergeron, V.; et al. Epidural corticosteroid injections for sciatica due to herniated nucleus pulposus. N. Engl. J. Med. 1997, 336, 1634–1640. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups (n = 196) | FJI Group (n = 87) | PRI Group (n = 109) | p Value | |
|---|---|---|---|---|
| Gender | Men | 38% (33) | 44% (48) | 0.388 * |
| Woman | 62% (54) | 56% (61) | ||
| Age [yrs] | Mean ± SD | 66.2 ± 12.5 | 64.2 ± 11.6 | 0.248 † |
| Weight [kg] | Mean ± SD | 83.3 ± 16.7 | 83.5 ± 15.9 | 0.935 † |
| Height [m] | Mean ± SD | 1.7 ± 0.1 | 1.7 ± 0.1 | 0.254 † |
| BMI [kg/m2] | Mean ± SD | 28.8 ± 6.0 | 28.7 ± 5.1 | 0.883 † |
| Numeric rating scale (0–10) ‡ | Mean ± SD | 6.9 ± 1.2 | 7.1 ± 1.3 | 0.402 † |
| Oswestry Disability Index [%] (0–100) | Mean ± SD | 44.4 ± 13.2 | 47.3 ± 17.0 | 0.177 † |
| Grading of facet joint arthritis | Grade 3 | n.a. | ||
| (Fujiwara) | Grade 4 | |||
| Grading of nerve root compression | Moderate | 55% (48) | 56% (61) | n.a. |
| Severe | 45% (39) | 44% (48) |
| Time | Numeric Pain Rating Scale | Oswestry Disability Index | ||
|---|---|---|---|---|
| FJI Group (87) | PRI Group (109) | FJI Group (87) | PRI Group (109) | |
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | |
| Baseline | 6.9 ± 1.2 | 7.1 ± 1.3 | 44.4 ± 13.2 | 47.3 ± 17.0 |
| After intervention | 1.8 * ± 1.8 | 1.6 * ± 1.7 | - | - |
| 6 weeks † | 4.4 * ± 2.1 | 3.4 * ± 1.9 | 31.7 * ± 14.5 | 25.8 * ± 15.1 |
| 3 months † | 5.6 * ± 1.6 | 3.8 * ± 2.1 | 37.1 * ± 11.9 | 26.6 * ± 14.9 |
| 6 months † | 5.6 * ± 1.7 | 3.7 * ± 2.2 | 35.8 * ± 12.1 | 25.8 * ± 15.0 |
| 12 months † | 6.2 * ± 1.8 | 4.4 * ± 2.5 | 37.8 * ± 13.4 | 25.6 * ± 15.1 |
| ptreatment | <0.001 | <0.001 | ||
| ptime | <0.001 | <0.001 | ||
| ptreatment × time | <0.001 | <0.001 | ||
| Time | Numeric Pain Rating Scale (Back) | Numeric Pain Rating Scale (Leg) | ||
|---|---|---|---|---|
| FJI Group (87) | PRI Group (109) | FJI Group (87) | PRI Group (109) | |
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | |
| Baseline †‡ | 6.9 ± 1.7 | 5.7 ± 1.7 | 4.2 ± 2.8 | 7.2 ± 1.7 |
| After intervention † | 2.4 * ± 1.6 | 1.3 * ± 1.4 | 1.2 * ± 1.7 | 1.8 * ± 1.4 |
| 6 weeks †‡ | 4.6 * ± 2.3 | 2.6 * ± 2.1 | 2.6 * ± 2.5 | 3.5 * ± 2.3 |
| 3 months † | 5.7 * ± 1.9 | 2.9 * ± 2.3 | 3.4 * ± 2.5 | 3.9 * ± 2.6 |
| 6 months † | 5.7 * ± 2.0 | 2.8 * ± 2.4 | 3.4 * ± 2.5 | 3.6 * ± 2.6 |
| 12 months † | 6.0 * ± 1.9 | 3.6 * ± 2.6 | 4.5 ± 2.5 | 4.0 * ± 2.9 |
| ptreatment | <0.001 | 0.009 | ||
| ptime | <0.001 | <0.001 | ||
| ptreatment × time | <0.001 | <0.001 | ||
| Time | FJI Group (87) | PRI Group (109) | |
|---|---|---|---|
| Mean ± SD | Mean ± SD | p-Value † | |
| SF 36 (pcs) | |||
| Baseline | 31.1 ± 6.5 | 32.6 ± 7.4 | 0.120 |
| 12 months | 30.3 ± 9.4 * | 35.6 ± 7.2 * | <0.001 |
| SF 36 (mcs) | |||
| Baseline | 44.5 ± 8.3 | 47.8 ± 10.0 | 0.010 |
| 12 months | 43.3 ± 9.0 * | 48.3 ± 10.5 | 0.018 |
| FJI Group (87) | PRI Group (109) | |||
|---|---|---|---|---|
| Time | MacNab | Patients Treated | Patients Treated | p-Value |
| n (%) | n (%) | |||
| After intervention | Poor | 3 (3) | 0 (0) | 0.007 * |
| Fair | 11 (13) | 9 (8) | ||
| Good | 42 (48) | 37 (34) | ||
| Excellent | 31 (36) | 63 (58) | ||
| 6 weeks | Poor | 11 (13) | 2 (2) | <0.001 * |
| Fair | 34 (39) | 28 (26) | ||
| Good | 29 (33) | 39 (36) | ||
| Excellent | 13 (15) | 40 (37) | ||
| 3 months | Poor | 22 (25) | 9 (8) | <0.001 * |
| Fair | 41 (47) | 40 (37) | ||
| Good | 12 (14) | 32 (29) | ||
| Excellent | 11 (13) | 28 (26) | ||
| 6 months | Poor | 35 (40) | 22 (20) | <0.001 * |
| Fair | 40 (46) | 29 (27) | ||
| Good | 8 (9) | 31 (28) | ||
| Excellent | 4 (5) | 27 (25) | ||
| 12 months | Poor | 26 (30) | 10 (9) | <0.001 * |
| Fair | 38 (44) | 44 (40) | ||
| Good | 15 (17) | 28 (26) | ||
| Excellent | 8 (9) | 27 (25) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lindemann, C.; Zippelius, T.; Hochberger, F.; Hölzl, A.; Böhle, S.; Strube, P. Local Infiltrations in Patients with Radiculopathy or Chronic Low Back Pain Due to Segment Degeneration—Only A Diagnostic Value? J. Pers. Med. 2022, 12, 1791. https://doi.org/10.3390/jpm12111791
Lindemann C, Zippelius T, Hochberger F, Hölzl A, Böhle S, Strube P. Local Infiltrations in Patients with Radiculopathy or Chronic Low Back Pain Due to Segment Degeneration—Only A Diagnostic Value? Journal of Personalized Medicine. 2022; 12(11):1791. https://doi.org/10.3390/jpm12111791
Chicago/Turabian StyleLindemann, Chris, Timo Zippelius, Felix Hochberger, Alexander Hölzl, Sabrina Böhle, and Patrick Strube. 2022. "Local Infiltrations in Patients with Radiculopathy or Chronic Low Back Pain Due to Segment Degeneration—Only A Diagnostic Value?" Journal of Personalized Medicine 12, no. 11: 1791. https://doi.org/10.3390/jpm12111791