1. Introduction
Wound healing requires a chronological sequence of complex biological processes [
1]. All tissues in the body essentially follow the same pattern to promote healing, with a focus on quick recovery [
2]. Nevertheless, these processes are dependent on intact hemostatic and inflammatory mechanisms that are widely influenced by genetic and environmental factors, especially in cases of wound healing that concern the oral cavity, which is characterized by a remarkably hostile environment based on its resident microbiome [
3].
Following oral surgery or tooth extraction, a sequence of healing processes are immediately initiated. The periodontal pocket is blocked by blood coagulation [
4], and a re-epithelization mechanism is initiated, followed by granulation tissue generation [
5]. After one week of tissue remodeling, bones replenishment occurs, and cavity closure is completed within a period of eight weeks after tooth extraction [
6,
7].
Notably, several factors interfere with healthy oral healing processes, including the tooth location, smoking, and mouth care attitudes [
8,
9]. Therefore, effective oral care and hygiene are crucial after surgery to minimize pain, inflammation, and dental plaque formation [
10]. Nevertheless, it can be a challenge for patients to maintain sufficiently high hygiene [
11]. Thus, efficient would healing detergents are necessary to sustain and accelerate recovery after oral surgery.
Nonprescription dental hygiene products are available and are normally sufficient for preventing common oral health problems. Chlorhexidine (CHX) is the most common antiplaque and antigingivitis agent [
12]. CHX is a cationic bisbiguanide compound with broad-spectrum antimicrobial properties. It binds to the microbe cell and precipitates the cell contents [
13,
14,
15]. CHX-gluconate is widely used in dentistry and is available as an oral rinse, gel, spray, and dental varnish. In their recent review article, Rajendiran et al. have summarized the current developments in antiplaque, antigingivitis, and antiperiodontitis properties of CHX and other compounds [
16].
Bone bioactive liquid (BBL) is a saline solution containing calcium chloride (CaCl
2) and magnesium dichloride hexahydrate (MgCl
2-6H
2O) with a net negative charge that promotes healing and soft and hard tissue regeneration in the wounded periodontal cavity [
17]. Furthermore, BBL significantly intensifies the concentration of hydroxyl groups at the wound surface and significantly improves hydration in comparison with other mouthwashes (unpublished data). BBL creates a hydrophilic environment that allows active ionic interactions with blood plasma, progenitor endothelial, and epithelial cells and, consequently, the coordination and communication between cells are significantly improved at the wound site [
17].
The aim of the present study is to compare the efficacy of BBL and CHX (0.12%) mouthwashes in improving clinical parameters and soft tissue healing after tooth extraction. The wound healing properties of BBL may support its usage as a new pharmaceutical product with good physical, chemical, and biological stabilities.
2. Materials and Methods
2.1. Study Population: Inclusion and Exclusion Criteria
The study cohort comprised 81 patients of male and female genders aged above 14 years old who had agreed to voluntarily participate in the clinical trial. The sociodemographic characteristics of the patient cohort are described in
Supplementary Table S1. Written informed consent was obtained from all study participants following the ethical guidelines of the Declaration of Helsinki and approved by the ethics committee at Complejo Hospitalario de Toledo and institutional review board, Spain (CEIm HM Hospitales 21.03.1786-GHM; protocol ID: V01-2021; date: 16 April 2021; Clinical Trial Registry Platform: Clinical Trial Gov. Press). Participant inclusion criteria included the following: systemically healthy, full mouth plaque and bleeding scores < 20%, healthy periodontium, and no local or systemic antibiotic or antiseptic treatments for 3 months prior to involvement in the study. Exclusion criteria included the use of medications that cause gingival enlargement or the presence of gingival idiopathic overgrowth; smokers; patients with systemic diseases or conditions that could interfere with routine periodontal therapy such as pregnancy or lactating females, uncontrolled periodontal disease, previous or current history of bisphosphonate treatment, immune deficiencies, uncontrolled diabetes, rheumatoid disease, radiotherapy, chemotherapy, infectious diseases.
2.2. Removal of Patients from Therapy or Assessment
Participants were free to withdraw from the study at any time, without any prejudice or justifications. If the patient prematurely discontinued the study, any relevant evaluations and observations and reasons for study discontinuation were recorded in the case report form (CRF). Participants discontinuing due to infection or medical reasons were monitored until complete recovery.
2.3. Study Design
The study was designed as a one-week randomized, prospective, double blind pilot clinical trial. This prospective study included patients who required two trans alveolar surgical extractions of inferior or superior third molar or any simple or surgical tooth extraction. The 171 dental extractions in 81 patients were randomly assigned to two groups: the control group (CG, 20 male and 22 female patients) received Perio-Aid Intensive Care mouthwash containing 0.12% CHX-di-gluconate (Dentaid, Barcelona, Spain); and the test group (TG, 19 male and 20 female patients) received BBL mouthwash, a bioactive solution generated in our laboratory, which is phosphate-buffered saline (PBS) solution containing 1.35 mM CaCl
2 and 0.75 mM MgCl
2-6H
2O with a net negative charge. Mouthwashes were administered twice a day for 7 days, and no eating or drinking was permitted for a period of 1 h after the treatment. After a period of 7 days, clinical parameter data were analyzed to determine clinical changes during the treatment. Patient follow-ups were conducted twice via phone calls at days 2 and 4 to determine the degree of postoperative pain as described in
Table 1. To respect patient data confidentiality, the data management system described in [
18] was applied.
2.4. Surgery Assessments
Three independent dentists participated in clinical data measurements and registrations. The study participants received a diagnostic workup including clinical examinations, oral photographs, and standardized periapical radiographs to evaluate the proposed surgical sites. Before the surgical procedure, patients underwent periodontal therapy and received extensive oral hygiene instructions for providing an improved oral environment. The protocols for full mouth plaque scores (FMPS) and full mouth bleeding scores (FMBS) were implemented exactly as described by T.J. O’Leary et al. [
19] and J. Ainamo et al. [
20], respectively, and were recorded after the hygienic phase of the periodontal therapy. No surgery was performed until patients reached FMPS < 20% and FMBS < 20%. Each patient received surgery on either of the two bilateral areas on different days. The surgical extractions of tooth were carried out with local anesthetic, raising a mucoperiosteal flap with osteotomy, and no periodontal dressing was applied postoperatively. Unless otherwise required, dental extractions were performed without stitches in both control and test groups to evaluate the healing capacity of both mouthwashes.
2.5. Post-Surgical Procedures
All the patients received 600 mg ibuprofen every 8 h for 4 days and either 500 mg amoxicillin every 8 h for 7 days or 100 mg doxycycline every 24 h for 5 days for patients allergic to amoxicillin. Patients were instructed to rinse with 15 mL mouthwash twice a day after their regular homecare practice for a period of 7 days. The use of ice packs was recommended for at least 3 h post-surgery. All the patients were instructed to discontinue tooth brushing at the surgical sites for 7 days. After 30 days, a professional prophylaxis was performed to remove stains caused by Perio-Aid Intensive Care mouthwash.
2.6. Wound Healing Measurement Procedures
After a period of 7 days, patients were examined for evaluation of healing. The early wound healing index (EHI) [
21] scores were determined by two blinded clinical examiners. The scale was applied with five different degrees, and scores 5 to 1 were applied based on the respective observations: complete flap closure without fibrin line; complete flap closure with fibrin line; complete flap closure with small fibrin clot(s); incomplete flap closure with partial necrosis; and incomplete flap closure with complete necrosis (more than 50% of the former flap is involved). In addition, EHI was assessed using the healing index of Landry et al. [
22], in which wounds were graded on a scale of 1–5 as described in
Supplementary Table S2. The wound area was classified as either partially or fully keratinized. In the case of partial keratinization, the wound area was further classified as partially or fully keratinized upon examination after an additional 7 days.
2.7. Procedures for Measurement of Post-Surgical Pain, Safety, and Discomfort
Efficacy measurements were assessed by pain scale evaluation post-surgery at days 2, 4, and 7 though a phone call with the patients in accordance with their subjective pain feeling. A modified visual analog scale (VAS) was applied as described in [
23]. No pain was scored as 0, moderate pain scale as 5, and maximum pain as 10. Furthermore, safety measurements were evaluated by the incidence of adverse events (AEs) and serious adverse events (SAEs) that could be detected by the investigator or communicated by the patient throughout the entire study.
2.8. Statistical and Analytical Methods
Shapiro–Wilk normality testing was performed to assess the normality of data distribution. Data are reported as mean and standard deviation or median and interquartile range (IQR) based on data distribution. Differences between treatments and gender were assessed using Mann–Whitney test or t-test based on data distribution. A two-tailed test with a p-value < 0.05 was considered the cut-off level for indicating statistical significance. Statistical Package for Social Sciences software (IBM SPSS, version 23, Chicago, IL, USA) was used for data analysis.
3. Results
In this study, no incidences of adverse events were observed, and no postoperative compilations were reported. Patients did not present statistically significant differences in terms of infection prevention between the CG and TG (p = 0.96).
3.1. BBL Mouthwash Dramatically Reduces VAS
In general, patients from both treatment groups showed a progressive decrease in pain over the consecutive week post-surgery (
Figure 1A). Nevertheless, statistical data analysis revealed that the CHX group showed a significant reduction in VAS only at day 7 (
p < 1 × 10
−5). Alternatively, the BBL group demonstrated a significant reduction in VAS starting on day 4 (
p < 1 × 10
−4) and was further reduced at day 7 (
p < 1 × 10
−8,
Figure 1A).
VAS at day 2 was lower in the BBL group than in the CHX group, though not significantly (
p = 0.084). However, significant differences in VAS scores were observed at days 4 and 7, with notable 50–70% lower values scored in the BBL group compared with the CHX group (
Figure 1A).
Since the study compromises patients from two different genders, we were interested to evaluate the VAS in each separately. VAS was comparable between males and females and no significant differences were recorded (
p = 0.78). The time course study indicated that the VAS had an identical trend in both genders, with a significant reduction starting at day 4 for the BBL group and starting at day 7 for the CHX group (
Figure 1B,C).
3.2. BBL Mouthwash Improves EHI
The total extracted teeth were 89 and 82 for the BBL and CHX groups, respectively. As observed in
Figure 2, both CHX and BBL treatments improved oral wound healing at day 7 post-surgery, independent of the number of extracted teeth. Nevertheless, wound closure was notably enhanced in response to BBL treatment.
Table 2 shows the EHI scores based on the Landry et al. [
22] classification for a total of 171 dental extracts performed in the patients cohort. In general, and independent of the position of dental extraction, the EHI scores were remarkably higher after BBL treatment than after CHX treatment. Taken together, these results indicate that BBL treatment enhances gingival tissue healing.
We then evaluated the EHI scores for both treatments. Data analysis revealed a statistically significant differences in EHI scores between the two treatments. The average of the total EHI score was 4.40 ± 0.56 for the BBL group and 3.1 ± 0.57 for the CHX group, indicating the remarkable healing process occurring in the BBL group.
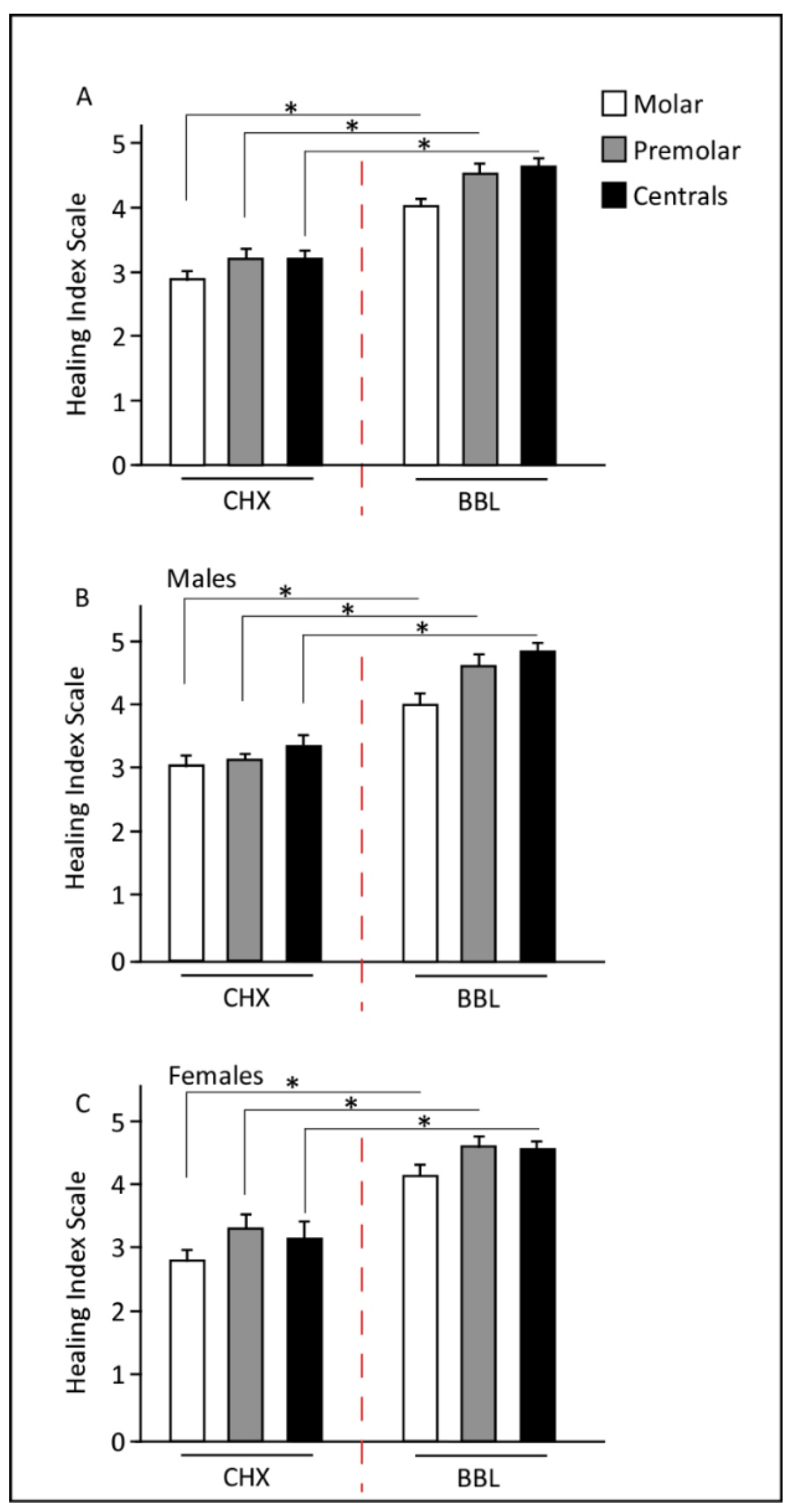
Since the tooth location influences the EHI score, we classified the extracted teeth into premolars, centrals, and molars and accordingly determined the EHI scores. As shown in
Figure 3A, the EHI score for each tooth segment was significantly higher in the BBL group compared with the CHX group. In the comparisons between tooth segments, molars had the lowest EHI scores, indicating a delayed healing process relative to the other tooth locations (
Figure 3A).
No significant differences in EHI scores were detected between genders (
p = 0.645). Both males and females showed identical patterns with respect to the tooth location segments, where a significant improvement in EHI score was observed in the BBL group relative to that of the CHX group (
Figure 3B,C).
4. Discussion
In our previous preclinical study, we applied pretreated bone level tapered (BLT) titanium implants in foxhound dogs with BBL. The data indicated that BBL improves the histological and histomorphometric characteristics of the implants, reduces titanium surface roughness, improves wettability, and promotes healing and soft and hard tissue regeneration at the implant site [
17]. In the current study, BBL was applied as a mouthwash to human patients who had teeth extraction surgeries, and its prospective clinical properties were compared to that of CHX mouthwash. Overall, the human data support the previous findings of the animal study and indicate significant improvements in wound healing and soft tissue regeneration from BBL. Notably, the study patient cohort consisted of a heterogenous population with different sociodemographic backgrounds that were randomly distributed in this double blinded study.
CHX is a gold standard mouthwash with antiplaque and antigingivitis properties [
24,
25]. Nevertheless, it has negative side effects that preclude long-term use and result in poor patient compliance [
25]. The adverse effects of CHX include burning sensation, tartar and calculus formation, soft tissue trauma and allergy, taste alteration, and teeth staining [
26,
27,
28,
29]. Therefore, studies have been directed toward the use of different of CHX concentrations and/or alternative product usage. Several studies compared the use of different CHX concentrations, which are thoroughly reviewed in [
29,
30,
31]. In general, studies indicate that there are no statistically significant differences in the efficacy of 0.12% and 0.2% CHX mouthwashes, and that concentrations above 0.2% will unnecessarily increase the incidence of unwanted side effects. Alternatives to CHX include cetylpyridinium chloride, oxidizing mouthwashes, and povidone-iodine (PVP-I). Although, some of these products show less adverse effects, their application is limited by the absence of clinical research, such as randomized clinical trials and systematic meta-analysis reviews, or the absence of commercially available formulations for intraoral use.
Bioactive BBL is a new commercial mouthwash solution that is basically a negatively charged liquid saline containing Ca2+ and Mg2+ salts. BBL has no taste, no odor, and does not induce allergic reactions. Comparison of the efficacy of CHX and BBL in human patients revealed that the latter dramatically reduces pain within a period of 4 days and promotes complete oral healing with 7 days. The current randomized, double blind clinical trial indicates that BBL is an effective mouthwash solution for prospective clinical applications. Nevertheless, further longitudinal studies are required to delineate its capacity based on antiplaque and antiseptic properties.
5. Conclusions
Clinical data collected from patient diaries revealed a statistically significant positive effect for the BBL mouthwash in improving post-operative quality of wound healing compared with CHX mouthwash both during and after 7 days of application. The application of both mouthwashes resulted in differential progressive pain reduction in consecutive weeks post-surgery; however, BBL resulted in significant pain relief starting at day 4. No gender differences associated with pain or would healing were observed in response to the applied mouthwashes. Together, the wound healing properties of BBL may support its usage as a new pharmaceutical product with good physical, chemical, and biological stabilities.
6. Study Limitation
On the follow up evaluation, patient assessments were conducted based on phone calls, which may raise some concerns about bias related to early health status post-surgery. Although, the clinical observations were performed by several specialized dentist who were blinded for the treatment type, bias concerns may also be raised about the VAS analysis. In addition, as part of general clinical practice, all patients were treated with antibiotics in addition to the study treatment, which may suggest that the observed study outcome is due to an effect of both the treatment and the antibiotic.
Supplementary Materials
The following supporting information can be downloaded at:
https://www.mdpi.com/article/10.3390/jpm12101725/s1, Supplementary Table S1: The sociodemographic characteristics of the patients involved in the study. Table S2: Healing Index as described by Landry et. al. 1988.
Author Contributions
E.F.-A. (Eduard Ferrés-Amat) and E.F.-A. (Elvira Ferrés-Amat) supervised and conducted meetings with patients and their evaluation. N.C., M.B., E.F.-P. and C.M., data analysis and interpretation. A.S.A.-M. and A.A.M., statistical analysis and were blinded for the outcome assessment and measurements M.A., study conception and design and data assembly. A.A.M. and M.A., data analysis, outcome assessment, interpretation, and manuscript writing. All authors have read and agreed to the published version of the manuscript.
Funding
This study was funded by the OTRI project, reference number 2020907094, signed in May 2020 with the Public University of Navarra, Navarra, Spain.
Institutional Review Board Statement
Approval for the human study and written informed consent was obtained from all participants or guardians of patients below 16 years old, The study was conducted in accordance with the ethical guidelines of the Declaration of Helsinki and approved by the ethics committee at CEIm HM hospital s, Spain (CEIm HM Hospitales 21.03.1786-GHM; protocol ID: V01-2021; date: 16 April 2021; Clinical Trial Registry Platform: Clinical Trial Gov. Press).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
The authors would like to thank Kuwait Foundation for Advancement of Sciences (KFAS) and Dasman Diabetes Institute are acknowledged for the support.
Conflicts of Interest
E.F-P., C.M., M.B. and M.A. declare that they are associated researchers at Biointelligent Technology Systems S.L. Bone Bioactive composition and uses thereof. European patents: EP353211, US 16/344,322. Apart from the above involvement by Biointelligent Technology Systems, the authors have no financial or nonfinancial competing interests to declare related to this manuscript.
References
- Bielefeld, K.A.; Amini-Nik, S.; Alman, B.A. Cutaneous wound healing: Recruiting developmental pathways for regeneration. Cell. Mol. Life Sci. 2013, 70, 2059–2081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, V.W.; Gurtner, G.C.; Longaker, M.T. Wound healing: A paradigm for regeneration. Mayo. Clin. Proc. 2013, 88, 1022–1031. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toma, A.I.; Fuller, J.M.; Willett, N.J.; Goudy, S.L. Oral wound healing models and emerging regenerative therapies. Transl. Res. 2021, 236, 17–34. [Google Scholar] [CrossRef] [PubMed]
- Discepoli, N.; Vignoletti, F.; Laino, L.; de Sanctis, M.; Munoz, F.; Sanz, M. Early healing of the alveolar process after tooth extraction: An experimental study in the beagle dog. J. Clin. Periodontol. 2013, 40, 638–644. [Google Scholar] [CrossRef] [PubMed]
- Trombelli, L.; Farina, R.; Marzola, A.; Bozzi, L.; Liljenberg, B.; Lindhe, J. Modeling and remodeling of human extraction sockets. J. Clin. Periodontol. 2008, 35, 630–639. [Google Scholar] [CrossRef]
- Pagni, G.; Pellegrini, G.; Giannobile, W.V.; Rasperini, G. Postextraction alveolar ridge preservation: Biological basis and treatments. Int. J. Dent. 2012, 2012, 151030. [Google Scholar] [CrossRef] [Green Version]
- Whetman, J.; Mealey, B.L. Effect of Healing Time on New Bone Formation After Tooth Extraction and Ridge Preservation with Demineralized Freeze-Dried Bone Allograft: A Randomized Controlled Clinical Trial. J. Periodontol. 2016, 87, 1022–1029. [Google Scholar] [CrossRef]
- Politis, C.; Schoenaers, J.; Jacobs, R.; Agbaje, J.O. Wound Healing Problems in the Mouth. Front. Physiol. 2016, 7, 507. [Google Scholar] [CrossRef] [Green Version]
- Glim, J.E.; van Egmond, M.; Niessen, F.B.; Everts, V.; Beelen, R.H. Detrimental dermal wound healing: What can we learn from the oral mucosa? Wound Repair Regen. 2013, 21, 648–660. [Google Scholar] [CrossRef]
- Ford, S.J. The importance and provision of oral hygiene in surgical patients. Int. J. Surg. 2008, 6, 418–419. [Google Scholar] [CrossRef]
- Goldenhart, A.L.; Nagy, H. Assisting Patients with Personal Hygiene; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Varoni, E.; Tarce, M.; Lodi, G.; Carrassi, A. Chlorhexidine (CHX) in dentistry: State of the art. Minerva Stomatol. 2012, 61, 399–419. [Google Scholar]
- Colombo, A.P.; Haffajee, A.D.; Dewhirst, F.E.; Paster, B.J.; Smith, C.M.; Cugini, M.A.; Socransky, S.S. Clinical and microbiological features of refractory periodontitis subjects. J. Clin. Periodontol. 1998, 25, 169–180. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, S.; Addy, M.; Wade, W. The mechanism of action of chlorhexidine. A study of plaque growth on enamel inserts in vivo. J. Clin. Periodontol. 1988, 15, 415–424. [Google Scholar] [CrossRef] [PubMed]
- Eick, S.; Seltmann, T.; Pfister, W. Efficacy of antibiotics to strains of periodontopathogenic bacteria within a single species biofilm—An in vitro study. J. Clin. Periodontol. 2004, 31, 376–383. [Google Scholar] [CrossRef] [PubMed]
- Rajendiran, M.; Trivedi, H.M.; Chen, D.; Gajendrareddy, P.; Chen, L. Recent Development of Active Ingredients in Mouthwashes and Toothpastes for Periodontal Diseases. Molecules 2021, 26, 2001. [Google Scholar] [CrossRef]
- Ferrés-Amat, E.; Al Madhoun, A.; Ferrés-Amat, E.; Al Demour, S.; Ababneh, M.A.; Ferrés-Padró, E.; Marti, C.; Carrio, N.; Barajas, M.; Atari, M. Histologic and Histomorphometric Evaluation of a New Bioactive Liquid BBL on Implant Surface: A Preclinical Study in Foxhound Dogs. Materials 2021, 14, 6217. [Google Scholar] [CrossRef]
- Krishnankutty, B.; Bellary, S.; Kumar, N.B.; Moodahadu, L.S. Data management in clinical research: An overview. Indian J. Pharmacol. 2012, 44, 168–172. [Google Scholar] [CrossRef]
- O’Leary, T.J.; Drake, R.B.; Naylor, J.E. The plaque control record. J. Periodontol. 1972, 43, 38. [Google Scholar] [CrossRef]
- Ainamo, J.; Bay, I. Problems and proposals for recording gingivitis and plaque. Int. Dent. J. 1975, 25, 229–235. [Google Scholar]
- Fickl, S.; Fischer, K.R.; Jockel-Schneider, Y.; Stappert, C.F.; Schlagenhauf, U.; Kebschull, M. Early wound healing and patient morbidity after single-incision vs. trap-door graft harvesting from the palate—A clinical study. Clin. Oral Investig. 2014, 18, 2213–2219. [Google Scholar] [CrossRef]
- Landry, R.G. Effectiveness of Benzydamine HC1 in the Treatment of Periodontal Post-Surgical Patients. Doctoral Dissertation, Faculty of Dentistry, University of Toronto, Toronto, ON, Canada, 1985. [Google Scholar]
- Haefeli, M.; Elfering, A. Pain assessment. Eur. Spine J. 2006, 15 (Suppl. 1), S17–S24. [Google Scholar] [CrossRef] [PubMed]
- Chye, R.M.L.; Perrotti, V.; Piattelli, A.; Iaculli, F.; Quaranta, A. Effectiveness of Different Commercial Chlorhexidine-Based Mouthwashes After Periodontal and Implant Surgery: A Systematic Review. Implant Dent. 2019, 28, 74–85. [Google Scholar] [CrossRef] [PubMed]
- Brookes, Z.L.S.; Bescos, R.; Belfield, L.A.; Ali, K.; Roberts, A. Current uses of chlorhexidine for management of oral disease: A narrative review. J. Dent. 2020, 103, 103497. [Google Scholar] [CrossRef] [PubMed]
- Flotra, L.; Gjermo, P.; Rolla, G.; Waerhaug, J. Side effects of chlorhexidine mouth washes. Scand. J. Dent. Res. 1971, 79, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Pemberton, M.N.; Gibson, J. Chlorhexidine and hypersensitivity reactions in dentistry. Br. Dent. J. 2012, 213, 547–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- James, P.; Parnell, C.; Whelton, H. The caries-preventive effect of chlorhexidine varnish in children and adolescents: A systematic review. Caries Res. 2010, 44, 333–340. [Google Scholar] [CrossRef]
- Berchier, C.E.; Slot, D.E.; Van der Weijden, G.A. The efficacy of 0.12% chlorhexidine mouthrinse compared with 0.2% on plaque accumulation and periodontal parameters: A systematic review. J. Clin. Periodontol. 2010, 37, 829–839. [Google Scholar] [CrossRef]
- Poppolo Deus, F.; Ouanounou, A. Chlorhexidine in Dentistry: Pharmacology, Uses, and Adverse Effects. Int. Dent. J. 2022, 72, 269–277. [Google Scholar] [CrossRef]
- Samanth, S.A.; Varghese, S.S. The Most Effective Concentration of Chlorhexidine as a Mouthwash-Systematic Review. J. Pharm. Sci. Res. 2017, 9, 233–236. [Google Scholar]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).

 ,
, 



{kind=link}
{kind=link}
{kind=link}