
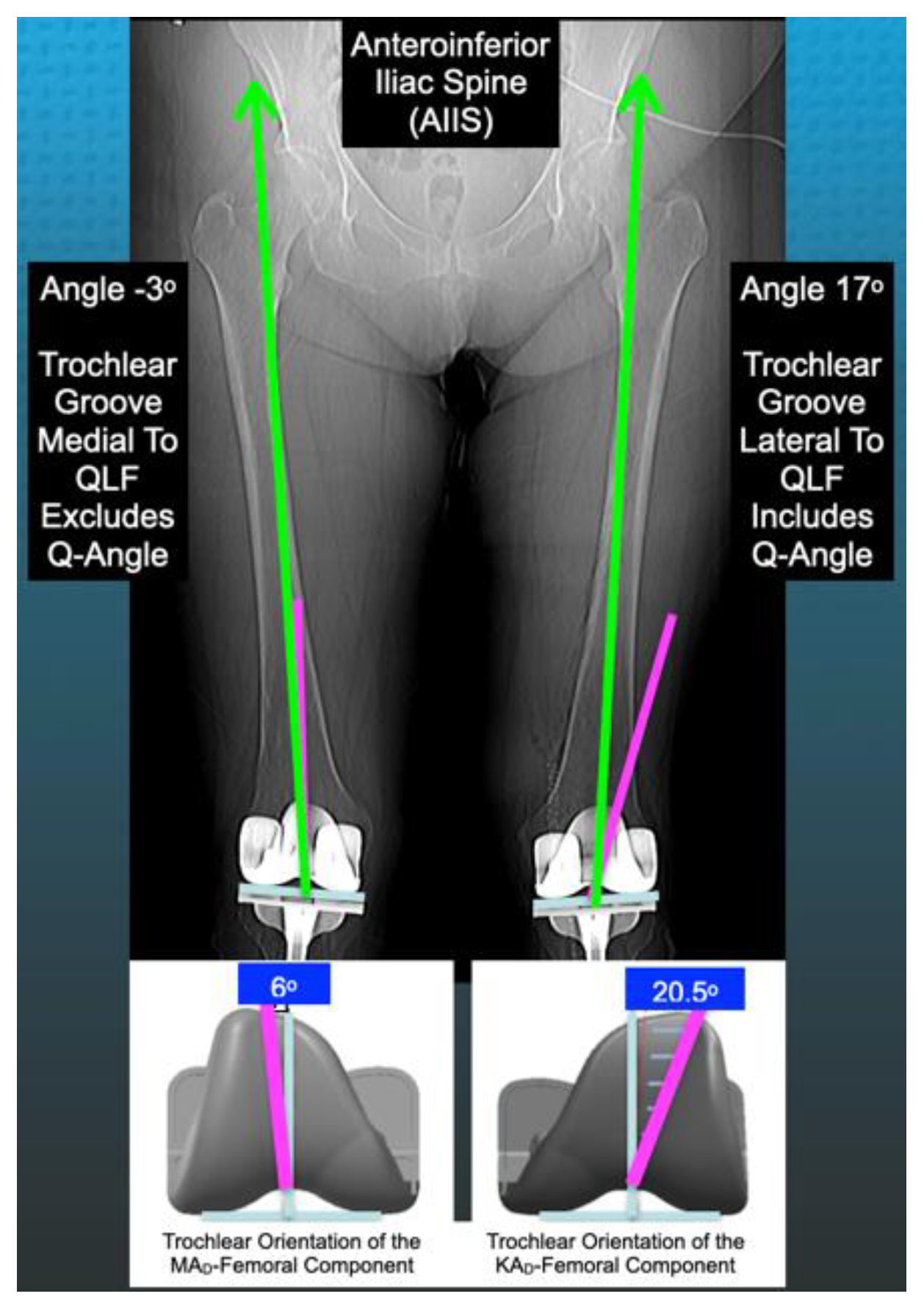
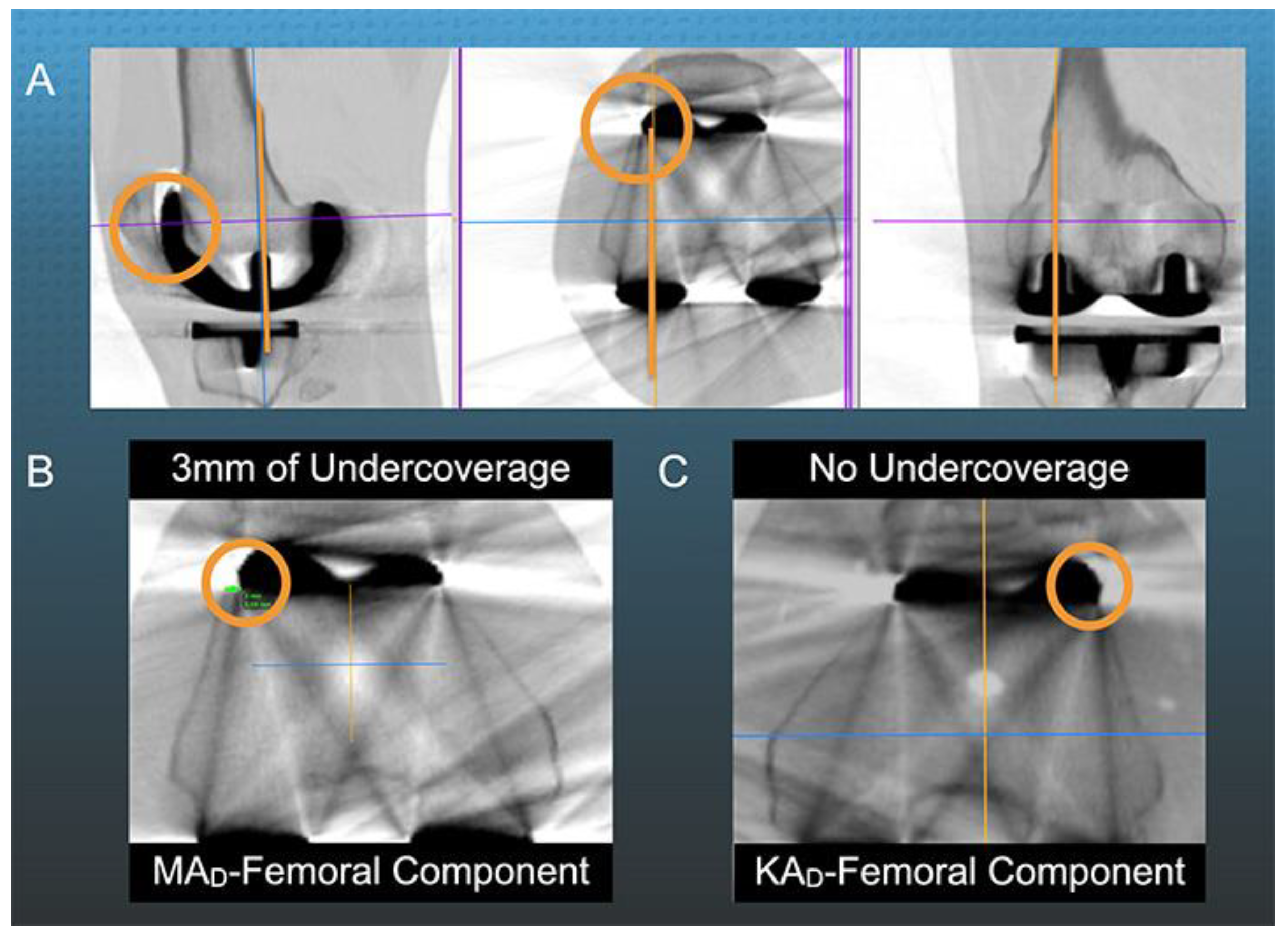
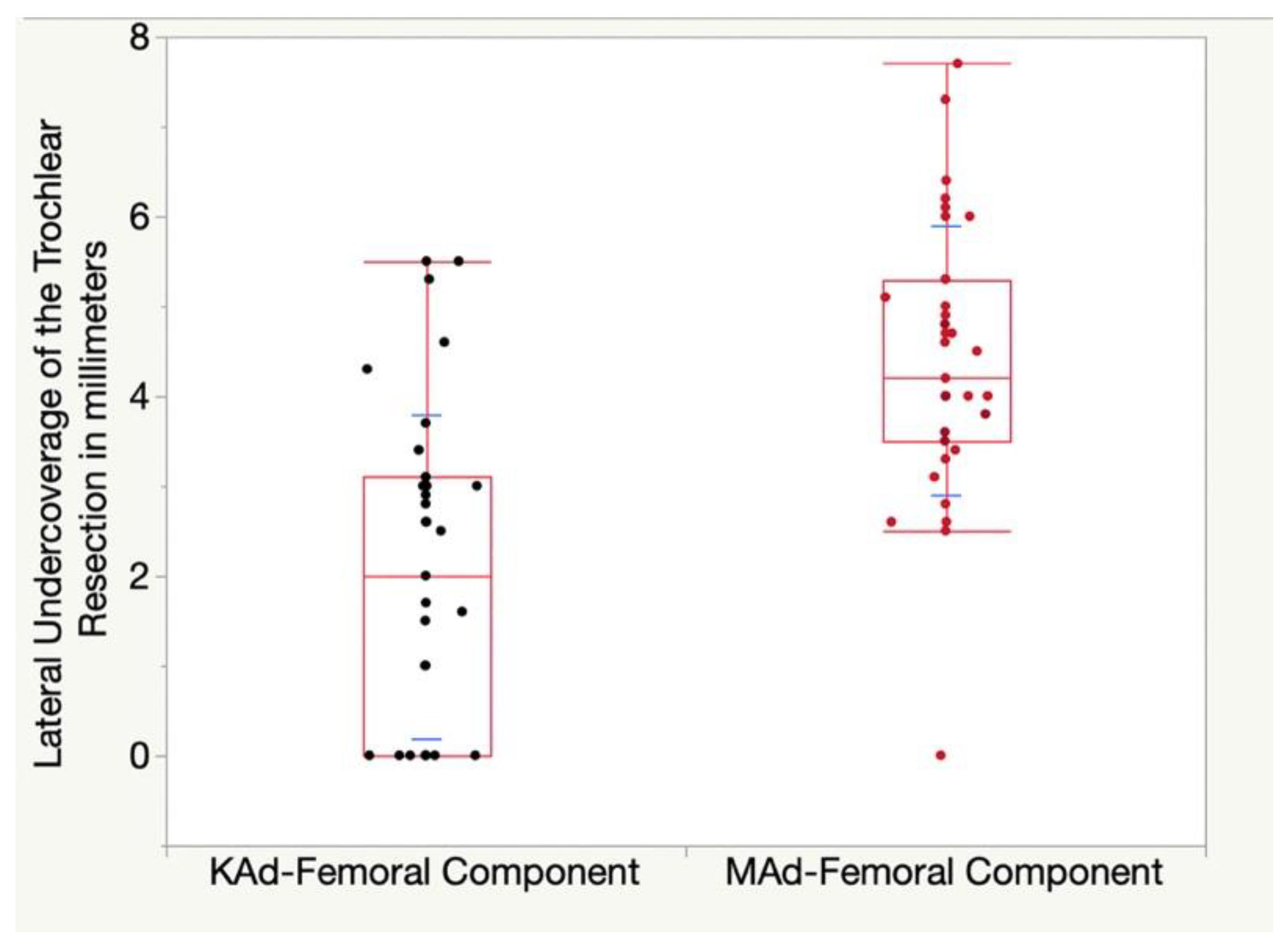
The Trochlear Groove of a Femoral Component Designed for Kinematic Alignment Is Lateral to the Quadriceps Line of Force and Better Laterally Covers the Anterior Femoral Resection Than a Mechanical Alignment Design


Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Rivière, C.; Iranpour, F.; Harris, S.; Auvinet, E.; Aframian, A.; Parratte, S.; Cobb, J. Differences in Trochlear Parameters between Native and Prosthetic Kinematically or Mechanically Aligned Knees. Orthop. Traumatol. Surg. Res. 2018, 104, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Wen, L.; Zhang, L.; Ma, D.; Dong, X.; Qu, T. Undercoverage of Lateral Trochlear Resection Is Correlated with the Tibiofemoral Alignment Parameters in Kinematically Aligned TKA: A Retrospective Clinical Study. BMC Musculoskelet. Disord. 2021, 22, 196. [Google Scholar] [CrossRef]
- Kim, J.-T.; Han, J.; Shen, Q.H.; Moon, S.W.; Won, Y.-Y. Morphological Patterns of Anterior Femoral Condylar Resection in Kinematically and Mechanically Aligned Total Knee Arthroplasty. J. Arthroplast. 2018, 33, 2506–2511. [Google Scholar] [CrossRef]
- Nedopil, A.J.; Singh, A.K.; Howell, S.M.; Hull, M.L. Does Calipered Kinematically Aligned TKA Restore Native Left to Right Symmetry of the Lower Limb and Improve Function? J. Arthroplast. 2018, 33, 398–406. [Google Scholar] [CrossRef] [PubMed]
- Nedopil, A.J.; Delman, C.; Howell, S.M.; Hull, M.L. Restoring the Patient’s Pre-Arthritic Posterior Slope Is the Correct Target for Maximizing Internal Tibial Rotation When Implanting a PCL Retaining TKA with Calipered Kinematic Alignment. J. Pers. Med. 2021, 11, 516. [Google Scholar] [CrossRef] [PubMed]
- Nedopil, A.J.; Howell, S.M.; Hull, M.L. What Mechanisms Are Associated with Tibial Component Failure after Kinematically-Aligned Total Knee Arthroplasty? Int. Orthop. 2017, 41, 1561–1569. [Google Scholar] [CrossRef] [PubMed]
- Hazratwala, K.; O’Callaghan, W.B.; Dhariwal, S.; 360 Knee Group; Wilkinson, M.P.R. Wide Variation in Tibial Slopes and Trochlear Angles in the Arthritic Knee: A CT Evaluation of 4116 Pre-Operative Knees. Knee Surg. Sports Traumatol. Arthrosc. 2022, 30, 3049–3060. [Google Scholar] [CrossRef]
- Nedopil, A.J.; Howell, S.M.; Hull, M.L. What Clinical Characteristics and Radiographic Parameters Are Associated with Patellofemoral Instability after Kinematically Aligned Total Knee Arthroplasty? Int. Orthop. 2017, 41, 283–291. [Google Scholar] [CrossRef]
- Klasan, A.; de Steiger, R.; Holland, S.; Hatton, A.; Vertullo, C.J.; Young, S.W. Similar Risk of Revision after Kinematically Aligned, Patient-Specific Instrumented Total Knee Arthroplasty, and All Other Total Knee Arthroplasty: Combined Results from the Australian and New Zealand Joint Replacement Registries. J. Arthroplast. 2020, 35, 2872–2877. [Google Scholar] [CrossRef]
- Rivière, C.; Dhaif, F.; Shah, H.; Ali, A.; Auvinet, E.; Aframian, A.; Cobb, J.; Howell, S.; Harris, S. Kinematic Alignment of Current TKA Implants Does Not Restore the Native Trochlear Anatomy. Orthop. Traumatol. Surg. Res. 2018, 104, 983–995. [Google Scholar] [CrossRef]
- D’Lima, D.D.; Chen, P.C.; Kester, M.A.; Colwell, C.W. Impact of Patellofemoral Design on Patellofemoral Forces and Polyethylene Stresses. J. Bone Jt. Surg. Am. 2003, 85, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Barink, M.; Van de Groes, S.; Verdonschot, N.; De Waal Malefijt, M. The Difference in Trochlear Orientation between the Natural Knee and Current Prosthetic Knee Designs; towards a Truly Physiological Prosthetic Groove Orientation. J. Biomech. 2006, 39, 1708–1715. [Google Scholar] [CrossRef] [PubMed]
- Ando, T.; Hirose, H.; Inoue, M.; Shino, K.; Doi, T. A New Method Using Computed Tomographic Scan to Measure the Rectus Femoris-Patellar Tendon Q-Angle Comparison with Conventional Method. Clin. Orthop. Relat. Res. 1993, 289, 213–219. [Google Scholar] [CrossRef]
- Hirschmann, M.T.; Moser, L.B.; Amsler, F.; Behrend, H.; Leclercq, V.; Hess, S. Phenotyping the Knee in Young Non-Osteoarthritic Knees Shows a Wide Distribution of Femoral and Tibial Coronal Alignment. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 1385–1393. [Google Scholar] [CrossRef]
- Dhaliwal, A.; Zamora, T.; Nedopil, A.J.; Howell, S.M.; Hull, M.L. Six Commonly Used Postoperative Radiographic Alignment Parameters Do Not Predict Clinical Outcome Scores after Unrestricted Caliper-Verified Kinematically Aligned TKA. J. Pers. Med. 2022, 12, 1468. [Google Scholar] [CrossRef] [PubMed]
- Koh, D.T.S.; Woo, Y.L.; Yew, A.K.S.; Yeo, S.-J. Kinematic Aligned Femoral Rotation Leads to Greater Patella Tilt but Similar Clinical Outcomes When Compared to Traditional Femoral Component Rotation in Total Knee Arthroplasty. A Propensity Score Matched Study. Knee Surg. Sports Traumatol. Arthrosc. 2021, 29, 1059–1066. [Google Scholar] [CrossRef] [PubMed]
- Howell, S.M.; Bini, S.A.; Steele, G.D. (Eds.) Calipered Kinematically Aligned Total Knee Arthroplasty Performed with Specific Manual Instrumentation, Verification Checks, and a Decision Tree. In Calipered Kinematically Aligned Total Knee Arthroplasty: Theory, Surgical Techniques, Perspectives, 1st ed.; Elsevier: Amsterdam, The Netherlands, 2021; Volume 1, p. 7. [Google Scholar]
- Howell, S.M.; Nedopil, A.J.; Hull, M.L. Negligible Effect of Surgeon Experience on the Accuracy and Time to Perform Unrestricted Caliper Verified Kinematically Aligned TKA with Manual Instruments. Knee Surg. Sports Traumatol. Arthrosc. 2022, 30, 2966–2974. [Google Scholar] [CrossRef] [PubMed]
- Nedopil, A.J.; Howell, S.M.; Hull, M.L. A TKA Insert with A Lateral Flat Articular Surface Maximizes External and Internal Tibial Orientations without Anterior Lift-Off Relative to Low- and Ultracongruent Surfaces. J. Pers. Med. 2022, 12, 1274. [Google Scholar] [CrossRef]
- Nedopil, A.J.; Zamora, T.; Shelton, T.; Howell, S.M.; Hull, M. A Best-Fit of an Anatomic Tibial Baseplate Closely Parallels the Flexion-Extension Plane and Covers a High Percentage of the Proximal Tibia. J. Knee Surg. 2021, 34, 1486–1494. [Google Scholar] [CrossRef]
- Bartlett, J.W.; Frost, C. Reliability, Repeatability and Reproducibility: Analysis of Measurement Errors in Continuous Variables. Ultrasound Obstet. Gynecol. 2008, 31, 466–475. [Google Scholar] [CrossRef]
- Tran, T.; McEwen, P.; Peng, Y.; Trivett, A.; Steele, R.; Donnelly, W.; Clark, G. Kinematic Alignment in Total Knee Arthroplasty: A Five-Year Prospective, Multicentre, Survivorship Study. Bone Jt. Open 2022, 3, 656–665. [Google Scholar] [CrossRef] [PubMed]
- Howell, S.M.; Gill, M.; Shelton, T.J.; Nedopil, A.J. Reoperations Are Few and Confined to the Most Valgus Phenotypes 4 Years after Unrestricted Calipered Kinematically Aligned TKA. Knee Surg. Sports Traumatol. Arthrosc. 2022, 30, 948–957. [Google Scholar] [CrossRef] [PubMed]
- Keshmiri, A.; Maderbacher, G.; Baier, C.; Benditz, A.; Grifka, J.; Greimel, F. Kinematic Alignment in Total Knee Arthroplasty Leads to a Better Restoration of Patellar Kinematics Compared to Mechanic Alignment. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 1529–1534. [Google Scholar] [CrossRef] [PubMed]
- Koh, I.J.; Park, I.J.; Lin, C.C.; Patel, N.A.; Chalmers, C.E.; Maniglio, M.; McGarry, M.H.; Lee, T.Q. Kinematically Aligned Total Knee Arthroplasty Reproduces Native Patellofemoral Biomechanics during Deep Knee Flexion. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 1520–1528. [Google Scholar] [CrossRef]
- Lozano, R.; Campanelli, V.; Howell, S.; Hull, M. Kinematic Alignment More Closely Restores the Groove Location and the Sulcus Angle of the Native Trochlea than Mechanical Alignment: Implications for Prosthetic Design. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 1504–1513. [Google Scholar] [CrossRef] [PubMed]
- Hull, M.L.; Howell, S.M. Differences in Trochlear Morphology from Native Using a Femoral Component Interfaced with an Anatomical Patellar Prosthesis in Kinematic Alignment and Mechanical Alignment. J. Knee Surg. 2022, 35, 625–633. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Preoperative Characteristics and Function Scores | KAd-FC Mean ± Standard Deviation (Range) | MAd-FC Mean ± Standard Deviation (Range) | p-Value |
|---|---|---|---|
| Extension (°) | 8 ± 8° (0 to 36°) | 6 ± 6° (0 to 25°) | 0.32 |
| Flexion (°) | 109 ± 14° (71 to 130°) | 108 ± 13° (69 to 128°) | 0.86 |
| Type of Osteoarthritic Knee Deformity | 80% varus, 5% valgus, 15% patellofemoral | 80% varus, 5% valgus, 15% patellofemoral | N.A. |
| Knee Society Score (100 best, 0 worst) | 50 ± 27 points (0 to 100) | 41 ± 21 points (0 to 80) | 0.14 |
| Knee Society Function Score (100 best, 0 worst) | 47 ± 23 points (5 to 90) | 45 ± 20 points (0 to 100) | 0.62 |
| Oxford Knee Score (48 best, 0 worst) | 20 ± 10 points (0 to 36) | 18 ± 7 points (5 to 31) | 0.34 |
| KOOS Jr (100 best, 0 worst) | 44 ± 20 points (0 to 66) | 39 ± 14 points (0 to 59) | 0.17 |
| Postoperative Alignment Parameter | Inter-Observer Intraclass Correlation | Intra-Observer Intraclass Correlation | Repeatability |
|---|---|---|---|
| Angle Between the Trochlear Groove and Quadriceps Line of Force | ICC = 0.82 # | ICC = 0.81 # | 0.2° |
| Undercoverage of the Lateral Anterior femoral resection | ICC = 0.92 * | ICC = 0.93 * | 0.5 mm |
| Patella Tilt Angle (PTA) | ICC = 0.88 # | ICC = 0.89 # | 0.9° |
| Clinical Characteristics Assessed Post-Operatively at 6-Weeks | KAd-FC Mean ± SD (Range) | MAd-FC Mean ± SD (Range) | p-Value |
|---|---|---|---|
| Extension (°) | 2 ± 3° (0 to 10°) | 2 ± 3° (0 to 10°) | 0.54 |
| Flexion (°) | 109 ± 11° (90 to 135°) | 107 ± 12° (70 to 126°) | 0.11 |
| Knee Society Score Knee (100 best, 0 worst) | 91 ± 12 points (40 to 100) | 86 ± 12 points (64 to 100) | 0.056 |
| Knee Society Score Function (100 best, 0 worst) | 57 ± 18 points (0 to 100) | 53 ± 18 points (10 to 80) | 0.53 |
| Oxford Knee Score (48 best, 0 worst) | 30 ± 8 points (8 to 44) | 32 ± 8 points (13 to 46) | 0.15 |
| KOOS Jr (100 best, 0 worst) | 61 ± 14 points (0 to 85) | 66 ± 15 points (31 to 100) | 0.11 |
| Forgotten Joint Score (100 best, 0 worst) | 41 ± 25 points (0 to 94) | 52 ± 29 points (0 to 100) | 0.08 |
| Radiological Parameters | KAd-FC Mean ± Standard Deviation (Range) | MAd-FC Mean ± Standard Deviation (Range) | p-Value |
|---|---|---|---|
| Hip-Knee-Ankle Angle (HKAA) | 178 ± 3.2° (170 to 182°) | 178 ± 3.3° (171 to 184°) | 0.83 |
| Distal Lateral Femoral Angle (DLFA) | 88 ± 2.4° (83 to 94°) | 88 ± 2.2° (83 to 93°) | 0.92 |
| Proximal Medial Tibial Angle (PMTA) | 85 ± 2° (82 to 89°) | 85 ± 2.6° (79 to 90°) | 0.67 |
| Tibial Slope Angle (TSA) | 84 ± 2.6° (80 to 89°) | 85 ± 3° (75 to 89°) | 0.29 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sappey-Marinier, E.; Howell, S.M.; Nedopil, A.J.; Hull, M.L. The Trochlear Groove of a Femoral Component Designed for Kinematic Alignment Is Lateral to the Quadriceps Line of Force and Better Laterally Covers the Anterior Femoral Resection Than a Mechanical Alignment Design. J. Pers. Med. 2022, 12, 1724. https://doi.org/10.3390/jpm12101724
Sappey-Marinier E, Howell SM, Nedopil AJ, Hull ML. The Trochlear Groove of a Femoral Component Designed for Kinematic Alignment Is Lateral to the Quadriceps Line of Force and Better Laterally Covers the Anterior Femoral Resection Than a Mechanical Alignment Design. Journal of Personalized Medicine. 2022; 12(10):1724. https://doi.org/10.3390/jpm12101724
Chicago/Turabian StyleSappey-Marinier, Elliot, Stephen M. Howell, Alexander J. Nedopil, and Maury L. Hull. 2022. "The Trochlear Groove of a Femoral Component Designed for Kinematic Alignment Is Lateral to the Quadriceps Line of Force and Better Laterally Covers the Anterior Femoral Resection Than a Mechanical Alignment Design" Journal of Personalized Medicine 12, no. 10: 1724. https://doi.org/10.3390/jpm12101724