
Job-Related Performance and Quality of Life Benefits in First Responders Given Access to H-Wave® Device Stimulation: A Retrospective Cohort Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source and Study Design
2.2. Data Collection
2.3. Statistical Analysis
3. Results
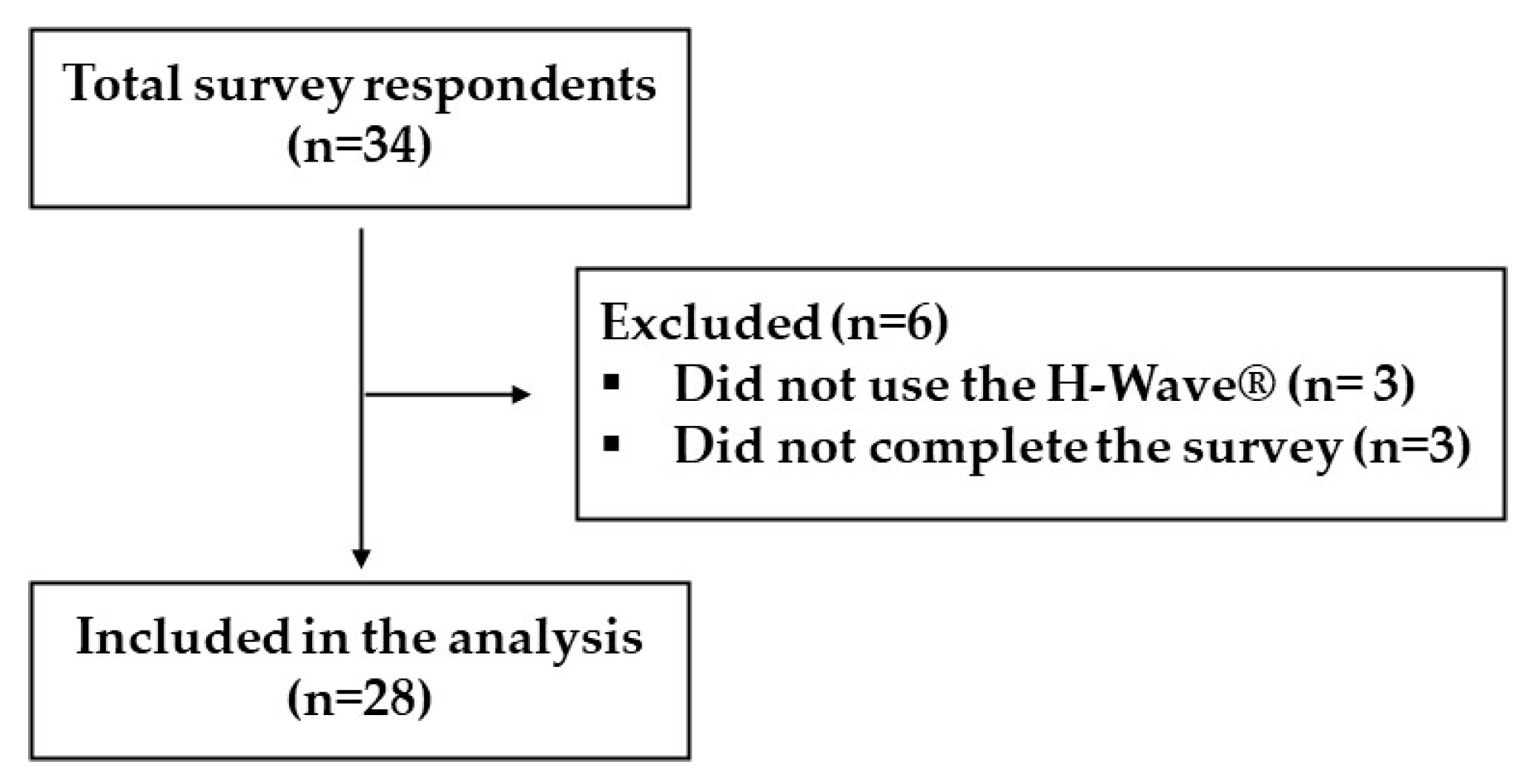
3.1. Cohort and Exclusion
3.2. Quality of Life-Related Survey Responses
3.3. Work-Related Survey Responses
3.4. Bivariate Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Topic | Questions |
|---|---|
| Attended Training Session | Did you attend an H-Wave training at your station? |
| Use of H-Wave® | Did you use the H-Wave? |
| Benefit From H-Wave® | Did you have a positive experience using H-Wave? |
| Reduction of Pain | Did your H-Wave treatment(s) reduce your pain? |
| Improvement in Sleep | Did your H-Wave treatment(s) improve your sleep? |
| Improvement in Mood | Did your H-Wave improve your mood? |
| Increased Range-of-Motion (ROM) | Did your H-Wave treatment(s) increase your range of motion? |
| Avoided Missing Work | Did your H-Wave treatment(s) helped you to avoid missed work? |
| Improvement in Physical Job Performance | Did your H-Wave treatment(s) improve physical job performance? |
| More Time Spent with Family | Did your H-Wave treatment(s) allow you to spend more time with family? |
| Postponed Workers Comp | Having access to H-Wave has postponed your need to file a work comp claim? |
| Use Frequency of H-Wave® | How many times did you use H-Wave? Choose one of the following: 1–5, 6–10, or 10+ |
| Would Benefit from Further Use of H-Wave® | Would it be beneficial to you to have access to H-Wave again? |
References
- Feldman, D.E.; Carlesso, L.C.; Nahin, R.L. Management of Patients with a Musculoskeletal Pain Condition that is Likely Chronic: Results from a National Cross Sectional Survey. J. Pain 2020, 21, 869–880. [Google Scholar] [CrossRef]
- Hagen, K.; Linde, M.; Heuch, I.; Stovner, L.J.; Zwart, J.-A. Increasing prevalence of chronic musculoskeletal complaints. A large 11-year follow-up in the general population (HUNT 2 and 3). Pain Med. 2011, 12, 1657–1666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lehti, T.E.; Rinkinen, M.-O.; Aalto, U.; Roitto, H.M.; Knuutila, M.; Öhman, H.; Kautiainen, H.; Karppinen, H.; Tilvis, R.; Strandberg, T.; et al. Prevalence of Musculoskeletal Pain and Analgesic Treatment Among Community-Dwelling Older Adults: Changes from 1999 to 2019. Drugs Aging 2021, 38, 931–937. [Google Scholar] [CrossRef] [PubMed]
- Feldman, D.E.; Nahin, R.L. National Estimates of Chronic Musculoskeletal Pain and Its Treatment in Children, Adolescents, and Young Adults in the United States: Data from the 2007–2015 National Ambulatory Medical Care Survey. J. Pediatr. 2021, 233, 212–219.e1. [Google Scholar] [CrossRef]
- Saeki, S. Side Effects of Acetaminophen and their Management. Masui. Jpn. J. Anesthesiol. 2016, 65, 701–708. (In Japanese) [Google Scholar]
- Bovill, J.G. Mechanisms of actions of opioids and non-steroidal anti-inflammatory drugs. Eur. J. Anaesthesiol. Suppl. 1997, 15, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.P.; Vase, L.; Hooten, W.M. Chronic pain: An update on burden, best practices, and new advances. Lancet 2021, 397, 2082–2097. [Google Scholar] [CrossRef]
- Flynn, D.M. Chronic Musculoskeletal Pain: Nonpharmacologic, Noninvasive Treatments. Am. Fam. Physician 2020, 102, 465–477. [Google Scholar]
- Alonso Pérez, J.L.; Pérez, S.M.; Battaglino, A.; Villafañe, J.H.; Alonso-Sal, A.; Sánchez Romero, E.A. An Up-Date of the Muscle Strengthening Exercise Effectiveness in Postmenopausal Women with Osteoporosis: A Qualitative Systematic Review. J. Clin. Med. 2021, 10, 2229. [Google Scholar] [CrossRef] [PubMed]
- Fredin, K.; Loras, H. Manual therapy, exercise therapy or combined treatment in the management of adult neck pain—A systematic review and meta-analysis. Musculoskelet. Sci. Pract. 2017, 31, 62–71. [Google Scholar] [CrossRef] [PubMed]
- Teoli, D.; An, J. Transcutaneous Electrical Nerve Stimulation. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Muñoz-Fernández, A.C.; Barragán-Carballar, C.; Villafañe, J.H.; Martín-Pérez, S.; Alonso-Pérez, J.L.; Díaz-Meco, R.; García Jiménez, D.; Sánchez Romero, E.A. A new ultrasound-guided percutaneous electrolysis and exercise treatment in patellar tendinopathy: Three case reports. Front. Biosci. 2021, 26, 1166–1175. [Google Scholar]
- Gómez-Chiguano, G.F.; Navarro-Santana, M.J.; Cleland, J.A.; Arias-Buría, J.L.; Fernández-de-Las-Peñas, C.; Ortega-Santiago, R. Effectiveness of Ultrasound-Guided Percutaneous Electrolysis for Musculoskeletal Pain: A Systematic Review and Meta-Analysis. Pain Med. 2021, 22, 1055–1071. [Google Scholar] [CrossRef]
- Blum, K.; Chen, A.L.; Chen, T.J.; Prihoda, T.J.; Schoolfield, J.; DiNubile, N.; Waite, R.L.; Arcuri, V.; Kerner, M.; Braverman, E.R.; et al. The H-Wave device is an effective and safe non-pharmacological analgesic for chronic pain: A meta-analysis. Adv. Ther. 2008, 25, 644–657. [Google Scholar] [CrossRef]
- Blum, K.; Ho, C.-K.; Chen, A.; Fulton, M.; Fulton, B.; Westcott, W.; Reinl, G.; Braverman, E.; DiNubile, N.; Chen, T. The H-Wave((R)) Device Induces NODependent Augmented Microcirculation and Angiogenesis, Providing Both Analgesia and Tissue Healing in Sports Injuries. Physician Sportsmed. 2008, 36, 103–114. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.L.; Blum, K.; Callahan, M.F.; DiNubile, N.A.; Chen, T.J.; Waite, R.L. H-Wave induces arteriolar vasodilation in rat striated muscle via nitric oxide-mediated mechanisms. J. Orthop. Res. 2009, 27, 1248–1251. [Google Scholar] [CrossRef]
- Smith, T.L.; Callahan, M.F.; Blum, K.; Dinubile, N.A.; Chen, T.J.; Waite, R.L. H-Wave® effects on blood flow and angiogenesis in longitudinal studies in rats. J. Surg. Orthop. Adv. 2011, 20, 255–259. [Google Scholar]
- Williamson, T.K.; Rodriguez, H.C.; Gonzaba, A.; Poddar, N.; Norwood, S.M.; Gupta, A. H-Wave® Device Stimulation: A Critical Review. J. Pers. Med. 2021, 11, 1134. [Google Scholar] [CrossRef]
- Bureau of Labor Statistics. Injuries, Illnesses, and Fatalities: Police Officers. 27 April 2018. Available online: https://www.bls.gov/iif/oshwc/cfoi/policeofficers-2014.htm (accessed on 24 July 2022).
- Killip, S.C.; MacDermid, J.C.; Sinden, K.E.; Gewurtz, R.E.; Scott, L. Identifying predictors of return to work and the duration of time off work in first responders affected with musculoskeletal injuries or mental health issues. Int. Arch. Occup. Environ. Health 2022, 95, 723–735. [Google Scholar] [CrossRef]
- Reichard, A.A.; Jackson, L.L. Occupational injuries among emergency responders. Am. J. Ind. Med. 2010, 53, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Petit, A.; Bodin, J.; Delarue, A.; D’Escatha, A.; Fouquet, N.; Roquelaure, Y. Risk factors for episodic neck pain in workers: A 5-year prospective study of a general working population. Int. Arch. Occup. Environ. Health 2018, 91, 251–261. [Google Scholar] [CrossRef] [PubMed]
- Warshawsky, M.J. The Average US Retirement Age Increased over the Past 30 Years. American Enterprise Institute. 5 May 2022. Available online: https://www.aei.org/research-products/report/the-average-us-retirement-age-increased-over-the-past-30-years/#:~:text=Key%20Points,years%2C%20from%2062%20to%2065 (accessed on 24 July 2022).
- Casas, J.B.; Benuto, L.T. Work-related traumatic stress spillover in first responder families: A systematic review of the literature. Psychol. Trauma 2022, 14, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Porter, K.L.; Henriksen, R.C. The phenomenological experience of first responder spouses. Fam. J. 2016, 24, 44–51. [Google Scholar] [CrossRef] [Green Version]
- Paterson, J.L.; Sofianopoulos, S.; Williams, B. What paramedics think about when they think about fatigue: Contributing factors. Emerg. Med. Australas. 2014, 26, 139–144. [Google Scholar] [CrossRef]
- Julka, I.S.; Alvaro, M.; Kumar, D. Beneficial effects of electrical stimulation on neuropathic symptoms in diabetes patients. J. Foot Ankle Surg. 1998, 37, 191–194. [Google Scholar] [CrossRef]
- Blum, K.; Jacobs, W.; Modestino, E.J.; DiNubile, N.; Baron, D.; McLaughlin, T.; Siwicki, D.; Elman, I.; Moran, M.; Braverman, E.R.; et al. Insurance Companies Fighting the Peer Review Empire without any Validity: The Case for Addiction and Pain Modalities in the face of an American Drug Epidemic. SEJ Surg. Pain 2018, 1, 1–11. [Google Scholar]

| Proportion of Survey Respondents | Number of Survey Respondents | Reported Benefit |
|---|---|---|
| 92.86% | 26 | Positive experience * |
| 82.14% | 23 | Less pain * |
| 57.14% | 16 | Improved job performance |
| 53.57% | 15 | Increased range of motion |
| 35.71% | 10 | Improved sleep |
| 35.71% | 10 | Avoided missed work |
| 32.14% | 9 | Improved mood |
| 32.14% | 9 | More time with family |
| Avoid Missing Work | Total | ||||
| Yes | Not Sure | ||||
| Attended Training Session | Yes | 9 | 9 | 18 | |
| 32.14% | 32.14% | 64.29% | |||
| No | 1 | 9 | 10 | ||
| 3.57% | 32.14% | 35.71% | |||
| Total | 10 | 18 | 28 | ||
| 35.71% | 64.28% | 100% | |||
| H-Wave® Use Frequency | Total | ||||
| 1 to 5 | 6 to 10 | 10+ | |||
| Attended Training Session | Yes | 1 | 4 | 13 | 18 |
| 3.57% | 14.29% | 46.43% | 64.29% | ||
| No | 4 | 4 | 2 | 10 | |
| 14.29% | 14.29% | 7.14% | 35.71% | ||
| Total | 5 | 8 | 15 | 28 | |
| 17.86% | 28.57% | 53.57% | 100% | ||
| Reduction in Pain | Total | ||||
| Yes | No | ||||
| Benefit from H-Wave® | Yes | 23 | 3 | 26 | |
| 82.14% | 10.71% | 92.86% | |||
| No | 0 | 2 | 2 | ||
| 0.00% | 7.14% | 7.14% | |||
| Total | 23 | 5 | 28 | ||
| 82.14% | 17.86% | 100% | |||
| Benefit from H-Wave® | Total | ||||
| Yes | No | ||||
| Use Frequency of H-Wave® | 1 to 5 | 3 | 2 | 5 | |
| 10.71% | 7.14% | 17.86% | |||
| 6 to 10 | 8 | 0 | 8 | ||
| 28.57% | 0.00% | 28.57% | |||
| 10+ | 15 | 0 | 15 | ||
| 53.57% | 0.00% | 53.57% | |||
| Total | 26 | 2 | 28 | ||
| 92.86% | 7.14% | 100% | |||
| Reduction in Pain | Total | ||||
| Yes | No | ||||
| Use Frequency of H-Wave® | 1 to 5 | 2 | 3 | 5 | |
| 7.14% | 10.71% | 17.86% | |||
| 6 to 10 | 8 | 0 | 8 | ||
| 28.57% | 0.00% | 28.57% | |||
| 10+ | 13 | 2 | 15 | ||
| 46.43% | 7.14% | 53.57% | |||
| Total | 23 | 5 | 28 | ||
| 82.14% | 17.86% | 100% | |||
| Increased Range-of-Motion (ROM) | Total | ||||
| Yes | No | ||||
| Use Frequency of H-Wave® | 1 to 5 | 1 | 4 | 5 | |
| 3.57% | 14.29% | 17.86% | |||
| 6 to 10 | 7 | 1 | 8 | ||
| 25.00% | 3.57% | 28.57% | |||
| 10+ | 7 | 8 | 15 | ||
| 25.00% | 28.57% | 53.57% | |||
| Total | 15 | 13 | 28 | ||
| 53.57% | 46.43% | 100% | |||
| Avoided Missing Work | Total | ||||
| Yes | No | ||||
| Use Frequency of H-Wave® | 1 to 5 | 0 | 0 | 5 | |
| 0.00% | 0.00% | 17.86% | |||
| 6 to 10 | 2 | 1 | 8 | ||
| 7.14% | 3.57% | 28.57% | |||
| 10+ | 8 | 0 | 15 | ||
| 28.57% | 0.00% | 53.57% | |||
| Total | 10 | 1 | 28 | ||
| 35.71% | 3.57% | 100% | |||
| Would Benefit from Further Use of H-Wave® | Total | ||||
| Yes | No | ||||
| Use Frequency of H-Wave® | 1 to 5 | 3 | 1 | 5 | |
| 10.71% | 3.57% | 17.86% | |||
| 6 to 10 | 5 | 3 | 8 | ||
| 17.86% | 10.71% | 28.57% | |||
| 10+ | 14 | 0 | 15 | ||
| 50.00% | 0.00% | 53.57% | |||
| Total | 22 | 4 | 28 | ||
| 78.57% | 14.29% | 100% | |||
| Improvement in Sleep | Total | ||||
| Yes | No | ||||
| Reduction of Pain | Yes | 10 | 13 | 23 | |
| 35.71% | 46.43% | 82.14% | |||
| No | 0 | 5 | 5 | ||
| 0.00% | 17.86% | 17.86% | |||
| Total | 10 | 18 | 28 | ||
| 35.71% | 64.29% | 100% | |||
| Increased Range-of-Motion (ROM) | Total | ||||
| Yes | No | ||||
| Reduction of Pain | Yes | 15 | 8 | 23 | |
| 53.57% | 28.57% | 82.14% | |||
| No | 0 | 5 | 5 | ||
| 0.00% | 17.86% | 17.86% | |||
| Total | 15 | 13 | 28 | ||
| 53.57% | 46.43% | 100% | |||
| Improvement in Physical Job Performance | Total | ||||
| Yes | No | ||||
| Reduction of Pain | Yes | 15 | 8 | 23 | |
| 53.57% | 28.57% | 82.14% | |||
| No | 1 | 4 | 5 | ||
| 3.57% | 14.29% | 17.86% | |||
| Total | 16 | 12 | 28 | ||
| 57.14% | 42.86% | 100% | |||
| More Time Spent with Family | Total | ||||
| Yes | No | ||||
| Improvement in Mood | Yes | 6 | 3 | 9 | |
| 21.43% | 10.71% | 32.14% | |||
| No | 3 | 16 | 19 | ||
| 10.71% | 57.14% | 67.86% | |||
| Total | 9 | 19 | 28 | ||
| 32.14% | 67.86% | 100% | |||
| More Time Spent with Family | Total | ||||
| Yes | No | ||||
| Increased Range of Motion | Yes | 7 | 8 | 15 | |
| 25.00% | 28.57% | 53.57% | |||
| No | 2 | 11 | 13 | ||
| 7.14% | 39.29% | 46.43% | |||
| Total | 9 | 19 | 28 | ||
| 32.14% | 67.86% | 100% | |||
| More Time Spent with Family | Total | ||||
| Yes | No | ||||
| Improvement in Physical Job Performance | Yes | 8 | 8 | 16 | |
| 28.57% | 28.57% | 57.14% | |||
| No | 1 | 11 | 12 | ||
| 3.57% | 39.29% | 42.86% | |||
| Total | 9 | 19 | 28 | ||
| 32.14% | 67.86% | 100% | |||
| Would Benefit from Further Use of H-Wave® | Total | ||||
| Yes | No | ||||
| Improvement in Physical Job Performance | Yes | 14 | 2 | 16 | |
| 50.00% | 7.14% | 57.14% | |||
| No | 8 | 4 | 12 | ||
| 28.57% | 14.29% | 42.86% | |||
| Total | 22 | 6 | 28 | ||
| 78.57% | 21.43% | 100% | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Williamson, T.K.; Rodriguez, H.C.; Han, D.; Norwood, S.M.; Gupta, A. Job-Related Performance and Quality of Life Benefits in First Responders Given Access to H-Wave® Device Stimulation: A Retrospective Cohort Study. J. Pers. Med. 2022, 12, 1674. https://doi.org/10.3390/jpm12101674
Williamson TK, Rodriguez HC, Han D, Norwood SM, Gupta A. Job-Related Performance and Quality of Life Benefits in First Responders Given Access to H-Wave® Device Stimulation: A Retrospective Cohort Study. Journal of Personalized Medicine. 2022; 12(10):1674. https://doi.org/10.3390/jpm12101674
Chicago/Turabian StyleWilliamson, Tyler K., Hugo C. Rodriguez, David Han, Stephen M. Norwood, and Ashim Gupta. 2022. "Job-Related Performance and Quality of Life Benefits in First Responders Given Access to H-Wave® Device Stimulation: A Retrospective Cohort Study" Journal of Personalized Medicine 12, no. 10: 1674. https://doi.org/10.3390/jpm12101674