
Evaluation of Sarcopenia, Frailty, and Inflammation on Adverse Events and Survival Outcomes in Patients with Oral Cavity Squamous Cell Carcinoma under Adjuvant Chemoradiotherapy


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Study Design
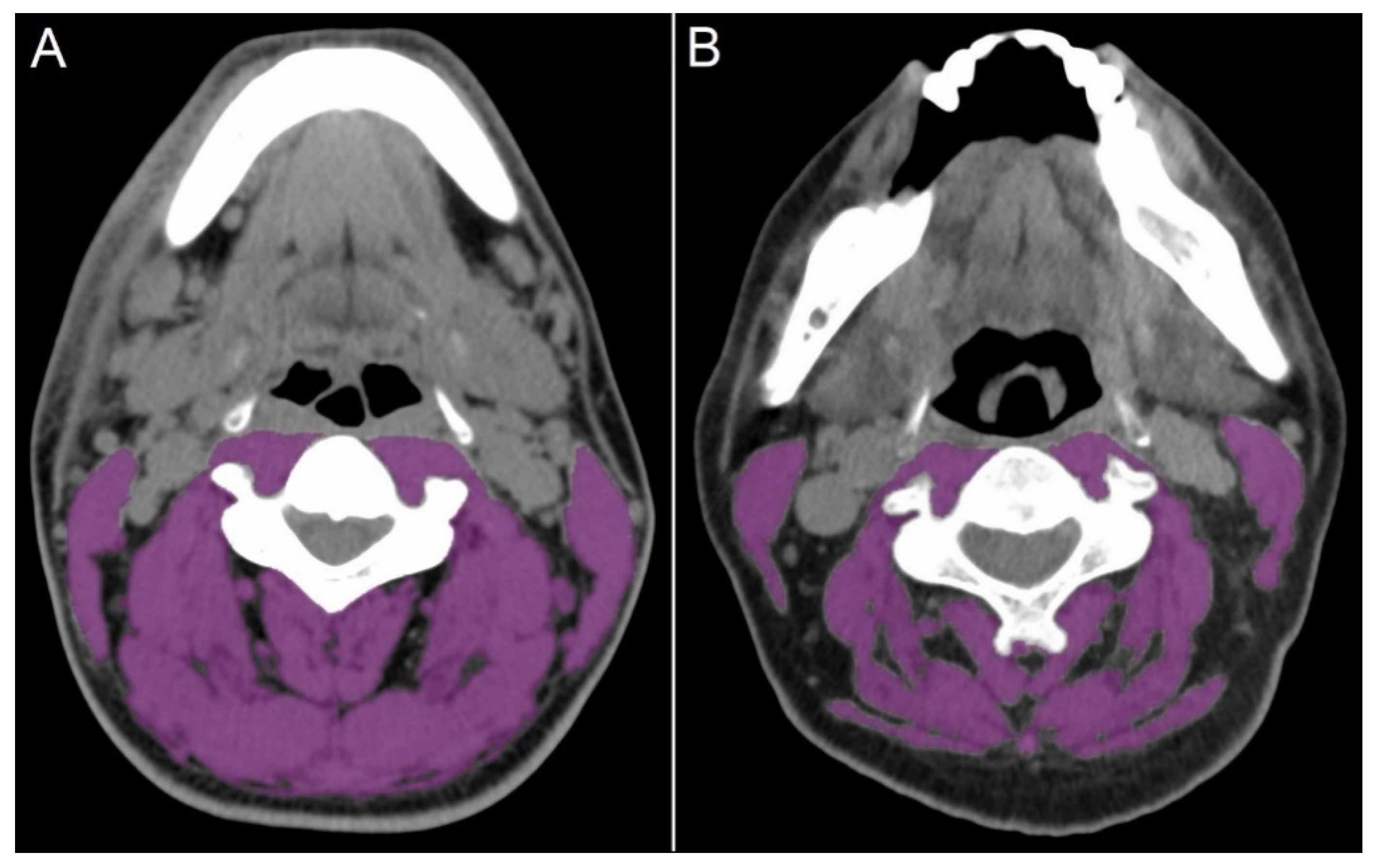
2.2. Definition of Sarcopenia, Frailty, and Inflammatory Status
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Hematologic Toxicities under CRT According to Sarcopenia and Frailty Status
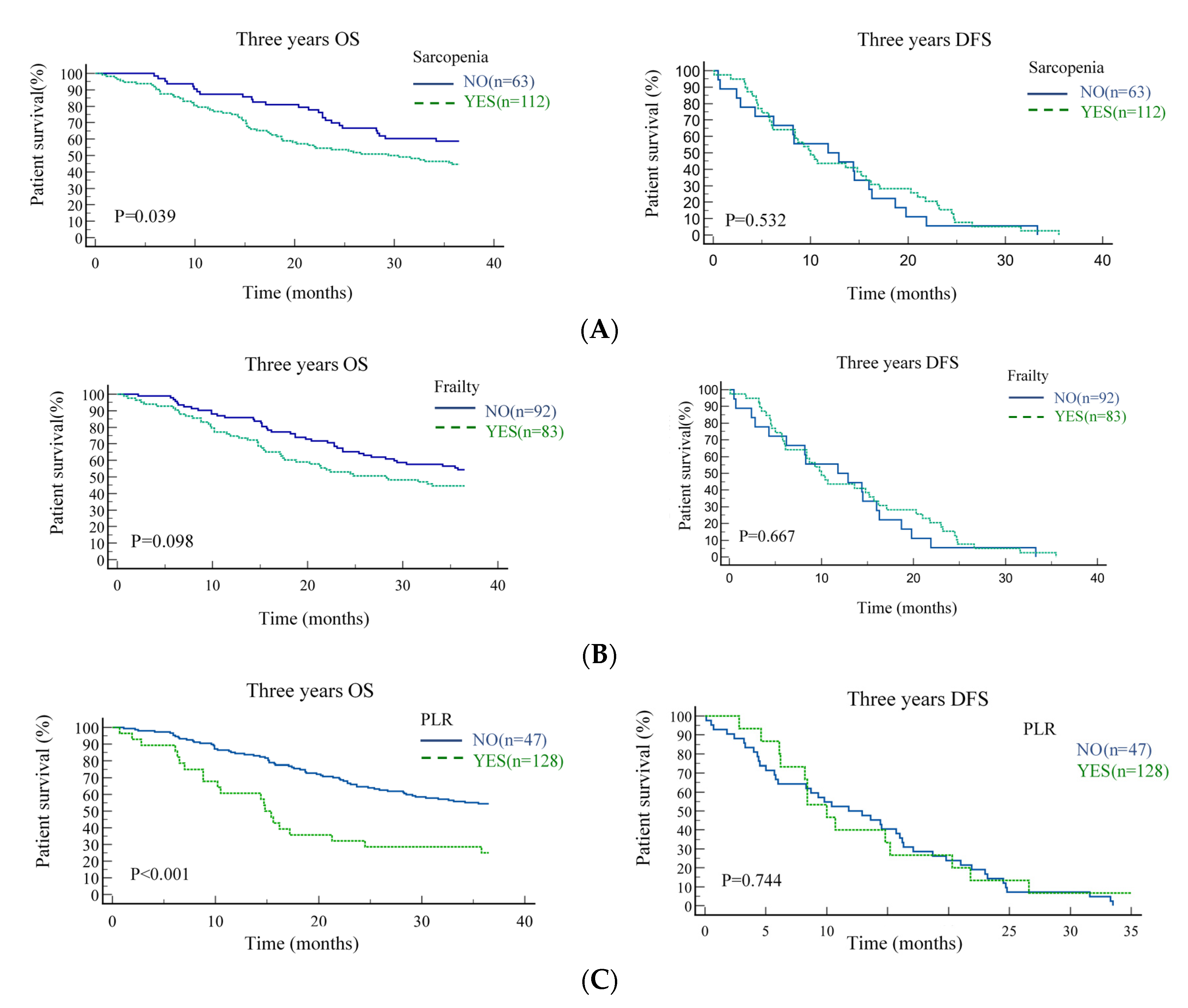
3.3. Survival Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Pfister, D.G.; Spencer, S.; Adelstein, D.; Adkins, D.; Anzai, Y.; Brizel, D.M.; Bruce, J.Y.; Bruce, P.M.; Caudell, J.Y.; Cmelak, T.; et al. Head and Neck Cancers, Version 2.2020, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2020, 18, 873–898. [Google Scholar] [CrossRef]
- Kim, D.; Li, R. Contemporary Treatment of Locally Advanced Oral Cancer. Curr. Treat. Options Oncol. 2019, 20, 32. [Google Scholar] [CrossRef]
- Cramer, J.D.; Johnson, J.T.; Nilsen, M.L. Pain in Head and Neck Cancer Survivors: Prevalence, Predictors, and Quality-of-Life Impact. Otolaryngol. Head Neck Surg. 2018, 159, 853–858. [Google Scholar] [CrossRef]
- Santilli, V.; Bernetti, A.; Mangone, M.; Paoloni, M. Clinical definition of sarcopenia. Clin. Cases Miner. Bone Metab. 2014, 11, 177–180. [Google Scholar] [CrossRef] [PubMed]
- Grossberg, A.J.; Chamchod, S.; Fuller, C.D.; Mohamed, A.S.; Heukelom, J.; Eichelberger, H.; Kantor, M.E.; Hutcheson, K.A.; Gunn, G.B.; Garden, A.S.; et al. Association of Body Composition with Survival and Locoregional Control of Radiotherapy-Treated Head and Neck Squamous Cell Carcinoma. JAMA Oncol. 2016, 2, 782–789. [Google Scholar] [CrossRef]
- Ganju, R.G.; Morse, R.; Hoover, A.; TenNapel, M.; Lominska, C.E. The impact of sarcopenia on tolerance of radiation and outcome in patients with head and neck cancer receiving chemoradiation. Radiother. Oncol. 2019, 137, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.; Zhu, D.; Kraus, D.; Tham, T. Radiologically Defined Sarcopenia Affects Survival in Head and Neck Cancer: A Meta-Analysis. Laryngoscope 2021, 131, 333–341. [Google Scholar] [CrossRef] [PubMed]
- Wendrich, A.W.; Swartz, J.E.; Bril, S.I.; Wegner, I.; de Graeff, A.; Smid, E.J.; Pothen, A.J. Low skeletal muscle mass is a predictive factor for chemotherapy dose-limiting toxicity in patients with locally advanced head and neck cancer. Oral Oncol. 2017, 71, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Achim, V.; Bash, J.; Mowery, A.; Guimaraes, A.R.; Li, R.; Schindler, J.; Wax, M.; Andersen, P.; Clayburghet, D. Prognostic Indication of Sarcopenia for Wound Complication After Total Laryngectomy. JAMA Otolaryngol. Head Neck Surg. 2017, 143, 1159–1165. [Google Scholar] [CrossRef] [Green Version]
- Bril, S.I.; Pezier, T.F.; Tijink, B.M.; Janssen, L.M.; Braunius, W.W.; de Bree, R. Preoperative low skeletal muscle mass as a risk factor for pharyngocutaneous fistula and decreased overall survival in patients undergoing total laryngectomy. Head Neck 2019, 41, 1745–1755. [Google Scholar] [CrossRef] [Green Version]
- Nishikawa, D.; Hanai, N.; Suzuki, H.; Koide, Y.; Beppu, S.; Hasegawa, Y. The Impact of Skeletal Muscle Depletion on Head and Neck Squamous Cell Carcinoma. ORL J. Otorhinolaryngol. Relat. Spec. 2018, 80, 1–9. [Google Scholar] [CrossRef]
- Ueno, H.; Hawrylowicz, C.M.; Banchereau, J. Immunological intervention in human diseases. J. Transl. Med. 2007, 5, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Szilasi, Z.; Jósa, V.; Zrubka, Z.; Mezei, T.; Vass, T.; Merkel, K.; Helfferich, F.; Baranyai, Z. Neutrophil-To-Lymphocyte and Platelet-To-Lymphocyte Ratios as Prognostic Markers of Survival in Patients with Head and Neck Tumours—Results of a Retrospective Multicentric Study. Int. J. Environ. Res. Public Health 2020, 17, 1742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Vries, N.M.; Staal, J.B.; van Ravensberg, C.D.; Hobbelen, J.S.; Olde Rikkert, M.G.; Nijhuis-van der Sanden, M.W. Outcome instruments to measure frailty: A systematic review. Ageing Res. Rev. 2011, 10, 104–114. [Google Scholar] [CrossRef] [PubMed]
- Dodds, R.; Sayer, A.A. Sarcopenia and frailty: New challenges for clinical practice. Clin. Med. 2016, 16, 455. [Google Scholar] [CrossRef]
- Ethun, C.G.; Bilen, M.A.; Jani, A.B.; Maithel, S.K.; Ogan, K.; Master, V.A. Frailty and cancer: Implications for oncology surgery, medical oncology, and radiation oncology. CA Cancer J. Clin. 2017, 67, 362–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldstein, D.P.; Sklar, M.C.; de Almeida, J.R.; Gilbert, R.; Gullane, P.; Irish, J.; Brown, D.; Higgins, K.; Enepekides, D.; Xu, W.; et al. Frailty as a predictor of outcomes in patients undergoing head and neck cancer surgery. Laryngoscope 2020, 130, E340–E345. [Google Scholar] [CrossRef]
- Abt, N.B.; Richmon, J.D.; Koch, W.M.; Eisele, D.W.; Agrawal, N. Assessment of the Predictive Value of the Modified Frailty Index for Clavien-Dindo Grade IV Critical Care Complications in Major Head and Neck Cancer Operations. JAMA Otolaryngol. Head Neck Surg. 2016, 142, 658–664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adams, P.; Ghanem, T.; Stachler, R.; Hall, F.; Velanovich, V.; Rubinfeld, I. Frailty as a predictor of morbidity and mortality in inpatient head and neck surgery. JAMA Otolaryngol. Head Neck Surg. 2013, 139, 783–789. [Google Scholar] [CrossRef] [Green Version]
- Wachal, B.; Johnson, M.; Burchell, A.; Sayles, H.; Rieke, K.; Lindau, R.; Lydiatt, W.; Panwaret, A. Association of Modified Frailty Index Score With Perioperative Risk for Patients Undergoing Total Laryngectomy. JAMA Otolaryngol. Head Neck Surg. 2017, 143, 818–823. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.H.; Chao, K.S.; Leu, Y.S.; Lee, J.C.; Liu, C.J.; Huang, Y.C.; Chang, Y.F.; Chen, W.H.; Tsai, J.T.; Chen, Y.J. Guideline and preliminary clinical practice results for dose specification and target delineation for postoperative radiotherapy for oral cavity cancer. Head Neck 2015, 37, 933–939. [Google Scholar] [CrossRef]
- National Cancer Institute (NCI). Common Terminology Criteria for Adverse Events (CTCAE) v5.0 U.S. Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/ctc.htm#ctc_50 (accessed on 21 February 2021).
- Heymsfield, S.B.; Wang, Z.; Baumgartner, R.N.; Ross, R. Human body composition: Advances in models and methods. Annu. Rev. Nutr. 1997, 17, 527–558. [Google Scholar] [CrossRef]
- Swartz, J.E.; Pothen, A.J.; Wegner, I.; Smid, E.J.; Swart, K.M.; de Bree, R.; Leenen, L.P.H.; Grolman, W. Feasibility of using head and neck CT imaging to assess skeletal muscle mass in head and neck cancer patients. Oral Oncol. 2016, 62, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Ufuk, F.; Herek, D.; Yüksel, D. Diagnosis of Sarcopenia in Head and Neck Computed Tomography: Cervical Muscle Mass as a Strong Indicator of Sarcopenia. Clin. Exp. Otorhinolaryngol. 2019, 12, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Van Rijn-Dekker, M.I.; van den Bosch, L.; van den Hoek, J.G.M.; Bijl, H.P.; van Aken, E.S.M.; van der Hoorn, A.; Oosting, S.F.; Halmos, H.G.; Witjes, M.J.H.; van der Laan, H.P.; et al. Impact of sarcopenia on survival and late toxicity in head and neck cancer patients treated with radiotherapy. Radiother. Oncol. 2020, 147, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Rosset, A.; Spadola, L.; Ratib, O. OsiriX: An open-source software for navigating in multidimensional DICOM images. J. Digit. Imaging 2004, 17, 205–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Velanovich, V.; Antoine, H.; Swartz, A.; Peters, D.; Rubinfeld, I. Accumulating deficits model of frailty and postoperative mortality and morbidity: Its application to a national database. J. Surg. Res. 2013, 183, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Hermiz, S.J.R.; Lauzon, S.; Brown, G.; Herrera, F.A. Use of a 5-Item Modified Frailty Index for Risk Stratification in Patients Undergoing Breast Reconstruction. Ann. Plast Surg. 2021, 86, S615–S621. [Google Scholar] [CrossRef] [PubMed]
- Subramaniam, S.; Aalberg, J.J.; Soriano, R.P.; Divino, C.M. New 5-Factor Modified Frailty Index Using American College of Surgeons NSQIP Data. J. Am. Coll. Surg. 2018, 226, 173–181. [Google Scholar] [CrossRef]
- Chimukangara, M.; Helm, M.C.; Frelich, M.J.; Bosler, M.E.; Rein, L.E.; Szabo, A.; Gould, J.C. A 5-item frailty index based on NSQIP data correlates with outcomes following paraesophageal hernia repair. Surg. Endosc. 2017, 31, 2509–2519. [Google Scholar] [CrossRef]
- Youden, W.J. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]
- Zhang, Y.; Zheng, L.; Quan, L.; Du, L. Prognostic role of platelet-to-lymphocyte ratio in oral cancer: A meta-analysis. J. Oral Pathol. Med. 2021, 50, 274–279. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Liu, S.H.; Dai, K.Y.; Huang, Y.M.; Li, C.; Chen, J.C.; Leu, Y.S.; Liu, C.J.; Chen, Y.J. Sarcopenia and Systemic Inflammation Synergistically Impact Survival in Oral Cavity Cancer. Laryngoscope 2021, 131, E1530–E1538. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.H.; Lue, K.H.; Hsieh, T.C.; Liu, S.H.; Wang, T.F.; Peng, T.C. Association between sarcopenia and clinical outcomes in patients with esophageal cancer under neoadjuvant therapy. Anticancer. Res. 2020, 40, 1175–1181. [Google Scholar] [CrossRef]
- Posner, M.R.; Hershock, D.M.; Blajman, C.R.; Mickiewicz, E.; Winquist, E.; Gorbounova, V.; Tjulandin, S.; Shin, D.M.; Cullen, K.; Ervin, T.J.; et al. Cisplatin and fluorouracil alone or with docetaxel in head and neck cancer. N. Engl. J. Med. 2007, 357, 1705–1715. [Google Scholar] [CrossRef] [Green Version]
- Ganz, T. Anemia of Inflammation. N. Engl. J. Med. 2019, 381, 1148–1157. [Google Scholar] [CrossRef] [PubMed]
- Chindapasirt, J. Sarcopenia in Cancer Patients. Asian Pac. J. Cancer Prev. 2015, 16, 8075–8077. [Google Scholar] [CrossRef] [Green Version]
- Mhadgut, H.; Galadima, H.; Tahhan, H.R. Thrombocytosis in iron deficiency anemia. Blood 2018, 132, 4985. [Google Scholar] [CrossRef]
- Franco, A.T.; Corken, A.; Ware, J. Platelets at the interface of thrombosis, inflammation, and cancer. Blood 2015, 126, 582–588. [Google Scholar] [CrossRef] [Green Version]
- Chow, L.Q.M. Head and Neck Cancer. N. Engl. J. Med. 2020, 38, 60–72. [Google Scholar] [CrossRef] [PubMed]
- Rittberg, R.; Zhang, H.; Lambert, P.; Kudlovich, R.; Kim, C.A.; Dawe, D.E. Utility of the modified frailty index in predicting toxicity and cancer outcomes for older adults with advanced pancreatic cancer receiving first-line palliative chemotherapy. J. Geriatr. Oncol. 2021, 12, 112–117. [Google Scholar] [CrossRef] [PubMed]
- Handforth, C.; Clegg, A.; Young, C.; Simpkins, S.; Seymour, M.T.; Selby, P.J.; Young, J. The prevalence and outcomes of frailty in older cancer patients: A systematic review. Ann. Oncol 2015, 26, 1091–1101. [Google Scholar] [CrossRef]
- Van Deudekom, F.J.; Schimberg, A.S.; Kallenberg, M.H.; Slingerland, M.; van der Velden, L.A.; Mooijaart, S.P. Functional and cognitive impairment, social environment, frailty and adverse health outcomes in older patients with head and neck cancer, a systematic review. Oral Oncol. 2017, 64, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Zwart, A.T.; Becker, J.N.; Lamers, M.J.; Dierckx, R.A.J.O.; de Bock, G.H.; Halmos, G.B.; van der Hoorn, A. Skeletal muscle mass and sarcopenia can be determined with 1.5-T and 3-T neck MRI scans, in the event that no neck CT scan is performed. Eur. Radiol. 2021, 31, 4053–4062. [Google Scholar] [CrossRef] [PubMed]
- Bernier, J.; Domenge, C.; Ozsahin, M.; Matuszewska, K.; Lefèbvre, J.L.; Greiner, R.H.; Giralt, J.; Maingon, P.; Rol land, F.; Bolla, M.; et al. Postoperative irradiation with or without concomitant chemotherapy for locally advanced head and neck cancer. N. Engl. J. Med. 2004, 350, 1945–1952. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variable | Total (n = 175) | Sarcopenia (n = 112) | No Sarcopenia (n = 63) | p |
|---|---|---|---|---|
| Age, years | ||||
| Mean (SD) | 53.9 (9.9) | 54 (9.5) | 54 (10.4) | 0.384 |
| Sex, n (%) | ||||
| Male | 151 (86.3) | 112 (100) | 39 (61.9) | <0.001 |
| Female | 24 (13.7) | 0 (0) | 24 (38.1) | |
| Alcohol, n (%) | ||||
| Never drinker | 40 (22.9) | 19 (16.9) | 21 (33.3) | 0.031 |
| Ever drinker | 135 (77.1) | 93 (83.1) | 42 (66.7) | |
| Smoking, n (%) | ||||
| Never drinker | 34 (19.4) | 22 (19.6) | 11 (17.4) | 0.592 |
| Ever drinker | 141 (80.6) | 90 (80.4) | 52 (82.6) | |
| Betel nut, n (%) | ||||
| Never chewing | 35 (20.0) | 18 (16.1) | 17 (26.9) | 0.101 |
| Ever chewing | 140 (80.0) | 94 (83.9) | 46 (73.1) | |
| mFI-5 | ||||
| 0 | 92 (52.5) | 52 (46.4) | 38 (60.3) | 0.031 |
| 1 | 57 (32.6) | 37 (33.0) | 20 (31.8) | |
| ≥2 | 26 (14.9) | 23 (20.6) | 5 (7.9) | |
| Cancer site | ||||
| Buccal | 58 (33.1) | 37 (33.0) | 21 (33.3) | 0.080 |
| Lower gum | 27 (15.4) | 17 (15.1) | 10 (15.9) | |
| Tongue | 59 (33.7) | 33 (29.4) | 26 (41.3) | |
| Other sites | 31 (17.8) | 25 (22.5) | 6 (9.5) | |
| Clinical Stage | ||||
| I | 16 (9.1) | 9 (8.0) | 7 (11.1) | 0.624 |
| II | 38 (21.7) | 23 (20.5) | 15 (23.8) | |
| III | 10 (5.7) | 5 (4.5) | 5 (7.9) | |
| IV | 111 (63.5) | 75 (67.0) | 36 (57.2) | |
| PNI | ||||
| Negative | 79 (45.1) | 50 (44.6) | 29 (46.0) | 0.947 |
| Positive | 96 (54.9) | 62 (55.4) | 34 (54.0) | |
| LVI | ||||
| Negative | 80 (45.7) | 53 (47.3) | 27 (42.9) | 0.451 |
| Positive | 95 (54.3) | 59 (52.7) | 36 (57.1) | |
| ECS | ||||
| Negative | 130 (74.3) | 82 (73.2) | 48 (76.2) | 0.702 |
| Positive | 45 (25.7) | 30 (26.8) | 15 (23.8) | |
| BMI, kg/m2 | ||||
| Mean (SD) | 25.2 (5.3) | 23.6 (3.4) | 28.1 (5.5) | <0.001 |
| Albumin | ||||
| Median (IQR) | 3.4 (3.1–3.7) | 3.4 (3.1–3.7) | 3.4 (3.1–3.7) | 0.610 |
| SMI, cm2/m2 | ||||
| Mean ± SD | 42.9 (8.8) | 38.8 (5.7) | 49.6 (8.1) | <0.001 |
| Hemoglobin | ||||
| Mean ± SD | 11.4 (1.9) | 11.5 (1.9) | 11.0 (1.6) | 0.754 |
| NLR | ||||
| Median (IQR) | 3.4 (2.2–5.3) | 3.9 (2.2–6.6) | 3.3 (2.2–4.8) | 0.072 |
| PLR | ||||
| Median (IQR) | 223.2 (142.7–341.4) | 228.7 (147.8–347.3) | 218.2 (142.6–326.6) | 0.652 |
| Toxicities | Sarcopenia (n = 112) | No Sarcopenia (n = 63) | p | mFI-5 ≥ 1 (n = 83) | mFI-5 = 0 (n = 92) | p |
|---|---|---|---|---|---|---|
| Anemia n (%) | ||||||
| Grade 0–2 | 92 (82.1) | 59 (93.6) | 0.021 | 71 (85.5) | 80 (86.6) | 0.841 |
| Grade 3–4 | 20 (17.9) | 4 (6.4) | 12 (14.5) | 12 (13.4) | ||
| Febrile neutropenia n (%) | ||||||
| Grade 0–2 | 104 (92.9) | 61 (96.8) | 0.110 | 80 (96.4) | 87 (94.5) | 0.384 |
| Grade 3-4 | 8 (7.1) | 2 (3.2) | 3 (3.6) | 5 (5.5) | ||
| Infection n (%) | ||||||
| Grade 0–2 | 95 (84.8) | 57 (90.5) | 0.181 | 72 (86.7) | 80 (86.9) | 0.605 |
| Grade 3–4 | 17 (15.2) | 6 (9.5) | 11 (13.3) | 12 (13.1) | ||
| Univariate | Multivariate | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Anemia | Febrile Neutropenia | Infection | Anemia | |||||||||
| OR | 95% CI | p | OR | 95% CI | p | OR | 95% CI | p | OR | 95% CI | p | |
| Age (≤65 vs. >65) | 0.921 | (0.514–1.528) | 0.780 | 0.921 | (0.524–1.582) | 0.781 | 1.625 | (0.75–3.62) | 0.201 | |||
| Stage (I–II vs. III–IV) | 0.918 | (0.325–2.703) | 0.971 | 1.612 | (0.332–8.090) | 0.554 | 2.118 | (0.70–6.79) | 0.172 | |||
| Sarcopenia (no vs. yes) | 1.739 | (1.931–3.107) | 0.040 | 0.835 | (0.567–1.471) | 0.532 | 2.024 | (0.71–5.82) | 0.187 | 1.871 | (1.051–3.320) | 0.040 |
| Hb (>11 vs. ≤11) | 3.326 | (1.171–9.615) | 0.021 | 1.217 | (0.276–5.610) | 0.805 | 3.010 | (1.16–7.77) | 0.023 | 2.821 | (0.925–8.208) | 0.058 |
| NLR (≤3.4 vs. >3.4) | 3.622 | (1.278–10.02) | 0.011 | 0.835 | (0.116–4.529) | 0.853 | 1.714 | (0.68–4.46) | 0.241 | |||
| PLR (≤385 vs. >385) | 2.018 | (0.616–6.448) | 0.204 | 0.922 | (0.542–1.835) | 0.781 | 1.349 | (0.49–4.49) | 0.473 | 3.102 | (1.017–8.912) | 0.033 |
| Overall Survival | Disease-Free Survival | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Univariate | Multivariate | Univariate | |||||||
| HR | 95% CI | p | HR | 95% CI | p | HR | 95% CI | p | |
| Age | 0.990 | (0.861–1.622) | 0.918 | 0.972 | (0.915–1.215) | 0.072 | |||
| Stage (I–II vs. III–IV) | 2.352 | (1.415–3.180) | <0.001 | 1.820 | (1.201–3.323) | 0.042 | 1.464 | (0.812–2.670) | 1.195 |
| PNI (negative vs. positive) | 1.631 | (1.104–2.423) | 0.011 | 1.114 | (0.713–1.779) | 0.542 | 1.163 | (0.925–2.580) | 0.061 |
| LVI (negative vs. positive) | 1.172 | (0.709–1.731) | 0.410 | 1.513 | (0.819–2.460) | 0.112 | |||
| ECS (negative vs. positive) | 1.727 | (1.122–2.624) | 0.014 | 1.505 | (0.971–2.461) | 0.068 | 1.125 | (0.710–2.204) | 0.443 |
| mFI (0 vs. ≥1) | 1.273 | (0.781–2.108) | 0.321 | 1.718 | (0.921–3.590) | 0.692 | |||
| BMI (≥18.5 vs. <18.5 kg/m2) | 2.005 | (0.819–4.710) | 0.082 | 0.823 | (0.471–1.487) | 0.543 | |||
| Sarcopenia (no vs. yes) | 1.745 | (1.123–2.627) | 0.016 | 1.643 | (1.202–2.670) | 0.034 | 2.623 | (0.912–4.570) | 0.532 |
| Hb (≤11 vs. >11) | 0.906 | (0.48–2.411) | 0.896 | 0.619 | (0.317–1.249) | 0.251 | |||
| NLR (≤3.4 vs. >3.4) | 1.793 | (1.116–2.176) | <0.001 | 1.006 | (0.529–1.772) | 0.974 | 1.607 | (0.732–3.540) | 0.232 |
| PLR (≤385 vs. >385) | 2.620 | (1.610–4.213) | <0.001 | 1.983 | (1.206–2.553) | 0.033 | 2.205 | (0.876–2.182) | 0.748 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, C.-H.; Chen, P.-R.; Lue, K.-H.; Hsieh, T.-C.; Chou, Y.-F. Evaluation of Sarcopenia, Frailty, and Inflammation on Adverse Events and Survival Outcomes in Patients with Oral Cavity Squamous Cell Carcinoma under Adjuvant Chemoradiotherapy. J. Pers. Med. 2021, 11, 936. https://doi.org/10.3390/jpm11090936
Huang C-H, Chen P-R, Lue K-H, Hsieh T-C, Chou Y-F. Evaluation of Sarcopenia, Frailty, and Inflammation on Adverse Events and Survival Outcomes in Patients with Oral Cavity Squamous Cell Carcinoma under Adjuvant Chemoradiotherapy. Journal of Personalized Medicine. 2021; 11(9):936. https://doi.org/10.3390/jpm11090936
Chicago/Turabian StyleHuang, Chun-Hou, Peir-Rorg Chen, Kun-Han Lue, Tsung-Cheng Hsieh, and Yu-Fu Chou. 2021. "Evaluation of Sarcopenia, Frailty, and Inflammation on Adverse Events and Survival Outcomes in Patients with Oral Cavity Squamous Cell Carcinoma under Adjuvant Chemoradiotherapy" Journal of Personalized Medicine 11, no. 9: 936. https://doi.org/10.3390/jpm11090936