
Colchicine Use and Risks of Stroke Recurrence in Acute Non-Cardiogenic Ischemic Stroke Patients: A Population-Based Cohort Study

 , , ,
, , ,
Abstract
:
1. Introduction
2. Methods
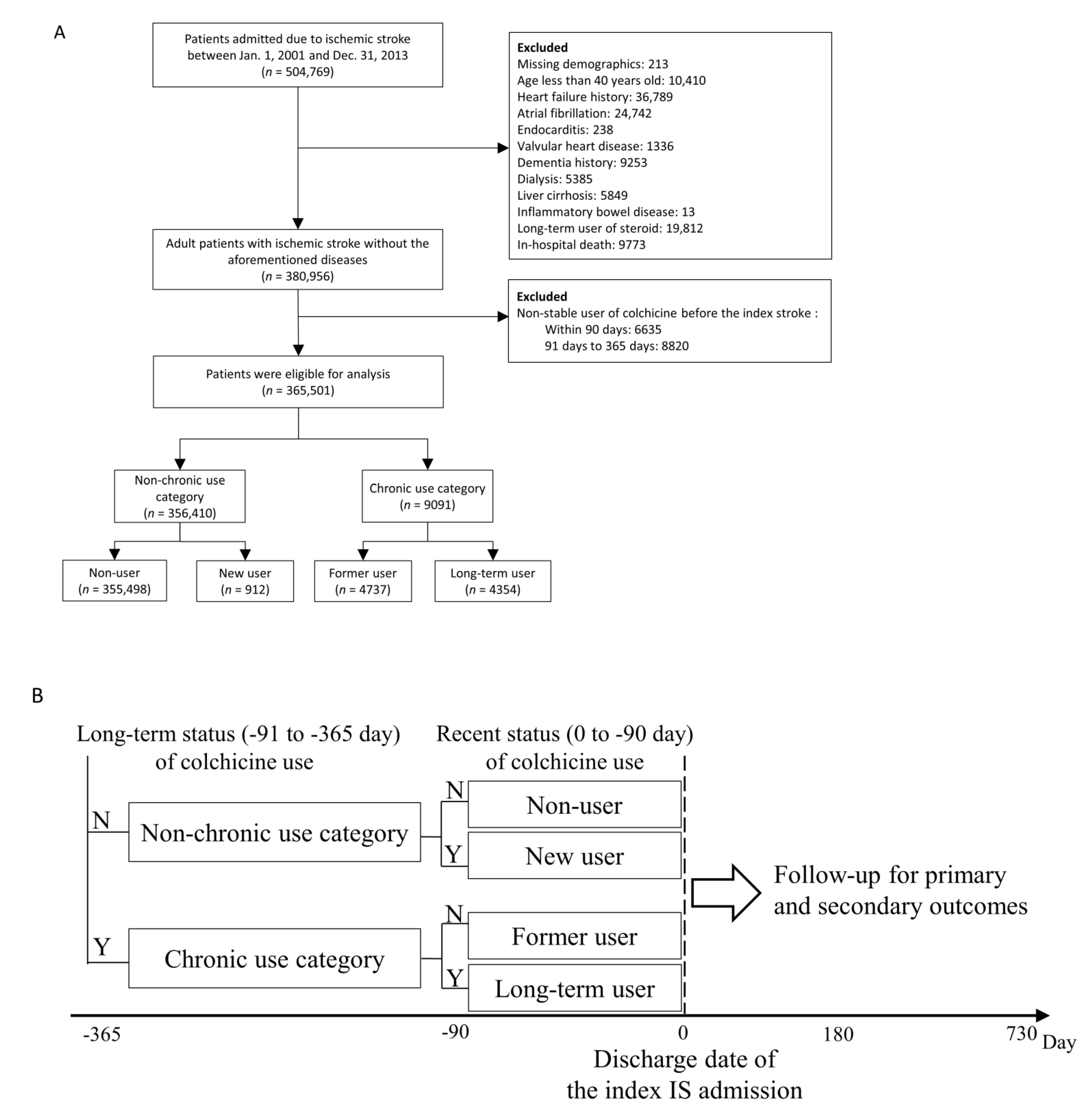
2.1. Data Source and Patient Identification
2.2. Exposure to the Study Drug
2.3. Covariates
2.4. Outcome Measurement
2.5. Statistical Analysis
3. Results
3.1. Study Patients
3.2. Baseline Characteristics
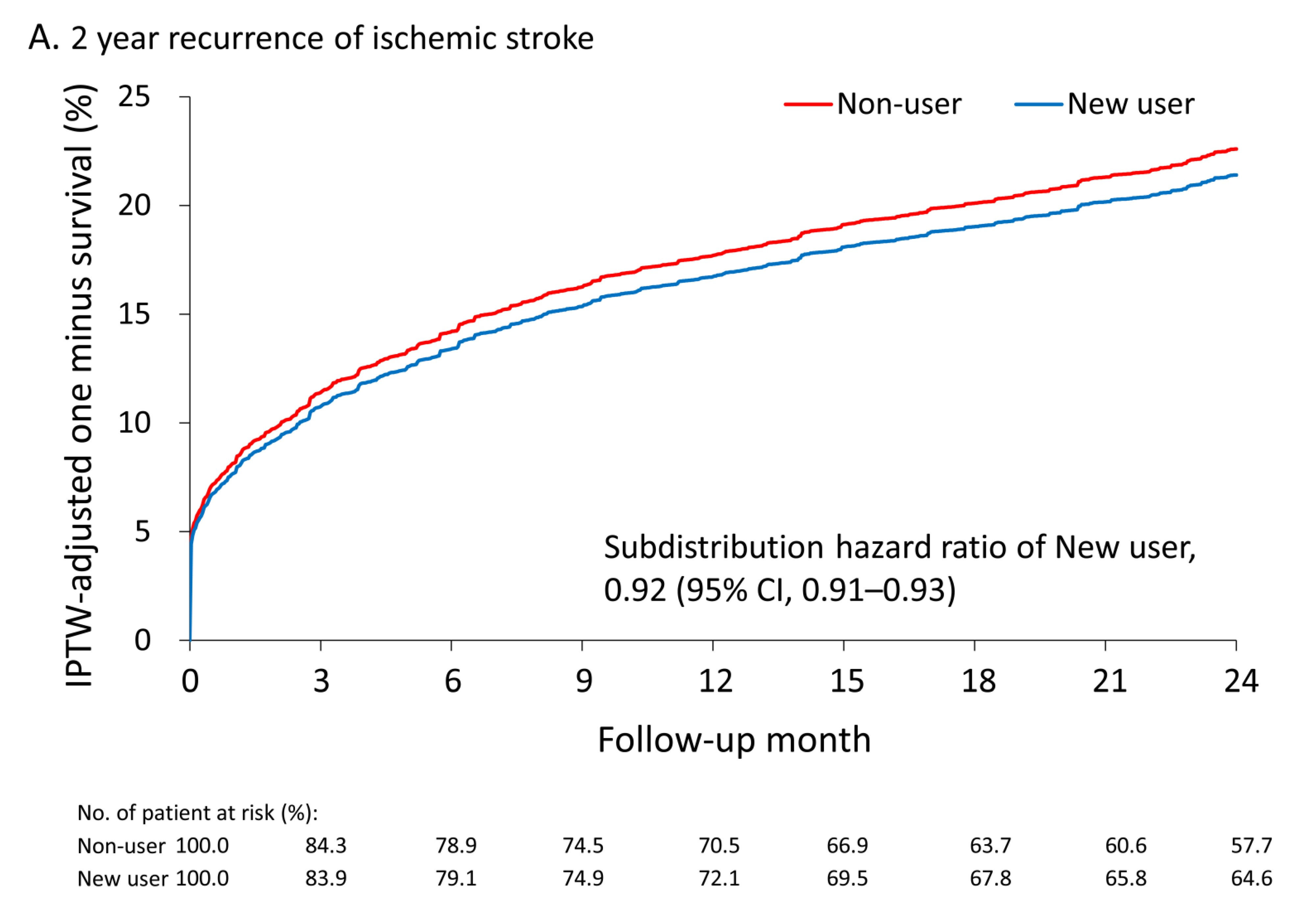
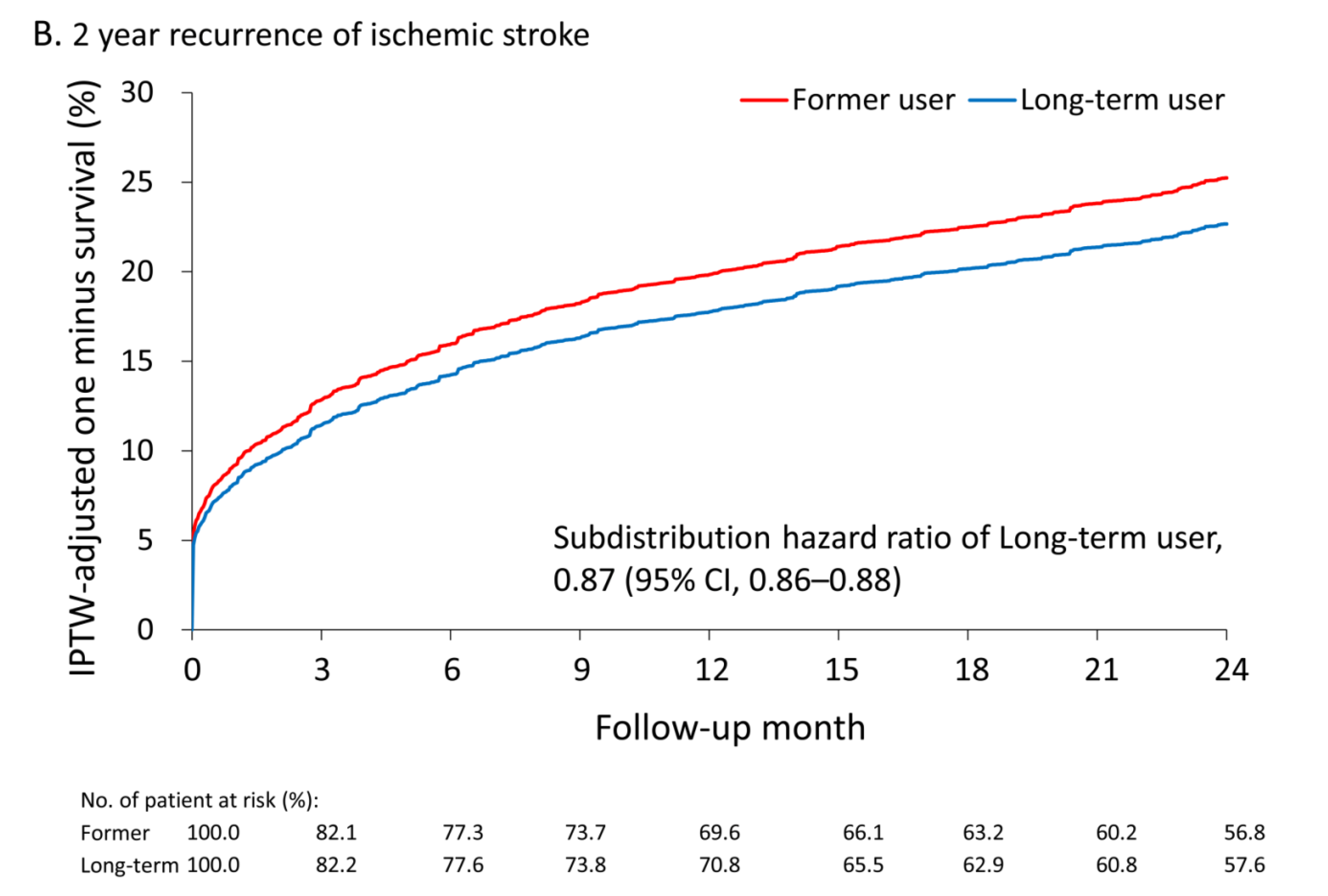
3.3. Primary Outcome
3.4. Secondary Outcomes
3.5. Subgroup Analyses for the Risk of Recurrent IS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kernan, W.N.; Ovbiagele, B.; Black, H.R.; Bravata, D.M.; Chimowitz, M.I.; Ezekowitz, M.D.; Fang, M.C.; Fisher, M.; Furie, K.L.; Heck, D.V.; et al. Guidelines for the prevention of stroke in patients with stroke and transient ischemic attack: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2014, 45, 2160–2236. [Google Scholar] [CrossRef]
- Hankey, G.J. Secondary stroke prevention. Lancet Neurol. 2014, 13, 178–194. [Google Scholar] [CrossRef]
- Kelly, P.J.; Murphy, S.; Coveney, S.; Purroy, F.; Lemmens, R.; Tsivgoulis, G.; Price, C. Anti-inflammatory approaches to ischaemic stroke prevention. J. Neurol. Neurosurg. Psychiatry 2018, 89, 211–218. [Google Scholar] [CrossRef]
- Thompson, P.L.; Nidorf, S.M. Colchicine: An affordable anti-inflammatory agent for atherosclerosis. Curr. Opin. Lipidol. 2018, 29, 467–473. [Google Scholar] [CrossRef]
- Stone, N.J.; Robinson, J.G.; Lichtenstein, A.H.; Bairey Merz, C.N.; Blum, C.B.; Eckel, R.H.; Goldberg, A.C.; Gordon, D.; Levy, D.; Lloyd-Jones, D.M.; et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014, 129, S1–S45. [Google Scholar] [CrossRef] [PubMed]
- Amarenco, P.; Kim, J.S.; Labreuche, J.; Charles, H.; Abtan, J.; Bejot, Y.; Cabrejo, L.; Cha, J.K.; Ducrocq, G.; Giroud, M.; et al. A Comparison of Two LDL Cholesterol Targets after Ischemic Stroke. N. Engl. J. Med. 2020, 382, 9. [Google Scholar] [CrossRef] [PubMed]
- Tardif, J.C.; Kouz, S.; Waters, D.D.; Bertrand, O.F.; Diaz, R.; Maggioni, A.P.; Pinto, F.J.; Ibrahim, R.; Gamra, H.; Kiwan, G.S.; et al. Efficacy and Safety of Low-Dose Colchicine after Myocardial Infarction. N. Engl. J. Med. 2019, 381, 2497–2505. [Google Scholar] [CrossRef] [PubMed]
- Nidorf, S.M.; Eikelboom, J.W.; Budgeon, C.A.; Thompson, P.L. Low-dose colchicine for secondary prevention of cardiovascular disease. J. Am. Coll. Cardiol. 2013, 61, 404–410. [Google Scholar] [CrossRef]
- Solomon, D.H.; Liu, C.C.; Kuo, I.H.; Zak, A.; Kim, S.C. Effects of colchicine on risk of cardiovascular events and mortality among patients with gout: A cohort study using electronic medical records linked with Medicare claims. Ann. Rheum. Dis. 2016, 75, 1674–1679. [Google Scholar] [CrossRef]
- Katsanos, A.H.; Palaiodimou, L.; Price, C.; Giannopoulos, S.; Lemmens, R.; Kosmidou, M.; Georgakis, M.K.; Weimar, C.; Kelly, P.J.; Tsivgoulis, G. Colchicine for stroke prevention in patients with coronary artery disease: A systematic review and meta-analysis. Eur. J. Neurol. 2020, 27, 1035–1038. [Google Scholar] [CrossRef]
- Andreis, A.; Imazio, M.; Piroli, F.; Avondo, S.; Casula, M.; Paneva, E.; De Ferrari, G.M. Efficacy and safety of colchicine for the prevention of major cardiovascular and cerebrovascular events in patients with coronary artery disease: A systematic review and meta-analysis on 12,869 patients. Eur. J. Prev. Cardiol. Epub ahead of print. 2021. [Google Scholar] [CrossRef] [PubMed]
- Fiolet, A.T.L.; Opstal, T.S.J.; Mosterd, A.; Eikelboom, J.W.; Jolly, S.S.; Keech, A.C.; Kelly, P.; Tong, D.C.; Layland, J.; Nidorf, S.M.; et al. Efficacy and safety of low-dose colchicine in patients with coronary disease: A systematic review and meta-analysis of randomized trials. Eur. Heart J. 2021, 42, 2765–2775. [Google Scholar] [CrossRef] [PubMed]
- Samuel, M.; Tardif, J.C.; Bouabdallaoui, N.; Khairy, P.; Dube, M.P.; Blondeau, L.; Guertin, M.C. Colchicine for Secondary Prevention of Cardiovascular Disease: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Can. J. Cardiol. 2021, 37, 776–785. [Google Scholar] [CrossRef]
- Hsieh, C.Y.; Chen, C.H.; Li, C.Y.; Lai, M.L. Validating the diagnosis of acute ischemic stroke in a National Health Insurance claims database. J. Formos Med. Assoc. 2015, 114, 254–259. [Google Scholar] [CrossRef]
- Hsieh, C.Y.; Su, C.C.; Shao, S.C.; Sung, S.F.; Lin, S.J.; Kao Yang, Y.H.; Lai, E.C. Taiwan’s National Health Insurance Research Database: Past and future. Clin. Epidemiol. 2019, 11, 349–358. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.H.; Chen, T.H.; Lin, M.S.; Hung, M.J.; Chung, C.M.; Cherng, W.J.; Lee, T.H.; Lin, Y.S. Ezetimibe-Simvastatin Therapy Reduce Recurrent Ischemic Stroke Risks in Type 2 Diabetic Patients. J. Clin. Endocrinol. Metab. 2016, 101, 2994–3001. [Google Scholar] [CrossRef]
- Tagalakis, V.; Eberg, M.; Kahn, S.; Azoulay, L. Use of statins and reduced risk of recurrence of VTE in an older population. A population-based cohort study. Thromb. Haemost. 2016, 115, 1220–1228. [Google Scholar]
- Schmidt, M.; Cannegieter, S.C.; Johannesdottir, S.A.; Dekkers, O.M.; Horvath-Puho, E.; Sorensen, H.T. Statin use and venous thromboembolism recurrence: A combined nationwide cohort and nested case-control study. J. Thromb. Haemost. 2014, 12, 1207–1215. [Google Scholar] [CrossRef]
- Wu, C.S.; Lai, M.S.; Gau, S.S.; Wang, S.C.; Tsai, H.J. Concordance between patient self-reports and claims data on clinical diagnoses, medication use, and health system utilization in Taiwan. PLoS ONE 2014, 9, e112257. [Google Scholar] [CrossRef]
- Liu, C.H.; Lee, T.H.; Lin, Y.S.; Sung, P.S.; Wei, Y.C.; Li, Y.R. Pioglitazone and PPAR-gamma modulating treatment in hypertensive and type 2 diabetic patients after ischemic stroke: A national cohort study. Cardiovasc. Diabetol. 2020, 19, 2. [Google Scholar] [CrossRef]
- Sung, S.F.; Hsieh, C.Y.; Lin, H.J.; Chen, Y.W.; Chen, C.H.; Kao Yang, Y.H.; Hu, Y.H. Validity of a stroke severity index for administrative claims data research: A retrospective cohort study. BMC Health Serv. Res. 2016, 16, 509. [Google Scholar] [CrossRef]
- Chen, Y.L.; Wang, H.T.; Chen, H.C.; Liu, W.H.; Hsueh, S.; Chung, W.J.; Wu, P.J.; Liu, C.H.; Chung, C.M.; Lin, Y.S. A risk stratification scoring system for new-onset atrial fibrillation after ischemic stroke: A National cohort study. Medicine 2020, 99, e20881. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.H.; Lin, Y.S.; Chi, C.C.; Liou, C.W.; Lee, J.D.; Peng, T.I.; Lee, T.H. Choices for long-term hypertensive control in patients after first-ever hemorrhagic stroke: A nationwide cohort study. Ther. Adv. Neurol. Disord. 2018, 11, 1756286418802688. [Google Scholar] [CrossRef] [PubMed]
- McCaffrey, D.F.; Griffin, B.A.; Almirall, D.; Slaughter, M.E.; Ramchand, R.; Burgette, L.F. A tutorial on propensity score estimation for multiple treatments using generalized boosted models. Stat. Med. 2013, 32, 3388–3414. [Google Scholar] [CrossRef]
- Nidorf, S.M.; Fiolet, A.T.L.; Mosterd, A.; Eikelboom, J.W.; Schut, A.; Opstal, T.S.J.; The, S.H.K.; Xu, X.F.; Ireland, M.A.; Lenderink, T.; et al. Colchicine in Patients with Chronic Coronary Disease. N. Engl. J. Med. 2020, 383, 1838–1847. [Google Scholar] [CrossRef]
- Marnane, M.; Prendeville, S.; McDonnell, C.; Noone, I.; Barry, M.; Crowe, M.; Mulligan, N.; Kelly, P.J. Plaque inflammation and unstable morphology are associated with early stroke recurrence in symptomatic carotid stenosis. Stroke 2014, 45, 801–806. [Google Scholar] [CrossRef]
- Leung, Y.Y.; Yao Hui, L.L.; Kraus, V.B. Colchicine—Update on mechanisms of action and therapeutic uses. Semin. Arthritis Rheum. 2015, 45, 341–350. [Google Scholar] [CrossRef]
- Fanola, C.L.; Morrow, D.A.; Cannon, C.P.; Jarolim, P.; Lukas, M.A.; Bode, C.; Hochman, J.S.; Goodrich, E.L.; Braunwald, E.; O’Donoghue, M.L. Interleukin-6 and the Risk of Adverse Outcomes in Patients after an Acute Coronary Syndrome: Observations From the SOLID-TIMI 52 (Stabilization of Plaque Using Darapladib-Thrombolysis in Myocardial Infarction 52) Trial. J. Am. Heart Assoc. 2017, 6, e005637. [Google Scholar] [CrossRef]
- Whiteley, W.; Jackson, C.; Lewis, S.; Lowe, G.; Rumley, A.; Sandercock, P.; Wardlaw, J.; Dennis, M.; Sudlow, C. Association of circulating inflammatory markers with recurrent vascular events after stroke: A prospective cohort study. Stroke 2011, 42, 10–16. [Google Scholar] [CrossRef]
- Segal, H.C.; Burgess, A.I.; Poole, D.L.; Mehta, Z.; Silver, L.E.; Rothwell, P.M. Population-based study of blood biomarkers in prediction of subacute recurrent stroke. Stroke 2014, 45, 2912–2917. [Google Scholar] [CrossRef] [PubMed]
- Jashari, F.; Ibrahimi, P.; Nicoll, R.; Bajraktari, G.; Wester, P.; Henein, M.Y. Coronary and carotid atherosclerosis: Similarities and differences. Atherosclerosis 2013, 227, 193–200. [Google Scholar] [CrossRef]
- Abu Mellal, A.; Hussain, N.; Said, A.S. The clinical significance of statins-macrolides interaction: Comprehensive review of in vivo studies, case reports, and population studies. Ther. Clin. Risk Manag. 2019, 15, 921–936. [Google Scholar] [CrossRef]
- Tsai, C.F.; Thomas, B.; Sudlow, C.L. Epidemiology of stroke and its subtypes in Chinese vs white populations: A systematic review. Neurology 2013, 81, 264–272. [Google Scholar] [CrossRef]
- Amarenco, P.; Albers, G.W.; Denison, H.; Easton, J.D.; Evans, S.R.; Held, P.; Hill, M.D.; Jonasson, J.; Kasner, S.E.; Ladenvall, P.; et al. Efficacy and safety of ticagrelor versus aspirin in acute stroke or transient ischaemic attack of atherosclerotic origin: A subgroup analysis of SOCRATES, a randomised, double-blind, controlled trial. Lancet Neurol. 2017, 16, 301–310. [Google Scholar] [CrossRef]
- Tuttolomondo, A.; Di Raimondo, D.; Pecoraro, R.; Arnao, V.; Pinto, A.; Licata, G. Inflammation in ischemic stroke subtypes. Curr. Pharm. Des. 2012, 18, 4289–4310. [Google Scholar] [CrossRef] [PubMed]
- Boehme, A.K.; McClure, L.A.; Zhang, Y.; Luna, J.M.; Del Brutto, O.H.; Benavente, O.R.; Elkind, M.S. Inflammatory Markers and Outcomes after Lacunar Stroke: Levels of Inflammatory Markers in Treatment of Stroke Study. Stroke 2016, 47, 659–667. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Wang, Y.; Wang, J.; Anne Stetler, R.; Yang, Q.W. Inflammation in intracerebral hemorrhage: From mechanisms to clinical translation. Prog. Neurobiol. 2014, 115, 25–44. [Google Scholar] [CrossRef] [PubMed]
- Cho, H.J.; Lee, J.H.; Kim, Y.J.; Moon, Y.; Ko, S.M.; Kim, H.Y. Comprehensive evaluation of coronary artery disease and aortic atherosclerosis in acute ischemic stroke patients: Usefulness based on Framingham risk score and stroke subtype. Cerebrovasc. Dis. 2011, 31, 592–600. [Google Scholar] [CrossRef] [PubMed]
- Spartalis, M.; Spartalis, E.; Tzatzaki, E.; Tsilimigras, D.I.; Moris, D.; Kontogiannis, C.; Kaminiotis, V.V.; Paschou, S.A.; Chatzidou, S.; Siasos, G. The Beneficial Therapy with Colchicine for Atherosclerosis via Anti-inflammation and Decrease in Hypertriglyceridemia. Cardiovasc. Hematol. Agents Med. Chem. 2018, 16, 74–80. [Google Scholar] [CrossRef]
- Lomivorotov, V.V.; Efremov, S.M.; Pokushalov, E.A.; Karaskov, A.M. New-Onset Atrial Fibrillation after Cardiac Surgery: Pathophysiology, Prophylaxis, and Treatment. J. Cardiothorac. Vasc. Anesth. 2016, 30, 200–216. [Google Scholar] [CrossRef]
- Salih, M.; Smer, A.; Charnigo, R.; Ayan, M.; Darrat, Y.H.; Traina, M.; Morales, G.X.; DiBiase, L.; Natale, A.; Elayi, C.S. Colchicine for prevention of post-cardiac procedure atrial fibrillation: Meta-analysis of randomized controlled trials. Int. J. Cardiol. 2017, 243, 258–262. [Google Scholar] [CrossRef]
- Tandon, K.; Tirschwell, D.; Longstreth, W.T., Jr.; Smith, B.; Akoum, N. Embolic stroke of undetermined source correlates to atrial fibrosis without atrial fibrillation. Neurology 2019, 93, e381–e387. [Google Scholar] [CrossRef] [PubMed]
- Singh, J.A.; Cleveland, J.D. Gout and the risk of incident atrial fibrillation in older adults: A study of US Medicare data. RMD Open 2018, 4, e000712. [Google Scholar] [CrossRef] [PubMed]
- Kyriacou, D.N.; Lewis, R.J. Confounding by Indication in Clinical Research. JAMA 2016, 316, 1818–1819. [Google Scholar] [CrossRef]
- Tong, D.C.; Quinn, S.; Nasis, A.; Hiew, C.; Roberts-Thomson, P.; Adams, H.; Sriamareswaran, R.; Htun, N.M.; Wilson, W.; Stub, D.; et al. Colchicine in Patients with Acute Coronary Syndrome: The Australian COPS Randomized Clinical Trial. Circulation 2020, 142, 1890–1900. [Google Scholar] [CrossRef] [PubMed]
- FitzGerald, J.D.; Dalbeth, N.; Mikuls, T.; Brignardello-Petersen, R.; Guyatt, G.; Abeles, A.M.; Gelber, A.C.; Harrold, L.R.; Khanna, D.; King, C.; et al. 2020 American College of Rheumatology Guideline for the Management of Gout. Arthritis Rheumatol. 2020, 72, 879–895. [Google Scholar] [CrossRef]
- Kumral, E.; Karaman, B.; Orman, M.; Kabaroglu, C. Association of uric acid and carotid artery disease in patients with ischemic stroke. Acta Neurol. Scand. 2014, 130, 11–17. [Google Scholar] [CrossRef]
- Hansildaar, R.; Vedder, D.; Baniaamam, M.; Tausche, A.K.; Gerritsen, M.; Nurmohamed, M.T. Cardiovascular risk in inflammatory arthritis: Rheumatoid arthritis and gout. Lancet Rheumatol. 2021, 3, e58–e70. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Non-Chronic Use Category | Chronic Use Category | ||||
|---|---|---|---|---|---|
| Variable | Non-User (n = 355,498) | New User (n = 912) | Former User (n = 4737) | Long-Term User (n = 4354) | MASD |
| Age, years | 68.6 ± 11.8 | 69.5 ± 11.1 | 69.6 ± 11.1 | 70.0 ± 10.8 | 0.12 |
| Age group, year | |||||
| 40–64 years | 131,323 (36.9) | 299 (32.8) | 1527 (32.2) | 1321 (30.3) | 0.14 |
| 65–74 years | 106,785 (30.0) | 290 (31.8) | 1553 (32.8) | 1451 (33.3) | 0.07 |
| ≥75 years | 117,390 (33.0) | 323 (35.4) | 1657 (35.0) | 1582 (36.3) | 0.07 |
| Male sex | 202,812 (57.1) | 686 (75.2) | 3678 (77.6) | 3553 (81.6) | 0.50 |
| Hospital level | |||||
| Medical center (teaching hospital) | 102,367 (28.8) | 266 (29.2) | 1359 (28.7) | 1380 (31.7) | 0.07 |
| Regional/district hospital | 253,131 (71.2) | 646 (70.8) | 3378 (71.3) | 2974 (68.3) | 0.07 |
| Comorbidity | |||||
| Previous ischemic stroke | 34,395 (9.7) | 95 (10.4) | 454 (9.6) | 501 (11.5) | 0.07 |
| Previous hemorrhagic stroke | 3910 (1.10) | 12 (1.32) | 45 (0.95) | 42 (0.96) | 0.04 |
| Gout | 18,267 (5.1) | 601 (65.9) | 3484 (73.5) | 3670 (84.3) | 3.08 |
| Diabetes mellitus | 136,455 (38.4) | 344 (37.7) | 1688 (35.6) | 1489 (34.2) | 0.09 |
| Hypertension | 265,395 (74.7) | 768 (84.2) | 4077 (86.1) | 3813 (87.6) | 0.30 |
| Previous myocardial infarction | 7104 (2.0) | 30 (3.3) | 152 (3.2) | 180 (4.1) | 0.15 |
| Coronary artery disease | 68,294 (19.2) | 254 (27.9) | 1246 (26.3) | 1213 (27.9) | 0.22 |
| Chronic kidney disease | 9352 (2.6) | 95 (10.4) | 420 (8.9) | 504 (11.6) | 0.54 |
| COPD | 30,791 (8.7) | 130 (14.3) | 576 (12.2) | 498 (11.4) | 0.20 |
| Dyslipidemia | 116,734 (32.8) | 352 (38.6) | 1939 (40.9) | 1689 (38.8) | 0.17 |
| Previous malignancy | 15,448 (4.3) | 32 (3.5) | 232 (4.9) | 191 (4.4) | 0.07 |
| Carotid stenting or endarterectomy | 654 (0.18) | 2 (0.22) | 9 (0.19) | 16 (0.37) | 0.04 |
| CCI score | 2.5 ± 1.6 | 2.9 ± 1.8 | 2.7 ± 1.8 | 2.8 ± 1.7 | 0.27 |
| Estimated NIHSS | 6.6 ± 5.1 | 6.5 ± 5.0 | 6.7 ± 5.3 | 6.8 ± 5.3 | 0.04 |
| Estimated NIHSS group | |||||
| ≤5 | 244,478 (68.8) | 629 (69.0) | 3285 (69.3) | 2933 (67.4) | 0.04 |
| 6–13 | 68,757 (19.3) | 187 (20.5) | 869 (18.3) | 875 (20.1) | 0.06 |
| >13 | 42,263 (11.9) | 96 (10.5) | 583 (12.3) | 546 (12.5) | 0.06 |
| Anti-hypertensive agent | |||||
| ACEI/ARB | 164,366 (46.2) | 498 (54.6) | 2504 (52.9) | 2381 (54.7) | 0.17 |
| CCB | 149,514 (42.1) | 458 (50.2) | 2289 (48.3) | 2319 (53.3) | 0.23 |
| Alpha-blocker | 20,721 (5.8) | 82 (9.0) | 434 (9.2) | 457 (10.5) | 0.20 |
| Beta-blocker | 87,688 (24.7) | 261 (28.6) | 1409 (29.7) | 1406 (32.3) | 0.18 |
| Thiazide | 18,483 (5.2) | 59 (6.5) | 274 (5.8) | 235 (5.4) | 0.06 |
| Loop diuretics | 21,111 (5.9) | 92 (10.1) | 427 (9.0) | 518 (11.9) | 0.25 |
| Spironolactone | 3462 (1.0) | 16 (1.8) | 64 (1.4) | 66 (1.5) | 0.08 |
| Others | 7770 (2.2) | 31 (3.4) | 115 (2.4) | 147 (3.4) | 0.08 |
| Number of anti-hypertensive agents | |||||
| 0 | 103,446 (29.1) | 197 (21.6) | 1000 (21.1) | 776 (17.8) | 0.28 |
| 1–2 | 194,957 (54.8) | 495 (54.3) | 2706 (57.1) | 2478 (56.9) | 0.06 |
| 3–4 | 54,429 (15.3) | 205 (22.5) | 978 (20.6) | 1027 (23.6) | 0.20 |
| ≥5 | 2666 (0.75) | 15 (1.64) | 53 (1.12) | 73 (1.68) | 0.08 |
| Average numbers of antihypertensive agents | 1.33 ± 1.16 | 1.64 ± 1.24 | 1.59 ± 1.20 | 1.73 ± 1.22 | 0.34 |
| Antidiabetic agent | |||||
| Biguanide (Metformin) | 78,222 (22.0) | 142 (15.6) | 759 (16.0) | 622 (14.3) | 0.19 |
| TZD | 11,565 (3.3) | 31 (3.4) | 114 (2.4) | 110 (2.5) | 0.06 |
| Sulfonylurea | 80,173 (22.6) | 170 (18.6) | 826 (17.4) | 755 (17.3) | 0.13 |
| DPP4i | 9095 (2.6) | 13 (1.4) | 131 (2.8) | 82 (1.9) | 0.09 |
| Glinide | 11,945 (3.4) | 41 (4.5) | 162 (3.4) | 144 (3.3) | 0.07 |
| Alpha glucosidase inhibitors | 13,758 (3.9) | 39 (4.3) | 170 (3.6) | 160 (3.7) | 0.04 |
| Insulin | 16,766 (4.7) | 44 (4.8) | 188 (4.0) | 175 (4.0) | 0.04 |
| Average number of antidiabetic agents | 0.62 ± 1.02 | 0.53 ± 0.96 | 0.50 ± 0.93 | 0.47 ± 0.88 | 0.16 |
| Other medications | |||||
| Aspirin | 61,619 (17.3) | 237 (26.0) | 1012 (21.4) | 1176 (27.0) | 0.26 |
| Clopidogrel | 4424 (1.2) | 28 (3.1) | 101 (2.1) | 137 (3.1) | 0.17 |
| Cilostazol | 1808 (0.51) | 7 (0.77) | 45 (0.95) | 43 (0.99) | 0.07 |
| Statin | 28,865 (8.1) | 132 (14.5) | 591 (12.5) | 638 (14.7) | 0.24 |
| Fibrate | 19,410 (5.5) | 92 (10.1) | 365 (7.7) | 367 (8.4) | 0.20 |
| NSAIDs including Cox-2 | 78,075 (22.0) | 367 (40.2) | 1881 (39.7) | 2105 (48.3) | 0.63 |
| Steroid | 8541 (2.4) | 45 (4.9) | 207 (4.4) | 265 (6.1) | 0.24 |
| Gout medications | |||||
| Allopurinol | 3692 (1.0) | 190 (20.8) | 564 (11.9) | 1352 (31.1) | 2.40 |
| Benzbromarone | 6243 (1.8) | 343 (37.6) | 775 (16.4) | 1519 (34.9) | 2.33 |
| Sulfinpyrazone | 348 (0.10) | 15 (1.64) | 48 (1.01) | 111 (2.55) | 0.65 |
| Febuxostat | 8 (0.002) | 0 (0.000) | 5 (0.106) | 3 (0.069) | 0.16 |
| Follow-up year | 5.0 ± 3.6 | 5.2 ± 3.5 | 4.5 ± 3.5 | 5.1 ± 3.5 | 0.32 |
| Number of Event (%) | HR or SHR (95% CI) | |||||
|---|---|---|---|---|---|---|
| Non-Chronic Use Category | Chronic Use Category | |||||
| Variable | Non-User | New User | Former User | Long-Term User | New User vs. Non-User | Long-Term User vs. Former User |
| 6 month | ||||||
| Primary outcome | ||||||
| Recurrence of ischemic stroke | 13.6 | 13.2 | 15.9 | 14.2 | 0.95 (0.94–0.97) * | 0.87 (0.86–0.88) * |
| Secondary outcome | ||||||
| Cardiovascular death | 2.7 | 5.4 | 2.8 | 4.5 | 2.03 (1.97–2.08) * | 1.62 (1.57–1.67) * |
| All-cause mortality | 4.9 | 6.9 | 5.6 | 7.5 | 1.43 (1.40–1.46) * | 1.35 (1.32–1.38) * |
| New-diagnosedatrial fibrillation | 3.3 | 2.4 | 3.1 | 4.3 | 0.73 (0.70–0.75) * | 1.39 (1.35–1.44) * |
| 2 year | ||||||
| Primary outcome | ||||||
| Recurrence of ischemic stroke | 21.0 | 20.1 | 23.5 | 21.0 | 0.92 (0.91–0.93) * | 0.87 (0.86–0.88) * |
| Secondary outcome | ||||||
| Cardiovascular death | 6.7 | 8.8 | 6.9 | 7.6 | 1.28 (1.26–1.31) * | 1.11 (1.09–1.14) * |
| All-cause mortality | 12.5 | 15.2 | 12.1 | 13.2 | 1.18 (1.17–1.20) * | 1.10 (1.08–1.12) * |
| New-diagnosedatrial fibrillation | 5.1 | 4.8 | 4.2 | 6.7 | 0.91 (0.88–0.93) * | 1.61 (1.57–1.65) * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, C.-H.; Lin, Y.-S.; Sung, P.-S.; Wei, Y.-C.; Chang, T.-Y.; Lee, T.-H.; Lee, C.-Y.; Li, Y.-R. Colchicine Use and Risks of Stroke Recurrence in Acute Non-Cardiogenic Ischemic Stroke Patients: A Population-Based Cohort Study. J. Pers. Med. 2021, 11, 935. https://doi.org/10.3390/jpm11090935
Liu C-H, Lin Y-S, Sung P-S, Wei Y-C, Chang T-Y, Lee T-H, Lee C-Y, Li Y-R. Colchicine Use and Risks of Stroke Recurrence in Acute Non-Cardiogenic Ischemic Stroke Patients: A Population-Based Cohort Study. Journal of Personalized Medicine. 2021; 11(9):935. https://doi.org/10.3390/jpm11090935
Chicago/Turabian StyleLiu, Chi-Hung, Yu-Sheng Lin, Pi-Shan Sung, Yi-Chia Wei, Ting-Yu Chang, Tsong-Hai Lee, Ching-Yu Lee, and Yan-Rong Li. 2021. "Colchicine Use and Risks of Stroke Recurrence in Acute Non-Cardiogenic Ischemic Stroke Patients: A Population-Based Cohort Study" Journal of Personalized Medicine 11, no. 9: 935. https://doi.org/10.3390/jpm11090935