
Current Trends in Advanced Alginate-Based Wound Dressings for Chronic Wounds

 , ,
, ,  ,
,  , and
, and
Abstract
:1. Introduction
2. Chronic Wounds Mechanisms and Alginates Roles
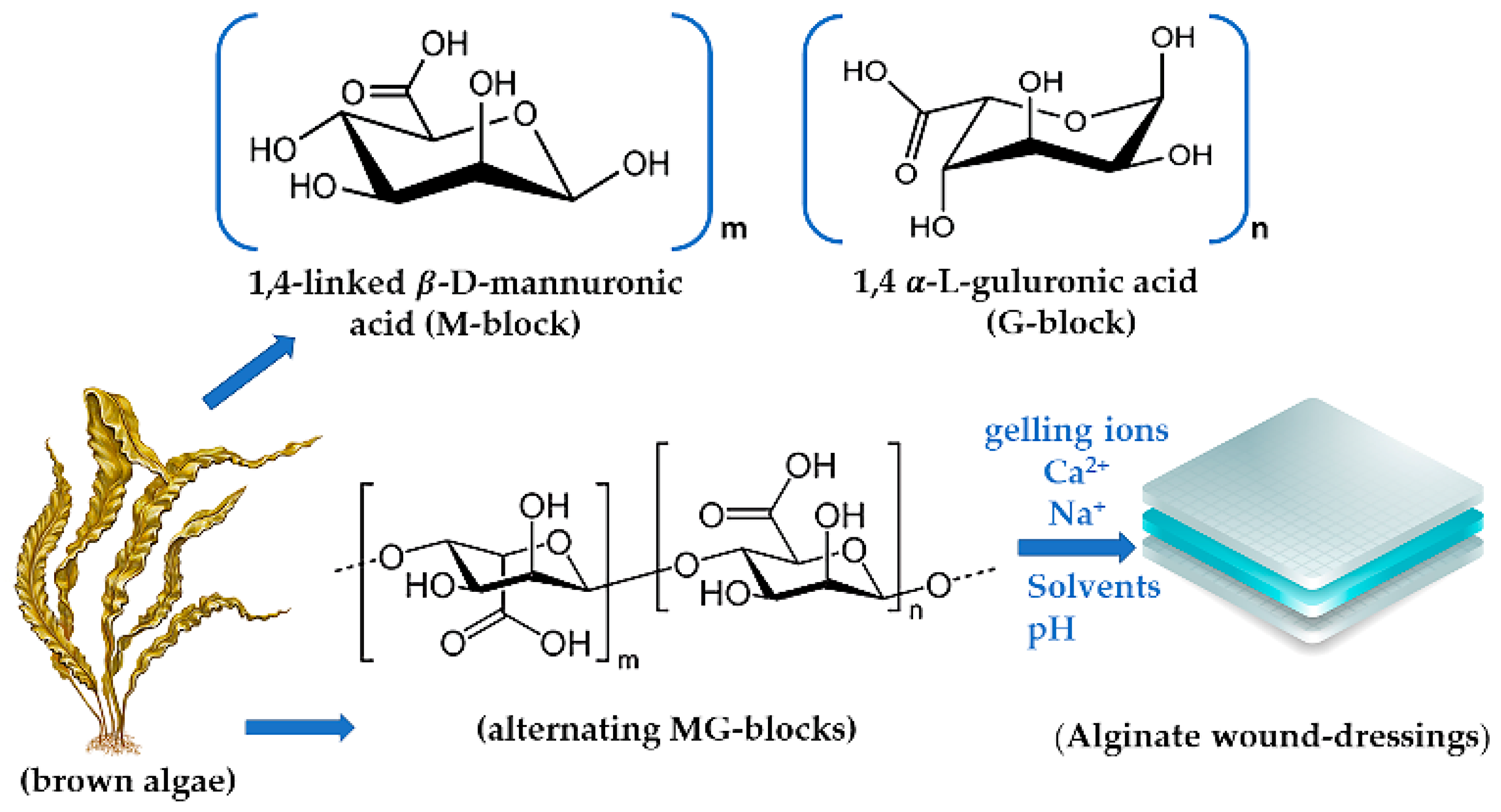
3. Alginate Physical Properties
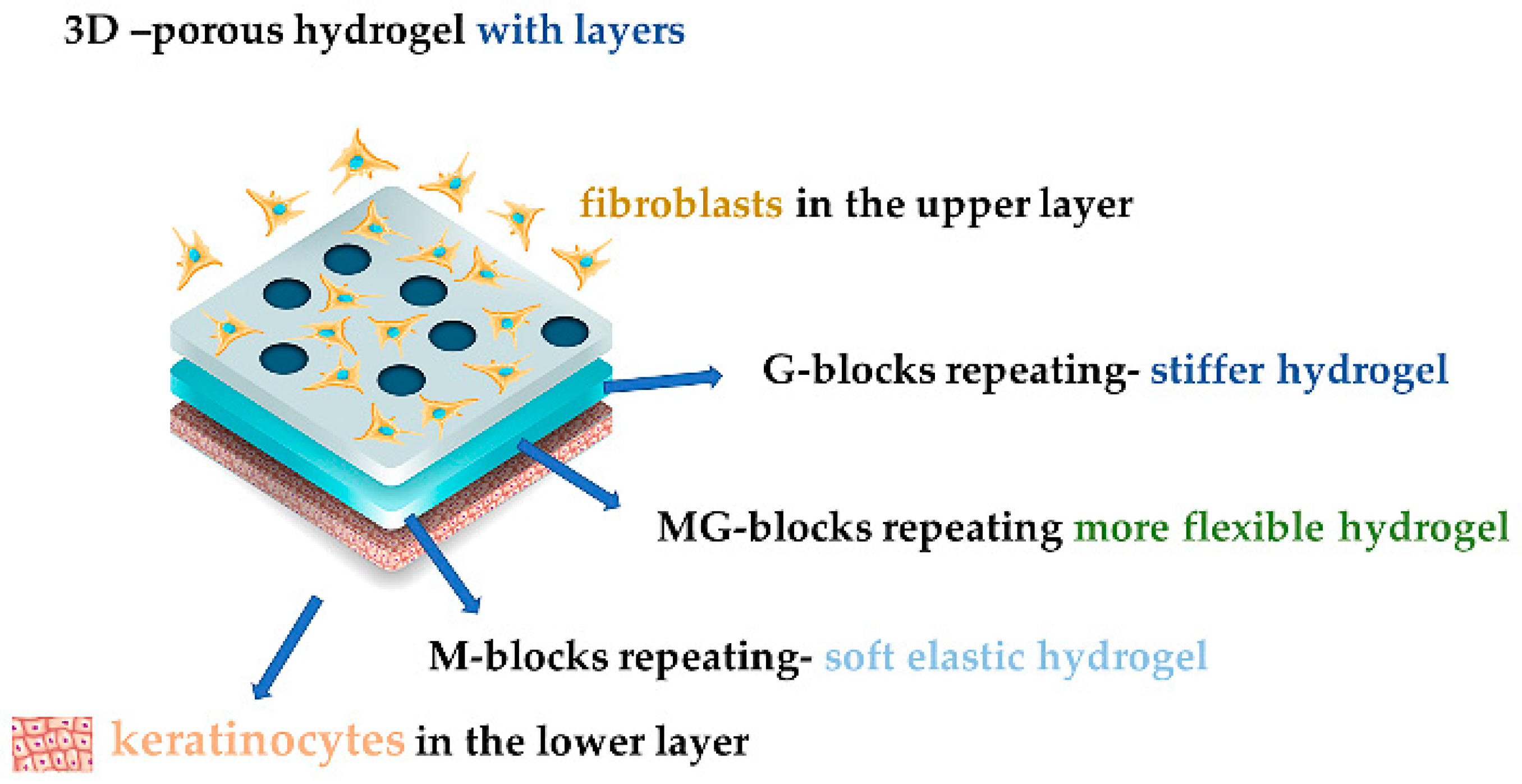
4. Alginate-Based Hydrogels for Wound Healing
5. Alginate-Based Beads and Microcapsules for Wound Healing
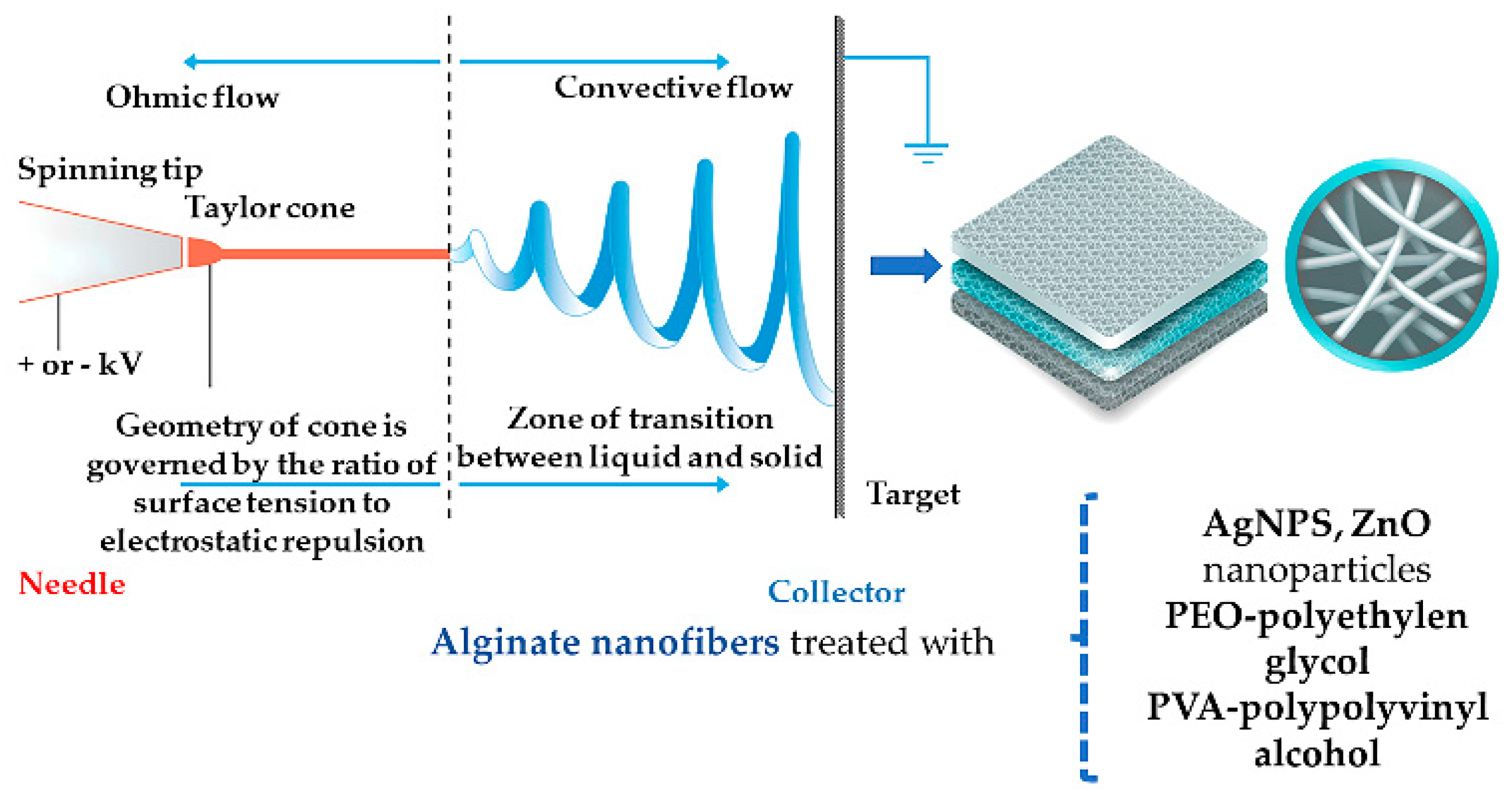
6. Alginate-Based Nanofibers and Fibers for Wound Healing

{kind=link}
{kind=link}
{kind=link}
| Composition | Study Type/Target | Ref. |
|---|---|---|
| 2% Na ALG solution—16% PVA solution—0.5, 1, 2, 5% ZnO-NPs; Na ALG/PVA ratio 1:1 | Composite nanofiber characterization, antibacterial effect, cell adhesion potential, cytotoxicity | [11,87] |
| Na ALG from unmodified methacrylated ALG—1% w/v RGD-modified methacrylated ALG—methacrylated heparin—4% w/v PEO; Na ALG/PEO ratio 1:1 | Nanofiber characterization, cell interaction, adhesion and proliferation, binding and releasing heparin tests | [28,96] |
| 4 wt % Na ALG—5 wt % PEO—0.5 wt % Triton X-100—5 wt % DMSO; Na ALG/PEO ratios: 65:35, 50:50, 35:65 | Nanofiber characterization, fibroblast proliferation | [86,94] |
| 8 wt % PVA—2% w/w Na ALG—3.2% w/v ciprofloxacin; PVA/Na ALG ratio: 5.5:1 | Nanofiber characterization, swelling, drug incorporation and release; in vivo tests on rabbits: drug release, wound healing | [94,95] |
| 1, 2, 3% wt of Na ALG—PEO—0.3 wt % Lecithin—5% w/w CaCl2; 1, 2, 3% wt of Na ALG/PEO weight % ratios: 1:1, 2:1, 3:1, 1:2, 2:2, 3:2 | Solution characterization: viscosity, conductivity; Nanofiber characterization: structure, water absorption, fibroblast attachment | [93,94] |
| 6% w/v Na ALG—0.1, 0.15, 2% chitin whisker Chitin whisker/ALG weight ratio: 0.05–2% | Whiskers and fibers characterization | [62,65,97] |
| ZnCl2—Ca ALG fibers | Antimicrobial and immuno-modulatory effects for wound healing keratinocyte migration, ppm Zn release | [11,42,89,98,99] |
| AgNO3—6% Ca ALG fibers | Antimicrobial effect | [11,89,98,100] |
| 0.5–0.75% w/v Chitosan—0.5–1% w/v ALG—Dexamethasone/BSA/PDGF-bb/Avidin fibers | Drug incorporation and release, PDGF-bb bioactivity | [49,90] |
| 0, 0.014, 0.041% w/v Chitosan—0.001% w/v Na ALG—Ninhydrin—CaCl2 in fibers | Filament characterization | [49,101] |
| 1.5 w % Na ALG—Ag-NPs in crosslinked fibers | Wound healing effect on SKH-1 mice | [102] |
7. Other Alginate-Based Dressings
| Composition | Study Type/Target | Ref. |
|---|---|---|
| Na ALG—0.1% w/v I-labeled SDF-1 plasmid Na ALG—0.0001% w/v (1 ng/µL) I-labeled SDF-1 protein | Acute surgical wounds on Yorkshire pigs: SDF-1 release kinetics, wound healing rate, scar formation | [42,115] |
| Viscose/silver/ALG Vis/Ag-NPs/ALG Viscose/silver/ALG/nicotinamide Viscose/silver/ALG/nicotinamide/CaCl2 0.5–1.5% w/w Na ALG in nonwoven fabric | Burn—diabetic rats | [105] |
| Chitosan 4% w/v—1% w/w CH3COOH—4% ALG Chitosan 4% w/v—1% w/w CH3COOH—4% CG w/v—5.7% NaCl | Comparative drug release system study: swelling, Diltiazem HCl-loaded tablet formulation, dissolution in 1:1 complex systems | [116] |
| Ca ALG versus silicone-coated polyamide net | Comparative randomized trial: healing and slippage rate, removal discomfort degree on skin graft donor sites | [117,118] |
| 2% w/v Na ALG—pH-responsive dye—glycerol 0–60% w/v | Flexible microfibers description, real-time pH modifications on the pig wound site | [112] |
| collagen—0.5, 1.0, 1.5, 2.0, 3.0, 4.0, 5.0% alginic acid, at 3:1 ratio in cross-linked sheet | Sheet characterization | [98,119] |
| 75% Alginic acid solution 2% w/v– 45S5 bioactive glass—25% cell suspension | VEGF secretion, cell viability, cytotoxicity | [120] |
| Polyox®—CG—Streptomycin—Diclofenac (0.75:0.25:0.3:0.25 g) Polyox®—0.5 g Na ALG—Streptomycin—Diclofenac (0.5:0.5:0.25:0.1 g) | Wafer characterization, adhesion, drug release, swelling | [23,111] |
| 2% w/v Alginic acid—murine antisense nucleotides (Cx43asODN) based scaffolds | Wounded ICR mice: inflammatory response, re-epithelization | [11,104] |
| 20 µg Smad3 ASOs in Na ALG and chitosan 1:1, 1:2, 1:4, 1:8, 1:16 ALG/chitosan ratio in PEC | Scaffold characterization, wound healing in C57BL/6 mice | [40,62,65] |
| gelatin—1 wt % Na ALG (with or without 0.4 mg/cm2 AgSD) sponge | Wistar rat wound healing | [11,98,121] |
| 1% solution silk fibroin—1% solution alginic acid in 10:0, 5:5 and 0:10 ratios sponge | Sprague Dawley rats full thickness wound | [98,122] |
| 2 or 4% w/v high G and high M ALG—0.1–10% w/w PEG—9.5% w/v poly(D,L-lactide-co-glycolide) (PLGA)—0.5% w/v insulin microparticles in sponge | Sponge characterization: density, tensile strength, water vapor transmission rate and absorption capacity. In vitro study: interaction with HaCaT cells, insulin release | [23,114] |
| Chitosan—1% w/w Na ALG—hematoxylin-eosin—DHEA—AgSD in PEC sponge | Microscope assay, in vitro drug release, cytotoxicity, antibacterial effect, in vivo burn healing on BALB/C mice | [49,123] |
| ALG—0.2, 0.4% chitosan—0.1, 0.5% all-trans retinoic acid (ATRA). 1:10 ATRA/ALG ratio in microparticles | Microparticles characterization, encapsulation efficiency, dermal localization, ATRA skin release | [42,124] |
| 2% Na ALG (61% M and 39% G)—2–4 µg VEGF in microspheres | In vitro drug release, in vivo angiogenesis | [125] |
8. Commercially Available Pharmaceutical Alginate-Based Products
| Name | Composition/Target | Study Type/Effects | Ref. |
|---|---|---|---|
| ALGS6 Ag (Prescribed/Over-The-Counter) | Ca ALG fiber—Lyocell fiber—1.7% Ag+ Surgical, traumatic, acute and chronic wounds, ulcers, first and second degree burns; Minor cuts, burns | Exudate absorption, gel forming, wound healing promoter if changed weekly | [142] |
| Aquacel™ Ag EXTRA™ Hydrofiber™ (Prescribed/OTC) | Bi-layer Na ALG CMC—Ag+—strengthening fibers; Surgical, traumatic, exuding, infected, and painful wounds, second degree burns, ulcers or for minor cuts or burns | Bacterial inhibition, absorbs the wound exudate while forming a gel, it must be changed every 1–2 weeks | [142] |
| Calgitrol™ foam or SilverSite™ | Ag+ in Ag ALG—Ca ALG—polyurethane foam | Antimicrobial effect, cytotoxicity | [23,143,144,145] |
| Fibracol 10% Ca ALG in Fibracol Plus® dressing | 90% Collagen—10% Ca ALG; Exuding full- and partial-thickness wounds, second degree burns; diabetic, pressure, and venous ulcers | Clinical Trial: healing time of diabetic foot ulcers | [16,32,146] |
| Flaminal® gel | ALG—PEG matrix—notatin—lactoperoxidase—guaiacol; burns, post-surgery wounds, diabetic, leg and pressure ulcers. If used with H2O2 and SCN- it has a bacteriostatic effect against both gram-positive and gram-negative bacteria. | Antimicrobial and bacteriostatic effect, wound surface moisturizer, exudate absorber, debrides necrotic tissue | [32,129,147,148] |
| Guardix-SG® | Na ALG—poloxamer—CaCl2; post-surgery (silicone implantation, blepharoplasty) | In vivo post-surgery studies on rabbits: thermosensitive gel, mechanical barrier formation, suppression of capsular contracture, reduced inflammation and fibrosis | [32,149,150] |
| Hyalogran® dressing | Hyaluronic acid ester—Na ALG; Leg and pressure sores, diabetic and ischemic wounds (with slough or necrosis) | Exudate absorption, gel transformation, necrotic tissue removal | [32,140] |
| Kaltostat® | 80% High G Ca ALG—20% NaALG; Acute and chronic wounds with moderate to heavy exudate | Wound healing | [6,28,49,62,63,64,65,151] |
| Luofucon® Antibacterial Alginate Wound Dressing (OTC) | Ca ALG—Ag; minor cuts, abrasions, and burns | Changed daily it has antibacterial effect and promotes wound healing | [126] |
| Luofucon® Extra Silver Alginate Dressing (PO) | Ca ALG—Ag; moderate to heavily exuding wounds, ulcers, trauma-inflicted or post-operative wounds, infected wounds, grafts | Antibacterial effect for seven days and it promotes wound healing | [126] |
| Medihoney® (gel, hydrogel or paste) | Ca ALG—Manuka honey; ulcers: hemorrhagic, heavily exuding, diabetic foot, leg (arterial or venous), pressure (partial or full-thickness) ulcers. First and second partial thickness burns. Surgical and traumatic wounds | Antibacterial effect | [3,23] |
| Purilon Gel® | Na CMC—Ca ALG; Used with another dressing for first and second degree burns or sloughy and necrotic wounds | Wound surface moisturizer | [32,147,152,153] |
| Saf-gel® | Carbomer propylene glycol sodium—Ca ALG; Abrasions, cuts, sloughy and necrotic wounds, second degree burns, non-infected diabetic foot ulcers, and pressure and venous ulcers | Wound healing and surface moisturizer. | [32,147,154] |
| SeaSorb® fine foam sheet | Na ALG/Ca ALG—polyethylene net; Heavily exuding wounds: cavity wounds, second degree burns, diabetic, leg and pressure ulcers, spina bifida | Human clinical trials: fiber to gel transformation, tolerance, healing rate with reduced exudate, maceration and pain intensity | [32,155,156] |
| Silvercel™ | 36% Ca ALG with high G—6% CMC—28% Ag (111 mg Ag/100 cm2)—30% EasyLift Precision Film (Acelity/Systagenix) | Pig and human trials, wound healing | [141,157,158,159,160,161,162] |
| Tromboguard® bi-layer dressing | Polyurethane sponge—chitosan + Na ALG + Ca ALG + Ag+; Traumatic and post-surgery wounds | Antibacterial effect and strong hemostatic | [32] |
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Sen, C.K.; Gordillo, G.M.; Roy, S.; Kirsner, R.; Lambert, L.; Hunt, T.K.; Gottrup, F.; Gurtner, G.C.; Longaker, M.T. Human Skin Wounds: A Major Snoballing Threat to Public Health and Economy. Wound Repair Regen. 2009, 17, 763–771. [Google Scholar] [CrossRef] [Green Version]
- Chandran, S.; Seetharaman, A.; Rajalekshmi, G.; Pandimadevi, M. Potential wound healing materials from the natural polymers—A review. Int. J. Pharma. Bio Sci. 2015, 6, 1365–1389. [Google Scholar]
- Das, S.; Baker, A.B. Biomaterials and Nanotherapeutics for Enhancing Skin Wound Healing. Front. Bioeng. Biotechnol. 2016, 4, 82. [Google Scholar] [CrossRef] [PubMed]
- Erdogan, I.; Bayraktar, O.; Uslu, M.E.; Tuncel, O. Wound Healing Effects of Various Fractions of Olive Leaf Extract (OLE) on Mouse Fibroblasts. Rom. Biotechnol. Lett. 2018, 23, 14217–14228. [Google Scholar] [CrossRef]
- Miricioiu, M.G.; Niculescu, V.C.; Filote, C.; Raboaca, M.S.; Nechifor, G. Coal fly ash derived silica nanomaterial for mmms-application in CO2/CH4 separation. Membranes 2021, 11, 78. [Google Scholar] [CrossRef]
- Aramwit, P. Introduction to biomaterials for wound healing. In Wound Healing Biomaterials; Elsevier Ltd.: London, UK, 2016; Volume 2, pp. 3–38. ISBN 9780081006061. [Google Scholar]
- Liu, J.; Zheng, H.; Dai, X.; Sun, S.; Machens, H.G.; Schilling, A.F. Biomaterials for Promoting Wound Healing in Diabetes. J. Tissue Sci. Eng. 2017, 8, 193–196. [Google Scholar] [CrossRef]
- Mihai, M. Novel biocompatible chitosan based multilayer films. Rom. Biotechnol. Lett. 2011, 16, 6313–6321. [Google Scholar]
- Barbu, A.; Neamțu, M.B.; Zăhan, M.; Mireșan, V. Trends in alginate-based films and membranes for wound healing. Rom. Biotechnol. Lett. 2020, 25, 1683–1689. [Google Scholar] [CrossRef]
- Alizadehgiashi, M.; Nemr, C.R.; Chekini, M.; Ramos, D.P.; Mittal, N.; Ahmed, S.U.; Khuu, N.; Kelley, S.O.; Kumacheva, E. Multifunctional 3D-Printed Wound Dressings. ACS Nano 2021, 15, 12375–12387. [Google Scholar] [CrossRef]
- Chaudhari, A.A.; Vig, K.; Baganizi, D.R.; Sahu, R.; Dixit, S.; Dennis, V.; Singh, S.R.; Pillai, S.R. Future prospects for scaffolding methods and biomaterials in skin tissue engineering: A review. Int. J. Mol. Sci. 2016, 17, 1974. [Google Scholar] [CrossRef] [PubMed]
- Chin, C.Y.; Gan, J.E. Formulation and characterisation of alginate hydrocolloid film dressing loaded with gallic acid for potential chronic wound healing. F1000Research 2021, 10, 451. [Google Scholar] [CrossRef]
- Snyder, D.; Sullivan, N.; Margolis, B.D.; Schoelles, K. Skin substitutes for treating chronic wounds—Technical brief. In Technology Assessment Program—Technical Brief; Project ID No. WNDT0818. (Prepared by the ECRI Institute-Penn Medicine Evidence-Based Practice Center under Contract No. HHSA 290-2015-00005-I); Agency for Healthcare Research and Quality: Rockville, MD, USA, February 2020. Available online: http://www.ahrq.gov/research/findings/ta/index.html (accessed on 31 May 2021).
- Koga, A.Y.; Felix, J.C.; Silvestre, R.G.M.; Lipinski, L.C.; Carletto, B.; Kawahara, F.A.; Pereira, A.V. Evaluation of wound healing effect of alginate film containing aloe vera gel and cross-linked with zinc chloride. Acta Cir. Bras. 2020, 35, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Clark, M. Technology update: Rediscovering alginate dressings. Wounds Int. 2012, 3, 3–6. [Google Scholar] [CrossRef]
- Dumville, J.; O’Meara, S.; Deshpande, S.; Speak, K. Alginate dressings for healing diabetic foot ulcers. Cochrane Database Syst. Rev. 2013, 6, CD009110. [Google Scholar] [CrossRef] [PubMed]
- Radu, C.-D.; Parteni, O.; Sandu, I.G.; Lisa, G.; Munteanu, C.; Lupu, V.V. Specific characterization of a multilayer biomaterial controlled release of tacrolimus. Rev. Chim. 2016, 67, 199–204. [Google Scholar]
- Samimi, M.; Validov, S. Characteristics of pDNA-loaded chitosan/alginate-dextran sulfate nanoparticles with high transfection efficiency. Rom. Biotechnol. Lett. 2018, 23, 13996–14006. [Google Scholar] [CrossRef]
- Yussof, S.J.M.; Omar, E.; Pai, D.R.; Sood, S. Cellular events and biomarkers of wound healing. Indian J. Plast. Surg. 2012, 45, 220–228. [Google Scholar] [CrossRef]
- Nagaraja, S.; Wallqvist, A.; Reifman, J.; Mitrophanov, A.Y. Computational Approach To Characterize Causative Factors and Molecular Indicators of Chronic Wound Inflammation. J. Immunol. 2014, 192, 1824–1834. [Google Scholar] [CrossRef] [Green Version]
- Mathew-Steiner, S.S.; Roy, S.; Sen, C.K. Collagen in wound healing. Bioengineering 2021, 8, 63. [Google Scholar] [CrossRef]
- Chen, F.M.; Liu, X. Advancing biomaterials of human origin for tissue engineering. Prog. Polym. Sci. 2016, 53, 86–168. [Google Scholar] [CrossRef] [Green Version]
- Boateng, J.; Catanzano, O. Advanced Therapeutic Dressings for Effective Wound Healing—A Review. J. Pharm. Sci. 2015, 104, 3653–3680. [Google Scholar] [CrossRef] [Green Version]
- Matei, A.M.; Caruntu, C.; Tampa, M.; Georgescu, S.R.; Matei, C.; Constantin, M.M.; Constantin, T.V.; Calina, D.; Ciubotaru, D.A.; Badarau, I.A.; et al. Applications of nanosized-lipid-based drug delivery systems in wound care. Appl. Sci. 2021, 11, 4915. [Google Scholar] [CrossRef]
- Pastar, I.; Stojadinovic, O.; Yin, N.C.; Ramirez, H.; Nusbaum, A.G.; Sawaya, A.; Patel, S.B.; Khalid, L.; Isseroff, R.R.; Tomic-Canic, M. Epithelialization in Wound Healing: A Comprehensive Review. Adv. Wound Care 2014, 3, 445–464. [Google Scholar] [CrossRef] [Green Version]
- Orsted, H.L.; Keast, D.; Forest-lalande, L. Basic Principles of Wound Healing An understanding of the basic physiology of wound healing provides. Wound Care Can. 2011, 9, 4–12. [Google Scholar]
- Ching, C.S.; Phillips, T.J.; Howard, C.E.; Panova, I.P.; Hayes, C.M.; Asandra, A.S.; Park, H.Y. Chronic wound fluid suppresses proliferation of dermal fibroblasts through a Ras-mediated signaling pathway. J. Investig. Dermatol. 2005, 124, 466–474. [Google Scholar] [CrossRef] [Green Version]
- De Jesus Raposo, M.F.; De Morais, A.M.B.; De Morais, R.M.S.C. Marine polysaccharides from algae with potential biomedical applications. Mar. Drugs 2015, 13, 2967. [Google Scholar] [CrossRef]
- Raguvaran, R.; Manuja, B.K.; Chopra, M.; Thakur, R.; Anand, T.; Kalia, A.; Manuja, A. Sodium alginate and gum acacia hydrogels of ZnO nanoparticles show wound healing effect on fibroblast cells. Int. J. Biol. Macromol. 2017, 96, 185–191. [Google Scholar] [CrossRef]
- Badea, V.; Paula Balaban, D.P.; Rapeanu, G.; Amariei, C.; Badea, C.F. The antibacterial activity evaluation of Cystoseira barbata biomass and some alginates upon bacteria from oropharyngeal cavity. Rom. Biotechnol. Lett. 2009, 14, 4851–4857. [Google Scholar]
- Spadari, C.d.C.; Lopes, L.B.; Ishida, K. Potential use of alginate-based carriers as antifungal delivery system. Front. Microbiol. 2017, 8, 97. [Google Scholar] [CrossRef] [Green Version]
- Szekalska, M.; Pucilowska, A.; Szymanska, E.; Ciosek, P.; Winnicka, K. Alginate: Current Use and Future Perspectives in Pharmaceutical and Biomedical Applications. Int. J. Polym. Sci. 2016, 2016, 7697031. [Google Scholar] [CrossRef] [Green Version]
- Ueno, M.; Oda, T. Effects of Alginate Oligosaccharides on the Growth of Marine Microalgae. In Marine Algae Extracts: Processes, Products, and Applications; Kim, S.-K., Chojnacka, K., Eds.; Wiley-VCH: Weinheim, Germany, 2015; Volumes 1–2, pp. 213–226. ISBN 9783527679577. [Google Scholar]
- Wiegand, C.; Hipler, U.C. Polymer-based biomaterials as dressings for chronic stagnating wounds. Macromol. Symp. 2010, 294, 1–13. [Google Scholar] [CrossRef]
- Pawar, H.V.; Tetteh, J.; Boateng, J.S. Preparation, optimisation and characterisation of novel wound healing film dressings loaded with streptomycin and diclofenac. Colloids Surf. B Biointerfaces 2012, 102, 102–110. [Google Scholar] [CrossRef]
- Liakos, I.; Rizzello, L.; Scurr, D.J.; Pompa, P.P.; Bayer, I.S.; Athanassiou, A. All-natural composite wound dressing films of essential oils encapsulated in sodium alginate with antimicrobial properties. Int. J. Pharm. 2014, 463. [Google Scholar] [CrossRef]
- Raducu, L.; Cozma, C.N.; Balcangiu-Stroescu, A.E.; Avino, A.; Tanasescu, A.D.; Balan, D.G.; Jecan, C.R. Our Experience in Chronic Wounds Care with Polyurethane Foam. Rev. Chim. 2018, 69, 585–586. [Google Scholar] [CrossRef]
- Mushollaeni, W. The physicochemical characteristics of sodium alginate from Indonesian brown seaweeds. Arab. J. Chem. 2011, 5, 349–352. [Google Scholar]
- Ivancic, A. Recent Trends in Alginate, Chitosan and Alginate-Chitosan Antimicrobial Systems. Chem. J. Mold. 2017, 11, 17–25. [Google Scholar] [CrossRef]
- Hong, H.J.; Jin, S.E.; Park, J.S.; Ahn, W.S.; Kim, C.K. Accelerated wound healing by smad3 antisense oligonucleotides-impregnated chitosan/alginate polyelectrolyte complex. Biomaterials 2008, 29, 4831–4837. [Google Scholar] [CrossRef] [PubMed]
- Rhein-Knudsen, N.; Ale, M.T.; Ajalloueian, F.; Meyer, A.S. Characterization of alginates from Ghanaian brown seaweeds: Sargassum spp. and Padina spp. Food Hydrocoll. 2017, 71, 236–244. [Google Scholar] [CrossRef]
- Lee, K.Y.; Mooney, D.J. Alginate: Properties and biomedical applications. Prog. Polym. Sci. 2012, 37, 106–126. [Google Scholar] [CrossRef] [Green Version]
- Lotfipour, F.; Mirzaeei, S.; Maghsoodi, M. Evaluation of the effect of CaCl2 and alginate concentrations and hardening time on the characteristics of Lactobacillus acidophilus loaded alginate beads using response surface analysis. Adv. Pharm. Bull. 2012, 2, 71–78. [Google Scholar] [CrossRef]
- Pawar, S.N. Chemical Modification of Alginates in Organic Media. Ph.D. Thesis, Virginia Polytechnic Institute and State University, Blacksburg, VA, USA, 2013. [Google Scholar]
- Maritz, J.; Krieg, H.M.; Yeates, C.A.; Botes, A.L.; Breytenbach, J.C. Calcium alginate entrapment of the yeast Rhodosporidium toruloides for the kinetic resolution of 1,2-epoxyoctane. Biotechnol. Lett. 2003, 25, 1775–1781. [Google Scholar] [CrossRef]
- Nicolae, V.; Neamtu, B.; Picu, O.; Stefanache, M.A.M.; Cioranu, V.S.I. The comparative evaluation of salivary biomarkers (Calcium, Phosphate, Salivary pH) in Cario-resistance versus Cario-activity. Rev. Chim. 2016, 67, 821–824. [Google Scholar]
- Pereira, R.; Carvalho, A.; Vaz, D.C.; Gil, M.H.; Mendes, A.; Bártolo, P. Development of novel alginate based hydrogel films for wound healing applications. Int. J. Biol. Macromol. 2013, 52, 221–230. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.; Singh, D. Radiation synthesis of PVP/alginate hydrogel containing nanosilver as wound dressing. J. Mater. Sci. Mater. Med. 2012, 23, 2649–2658. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.M.; Moxon, S.; Morris, G.A. Biopolymers as wound healing materials. In Wound Healing Biomaterials; Ågren, M., Ed.; Woodhead Publishing: Cambridge, UK, 2016; Volume 2, pp. 261–287. ISBN 9780081006061. [Google Scholar]
- Bhardwaj, T.R.; Kanwar, M.; Lal, R.; Gupta, A. Natural gums and modified natural gums as sustained release carriers. Drug Dev. Ind. Pharm. 2000, 26, 1025–1038. [Google Scholar] [CrossRef]
- Stoica, A.E.; Chircov, C.; Grumezescu, A.M. Nanomaterials for Wound Dressings: An Up-to-Date Overview. Molecules 2020, 25, 2699. [Google Scholar] [CrossRef]
- Koehler, J.; Brandl, F.P.; Goepferich, A.M. Hydrogel wound dressings for bioactive treatment of acute and chronic wounds. Eur. Polym. J. 2018, 100, 1–11. [Google Scholar] [CrossRef]
- Rezvani Ghomi, E.; Khalili, S.; Nouri Khorasani, S.; Esmaeely Neisiany, R.; Ramakrishna, S. Wound dressings: Current advances and future directions. J. Appl. Polym. Sci. 2019, 136, 47738. [Google Scholar] [CrossRef] [Green Version]
- Augst, A.D.; Kong, H.J.; Mooney, D.J. Alginate Hydrogels as Biomaterials. Macromol. Biosci. 2006, 6, 623–633. [Google Scholar] [CrossRef]
- Coviello, T.; Matricardi, P.; Marianecci, C.; Alhaique, F. Polysaccharide hydrogels for modified release formulations. J. Control. Release 2007, 119, 5–24. [Google Scholar] [CrossRef]
- Josef, E.; Zilberman, M.; Bianco-Peled, H. Composite alginate hydrogels: An innovative approach for the controlled release of hydrophobic drugs. Acta Biomater. 2010, 6, 4642–4649. [Google Scholar] [CrossRef] [PubMed]
- Balakrishnan, B.; Mohanty, M.; Umashankar, P.R.; Jayakrishnan, A. Evaluation of an in situ forming hydrogel wound dressing based on oxidized alginate and gelatin. Biomaterials 2005, 26, 6335–6342. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, L.P.; Cerqueira, M.T.; Correlo, V.M.; Reis, R.L.; Marques, A.P. Engineered hydrogel-based matrices for skin wound healing. In Wound Healing Biomaterials; Agren, M., Ed.; Elsevier Ltd.: London, UK, 2016; Volume 2, pp. 227–250. ISBN 9780081006061. [Google Scholar]
- Chicea, D.; Neamtu, B.; Chicea, R.; Chicea, L.M. The application of AFM for biological samples imaging. Dig. J. Nanomater. Biostruct. 2010, 5, 1015–1022. [Google Scholar]
- Neacsu, I.-A.; Melente, A.E.; Holban, A.-M.; Ficai, A.; Ditu, L.-M.; Kamerzan, C.-M.; Tihăuan, B.M.; Nicoara, A.I.; Bezirtzoglou, E.; Chifiriuc, M.-C. Novel hydrogels based on collagen and ZnO nanoparticles with antibacterial activity for improved wound dressings. Rom. Biotechnol. Lett. 2019, 24, 317–323. [Google Scholar] [CrossRef]
- Mohandas, A.; Kumar, S.; Raja, B.; Lakshmanan, V.-K.; Jayakumar, R. Exploration of alginate hydrogel/nano zinc oxide composite bandages for infected wounds. Int. J. Nanomed. 2015, 10, 53–66. [Google Scholar] [CrossRef] [Green Version]
- Jayakumar, R.; Prabaharan, M.; Kumar, P.T.S.; Nair, S.V.; Furuike, T.; Tamura, H. Novel Chitin and Chitosan Materials in Wound Dressing. In Biomedical Engineering, Trends in Materials Science; Laskovski, A., Ed.; InTech: Rijeka, Croatia, 2011; ISBN 9789537619824. [Google Scholar]
- Murakami, K.; Aoki, H.; Nakamura, S.; Nakamura, S.-i.; Takikawa, M.; Hanzawa, M.; Kishimoto, S.; Hattori, H.; Tanaka, Y.; Kiyosawa, T.; et al. Hydrogel blends of chitin/chitosan, fucoidan and alginate as healing-impaired wound dressings. Biomaterials 2010, 31, 83–90. [Google Scholar] [CrossRef]
- Murakami, K.; Ishihara, M.; Aoki, H.; Nakamura, S.; Nakamura, S.I.; Yanagibayashi, S.; Takikawa, M.; Kishimoto, S.; Yokoe, H.; Kiyosawa, T.; et al. Enhanced healing of mitomycin C-treated healing-impaired wounds in rats with hydrosheets composed of chitin/chitosan, fucoidan, and alginate as wound dressings. Wound Repair Regen. 2010, 18, 478–485. [Google Scholar] [CrossRef]
- Jayakumar, R.; Prabaharan, M.; Kumar, S.P.T.; Nair, S.V.; Tamura, H. Biomaterials based on chitin and chitosan in wound dressing applications. Biotechnol. Adv. 2011, 29, 322–337. [Google Scholar] [CrossRef]
- Rayyif, S.M.I.; Mohammed, H.B.; Curuțiu, C.; Bîrcă, A.C.; Grumezescu, A.M.; Vasile, B.Ș.; Dițu, L.M.; Lazăr, V.; Chifiriuc, M.C.; Mihăescu, G.; et al. ZnO Nanoparticles-Modified Dressings to Inhibit Wound Pathogens. Materials 2021, 14, 3084. [Google Scholar] [CrossRef]
- Strukova, S.M.; Dugina, T.N.; Chistov, I.V.; Lange, M.; Markvicheva, E.A.; Kuptsova, S.; Zubov, V.P.; Glusa, E. Immobilized thrombin receptor agonist peptide accelerates wound healing in mice. Clin. Appl. Thromb. 2001, 7, 325–329. [Google Scholar] [CrossRef]
- Lee, K.Y.; Peters, M.C.; Anderson, K.W.; Mooney, D.J. Controlled growth factor release from synthetic extracellular matrices. Nature 2000, 408, 998–1000. [Google Scholar] [CrossRef] [PubMed]
- Tanihara, M.; Suzuki, Y.; Yamamoto, E.; Noguchi, A.; Mizushima, Y. Sustained release of basic fibroblast growth factor and angiogenesis in a novel covalently crosslinked gel of heparin and alginate. J. Biomed. Mater. Res. 2001, 56, 216–221. [Google Scholar] [CrossRef]
- Oh, S.T.; Kim, W.R.; Kim, S.H.; Chung, Y.C.; Park, J.S. The preparation of polyurethane foam combined with pH-sensitive alginate/bentonite hydrogel for wound dressings. Fibers Polym. 2011, 12, 159–165. [Google Scholar] [CrossRef]
- Catanzano, O.; Straccia, M.C.; Miro, A.; Ungaro, F.; Romano, I.; Mazzarella, G.; Santagata, G.; Quaglia, F.; Laurienzo, P.; Malinconico, M. Spray-by-spray in situ cross-linking alginate hydrogels delivering a tea tree oil microemulsion. Eur. J. Pharm. Sci. 2015, 66, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Babavalian, H.; Latifi, A.M.; Shokrgozar, M.A.; Bonakdar, S.; Mohammadi, S.; Moghaddam, M.M. Analysis of healing effect of alginate sulfate hydrogel dressing containing antimicrobial peptide on wound infection caused by methicillin-resistant Staphylococcus aureus. Jundishapur J. Microbiol. 2015, 8, e28320. [Google Scholar] [CrossRef] [Green Version]
- Popa, E.G.; Gomes, M.E.; Reis, R.L. Cell delivery systems using alginate-carrageenan hydrogel beads and fibers for regenerative medicine applications. Biomacromolecules 2011, 12, 3952–3961. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.W.; Yoon, J.J.; Lee, J.H.; Kim, S.Y.; Jung, H.J.; Kim, S.J.; Joh, J.W.; Lee, H.H.; Lee, D.S.; Lee, S.K. Sustained release of vascular endothelial growth factor from calcium-induced alginate hydrogels reinforced by heparin and chitosan. Transplant. Proc. 2004, 36, 2464–2465. [Google Scholar] [CrossRef]
- Lee, K.Y.; Peters, M.C.; Mooney, D.J. Controlled drug delivery from polymers by mechanical signals. Adv. Mater. 2001, 13, 837–839. [Google Scholar] [CrossRef]
- Drury, J.L.; Mooney, D.J. Hydrogels for tissue engineering: Scaffold design variables and applications. Biomaterials 2003, 24, 4337–4351. [Google Scholar] [CrossRef]
- Shen, Y.; Xu, G.; Huang, H.; Wang, K.; Wang, H.; Lang, M.; Gao, H.; Zhao, S. Sequential Release of Small Extracellular Vesicles from Bilayered Thiolated Alginate/Polyethylene Glycol Diacrylate Hydrogels for Scarless Wound Healing. ACS Nano 2021, 15, 6352–6368. [Google Scholar] [CrossRef]
- Lu, W.; Bao, D.; Ta, F.; Liu, D.; Zhang, D.; Zhang, Z.; Fan, Z. Multifunctional Alginate Hydrogel Protects and Heals Skin Defects in Complex Clinical Situations. ACS Omega 2020, 5, 17152–17159. [Google Scholar] [CrossRef]
- Peretz, S.; Cinteza, O. Removal of some nitrophenol contaminants using alginate gel beads. Colloids Surf. A Physicochem. Eng. Asp. 2008, 319, 165–172. [Google Scholar] [CrossRef]
- Mohamadnia, Z.; Zohuriaan-Mehr, M.J.; Kabiri, K.; Jamshidi, A.; Mobedi, H. Ionically cross-linked carrageenan-alginate hydrogel beads. J. Biomater. Sci. Polym. Ed. 2008, 19, 47–59. [Google Scholar] [CrossRef] [PubMed]
- Al-Hosny, E.A.; Al-Helw, A.R.M.; Al-Dardini, M.A. Comparative study of in-vitro release and bioavailability of sustained release diclofenac sodium from certain hydrophilic polymers and commercial tablets in beagle dogs. Pharm. Acta Helv. 1997, 72, 159–164. [Google Scholar] [CrossRef]
- Mahdavinia, G.R.; Rahmani, Z.; Karami, S.; Pourjavadi, A. Magnetic/pH-sensitive κ-carrageenan/sodium alginate hydrogel nanocomposite beads: Preparation, swelling behavior, and drug delivery. J. Biomater. Sci. Polym. Ed. 2014, 25, 1891–1906. [Google Scholar] [CrossRef]
- Peters, M.C.; Isenberg, B.C.; Rowley, J.A.; Mooney, D.J. Release from alginate enhances the biological activity of vascular endothelial growth factor. J. Biomater. Sci. Polym. Ed. 1998, 9, 1267–1278. [Google Scholar] [CrossRef]
- Mori, M.; Rossi, S.; Bonferoni, M.C.; Ferrari, F.; Sandri, G.; Riva, F.; Del Fante, C.; Perotti, C.; Caramella, C. Calcium alginate particles for the combined delivery of platelet lysate and vancomycin hydrochloride in chronic skin ulcers. Int. J. Pharm. 2014, 461, 505–513. [Google Scholar] [CrossRef]
- Aderibigbe, B.A.; Buyana, B. Alginate in wound dressings. Pharmaceutics 2018, 10, 42. [Google Scholar] [CrossRef] [Green Version]
- Leung, V.; Hartwell, R.; Elizei, S.S.; Yang, H.; Ghahary, A.; Ko, F. Postelectrospinning modifications for alginate nanofiber-based wound dressings. J. Biomed. Mater. Res. Part B Appl. Biomater. 2014, 102, 508–515. [Google Scholar] [CrossRef]
- Shalumon, K.T.; Anulekha, K.H.; Nair, S.V.; Nair, S.V.; Chennazhi, K.P.; Jayakumar, R. Sodium alginate/poly(vinyl alcohol)/nano ZnO composite nanofibers for antibacterial wound dressings. Int. J. Biol. Macromol. 2011, 49, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Alven, S.; Nqoro, X.; Aderibigbe, B.A. Polymer-based materials loaded with curcumin for wound healing applications. Polymers 2020, 12, 2286. [Google Scholar] [CrossRef] [PubMed]
- Qin, Y. Alginate fibers: An overwiew of the production processes and applications in wound management. Polym. Int. 2008, 57, 171–180. [Google Scholar] [CrossRef]
- Liao, I.C.; Wan, A.C.A.; Yim, E.K.F.; Leong, K.W. Controlled release from fibers of polyelectrolyte complexes. J. Control. Release 2005, 104, 347–358. [Google Scholar] [CrossRef] [PubMed]
- Konwarh, R.; Misra, M.; Mohanty, A.K.; Karak, N. Diameter-tuning of electrospun cellulose acetate fibers: A Box-Behnken design (BBD) study. Carbohydr. Polym. 2013, 92, 1100–1106. [Google Scholar] [CrossRef]
- Ågren, M.S. Wound Healing Biomaterials Volume 2: Functional Biomaterials; Elsevier: London, UK, 2016; Volume 2, ISBN 9780081006061. [Google Scholar]
- Park, S.A.; Park, K.E.; Kim, W.D. Preparation of Sodium Alginate/Poly(ethylene oxide) Blend Nanofibers with Lecithin. Macromol. Res. 2010, 18, 891–896. [Google Scholar] [CrossRef]
- Norouzi, M.; Boroujeni, S.M.; Omidvarkordshouli, N.; Soleimani, M. Advances in Skin Regeneration: Application of Electrospun Scaffolds. Adv. Healthc. Mater. 2015, 4, 1114–1133. [Google Scholar] [CrossRef]
- Kataria, K.; Gupta, A.; Rath, G.; Mathur, R.B.; Dhakate, S.R. In vivo wound healing performance of drug loaded electrospun composite nanofibers transdermal patch. Int. J. Pharm. 2014, 469, 102–110. [Google Scholar] [CrossRef]
- Jeong, S.I.; Jeon, O.; Krebs, M.D.; Hill, M.C.; Alsberg, E. Biodegradable photo-crosslinked alginate nanofibre scaffolds with tuneable physical properties, cell adhesivity and growth factor release. Eur. Cells Mater. 2013, 24, 331–343. [Google Scholar] [CrossRef]
- Watthanaphanit, A.; Supaphol, P.; Tamura, H.; Tokura, S.; Rujiravanit, R. Fabrication, Structure, and Properties of Chitin Whisker-Reinforced Alginate Nanocomposite Fibers. J. Appl. Polym. Sci. 2008, 110, 890–899. [Google Scholar] [CrossRef]
- Mogoşanu, G.D.; Grumezescu, A.M. Natural and synthetic polymers for wounds and burns dressing. Int. J. Pharm. 2014, 463, 127–136. [Google Scholar] [CrossRef] [PubMed]
- Agren, M. Zinc in Wound repair. Arch. Derm. 1999, 135, 1273–1274. [Google Scholar] [CrossRef] [PubMed]
- Pielesz, A.; Machnicka, A.; Sarna, E. Antibacterial activity and scanning electron microscopy (SEM) examination of alginate-based films and wound dressings. Ecol. Chem. Eng. S 2011, 18, 197–210. [Google Scholar]
- Tamura, H.; Tsuruta, Y.; Tokura, S. Preparation of chitosan-coated alginate filament. Mater. Sci. Eng. C 2002, 20, 143–147. [Google Scholar] [CrossRef]
- Neibert, K.; Gopishetty, V.; Grigoryev, A.; Tokarev, I.; Al-Hajaj, N.; Vorstenbosch, J.; Philip, A.; Minko, S.; Maysinger, D. Wound-healing with mechanically robust and biodegradable hydrogel fibers loaded with silver nanoparticles. Adv. Healthc. Mater. 2012, 1, 621–630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kibungu, C.; Kondiah, P.P.D.; Kumar, P.; Choonara, Y.E. This Review Recent Advances in Chitosan and Alginate-Based Hydrogels for Wound Healing Application. Front. Mater. 2021, 8, 1960. [Google Scholar] [CrossRef]
- Gilmartin, D.J.; Alexaline, M.M.; Thrasivoulou, C.; Phillips, A.R.J.; Jayasinghe, S.N.; Becker, D.L. Integration of scaffolds into full-thickness skin wounds: The connexin response. Adv. Healthc. Mater. 2013, 2, 1151–1160. [Google Scholar] [CrossRef]
- Montaser, A.S.; Abdel-Mohsen, A.M.; Ramadan, M.A.; Sleem, A.A.; Sahffie, N.M.; Jancar, J.; Hebeish, A. Preparation and characterization of alginate/silver/nicotinamide nanocomposites for treating diabetic wounds. Int. J. Biol. Macromol. 2016, 92, 739–747. [Google Scholar] [CrossRef]
- Tsao, C.T.; Leung, M.; Chang, J.Y.-F.; Zhang, M. A simple material model to generate epidermal and dermal layers in vitro for skin regeneration. J. Mater. Chem. B 2014, 2, 5256–5264. [Google Scholar] [CrossRef]
- Zhang, H.; Cheng, J.; Ao, Q. Preparation of alginate-based biomaterials and their applications in biomedicine. Mar. Drugs 2021, 19, 264. [Google Scholar] [CrossRef]
- Kelso, M. The Importance of Acidic pH on Wound Healing the Importance of Acidic pH on Wound Healing—Why All the (pH)uss about Microenvironments? Wound Care Advisor: Doylestown, PA, USA, 2018; Available online: http://woundcareadvisor.com/wp-content/uploads/2018/09/Why-All-the-pHuss-About-Microenvironments.pdf (accessed on 31 May 2019).
- Martinotti, S.; Calabrese, G.; Ranzato, E. Honey and Wound Healing: New Solutions from an Old Remedy. In Wound Healing: Cellular Mechanisms, Alternative Therapies and Clinical Outcomes; Nova Science Publishers, Inc.: London, UK, 2015; pp. 43–48. ISBN 9781634634755. [Google Scholar]
- Ono, S.; Imai, R.; Ida, Y.; Shibata, D.; Komiya, T.; Matsumura, H. Increased wound pH as an indicator of local wound infection in second degree burns. Burns 2015, 41, 820–824. [Google Scholar] [CrossRef]
- Pawar, H.V.; Boateng, J.S.; Ayensu, I.; Tetteh, J. Multifunctional medicated lyophilised wafer dressing for effective chronic wound healing. J. Pharm. Sci. 2014, 103, 1720–1733. [Google Scholar] [CrossRef]
- Tamayol, A.; Akbari, M.; Zilberman, Y.; Comotto, M.; Lesha, E.; Serex, L.; Bagherifard, S.; Chen, Y.; Fu, G.; Ameri, S.K.; et al. Flexible pH-Sensing Hydrogel Fibers for Epidermal Applications. Adv. Healthc. Mater. 2016, 5, 711–719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Venugopal, V. Marine Products for Healthcare: Functional and Bioactive Nutraceutical Compounds from the Ocean; CRC Press Taylor & Francis Group: Boca Raton, FL, USA, 2009; ISBN 978-1-4200-5263-3. [Google Scholar]
- Hrynyk, M.; Martins-Green, M.; Barron, A.E.; Neufeld, R.J. Alginate-PEG sponge architecture and role in the design of insulin release dressings. Biomacromolecules 2012, 13, 1478–1485. [Google Scholar] [CrossRef] [PubMed]
- Rabbany, S.Y.; Pastore, J.; Yamamoto, M.; Miller, T.; Rafii, S.; Aras, R.; Penn, M. Continuous delivery of stromal cell-derived factor-1 from alginate scaffolds accelerates wound healing. Cell Transplant. 2010, 19, 399–408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tapia, C.; Escobar, Z.; Costa, E.; Sapag-Hagar, J.; Valenzuela, F.; Basualto, C.; Gai, M.N.; Yazdani-Pedram, M. Comparative studies on polyelectrolyte complexes and mixtures of chitosan-alginate and chitosan-carrageenan as prolonged diltiazem clorhydrate release systems. Eur. J. Pharm. Biopharm. 2004, 57, 65–75. [Google Scholar] [CrossRef]
- White, R.; Cowan, T.; Glover, D. Supporting evidence-based practice: A clinical review of TLC technology. J. Wound Care 2011, 1, 1–36. [Google Scholar]
- O’Donoghue, J.M.; O’Sullivan, S.T.; O’Shaughnessy, M.; O’Connor, T.P.F. Effects of a silicone-coated polyamide net dressing and calcium alginate on the healing of split skin graft donor sites: A prospective randomised trial. Acta Chir. Plast. 2000, 42, 3–6. [Google Scholar]
- Mitra, T.; Sailakshmi, G.; Gnanamani, A.; Raja, S.T.K.; Thiruselvi, T.; Gowri, V.M.; Selvaraj, N.V.; Ramesh, G.; Mandal, A.B. Preparation and characterization of a thermostable and biodegradable biopolymers using natural cross-linker. Int. J. Biol. Macromol. 2011, 48, 276–285. [Google Scholar] [CrossRef] [PubMed]
- Keshaw, H.; Forbes, A.; Day, R.M. Release of angiogenic growth factors from cells encapsulated in alginate beads with bioactive glass. Biomaterials 2005, 26, 4171–4179. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.S.; Lee, S.B.; Hong, S.R.; Lee, Y.M.; Song, K.W.; Park, M.H. Studies on gelatin-based sponges. Part III: A comparative study of cross-linked gelatin/alginate, gelatin/hyaluronate and chitosan/hyaluronate sponges and their application as a wound dressing in full-thickness skin defect of rat. J. Mater. Sci. Mater. Med. 2001, 12, 67–73. [Google Scholar] [CrossRef]
- Roh, D.H.; Kang, S.Y.; Kim, J.Y.; Kwon, Y.B.; Hae, Y.K.; Lee, K.G.; Park, Y.H.; Baek, R.M.; Heo, C.Y.; Choe, J.; et al. Wound healing effect of silk fibroin/alginate-blended sponge in full thickness skin defect of rat. J. Mater. Sci. Mater. Med. 2006, 17, 547–552. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Lee, H.C.; Oh, J.S.; Shin, B.A.; Oh, C.S.; Park, R.D.; Yang, K.S.; Cho, C.S. Polyelectrolyte complex composed of chitosan and sodium alginate for wound dressing application. J. Biomater. Sci. Polym. Ed. 1999, 10, 543–556. [Google Scholar] [CrossRef]
- Lira, A.A.M.; Rossetti, F.C.; Nanclares, D.M.A.; Neto, A.F.; Bentley, M.V.L.B.; Marchetti, J.M. Preparation and characterization of chitosan-treated alginate microparticles incorporating all-trans retinoic acid. J. Microencapsul. 2009, 26, 243–250. [Google Scholar] [CrossRef]
- Elçin, Y.M.; Dixit, V.; Gitnick, G. Extensive in vivo angiogenesis following controlled release of human vascular endothelial cell growth factor: Implications for tissue engineering and wound healing. Artif. Organs 2001, 25, 558–565. [Google Scholar] [CrossRef]
- Huizhou Foryou Medical Devices Co., Ltd. Luofucon Extra Silver Alginate Dressing (Rx Only)/Luofucon Antibacterial Alginate Wound Dressing (OTC) 2018. Available online: https://www.accessdata.fda.gov/cdrh_docs/pdf17/K172554.pdf (accessed on 31 May 2021).
- Luofucon PHMB Alginate Dressing (Rx Use) Premarket Notification. Available online: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpmn/pmn.cfm?ID=K201016 (accessed on 31 May 2021).
- Avino, A.; Cozma, C.-N.; Balcangiu-Stroescu, A.-E.; Tanasescu, M.-D.; Balan, D.G.; Timofte, D.; Stoicescu, S.M.; Hariga, C.-S.; Ionescu, D. Our Experience in Skin Grafting and Silver Dressing for Venous Leg Ulcers. Rev. Chim. 2019, 70, 742–744. [Google Scholar] [CrossRef]
- Rashaan, Z.M.; Krijnen, P.; van den Akker- van Marle, M.E.; van Baar, M.E.; Vloemans, A.F.P.; Dokter, J.; Tempelman, F.R.H.; van der Vlies, C.H.; Breederveld, R.S. Clinical effectiveness, quality of life and cost-effectiveness of Flaminal® versus Flamazine® in the treatment of partial thickness burns: Study protocol for a randomized controlled trial. Trials 2016, 17, 122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rashaan, Z.M.; Krijnen, P.; Kwa, K.A.A.; van der Vlies, C.H.; Schipper, I.B.; Breederveld, R.S. Flaminal® versus Flamazine® in the treatment of partial thickness burns: A randomized controlled trial on clinical effectiveness and scar quality (FLAM study). Wound Repair Regen. 2019, 27, 257–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porter, M.; Kelly, J. Pressure Ulcer Treatment in a Patient with Spina Bifida. Nurs. Stand. 2014, 28, 60–69. [Google Scholar] [CrossRef]
- Vivcharenko, V.; Przekora, A. Modifications of wound dressings with bioactive agents to achieve improved pro-healing properties. Appl. Sci. 2021, 11, 4114. [Google Scholar] [CrossRef]
- Rafter, L.; Reynolds, T.; Collier, M.; Rafter, M.; West, M. A clinical evaluation of Algivon® Plus manuka honey dressings for chronic wounds. Wounds UK 2017, 13, 132–140. [Google Scholar]
- Parker, J. Debridement of Chronic Leg Ulcers with Algivon. 2012. Available online: https://nl.advancismedical.com/uploads/files/documents/resources/UK/Debridement%20of%20chronic%20leg%20ulcers%20Algivon-%20Jane%20Parker.pdf (accessed on 28 August 2018).
- Activon® Manuka Honey. Available online: http://www.advancis.co.uk/uploads/files/files/ActivonWoundDressingGuide2015-A5V3.pdf (accessed on 27 August 2018).
- Algivon®—Alginate Dressing Impregnated with 100% Manuka Honey. Available online: http://www.advancis.co.uk/uploads/files/documents/resources/UK/AlgivonFactsheet.pdf (accessed on 27 August 2018).
- Preston, G. The Use of Activon® Tulle on a Venous Ulcer. Available online: https://uk.advancismedical.com/uploads/files/documents/resources/UK/Use%20of%20Activon%20Tulle%20on%20a%20venous%20ulcer(1).pdf (accessed on 28 August 2018).
- Activon® Tulle. Available online: http://www.advancis.co.uk/uploads/files/documents/resources/UK/ActivonTulle.pdf (accessed on 27 August 2018).
- Activon Tulle—Activon—Manuka Honey Dressings. Available online: http://www.advancis.co.uk/products/activon-manuka-honey/activon-tulle (accessed on 27 August 2018).
- Carella, S.; Maruccia, M.; Fino, P.; Onesti, M.G. An atypical case of Henoch-Shönlein purpura in a young patient: Treatment of the skin lesions with hyaluronic acid-based dressings. In Vivo 2013, 27, 147–152. [Google Scholar] [PubMed]
- Clark, R.; Bradbury, S. SILVERCEL® Non-Adherent made easy. Wounds Int. 2010, 1, 1–6. [Google Scholar]
- Rego, A. ALGS6 Ag Alginate Wound Dressing & AQUACEL Ag EXTRA Hydrofiber Dressing with Silver and Strengthening Fiber 2017. Available online: https://www.accessdata.fda.gov/cdrh_docs/pdf17/K172570.pdf (accessed on 29 August 2018).
- Scherr, G.H. Silver Alginate Foam Dressing: Silversite or Calgitrol 2006. pp. 202–211. Available online: https://www.accessdata.fda.gov/cdrh_docs/pdf4/K041268.pdf (accessed on 29 August 2018).
- Bhende, S.; Rothenburger, S. In Vitro Antimicrobial Effectiveness of 5 Catheter Insertion-Site Dressings. J. Assoc. Vasc. Access 2007, 12, 227–231. [Google Scholar] [CrossRef]
- Ullman, A.; Cooke, M.; Rickard, C. Examining the role of securement and dressing products to prevent central venous access device failure: A narrative review. J. Assoc. Vasc. Access 2015, 20, 99–110. [Google Scholar] [CrossRef]
- Donaghue, V.; Chrzan, J.; Rosenblum, B.; Giurini, J.; Habershaw, M.; Veves, A. Evaluation of a collagen-alginate wound dressing in the management of diabetic foot ulcers. Adv. Wound Care 1998, 11, 114–119. [Google Scholar] [PubMed]
- Sussman, C.; Bates-Jensen, B. Wound Care—A Collaborative Practice Manual for Health Professionals, 4th ed.; Sussman, C., Bates-Jensen, B.M., Eds.; Wolters Kluwer Health/Lippincott Williams & Wilkins: Baltimore, MD, USA; Philadelphia, PA, USA, 2012; Volume 53, ISBN 9788578110796. [Google Scholar]
- White, R. Flaminal: A novel approach to wound bioburden control. Wounds UK 2006, 2, 64–69. [Google Scholar]
- Park, S.O.; Han, J.; Minn, K.W.; Jin, U.S. Prevention of capsular contracture with Guardix-SG® after silicone implant insertion. Aesthetic Plast. Surg. 2013, 37, 543–548. [Google Scholar] [CrossRef]
- Sohn, E.J.; Ahn, H.B.; Roh, M.S.; Ryu, W.Y.; Kwon, Y.H. Efficacy of temperature-sensitive guardix-sg for adhesiolysis in experimentally induced eyelid adhesion in rabbits. Ophthal. Plast. Reconstr. Surg. 2013, 29, 458–463. [Google Scholar] [CrossRef]
- Kaltostat—Product Sheet 2011. Available online: https://marketingworld.convatec.com/MarketPortCore/MediaFile/DownloadByApplication?applicationToken=dc038e44b0b0ee4d8616f7b6880b24551bfecf237645a04fb5b76ab792a36858&itemId=82f0feec-e798-41e6-8f81-e16dfd5f8757&mediaFileId=c4dca46b-d305-489c-b2cc-1b74979e08 (accessed on 30 August 2018).
- Boateng, J.S.; Matthews, K.H.; Stevens, H.N.E.; Eccleston, G.M. Wound healing dressings and drug delivery systems: A review. J. Pharm. Sci. 2008, 97, 2892–2923. [Google Scholar] [CrossRef]
- Caló, E.; Khutoryanskiy, V.V. Biomedical applications of hydrogels: A review of patents and commercial products. Eur. Polym. J. 2015, 65, 252–267. [Google Scholar] [CrossRef] [Green Version]
- Fonder, M.A.; Lazarus, G.S.; Cowan, D.A.; Aronson-Cook, B.; Kohli, A.R.; Mamelak, A.J. Treating the chronic wound: A practical approach to the care of nonhealing wounds and wound care dressings. J. Am. Acad. Dermatol. 2008, 58, 185–206. [Google Scholar] [CrossRef] [PubMed]
- Bale, S.; Baker, N.; Crook, H.; Rayman, A.; Rayman, G.; Harding, K.G. Exploring the use of an alginate dressing for diabetic foot ulcers. J. Wound Care 2001, 10, 81–84. [Google Scholar] [CrossRef] [PubMed]
- Ausili, E.; Paolucci, V.; Triarico, S.; Maestrini, C.; Murolo, D.; Focarelli, B.; Rendeli, C. Treatment of pressure sores in spina bifida patients with calcium alginate and foam dressings. Eur. Rev. Med. Pharmacol. Sci. 2013, 17, 1642–1647. [Google Scholar]
- Kammerlander, G.; Afarideh, R.; Baumgartner, A.; Berger, M.; Fischelmayer, K.; Hirschberger, G.; Hangler, W.; Huber, A.; Kramml, M.; Locherer, E.; et al. Silvercel: Level two—Case studies. Clinical experiences of using a silver hydroalginate dressing in Austria, Switzerland & Germany. J. Wound Care 2008, 17, 384–388. [Google Scholar] [PubMed]
- Meaume, S.; Vallet, D.; Nguyen Morere, M.; Téot, L. Silvercel: Level one—RCT Study Evaluation of a silver-releasing hydroalginate dressing in chronic wounds with signs of local infection. J. Wound Care 2005, 14, 411–419. [Google Scholar] [CrossRef] [Green Version]
- Bell, A.; Hart, J. Silvercel: Level three—In vivo studies. Evaluation of two absorbent silver dressings in a porcine partial-thickness excisional wound model. J. Wound Care 2007, 16, 445–453. [Google Scholar] [CrossRef]
- Edwards, J. Use of SILVERCEL® NON-ADHERENT on burn wounds: A case series. Wounds UK 2013, 9, 81–84. [Google Scholar]
- Silvercel Guidelines. Available online: www.woundsinternational.com/uploads/resources/d426e9e2f7575b30a7a42c5f5bbdb82a.pdf (accessed on 27 August 2018).
- Gray, D. SilvercelTM non-adherent dressing: Taking the pain out of antimicrobial use. Wounds UK 2009, 5, 118–120. [Google Scholar]
- Wiegand, C.; Heinze, T.; Hipler, U.C. Comparative in vitro study on cytotoxicity, antimicrobial activity, and binding capacity for pathophysiological factors in chronic wounds of alginate and silver-containing alginate. Wound Repair Regen. 2009, 17, 511–521. [Google Scholar] [CrossRef]
- Boonkaew, B.; Barber, P.M.; Rengpipat, S.; Supaphol, P.; Kempf, M.; He, J.; John, V.T.; Cuttle, L. Development and characterization of a novel, antimicrobial, sterile hydrogel dressing for burn wounds: Single-step production with gamma irradiation creates silver nanoparticles and radical polymerization. J. Pharm. Sci. 2014, 103, 3244–3253. [Google Scholar] [CrossRef] [Green Version]



| Composition | Study Type/Target | Ref. |
|---|---|---|
| 1% w/v Na ALG—0.1% w/v acacia gum—1 mg/mL ZnO-NPs | Characterization, healing effects and cytotoxicity on sheep fibroblasts, antibacterial activity | [29] |
| 0.5–2.5% w/v LF 200S ALG hydrogel emulsion + 0.9, 1.4, 2.8% Tween 80/Span 20/isopropyl myristate oil/Ketoprofen ratio 26:1.25:4:1 Ca2+/D (+) gluconic acid δ-lactone molar ratio: 1:2 Ketoprofen microemulsion: 0.9, 1.4, 2.8% | Characterization, drug release, scattering patterns | [56] |
| alginate dialdehyde (ADA)—gelatin—0.1 M borax | Characterization and in vivo study on rat model | [57] |
| 60:20:2:4 w/w Na ALG—chitin/chitosan—fucoidan hydrogel sheet | Sprague-Dawley rats with full thickness wounds, gives a moist wound environment, easy application and removal, migration, cytotoxicity assay | [62,63,64,65,66] |
| encapsulated TRAP—0.5% w/w chitosan—PV-Ca ALG hydrogel film | C57 black 6/CBA mice wound healing | [67] |
| 10 g ALG—4 mg trypan blue, 10 g ALG—10 µg VEGF | Drug release: in vitro and in vivo on NOD and SCID mice, angiogenesis | [68] |
| 1% heparin—1% Na ALG—bFGF | Characterization, angiogenesis and bFGF release profile in Wistar rats | [69] |
| 10 & 15% Polyvinyl pyrrolidone—0.5 and 1% ALG—0, 30, 50, 70, and 100 ppm Ag-NPs. | Characterization, crosslinking degree, antimicrobial activity. Best results: 0.5% ALG, 15% PVP, 70 ppm Ag-NPs | [48] |
| Polyurethane foam—pH-sensitive Na ALG-bentonite hydrogels 1:0, 0.7:0.3, 0.5:0.5, 0.3:0.7 | Characterization, drug release from foam, cytotoxicity | [70] |
| Micro-emulsion 20% Tea tree oil—1% w/v ALG hydrogel | Characterization, oil dispersion, antimicrobial effect | [71] |
| 10% Na ALG sulfate—CM11 peptide | Mouse wound healing | [72] |
| ALG—k-CG ratio: 5:5, 7:3, 8:2 ALG—i-CG ratio: 5:5, 7:3, 8:2 | Formation and characterization; cytotoxicity, cell encapsulation | [73] |
| VEGF—2 wt % Na ALG, VEGF—0.05% chitosan—2 wt % Na ALG VEGF—heparin-coated chitosan—2 wt % Na ALG | In vitro drug release | [74] |
| 2 wt % ALG—trypan blue, 2 wt % ALG—methylene blue, 2 wt % ALG—VEGF | In vitro drug release | [75,76] |
| PEG diacrylate—thiolated ALG bilayered hydrogel with small extracellular vesicles (sEVs) | Characterization, rats and rabbit full thickness wound size reduction, sEVs release, angiogenesis, collagen arrangement | [77] |
| Sr2+ loaded Na ALG aldehyde—polyetherimide (PEI) | Characterization, hydrogel self-healing behavior, in vitro cell response, cytotoxicity, rat wound healing | [78] |
| Composition | Study Type/Target | Ref. |
|---|---|---|
| 3.5% Na ALG—3% KCl—3.5% k-CG—3% CaCl2 Na ALG/k-CG weight ratio: 10:0, 9:1, 8:2, 7:3, 6:4, 5:5, 4:6, 3:7, 2:8, 1:9, 0:10 | Characterization and thermostability | [80] |
| ALG—k-CG ratio: 5:5, 7:3, 8:2 ALG—i-CG ratio: 5:5, 7:3, 8:2 | Formation and characterization; cytotoxicity, cell encapsulation | [73] |
| 3% w/v diclofenac—1–3% w/v Na CMC—0.5% w/v AlCl3 6H2O 3% w/v diclofenac—1–3% w/v Na ALG—5% w/v AlCl3 | Drug content and particle size, disintegration, friability and in vitro dissolution test, in vivo test on beagles | [50,81] |
| Na ALG/k-CG %: 100, 75:25, 50:50, 25:75 + 0.125 g Fe3O4 | Hydrogel magnetic beads characterization, drug release, swelling | [82] |
| 2% w/v high M Na ALG—VEGF | In vitro drug analysis | [83] |
| Beads of 1% Ca ALG—0.25% platelet lysate—0.03% vancomycin hydrochloride | Particle characterization, drug and PDGF AB release, PBS absorption, cell proliferation | [84] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barbu, A.; Neamtu, B.; Zăhan, M.; Iancu, G.M.; Bacila, C.; Mireșan, V. Current Trends in Advanced Alginate-Based Wound Dressings for Chronic Wounds. J. Pers. Med. 2021, 11, 890. https://doi.org/10.3390/jpm11090890
Barbu A, Neamtu B, Zăhan M, Iancu GM, Bacila C, Mireșan V. Current Trends in Advanced Alginate-Based Wound Dressings for Chronic Wounds. Journal of Personalized Medicine. 2021; 11(9):890. https://doi.org/10.3390/jpm11090890
Chicago/Turabian StyleBarbu, Andreea, Bogdan Neamtu, Marius Zăhan, Gabriela Mariana Iancu, Ciprian Bacila, and Vioara Mireșan. 2021. "Current Trends in Advanced Alginate-Based Wound Dressings for Chronic Wounds" Journal of Personalized Medicine 11, no. 9: 890. https://doi.org/10.3390/jpm11090890