
Novel Digital Measurement Technique to Analyze the Palatine Suture Expansion after Palatine Rapid Maxillary Expansion Technique

 ,
,  and
and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design
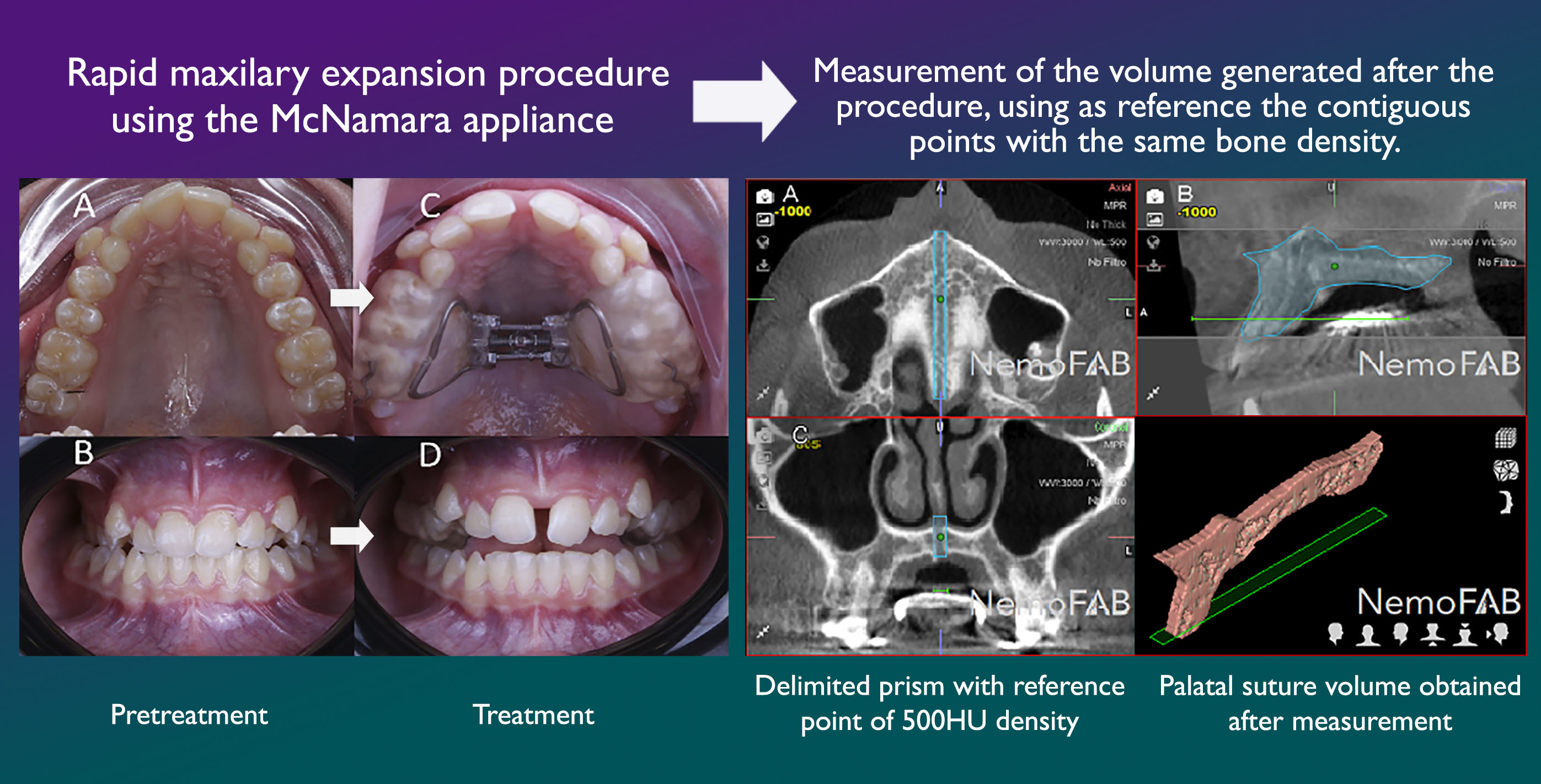
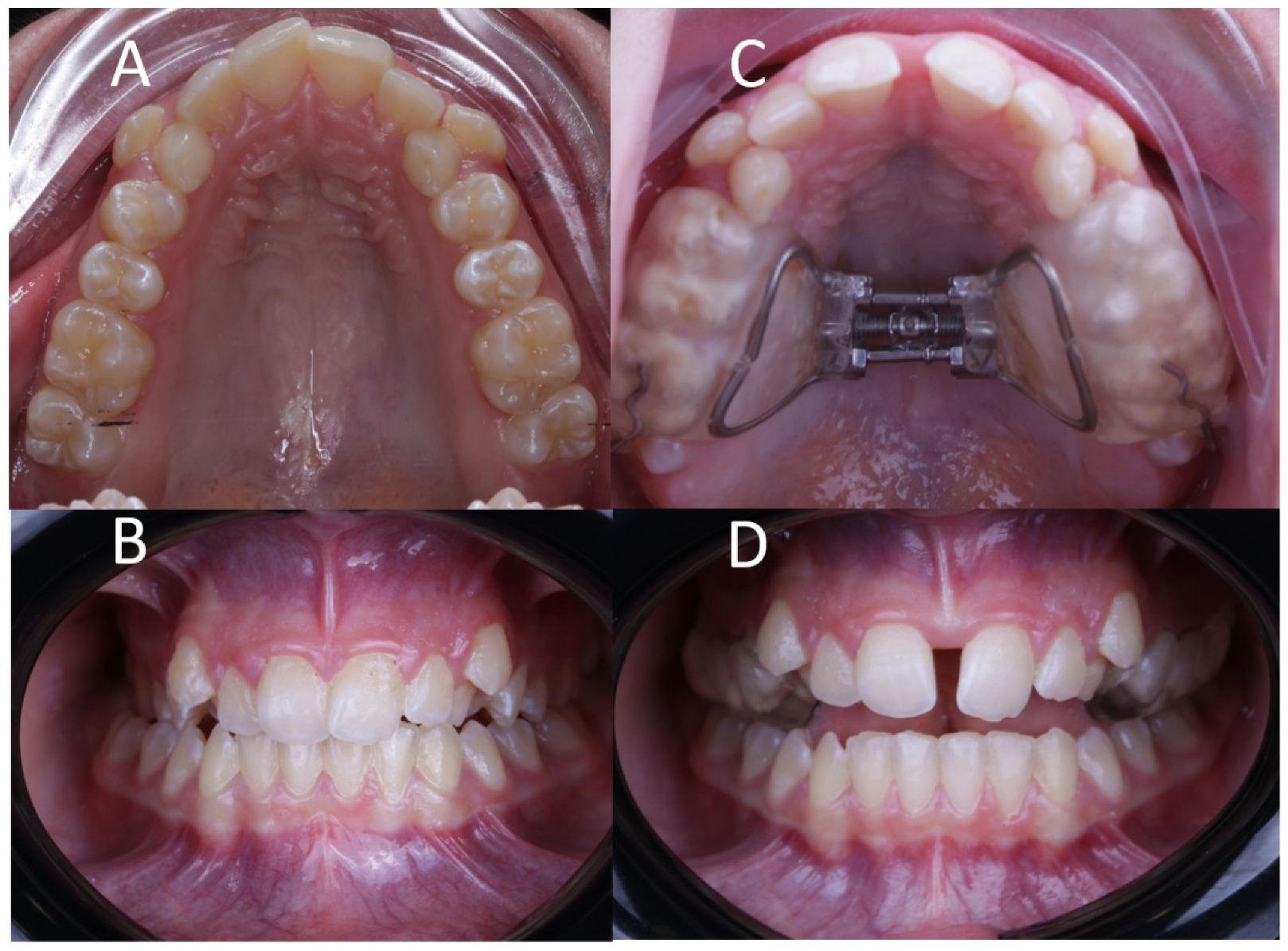
2.2. Clinical Procedure
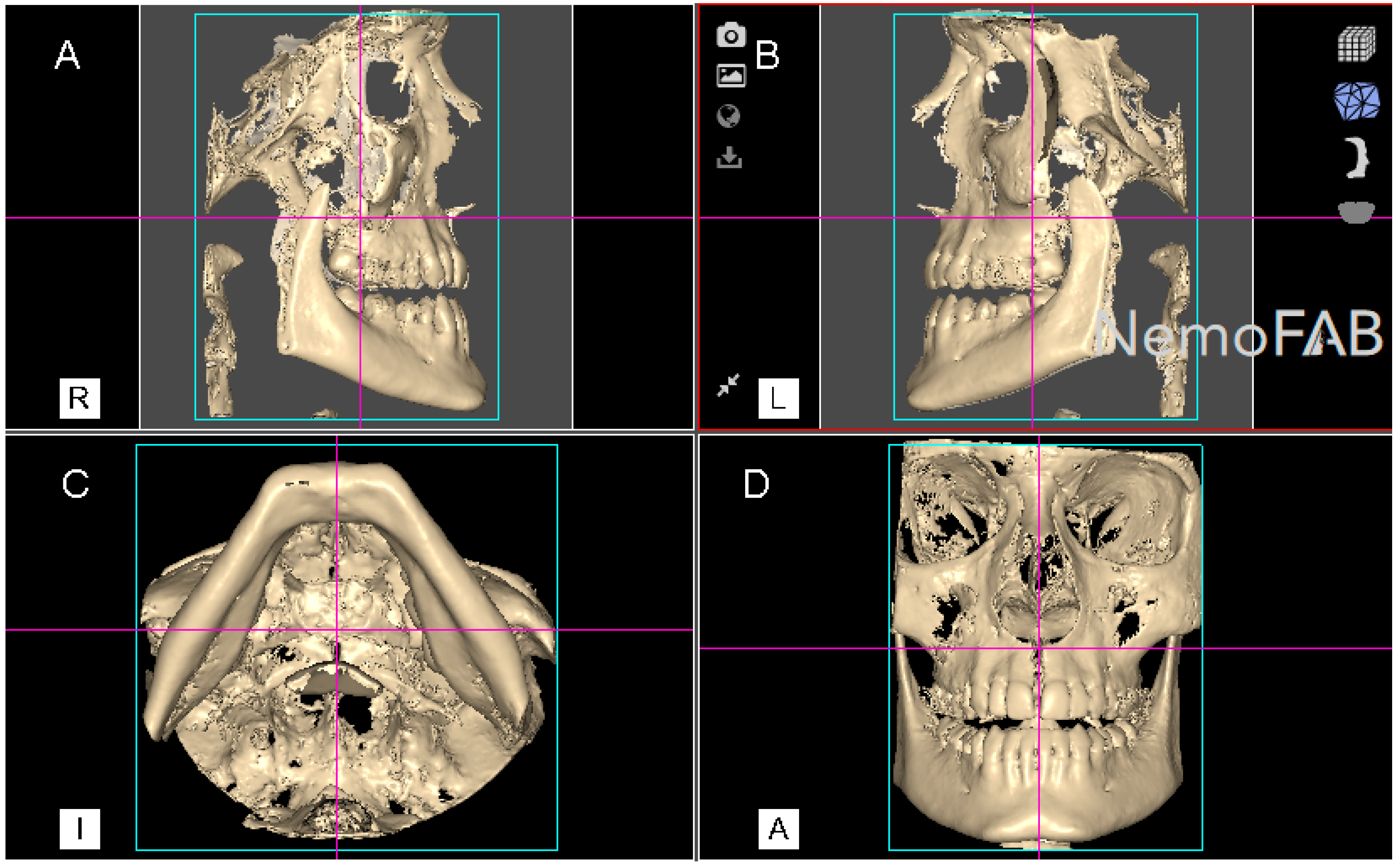
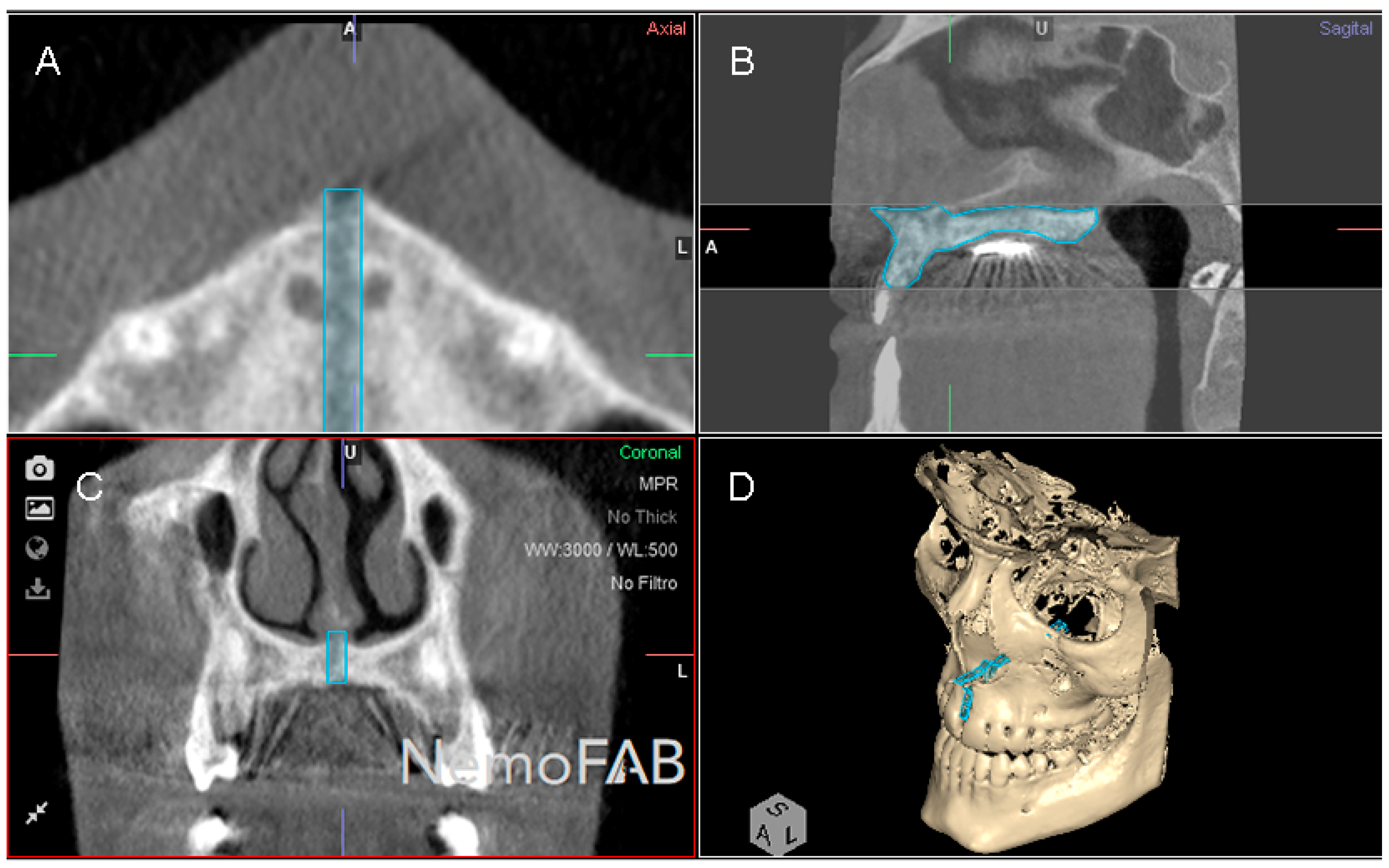
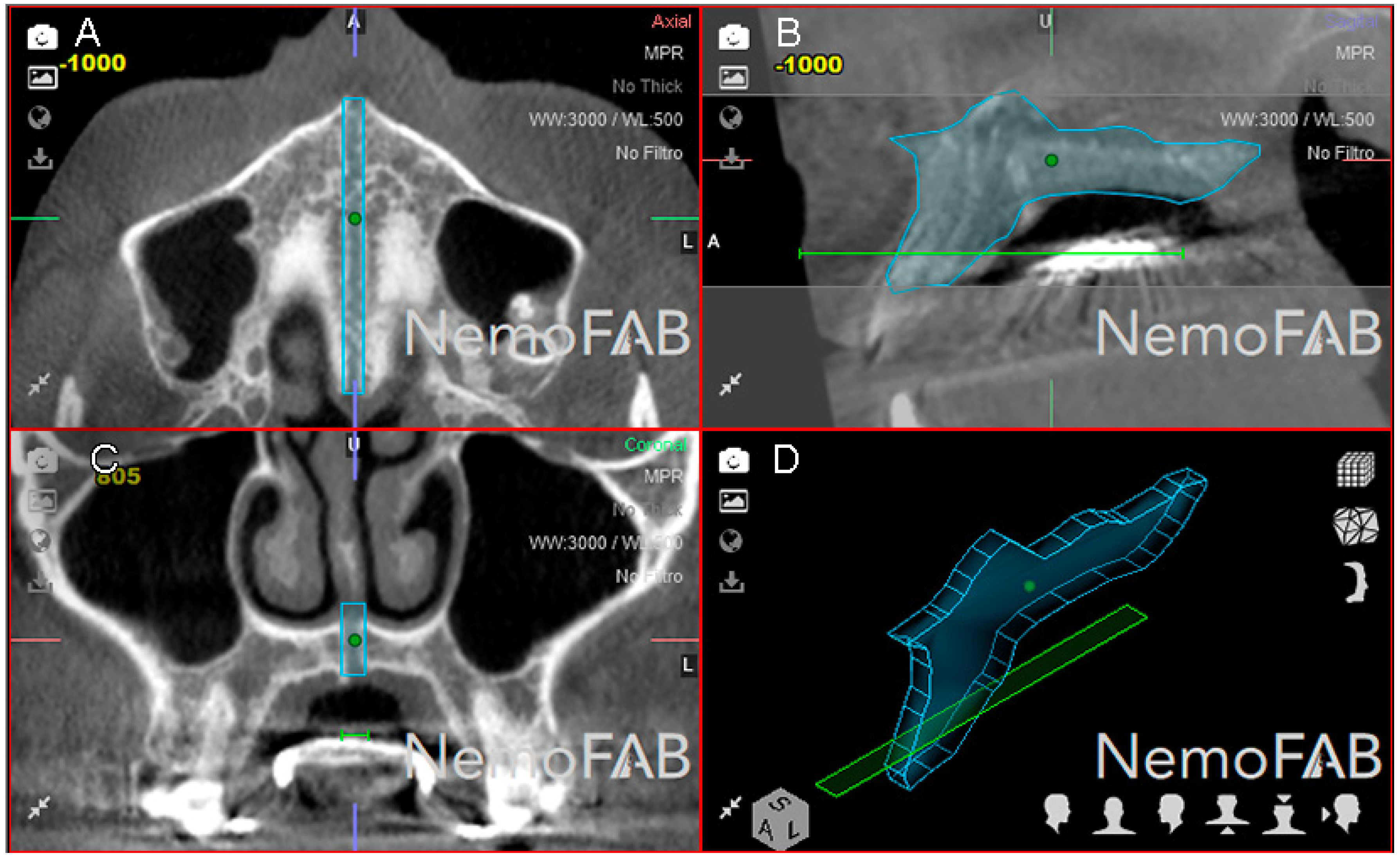
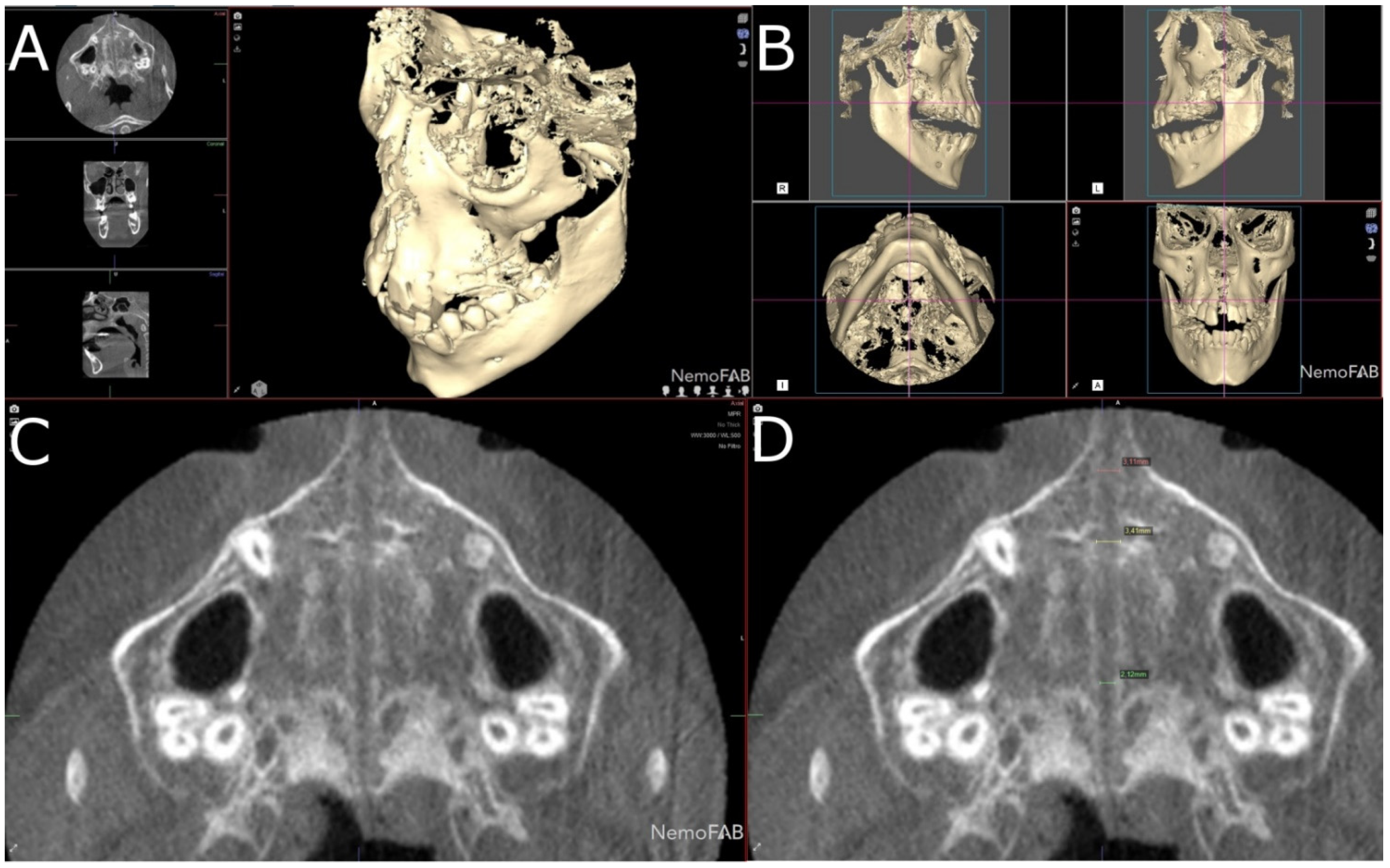
2.3. Measurement Procedure
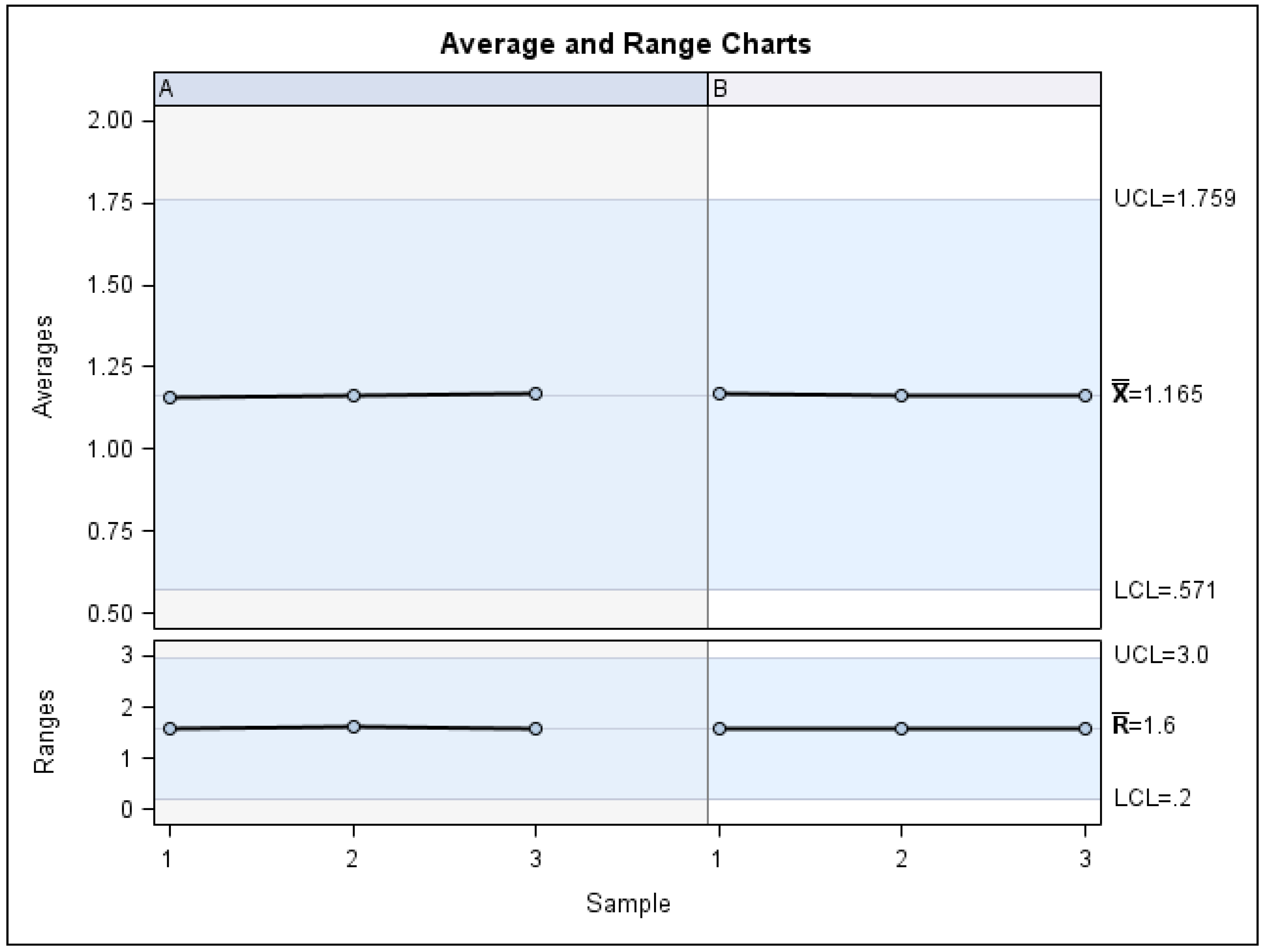
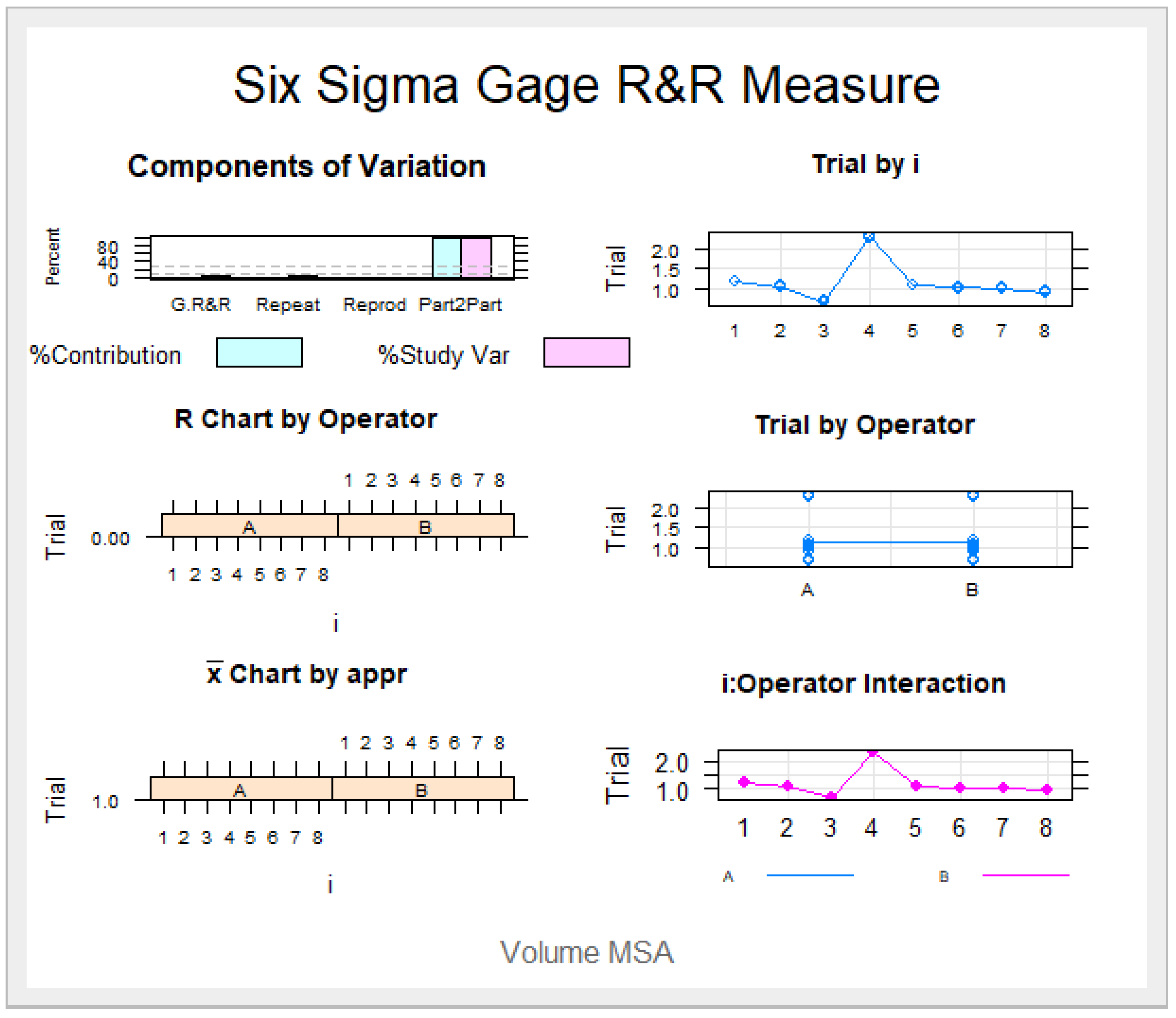
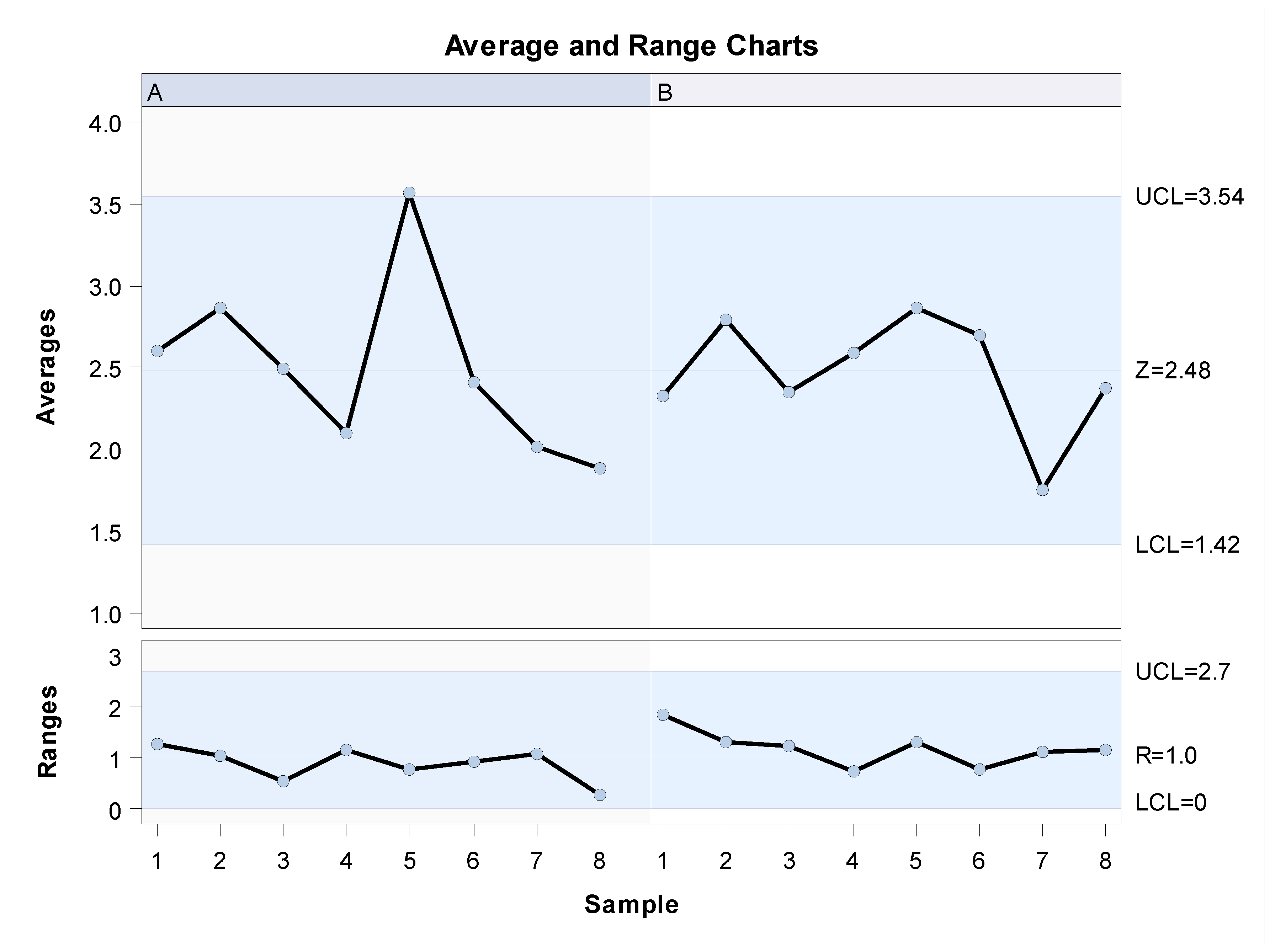
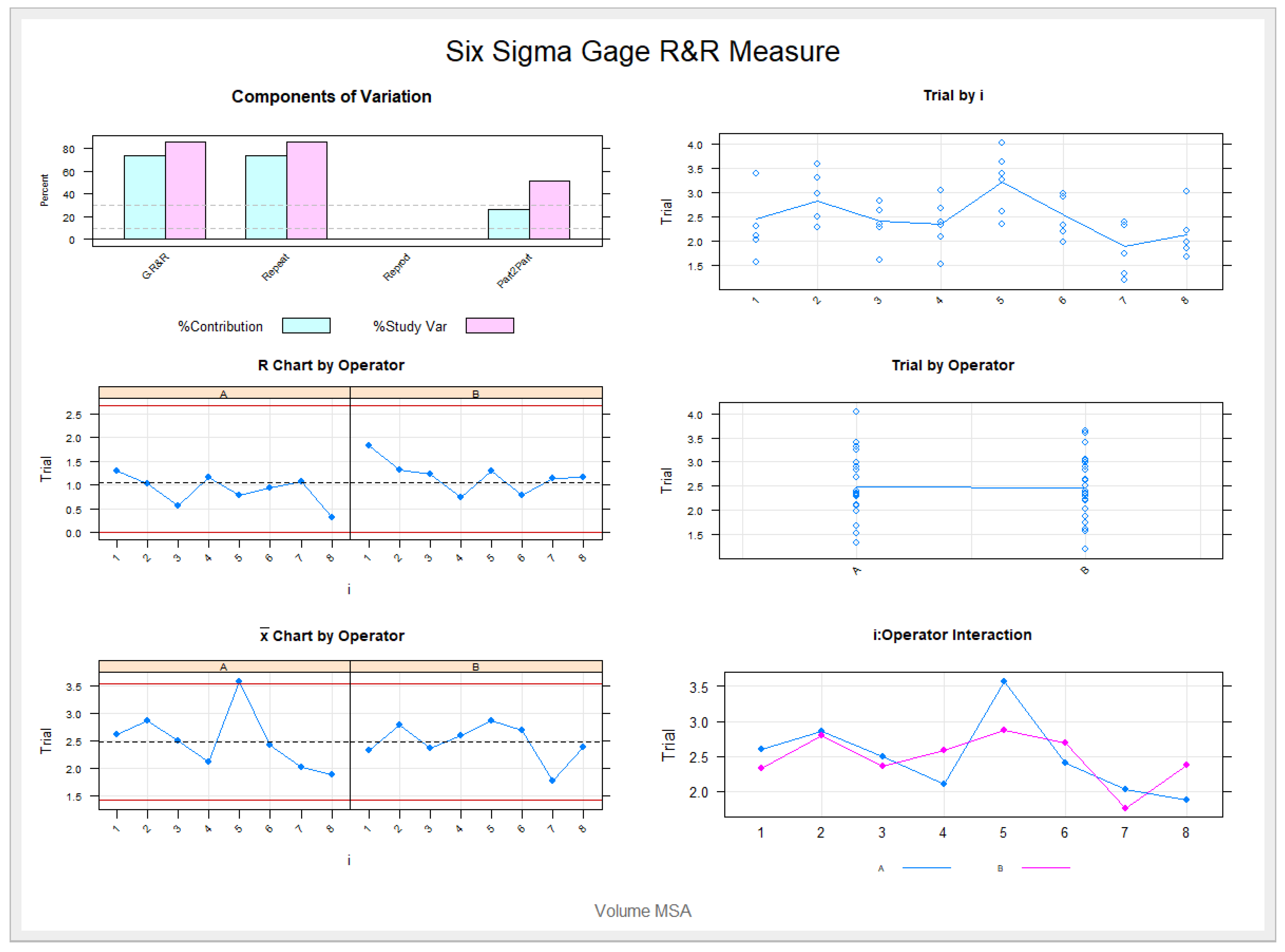
2.4. Validation of the Repeatability and Reproducibility
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Garrett, B.J.; Caruso, J.M.; Rungcharassaeng, K.; Farrage, J.R.; Kim, J.S.; Taylor, G.D. Skeletal effects to the maxilla after rapid maxillary expansion assessed with cone-beam computed tomography. Am. J. Orthod. Dentofac. Orthop. 2008, 134, 8.e1–8.e11. [Google Scholar] [CrossRef]
- Angell, E.C. Treatment of irregularities of the permanent or adult teeth. Dent. Cosmos 1860, 1, 540–544. [Google Scholar]
- Haas, A.J. Palatal expansion: Just the beginning of dentofacial orthopedics. Am. J. Orthod. 1970, 57, 219–255. [Google Scholar] [CrossRef]
- Kanomi, R.; Deguchi, T.; Kakuno, E.; Takano-Yamamoto, T.; Roberts, W.E. CBCT of skeletal changes following rapid maxillary expansion to increase arch-length with a development-dependent bonded or banded appliance. Angle Orthod. 2013, 83, 851–857. [Google Scholar] [CrossRef]
- Sánchez-Súcar, A.-M.; Sánchez-Súcar, F.-D.B.; Almerich-Silla, J.-M.; Paredes-Gallardo, V.; Montiel-Company, J.M.; García-Sanz, V.; Bellot-Arcís, C.; Sanchez-Sucar, F. Effect of rapid maxillary expansion on sleep apnea-hypopnea syndrome in growing patients. A meta-analysis. J. Clin. Exp. Dent. 2019, 11, e759–e767. [Google Scholar] [CrossRef]
- McNamara, J.A.; Lione, R.; Franchi, L.; Angelieri, F.; Cevidanes, L.H.; Darendeliler, M.A.; Cozza, P. The role of rapid maxillary expansion in the promotion of oral and general health. Prog. Orthod. 2015, 16, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogawa, T.; Enciso, R.; Shintaku, W.H.; Clark, G.T. Evaluation of cross-section airway configuration of obstructive sleep apnea. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2007, 103, 102–108. [Google Scholar] [CrossRef] [Green Version]
- Avrahami, E.; Solomonovich, A.; Englender, M. Axial CT measurements of the cross-sectional area of the oropharynx in adults with obstructive sleep apnea syndrome. Am. J. Neuroradiol. 1996, 17, 1107–1111. [Google Scholar]
- Lowe, A.A.; Fleetham, J.A.; Adachi, S.; Ryan, C. Cephalometric and computed tomographic predictors of obstructive sleep apnea severity. Am. J. Orthod. Dentofac. Orthop. 1995, 107, 589–595. [Google Scholar] [CrossRef]
- Lo Giudice, A.; Ronsivalle, V.; Lagravere, M.; Leonardi, R.; Martina, S.; Isola, G. Transverse dentoalveolar response of mandibular arch after rapid maxillary expansion (RME) with tooth-borne and bone-borne appliances. Angle Orthod. 2020, 90, 680–687. [Google Scholar] [CrossRef]
- Bazargani, F.; Feldmann, I.; Bondemark, L. Three-dimensional analysis of effects of rapid maxillary expansion on facial sutures and bones: A systematic review. Angle Orthod. 2013, 83, 1074–1082. [Google Scholar] [CrossRef]
- Loddi, P.P.; Pereira, M.D.; Wolosker, A.B.; Hino, C.T.; Kreniski, T.M.; Ferreira, L.M. Transverse Effects After Surgically Assisted Rapid Maxillary Expansion in the Midpalatal Suture Using Computed Tomography. J. Craniofacial Surg. 2008, 19, 433–438. [Google Scholar] [CrossRef]
- Pereira, J.D.S.; Jacob, H.B.; Locks, A.; Brunetto, M.; Ribeiro, G.L.U. Evaluation of the rapid and slow maxillary expansion using cone-beam computed tomography: A randomized clinical trial. Dent. Press J. Orthod. 2017, 22, 61–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cantarella, D.; Dominguez-Mompell, R.; Mallya, S.M.; Moschik, C.; Pan, H.C.; Miller, J.; Moon, W. Changes in the midpalatal and pterygopalatine sutures induced by micro-implant-supported skeletal expander, analyzed with a novel 3D method based on CBCT imaging. Prog. Orthod. 2017, 18, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Ballanti, F.; Lione, R.; Fanucci, E.; Franchi, L.; Baccetti, T.; Cozza, P. Immediate and Post-Retention Effects of Rapid Maxillary Expansion Investigated by Computed Tomography in Growing Patients. Angle Orthod. 2009, 79, 24–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lione, R.; Franchi, L.; Cozza, P. Does rapid maxillary expansion induce adverse effects in growing subjects? Angle Orthod. 2012, 83, 172–182. [Google Scholar] [CrossRef] [Green Version]
- Gryson, J.A. Changes in mandibular interdental distance concurrent with rapid maxillary expansion. Angle Orthod. 1977, 47, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Baratieri, C.; Alves, M.; Bolognese, A.M.; Nojima, M.C.G.; Nojima, L.I. Changes in skeletal and dental relationship in Class II Division I malocclusion after rapid maxillary expansion: A prospective study. Dental. Press J. Orthod. 2014, 19, 75–81. [Google Scholar] [CrossRef] [Green Version]
- Ghoneima, A.; Abdel-Fattah, E.; Eraso, F.; Fardo, D.; Kula, K.; Hartsfield, J. Skeletal and dental changes after rapid maxillary expansion: A computed tomography study. Aust. Orthod. J. 2010, 26, 141–148. [Google Scholar] [PubMed]
- Bruder, C.; Ortolani, C.L.F.; De Lima, T.A.; Artese, F.; Junior, K.F. Evaluation of palate area before and after rapid maxillary expansion, using cone-beam computed tomography. Dent. Press J. Orthod. 2019, 24, 40–45. [Google Scholar] [CrossRef] [Green Version]
- Primožič, J.; Baccetti, T.; Franchi, L.; Richmond, S.; Farčnik, F.; Ovsenik, M. Three-dimensional assessment of palatal change in a controlled study of unilateral posterior crossbite correction in the primary dentition. Eur. J. Orthod. 2011, 35, 199–204. [Google Scholar] [CrossRef] [Green Version]
- Marini, I.; Bonetti, G.A.; Achilli, V.; Salemi, G. A photogrammetric technique for the analysis of palatal three-dimensional changes during rapid maxillary expansion. Eur. J. Orthod. 2006, 29, 26–30. [Google Scholar] [CrossRef] [Green Version]
- Melgaço, C.A.; Columbano, J.; Jurach, E.M.; Nojima, M.D.C.G.; Sant’Anna, E.F.; Nojima, L.I. Rapid maxillary expansion effects: An alternative assessment method by means of cone-beam tomography. Dent. Press J. Orthod. 2014, 19, 88–96. [Google Scholar] [CrossRef]
- Sam, A.; Currie, K.; Oh, H.; Flores-Mir, C.; Lagravére-Vich, M. Reliability of different three-dimensional cephalometric landmarks in cone-beam computed tomography: A systematic review. Angle Orthod. 2018, 89, 317–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Angelieri, F.; Cevidanes, L.H.; Franchi, L.; Gonçalves, R.; Benavides, E.; McNamara, J.A., Jr. Midpalatal suture maturation: Classification method for individual assessment before rapid maxillary expansion. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 759–769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nota, A.; Tecco, S.; Caruso, S.; Severino, M.; Gatto, R.; Baldini, A. Analysis of errors in following the rapid maxillary expansion activation protocol: An observational study. Eur. J. Paediatr. Dent. 2019, 20, 116–118. [Google Scholar] [PubMed]
- Buzatu, R.; Nagib, R.; Dincă, M.; Vâlceanu, A.S.; Szuhanek, C.A. Midpalatal suture morphology and bone density evaluation after orthodontic expansion: A cone-bean computed tomography study in correlation with aesthetic parameters. Rom. J. Morphol. Embryol. 2018, 59, 803–809. [Google Scholar] [PubMed]
- Ghoneima, A.; Abdel-Fattah, E.; Hartsfield, J.; El-Bedwehi, A.; Kamel, A.; Kula, K. Effects of rapid maxillary expansion on the cranial and circummaxillary sutures. Am. J. Orthod. Dentofac. Orthop. 2011, 140, 510–519. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.; Xu, T.; Zou, W. Effects of rapid maxillary expansion on the midpalatal suture: A systematic review. Eur. J. Orthod. 2015, 37, 651–655. [Google Scholar] [CrossRef] [Green Version]
- Ludlow, J.B.; Gubler, M.; Cevidanes, L.; Mol, A. Precision of cephalometric landmark identification: Cone-beam computed tomography vs conventional cephalometric views. Am. J. Orthod. Dentofacial Orthop. 2009, 136, 312.e1–312.e10. [Google Scholar] [CrossRef] [Green Version]
- Lagravère, M.O.; Low, C.; Flores-Mir, C.; Chung, R.; Carey, J.; Heo, G.; Major, P.W. Intraexaminer and interexaminer reliabilities of landmark identification on digitized lateral cephalograms and formatted 3-dimensional cone-beam computerized tomography images. Am. J. Orthod. Dentofac. Orthop. 2010, 137, 598–604. [Google Scholar] [CrossRef]
- Van Vlijmen, O.J.C.; Maal, T.; Berg´e, S.J.; Bronkhorst, E.M.; Katsaros, C.; Kuijpers-Jagtman, A.M. A comparison between 2D and 3D cephalometry on CBCT scans of human skulls. Int. J. Oral Maxillofac. Surg. 2010, 39, 156–160. [Google Scholar] [CrossRef] [PubMed]
- Baka, Z.M.; Akin, M.; Uçar, F.I.; Ileri, Z.; Akın, M. Cone-beam computed tomography evaluation of dentoskeletal changes after asymmetric rapid maxillary expansion. Am. J. Orthod. Dentofac. Orthop. 2015, 147, 61–71. [Google Scholar] [CrossRef]
- Lagravère, M.O.; Heo, G.; Major, P.W.; Flores-Mir, C. Meta-analysis of immediate changes with rapid maxillary expansion treatment. J. Am. Dent. Assoc. 2006, 137, 44–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pangrazio-Kulbersh, V.; Wine, P.; Haughey, M.; Pajtas, B.; Kaczynski, R. Cone beam computed tomography evaluation of changes in the naso-maxillary complex associated with two types of maxillary expanders. Angle Orthod. 2012, 82, 448–457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christie, K.F.; Boucher, N.; Chung, C.-H. Effects of bonded rapid palatal expansion on the transverse dimensions of the maxilla: A cone-beam computed tomography study. Am. J. Orthod. Dentofac. Orthop. 2010, 137, S79–S85. [Google Scholar] [CrossRef] [PubMed]
- Mosleh, M.I.; Kaddah, M.A.; ElSayed, F.A.A.; ElSayed, H. Comparison of transverse changes during maxillary expansion with 4-point bone-borne and tooth-borne maxillary expanders. Am. J. Orthod. Dentofac. Orthop. 2015, 148, 599–607. [Google Scholar] [CrossRef]
- Koçer, G.; Sönmez, S.; Findik, Y.; Yazici, T. Reliability of the Linear Measurement (Contact) Method Compared with Stereophotogrammetry (Optical Scanning) for the Evaluation of Edema after Surgically Assisted Rapid Maxillary Expansion. Healthcare 2020, 8, 52. [Google Scholar] [CrossRef] [Green Version]
- Ricketts, R.M.; Roth, R.H.; Chaconas, S.J.; Schulhofr, J.; Engel, G.A. Orthodontic Diagnosis and Planning; Rocky Mountain Data Systems: Denver, CO, USA, 1982. [Google Scholar]
- Isfeld, D.; Flores-Mir, C.; Leon-Salazar, V.; Lagravère, M. Evaluation of a novel palatal suture maturation classification as assessed by cone-beam computed tomography imaging of a pre- and postexpansion treatment cohort. Angle Orthod. 2018, 89, 252–261. [Google Scholar] [CrossRef] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Operator | I | n | Mean | SD | Minimum | Maximum |
|---|---|---|---|---|---|---|
| A | 1 | 3 | 1.190 | 0.010 | 1.180 | 1.200 |
| 2 | 3 | 1.060 | 0.010 | 1.050 | 1.070 | |
| 3 | 3 | 0.693 | 0.015 | 0.680 | 0.710 | |
| 4 | 3 | 2.290 | 0.017 | 2.280 | 2.310 | |
| 5 | 3 | 1.107 | 0.015 | 1.090 | 1.120 | |
| 6 | 3 | 1.023 | 0.006 | 1.020 | 1.030 | |
| 7 | 3 | 1.007 | 0.021 | 0.990 | 1.030 | |
| 8 | 3 | 0.940 | 0.000 | 0.940 | 0.940 | |
| B | 1 | 3 | 1.193 | 0.012 | 1.180 | 1.200 |
| 2 | 3 | 1.063 | 0.015 | 1.050 | 1.080 | |
| 3 | 3 | 0.697 | 0.015 | 0.680 | 0.710 | |
| 4 | 3 | 2.290 | 0.026 | 2.260 | 2.310 | |
| 5 | 3 | 1.103 | 0.015 | 1.090 | 1.120 | |
| 6 | 3 | 1.037 | 0.006 | 1.030 | 1.040 | |
| 7 | 3 | 1.017 | 0.015 | 1.000 | 1.030 | |
| 8 | 3 | 0.927 | 0.021 | 0.910 | 0.950 |
| Operator | I | n | Mean | SD | Minimum | Maximum |
|---|---|---|---|---|---|---|
| A | 1 | 3 | 2.603 | 0.696 | 2.110 | 3.400 |
| 2 | 3 | 2.863 | 0.525 | 2.290 | 3.320 | |
| 3 | 3 | 2.490 | 0.305 | 2.280 | 2.840 | |
| 4 | 3 | 2.103 | 0.585 | 1.520 | 2.690 | |
| 5 | 3 | 3.570 | 0.414 | 3.260 | 4.040 | |
| 6 | 3 | 2.410 | 0.469 | 1.980 | 2.910 | |
| 7 | 3 | 2.020 | 0.599 | 1.330 | 2.400 | |
| 8 | 3 | 1.880 | 0.173 | 1.680 | 1.980 | |
| B | 1 | 3 | 2.330 | 0.956 | 1.560 | 3.400 |
| 2 | 3 | 2.793 | 0.707 | 2.280 | 3.600 | |
| 3 | 3 | 2.353 | 0.660 | 1.600 | 2.830 | |
| 4 | 3 | 2.590 | 0.400 | 2.320 | 3.050 | |
| 5 | 3 | 2.870 | 0.688 | 2.350 | 3.650 | |
| 6 | 3 | 2.697 | 0.432 | 2.200 | 2.980 | |
| 7 | 3 | 1.753 | 0.565 | 1.200 | 2.330 | |
| 8 | 3 | 2.373 | 0.598 | 1.860 | 3.030 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Requena Pérez, M.; Zubizarreta-Macho, Á.; Colino Gallardo, P.; Albaladejo Martínez, A.; Garcovich, D.; Alvarado-Lorenzo, A. Novel Digital Measurement Technique to Analyze the Palatine Suture Expansion after Palatine Rapid Maxillary Expansion Technique. J. Pers. Med. 2021, 11, 962. https://doi.org/10.3390/jpm11100962
Requena Pérez M, Zubizarreta-Macho Á, Colino Gallardo P, Albaladejo Martínez A, Garcovich D, Alvarado-Lorenzo A. Novel Digital Measurement Technique to Analyze the Palatine Suture Expansion after Palatine Rapid Maxillary Expansion Technique. Journal of Personalized Medicine. 2021; 11(10):962. https://doi.org/10.3390/jpm11100962
Chicago/Turabian StyleRequena Pérez, Mariano, Álvaro Zubizarreta-Macho, Pedro Colino Gallardo, Alberto Albaladejo Martínez, Daniele Garcovich, and Alfonso Alvarado-Lorenzo. 2021. "Novel Digital Measurement Technique to Analyze the Palatine Suture Expansion after Palatine Rapid Maxillary Expansion Technique" Journal of Personalized Medicine 11, no. 10: 962. https://doi.org/10.3390/jpm11100962