
Clinical Significance of Peritumoral Adipose Tissue PET/CT Imaging Features for Predicting Axillary Lymph Node Metastasis in Patients with Breast Cancer

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
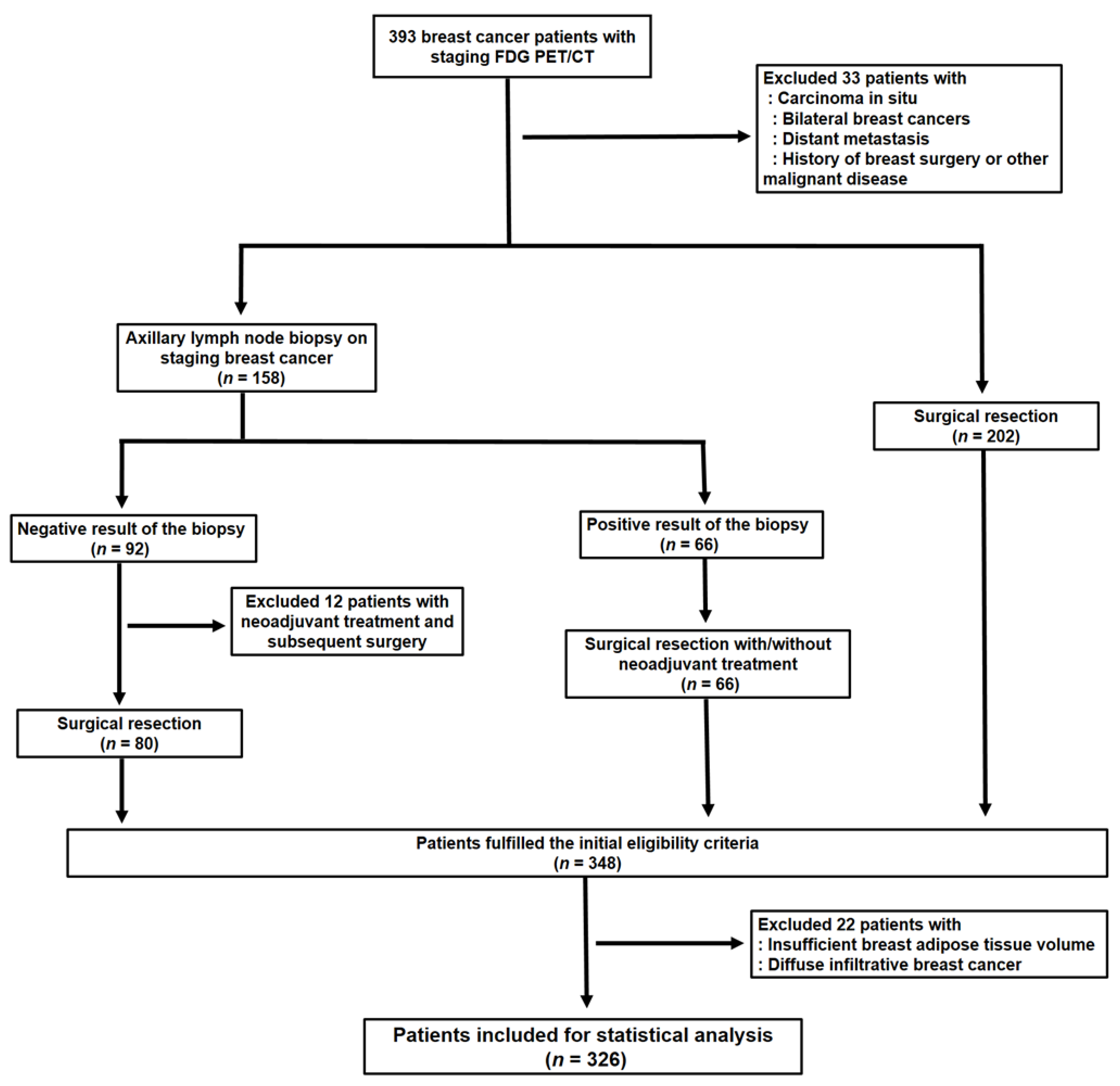
2.1. Study Population
2.2. FDG PET/CT Scans
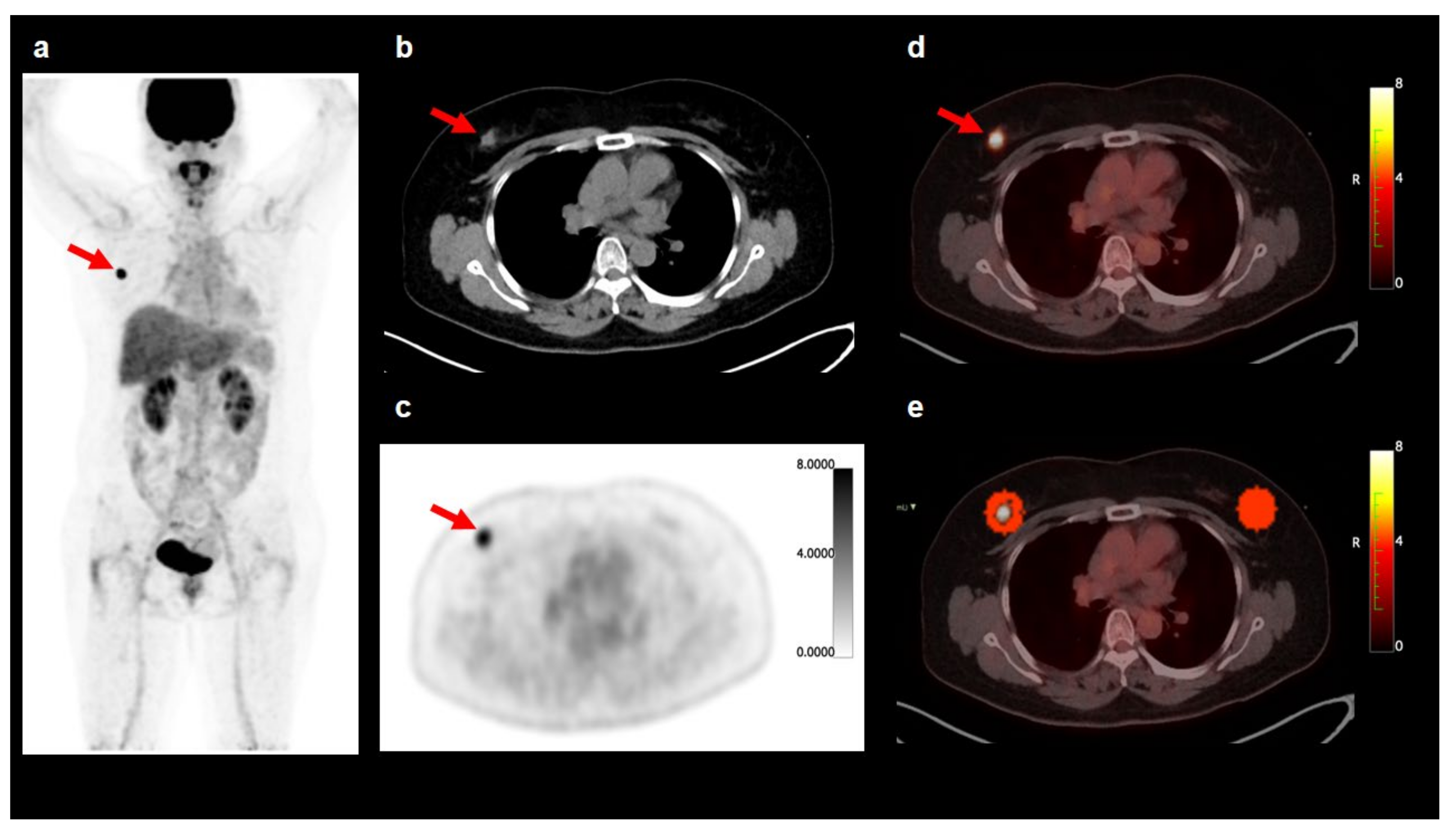
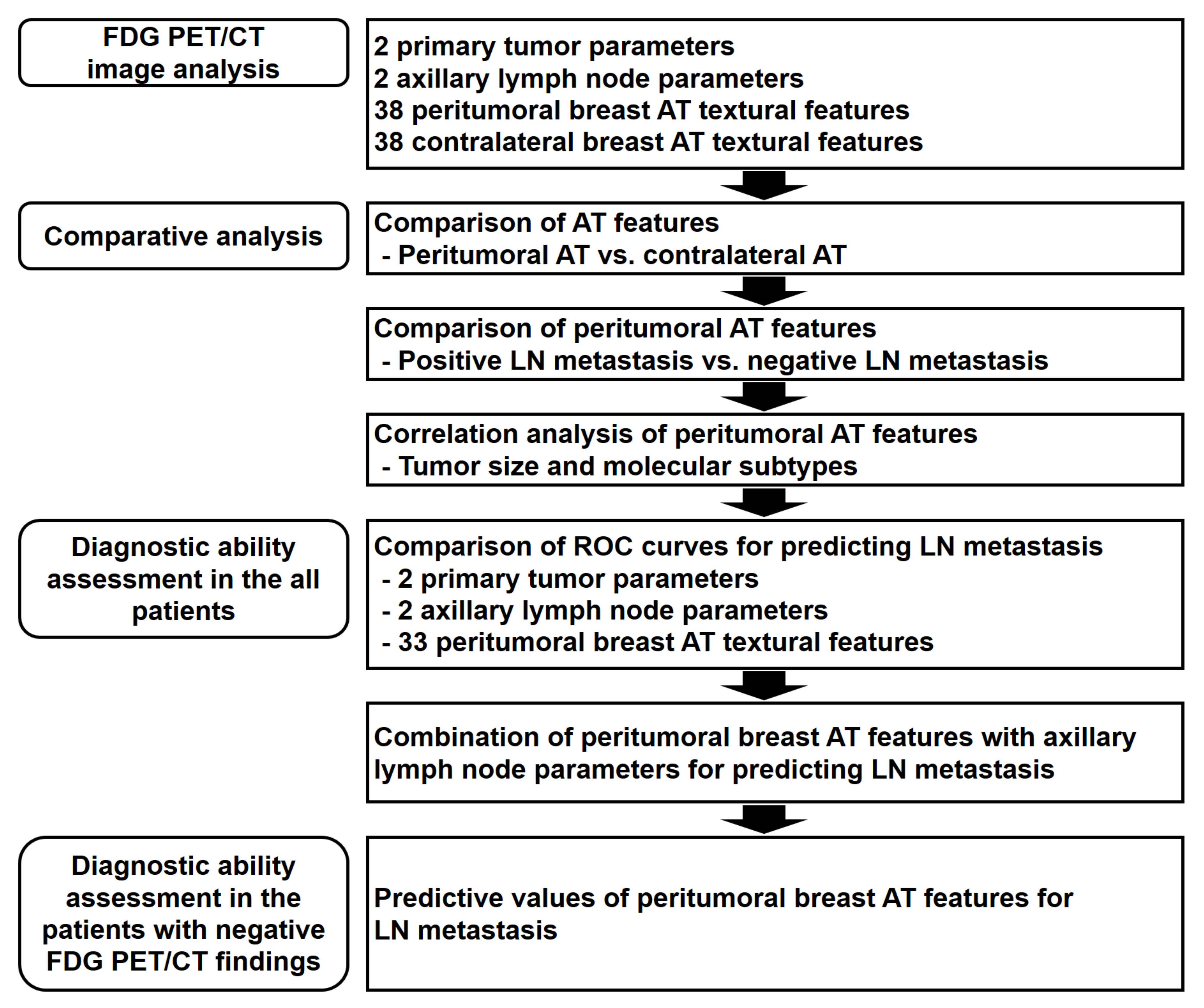
2.3. FDG PET/CT Image Analysis
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Comparison of Breast AT Imaging Features
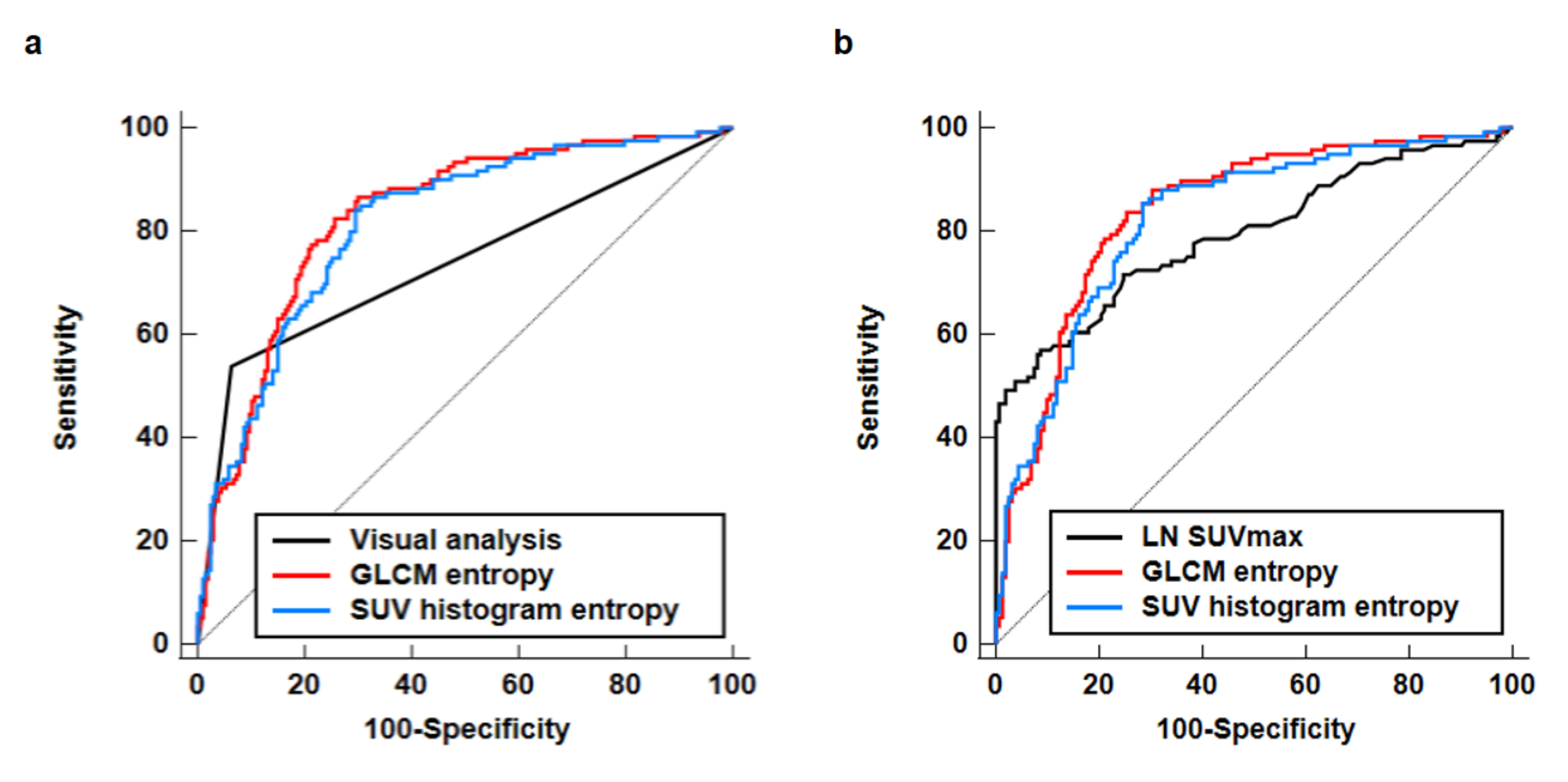
3.3. Diagnostic Ability for Predicting Axillary Lymph Node Metastasis
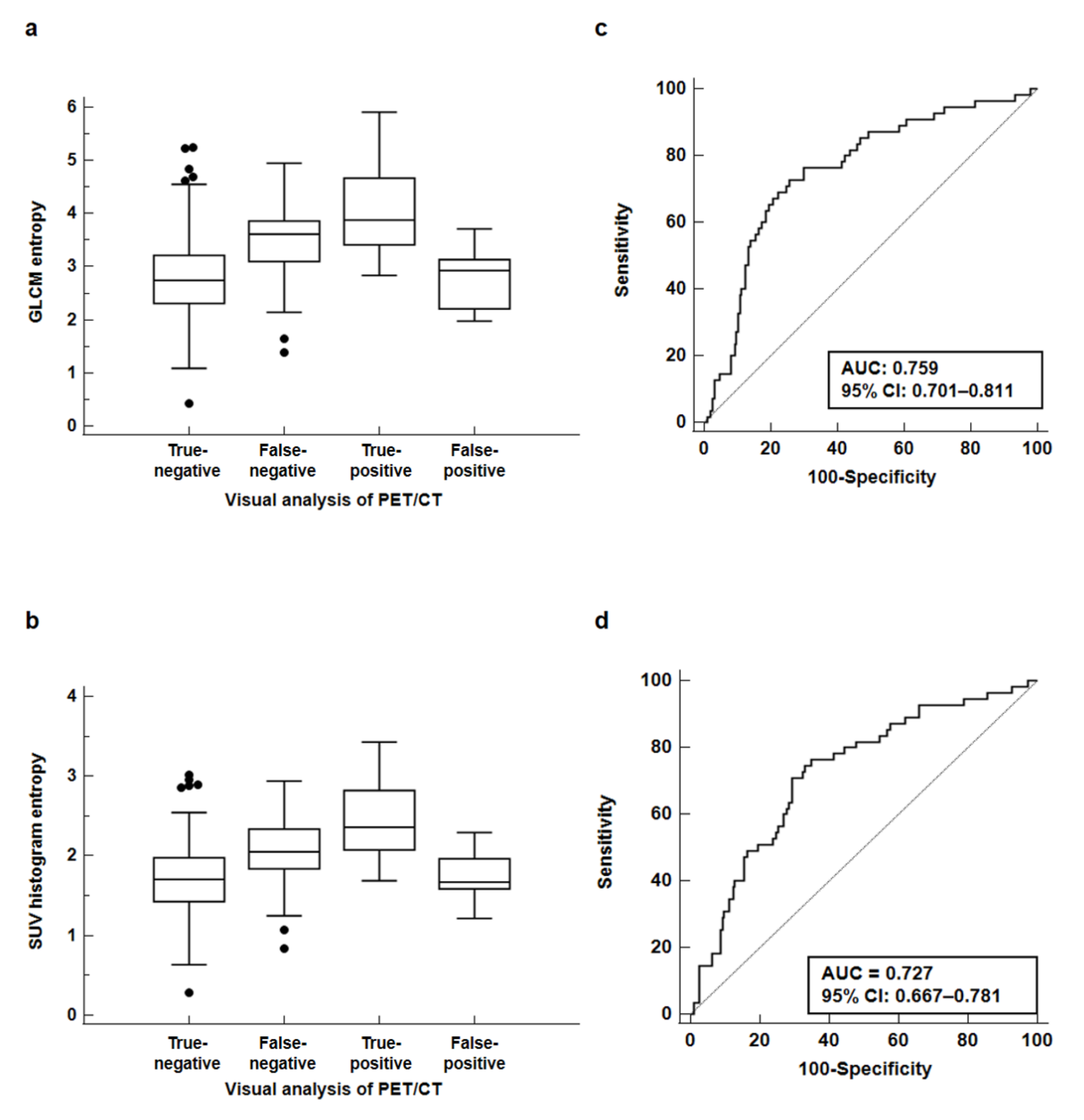
3.4. Predictive Value of GLCM Entropy and SUV Histogram Entropy in Patients with Negative Axillary Lymph Node Findings
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Brackstone, M.; Baldassarre, F.G.; Perera, F.E.; Cil, T.; Chavez Mac Gregor, M.; Dayes, I.S.; Engel, J.; Horton, J.K.; King, T.A.; Kornecki, A.; et al. Management of the axilla in early-stage breast cancer: Ontario Health (Cancer Care Ontario) and ASCO Guideline. J. Clin. Oncol. 2021, 39, 3056–3082. [Google Scholar] [CrossRef] [PubMed]
- Arriagada, R.; Le, M.G.; Dunant, A.; Tubiana, M.; Contesso, G. Twenty-five years of follow-up in patients with operable breast carcinoma: Correlation between clinicopathologic factors and the risk of death in each 5-year period. Cancer 2006, 106, 743–750. [Google Scholar] [CrossRef]
- Li, Z.; Kitajima, K.; Hirata, K.; Togo, R.; Takenaka, J.; Miyoshi, Y.; Kudo, K.; Ogawa, T.; Haseyama, M. Preliminary study of AI-assisted diagnosis using FDG-PET/CT for axillary lymph node metastasis in patients with breast cancer. EJNMMI Res. 2021, 11, 10. [Google Scholar] [CrossRef] [PubMed]
- Krag, D.N.; Anderson, S.J.; Julian, T.B.; Brown, A.M.; Harlow, S.P.; Ashikaga, T.; Weaver, D.L.; Miller, B.J.; Jalovec, L.M.; Frazier, T.G.; et al. Technical outcomes of sentinel-lymph-node resection and conventional axillary-lymph-node dissection in patients with clinically node-negative breast cancer: Results from the NSABP B-32 randomised phase III trial. Lancet Oncol. 2007, 8, 881–888. [Google Scholar] [CrossRef]
- Lumachi, F.; Basso, S.M.; Bonamini, M.; Marino, F.; Marzano, B.; Milan, E.; Waclaw, B.U.; Chiara, G.B. Incidence of arm lymphoedema following sentinel node biopsy, axillary sampling and axillary dissection in patients with breast cancer. In Vivo 2009, 23, 1017–1020. [Google Scholar] [PubMed]
- Wilke, L.G.; McCall, L.M.; Posther, K.E.; Whitworth, P.W.; Reintgen, D.S.; Leitch, A.M.; Gabram, S.G.; Lucci, A.; Cox, C.E.; Hunt, K.K.; et al. Surgical complications associated with sentinel lymph node biopsy: Results from a prospective international cooperative group trial. Ann. Surg. Oncol. 2006, 13, 491–500. [Google Scholar] [CrossRef] [PubMed]
- Sasada, S.; Masumoto, N.; Kimura, Y.; Kajitani, K.; Emi, A.; Kadoya, T.; Okada, M. Identification of axillary lymph node metastasis in patients with breast cancer using dual-phase FDG PET/CT. AJR Am. J. Roentgenol. 2019, 213, 1129–1135. [Google Scholar] [CrossRef]
- Kasem, J.; Wazir, U.; Mokbel, K. Sensitivity, specificity and the diagnostic accuracy of PET/CT for axillary staging in patients with stage I-III cancer: A systematic review of the literature. In Vivo 2021, 35, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Yoo, S.W.; Chowdhury, M.S.A.; Jeon, S.; Kang, S.R.; Lee, C.; Jabin, Z.; Kim, J.; Cho, S.G.; Song, H.C.; Bom, H.S.; et al. Clinical impact of F-18 FDG PET-CT on biopsy site selection in patients with suspected bone metastasis of unknown primary site. Nucl. Med. Mol. Imaging 2020, 54, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Song, B.I. A machine learning-based radiomics model for the prediction of axillary lymph-node metastasis in breast cancer. Breast. Cancer 2021, 28, 664–671. [Google Scholar] [CrossRef] [PubMed]
- Rybinska, I.; Mangano, N.; Tagliabue, E.; Triulzi, T. Cancer-associated adipocytes in breast cancer: Causes and consequences. Int. J. Mol. Sci. 2021, 22, 3775. [Google Scholar] [CrossRef] [PubMed]
- Duong, M.N.; Geneste, A.; Fallone, F.; Li, X.; Dumontet, C.; Muller, C. The fat and the bad: Mature adipocytes, key actors in tumor progression and resistance. Oncotarget 2017, 8, 57622–57641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalezic, A.; Udicki, M.; Srdic Galic, B.; Aleksic, M.; Korac, A.; Jankovic, A.; Korac, B. Tissue-specific warburg effect in breast cancer and cancer-associated adipose tissue-relationship between AMPK and glycolysis. Cancers 2021, 13, 2731. [Google Scholar] [CrossRef]
- Lee, J.W.; Kim, S.Y.; Lee, H.J.; Han, S.W.; Lee, J.E.; Lee, S.M. Prognostic significance of CT-attenuation of tumor-adjacent breast adipose tissue in breast cancer patients with surgical resection. Cancers 2019, 11, 1135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hisanaga, S.; Aoki, T.; Shimajiri, S.; Fujisaki, A.; Nakayama, T.; Hisaoka, M.; Hayashida, Y.; Inoue, Y.; Tashima, Y.; Korogi, Y. Peritumoral fat content correlates with histological prognostic factors in breast carcinoma: A study using iterative decomposition of water and fat with echo asymmetry and least-squares estimation (IDEAL). Magn. Reson. Med. Sci. 2021, 20, 28–33. [Google Scholar] [CrossRef] [Green Version]
- Obeid, J.P.; Stoyanova, R.; Kwon, D.; Patel, M.; Padgett, K.; Slingerland, J.; Takita, C.; Alperin, N.; Yepes, M.; Zeidan, Y.H. Multiparametric evaluation of preoperative MRI in early stage breast cancer: Prognostic impact of peri-tumoral fat. Clin. Transl. Oncol. 2017, 19, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Lee, S.M.; Chung, Y.A. Prognostic value of CT attenuation and FDG uptake of adipose tissue in patients with pancreatic adenocarcinoma. Clin. Radiol. 2018, 73, 1056.e1–1056.e10. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Son, M.W.; Chung, I.K.; Cho, Y.S.; Lee, M.S.; Lee, S.M. Significance of CT attenuation and F-18 fluorodeoxyglucose uptake of visceral adipose tissue for predicting survival in gastric cancer patients after curative surgical resection. Gastric. Cancer 2020, 23, 273–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.W.; Jeon, Y.S.; Kim, K.H.; Yang, H.J.; Lee, C.H.; Lee, S.M. Prognostic value of CT-attenuation and (18)F-fluorodeoxyglucose uptake of periprostatic adipose tissue in patients with prostate cancer. J. Pers. Med. 2020, 10, 185. [Google Scholar] [CrossRef] [PubMed]
- Kadrmas, D.J.; Casey, M.E.; Conti, M.; Jakoby, B.W.; Lois, C.; Townsend, D.W. Impact of time-of-flight on PET tumor detection. J. Nucl. Med. 2009, 50, 1315–1323. [Google Scholar] [CrossRef] [Green Version]
- Knäusl, B.; Rausch, I.F.; Bergmann, H.; Dudczak, R.; Hirtl, A.; Georg, D. Influence of PET reconstruction parameters on the TrueX algorithm. A combined phantom and patient study. Nuklearmedizin 2013, 52, 28–35. [Google Scholar] [CrossRef]
- Nioche, C.; Orlhac, F.; Boughdad, S.; Reuzé, S.; Goya-Outi, J.; Robert, C.; Pellot-Barakat, C.; Soussan, M.; Frouin, F.; Buvat, I. LIFEx: A freeware for radiomic feature calculation in multimodality imaging to accelerate advances in the characterization of tumor heterogeneity. Cancer Res. 2018, 78, 4786–4789. [Google Scholar] [CrossRef] [Green Version]
- Kang, J.; Lee, J.H.; Lee, H.S.; Cho, E.S.; Park, E.J.; Baik, S.H.; Lee, K.Y.; Park, C.; Yeu, Y.; Clemenceau, J.R.; et al. Radiomics features of (18)F-fluorodeoxyglucose positron-emission tomography as a novel prognostic signature in colorectal cancer. Cancers 2021, 13, 392. [Google Scholar] [CrossRef]
- Guezennec, C.; Bourhis, D.; Orlhac, F.; Robin, P.; Corre, J.B.; Delcroix, O.; Gobel, Y.; Schick, U.; Salaün, P.Y.; Abgral, R. Inter-observer and segmentation method variability of textural analysis in pre-therapeutic FDG PET/CT in head and neck cancer. PLoS ONE 2019, 14, e0214299. [Google Scholar] [CrossRef]
- Schisterman, E.F.; Perkins, N.J.; Liu, A.; Bondell, H. Optimal cut-point and its corresponding Youden Index to discriminate individuals using pooled blood samples. Epidemiology 2005, 16, 73–81. [Google Scholar] [CrossRef]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Dirat, B.; Bochet, L.; Dabek, M.; Daviaud, D.; Dauvillier, S.; Majed, B.; Wang, Y.Y.; Meulle, A.; Salles, B.; Le Gonidec, S.; et al. Cancer-associated adipocytes exhibit an activated phenotype and contribute to breast cancer invasion. Cancer Res. 2011, 71, 2455–2465. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.Y.; Attané, C.; Milhas, D.; Dirat, B.; Dauvillier, S.; Guerard, A.; Gilhodes, J.; Lazar, I.; Alet, N.; Laurent, V.; et al. Mammary adipocytes stimulate breast cancer invasion through metabolic remodeling of tumor cells. JCI Insight 2017, 2, e87489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freed, M.; Storey, P.; Lewin, A.A.; Babb, J.; Moccaldi, M.; Moy, L.; Kim, S.G. Evaluation of breast lipid composition in patients with benign tissue and cancer by using multiple gradient-echo MR imaging. Radiology 2016, 281, 43–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pahk, K.; Joung, C.; Kim, S. Visceral fat metabolic activity evaluated by preoperative (18) F-FDG PET/CT significantly affects axillary lymph node metastasis in postmenopausal luminal breast cancer. Sci. Rep. 2020, 10, 1348. [Google Scholar] [CrossRef] [Green Version]
- Han, M.S.; White, A.; Perry, R.J.; Camporez, J.P.; Hidalgo, J.; Shulman, G.I.; Davis, R.J. Regulation of adipose tissue inflammation by interleukin 6. Proc. Natl. Acad. Sci. USA 2020, 117, 2751–2760. [Google Scholar] [CrossRef] [Green Version]
- Zoico, E.; Rizzatti, V.; Darra, E.; Budui, S.L.; Franceschetti, G.; Vinante, F.; Pedrazzani, C.; Guglielmi, A.; De Manzoni, G.; Mazzali, G.; et al. Morphological and functional changes in the peritumoral adipose tissue of colorectal cancer patients. Obesity 2017, 25 (Suppl 2), S87–S94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piao, Y.J.; Kim, H.S.; Hwang, E.H.; Woo, J.; Zhang, M.; Moon, W.K. Breast cancer cell-derived exosomes and macrophage polarization are associated with lymph node metastasis. Oncotarget 2018, 9, 7398–7410. [Google Scholar] [CrossRef] [PubMed]
- Engin, A.B.; Engin, A.; Gonul, I.I. The effect of adipocyte-macrophage crosstalk in obesity-related breast cancer. J. Mol. Endocrinol. 2019, 62, R201–R222. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, J.; Ohtani, H.; Nakamura, K.; Shimokawa, I.; Kanematsu, T. Prognostic impact of marginal adipose tissue invasion in ductal carcinoma of the breast. Am. J. Clin. Pathol. 2008, 130, 382–388. [Google Scholar] [CrossRef]
- Yamaguchi, J.; Moriuchi, H.; Ueda, T.; Kawashita, Y.; Hazeyama, T.; Tateishi, M.; Aoki, S.; Uchihashi, K.; Nakamura, M. Active behavior of triple-negative breast cancer with adipose tissue invasion: A single center and retrospective review. BMC Cancer 2021, 21, 434. [Google Scholar] [CrossRef]
- Hotta, M.; Minamimoto, R.; Gohda, Y.; Miwa, K.; Otani, K.; Kiyomatsu, T.; Yano, H. Prognostic value of (18)F-FDG PET/CT with texture analysis in patients with rectal cancer treated by surgery. Ann. Nucl. Med. 2021, 35, 843–852. [Google Scholar] [CrossRef] [PubMed]
- Brown, P.J.; Zhong, J.; Frood, R.; Currie, S.; Gilbert, A.; Appelt, A.L.; Sebag-Montefiore, D.; Scarsbrook, A. Prediction of outcome in anal squamous cell carcinoma using radiomic feature analysis of pre-treatment FDG PET-CT. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 2790–2799. [Google Scholar] [CrossRef] [Green Version]
- Bailly, C.; Bodet-Milin, C.; Couespel, S.; Necib, H.; Kraeber-Bodéré, F.; Ansquer, C.; Carlier, T. Revisiting the robustness of PET-based textural features in the context of multi-centric trials. PLoS ONE 2016, 11, e0159984. [Google Scholar] [CrossRef]
- Kulahci, O.; Irkorucu, O.; Deveci, E.K.; Tas, Z.A. Relationship between lymph node metastasis and a low 18F-FDG PET/CT axillary suvmax value in breast cancer. J. Coll. Physicians Surg. Pak. 2021, 30, 511–516. [Google Scholar] [CrossRef] [PubMed]
- Kutluturk, K.; Simsek, A.; Comak, A.; Gonultas, F.; Unal, B.; Kekilli, E. Factors affecting the accuracy of (18)F-FDG PET/CT in evaluating axillary metastases in invasive breast cancer. Niger. J. Clin. Pract. 2019, 22, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Geng, J.; Zhang, X.; Prabhu, S.; Shahoei, S.H.; Nelson, E.R.; Swanson, K.S.; Anastasio, M.A.; Smith, A.M. 3D microscopy and deep learning reveal the heterogeneity of crown-like structure microenvironments in intact adipose tissue. Sci. Adv. 2021, 7, eave2480. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Number of Patients (%) | |
|---|---|---|
| Age (years) | 52 (30–85) 1 | |
| Obesity | Underweight/normal | 130 (39.9%) |
| Overweight/obesity | 196 (60.1%) | |
| Menopausal status | Premenopausal | 135 (41.4%) |
| Postmenopausal | 191 (58.6%) | |
| Histopathology | Intraductal carcinoma | 287 (88.0%) |
| Intralobular carcinoma | 39 (12.0%) | |
| Histologic grade | Grade 1 | 80 (24.6%) |
| Grade 2 | 160 (49.2%) | |
| Grade 3 | 85 (26.2%) | |
| Tumor size (cm) | 2.0 (0.4–15.0) 1 | |
| T stage | T1–T2 | 295 (90.5%) |
| T3–T4 | 31 (9.5%) | |
| Lymph node metastasis | No | 207 (63.5%) |
| Yes | 119 (36.5%) | |
| Molecular subtypes | Luminal A | 64 (19.6%) |
| Luminal B | 182 (55.8%) | |
| HER2-enriched (non-luminal) | 42 (12.9%) | |
| Triple-negative | 38 (11.7%) | |
| Maximum SUV of the primary tumor | 3.96 (1.50–37.90) 1 | |
| Maximum SUV of the axillary lymph node | 1.08 (0.36–27.07) 1 | |
| Neoadjuvant chemotherapy | No | 296 (90.8%) |
| Yes | 30 (9.2%) | |
| Treatment for primary breast cancer | Breast-conserving surgery | 229 (70.2%) |
| Total mastectomy | 97 (29.8%) | |
| Treatment for axillary lymph nodes | Sentinel lymph node biopsy | 184 (56.4%) |
| Axillary lymph node dissection | 142 (43.6%) | |
| Adjuvant treatment | No | 5 (1.5%) |
| CTx + RTx_HTx | 159 (48.8%) | |
| RTx + HTx | 94 (28.8%) | |
| HTx | 29 (8.9%) | |
| CTx | 16 (4.9%) | |
| CTx + HTx | 16 (4.9%) | |
| CTx + RTx | 4 (1.2%) | |
| RTx | 3 (0.9%) | |
| Parameters | Cutoff value | AUC (95% CI) | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) |
|---|---|---|---|---|---|---|
| Axillary lymph node parameters | ||||||
| Visual analysis | - | 0.739 (0.689–0.785) | 53.8 | 93.7 | 83.1 | 77.9 |
| Maximum SUV of the axillary lymph node 1 | 1.58 | 0.793 (0.741–0.839) | 56.9 | 91.4 | 82.5 | 74.7 |
| Peritumoral breast adipose tissue textural parameters | ||||||
| GLCM entropy | 3.16 | 0.830 (0.784–0.869) | 82.4 | 74.4 | 64.9 | 88.0 |
| SUV histogram entropy | 1.90 | 0.815 (0.768–0.855) | 84.0 | 70.5 | 62.1 | 88.5 |
| GLCM contrast | 0.63 | 0.780 (0.731–0.823) | 84.0 | 64.3 | 57.5 | 87.5 |
| GLZLM zone-length nonuniformity | 7.27 | 0.766 (0.716–0.811) | 58.8 | 83.1 | 66.7 | 77.8 |
| GLZLM high grey-level zone emphasis | 21.31 | 0.765 (0.715–0.810) | 67.2 | 74.9 | 60.6 | 79.9 |
| GLRLM high grey-level run emphasis | 9.41 | 0.763 (0.713–0.808) | 75.6 | 66.7 | 56.6 | 82.6 |
| GLRLM short-run high grey-level emphasis | 7.25 | 0.761 (0.711–0.806) | 79.8 | 62.8 | 55.2 | 84.4 |
| Visual Analysis | Maximum SUV of the Axillary Lymph Node 1 | ||||
|---|---|---|---|---|---|
| Negative | Positive | ≤1.58 | >1.58 | ||
| GLCM entropy | ≤3.16 | 15/158 (9.5%) | 6/16 (37.5%) | 13/122 (10.7%) | 6/17 (35.3%) |
| >3.16 | 40/91 (44.0%) | 58/61 (95.1%) | 37/76 (48.7%) | 60/63 (95.2%) | |
| SUV histogram entropy | ≤1.90 | 16/152 (10.5%) | 3/12 (25.0%) | 14/118 (11.9%) | 3/14 (21.4%) |
| >1.90 | 39/97 (40.2%) | 61/65 (93.8%) | 36/80 (45.0%) | 63/66 (95.5%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.W.; Kim, S.Y.; Han, S.W.; Lee, J.E.; Hong, S.H.; Lee, S.M.; Jo, I.Y. Clinical Significance of Peritumoral Adipose Tissue PET/CT Imaging Features for Predicting Axillary Lymph Node Metastasis in Patients with Breast Cancer. J. Pers. Med. 2021, 11, 1029. https://doi.org/10.3390/jpm11101029
Lee JW, Kim SY, Han SW, Lee JE, Hong SH, Lee SM, Jo IY. Clinical Significance of Peritumoral Adipose Tissue PET/CT Imaging Features for Predicting Axillary Lymph Node Metastasis in Patients with Breast Cancer. Journal of Personalized Medicine. 2021; 11(10):1029. https://doi.org/10.3390/jpm11101029
Chicago/Turabian StyleLee, Jeong Won, Sung Yong Kim, Sun Wook Han, Jong Eun Lee, Sung Hoon Hong, Sang Mi Lee, and In Young Jo. 2021. "Clinical Significance of Peritumoral Adipose Tissue PET/CT Imaging Features for Predicting Axillary Lymph Node Metastasis in Patients with Breast Cancer" Journal of Personalized Medicine 11, no. 10: 1029. https://doi.org/10.3390/jpm11101029