
The Clinical Contribution of Full-Field Electroretinography and 8-Year Experiences of Application in a Tertiary Medical Center

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. ffERG Recording
2.2. ffERG Data Interpretation
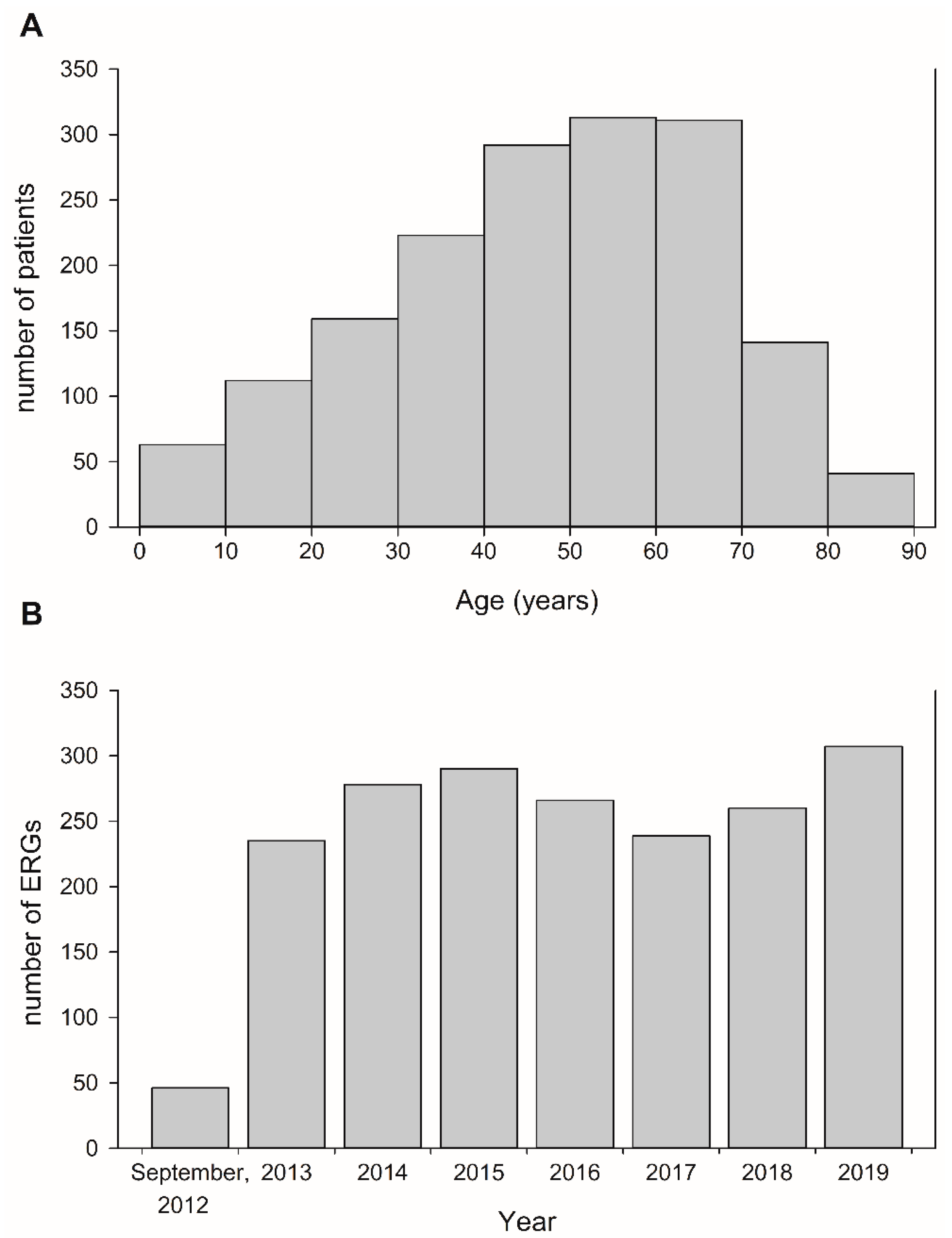
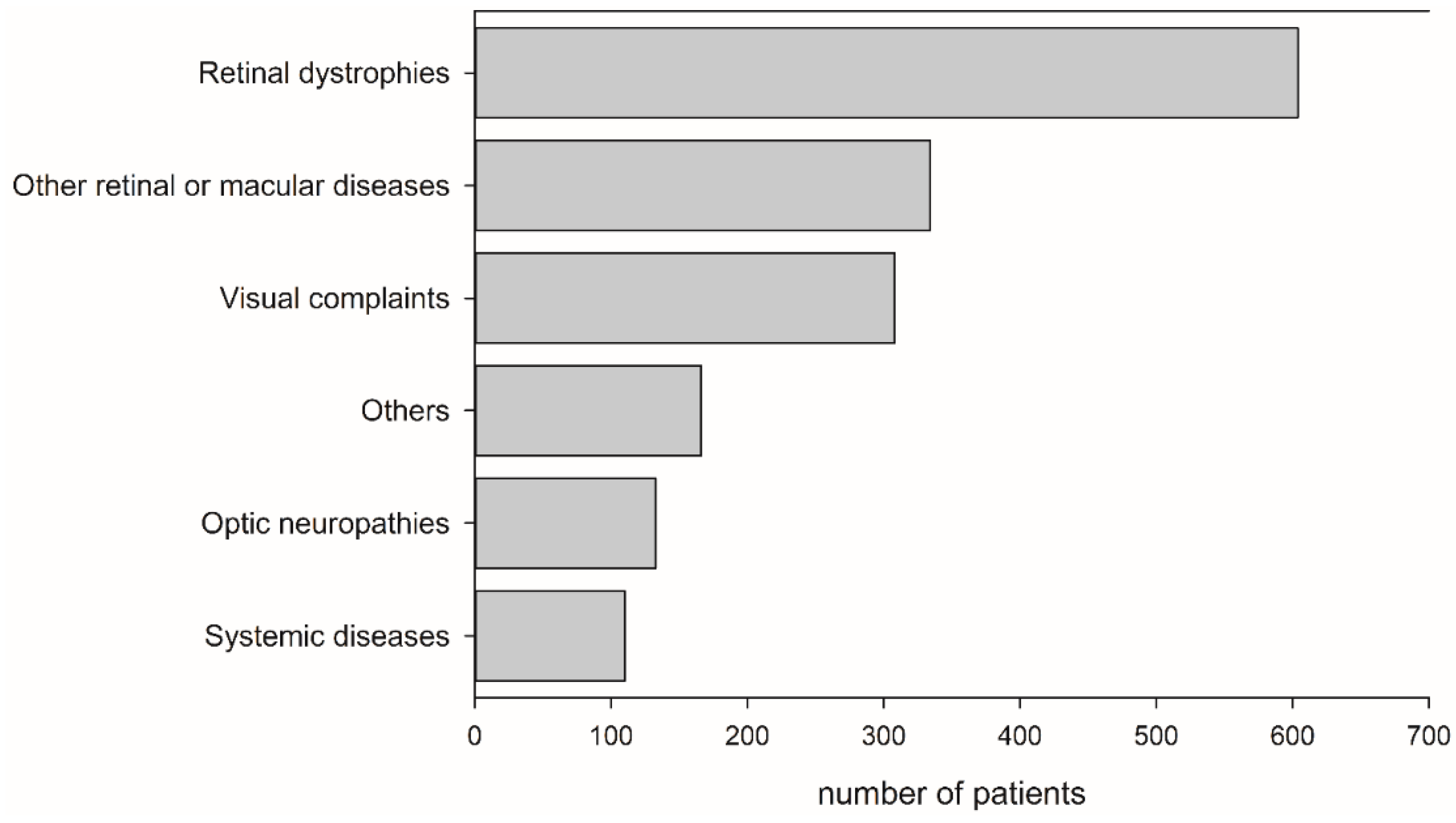
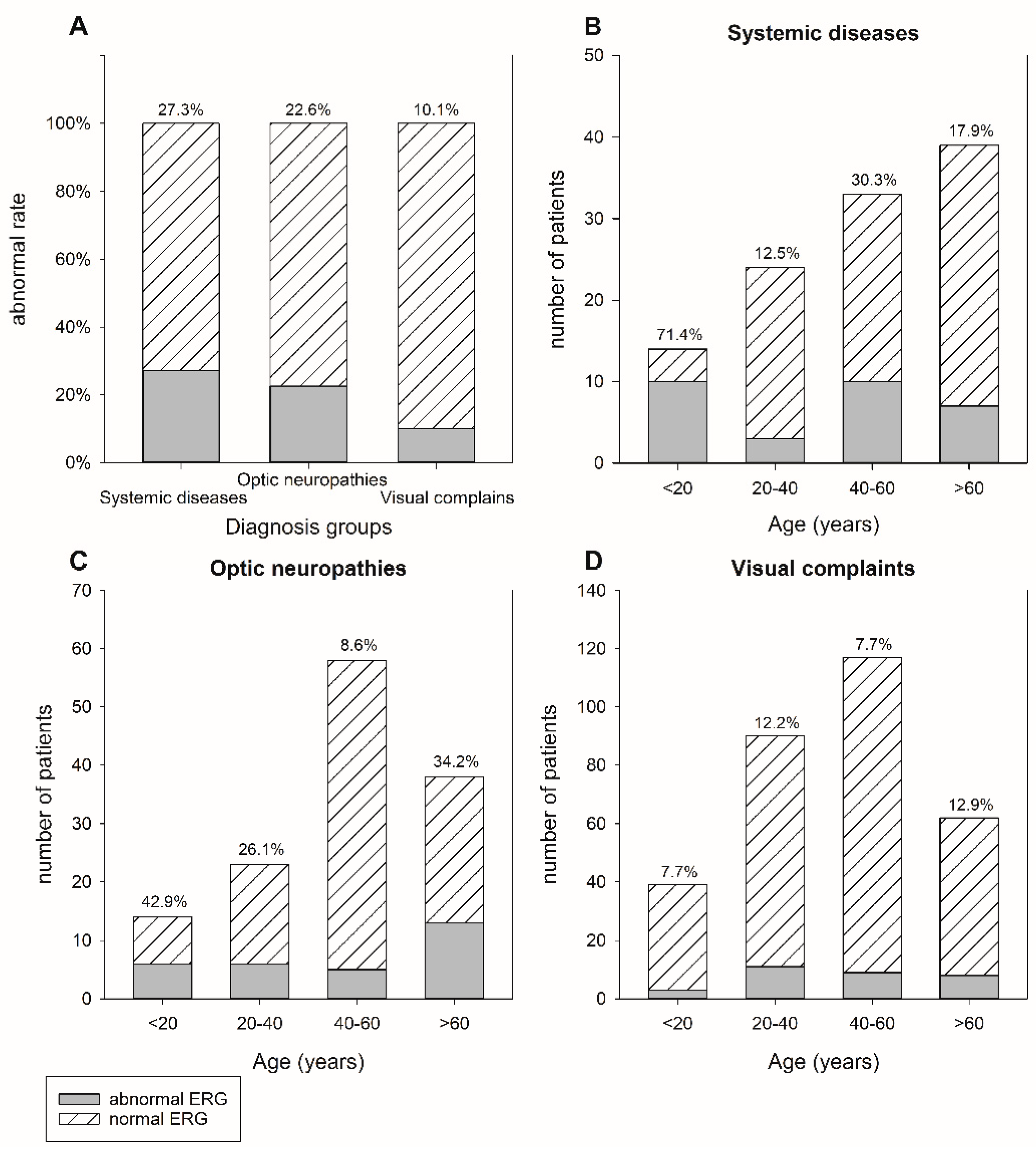
3. Results
4. Discussion
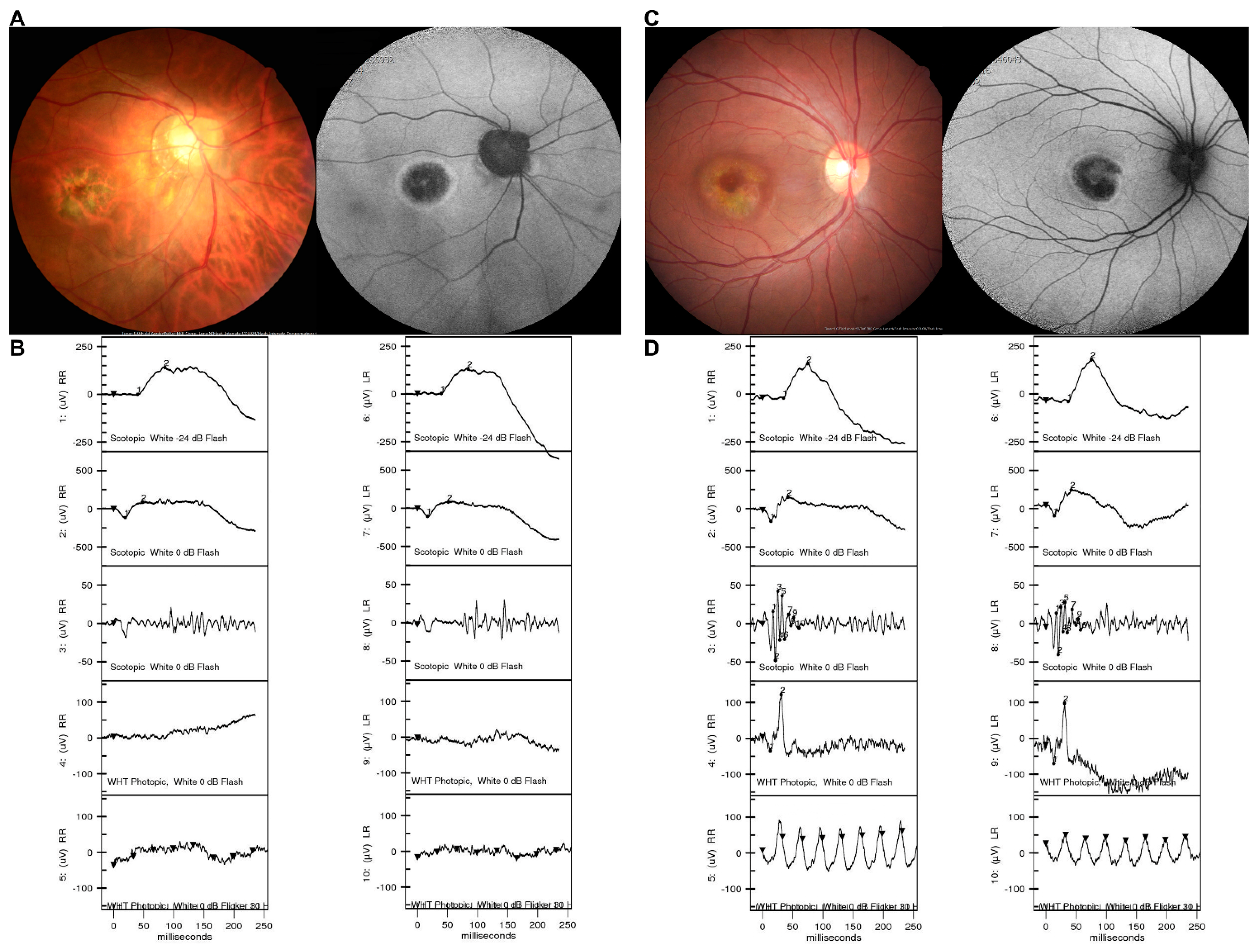
4.1. Evaluating Retinal Function and Confirming the Diagnosis
4.2. Identifying Further Diagnostic Clues
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kremers, J. The Assessment of L- and M-Cone Specific Electroretinographical Signals in the Normal and Abnormal Human Retina. Prog. Retin. Eye Res. 2003, 22, 579–605. [Google Scholar] [CrossRef]
- Hood, D.C. Assessing Retinal Function with the Multifocal Technique. Prog. Retin. Eye Res. 2000, 19, 607–646. [Google Scholar] [CrossRef]
- Hidajat, R.R.; Goode, D.H. The Clinical Value of Ophthalmic Electrodiagnosis in Children. Australas. Phys. Eng. Sci. Med. 2001, 24, 172–176. [Google Scholar] [CrossRef] [PubMed]
- Hood, D.C.; Birch, D.G. Beta Wave of the Scotopic (Rod) Electroretinogram as a Measure of the Activity of Human on-Bipolar Cells. J. Opt. Soc. Am. A Opt. Image Sci. Vis. 1996, 13, 623–633. [Google Scholar] [CrossRef] [PubMed]
- Hood, D.C.; Birch, D.G. Assessing Abnormal Rod Photoreceptor Activity with the a-Wave of the Electroretinogram: Applications and Methods. Doc. Ophthalmol. 1996, 92, 253–267. [Google Scholar] [CrossRef] [PubMed]
- Holder, G.E. Pattern Electroretinography (Perg) and an Integrated Approach to Visual Pathway Diagnosis. Prog. Retin. Eye Res. 2001, 20, 531–561. [Google Scholar] [CrossRef]
- Hood, D.C.; Seiple, W.; Holopigian, K.; Greenstein, V. A Comparison of the Components of the Multifocal and Full-Field Ergs. Vis. Neurosci. 1997, 14, 533–544. [Google Scholar] [CrossRef]
- Abràmoff, M.D.; Garvin, M.K.; Sonka, M. Retinal Imaging and Image Analysis. IEEE Rev. Biomed. Eng. 2010, 3, 169–208. [Google Scholar] [CrossRef] [Green Version]
- Spaide, R.F.; Fujimoto, J.G.; Waheed, N.K.; Sadda, S.R.; Staurenghi, G. Optical Coherence Tomography Angiography. Prog. Retin. Eye Res. 2018, 64, 1–55. [Google Scholar] [CrossRef]
- Yannuzzi, L.A.; Ober, M.D.; Slakter, J.S.; Spaide, R.F.; Fisher, Y.L.; Flower, R.W.; Rosen, R. Ophthalmic Fundus Imaging: Today and Beyond. Am. J. Ophthalmol. 2004, 137, 511–524. [Google Scholar] [CrossRef]
- Marmor, M.F.; Fulton, A.B.; Holder, G.E.; Miyake, Y.; Brigell, M.; Bach, M. Iscev Standard for Full-Field Clinical Electroretinography (2008 Update). Doc. Ophthalmol. 2009, 118, 69–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCulloch, D.L.; Marmor, M.F.; Brigell, M.G.; Hamilton, R.; Holder, G.E.; Tzekov, R.; Bach, M. Iscev Standard for Full-Field Clinical Electroretinography (2015 Update). Doc. Ophthalmol. 2015, 130, 1–12. [Google Scholar] [CrossRef]
- Rustum, K.; Hove, M.; Coupland, S. Electroretinograms and Normative Data. In Electroretinograms; Belusic, G., Ed.; IntechOpen: London, UK, 2011. [Google Scholar]
- Liu, H.; Ji, X.; Dhaliwal, S.; Rahman, S.N.; McFarlane, M.; Tumber, A.; Locke, J.; Wright, T.; Vincent, A.; Westall, C. Evaluation of Light- and Dark-Adapted Ergs Using a Mydriasis-Free, Portable System: Clinical Classifications and Normative Data. Doc. Ophthalmol. 2018, 137, 169–181. [Google Scholar] [CrossRef] [PubMed]
- Cordell, W.H.; Maturi, R.K.; Costigan, T.M.; Marmor, M.F.; Weleber, R.G.; Coupland, S.G.; Danis, R.P.; McGettigan, J.W., Jr.; Antoszyk, A.N.; Klise, S.; et al. Retinal Effects of 6 Months of Daily Use of Tadalafil or Sildenafil. Arch. Ophthalmol. 2009, 127, 367–373. [Google Scholar] [CrossRef]
- Davoudi, S.; Ebrahimiadib, N.; Yasa, C.; Sevgi, D.D.; Roohipoor, R.; Papavasilieou, E.; Comander, J.; Sobrin, L. Outcomes in Autoimmune Retinopathy Patients Treated with Rituximab. Am. J. Ophthalmol. 2017, 180, 124–132. [Google Scholar] [CrossRef]
- Camuglia, J.E.; Greer, R.M.; Welch, L.; Gole, G.A. Use of the Electroretinogram in a Paediatric Hospital. Clin. Exp. Ophthalmol. 2011, 39, 506–512. [Google Scholar] [CrossRef]
- Domínguez-Serrano, F.B.; Jiménez-López, E.; Jiménez, M.R.; Ponte-Zuñiga, B.; Gómez-Escobar, A.; Díaz-Granda, M.J.; Gutiérrez-Sánchez, E.; Morillo-Sánchez, M.J.; Menéndez-de-León, C.; Rodríguez-de-la-Rúa-Franch, E. Importance of Ocular Electrophysiology in the Diagnosis of Retinal Dystrophies. Arch. Soc. Esp. Oftalmol. (Engl. Ed.) 2019, 94, 160–164. [Google Scholar] [CrossRef]
- Whatham, A.R.; Nguyen, V.; Zhu, Y.; Hennessy, M.; Kalloniatis, M. The Value of Clinical Electrophysiology in the Assessment of the Eye and Visual System in the Era of Advanced Imaging. Clin. Exp. Optom. 2014, 97, 99–115. [Google Scholar] [CrossRef]
- Young, B.; Eggenberger, E.; Kaufman, D. Current Electrophysiology in Ophthalmology: A Review. Curr. Opin. Ophthalmol. 2012, 23, 497–505. [Google Scholar] [CrossRef]
- Birch, D.G. Surrogate Electroretinographic Markers for Assessing Therapeutic Efficacy in the Retina. Expert Rev. Mol. Diagn. 2004, 4, 693–703. [Google Scholar] [CrossRef] [PubMed]
- Zahid, S.; Jayasundera, T.; Rhoades, W.; Branham, K.; Khan, N.; Niziol, L.M.; Musch, D.C.; Heckenlively, J.R. Clinical Phenotypes and Prognostic Full-Field Electroretinographic Findings in Stargardt Disease. Am. J. Ophthalmol. 2013, 155, 465–473. [Google Scholar] [CrossRef] [Green Version]
- Langwińska-Wośko, E.; Szulborski, K.; Zaleska-Żmijewska, A.; Szaflik, J. Electrophysiological Testing as a Method of Cone-Rod and Cone Dystrophy Diagnoses and Prediction of Disease Progression. Doc. Ophthalmol. 2015, 130, 103–109. [Google Scholar] [CrossRef]
- Tan, A.C.; Chen, L.; Png, R.; Chia, A. The Diagnosis and Assessment of Visual Function in Singaporean Children with Electrophysiology: 10-Year Results. Doc. Ophthalmol. 2016, 132, 189–199. [Google Scholar] [CrossRef]
- Pescosolido, N.; Barbato, A.; Stefanucci, A.; Buomprisco, G. Role of Electrophysiology in the Early Diagnosis and Follow-up of Diabetic Retinopathy. J. Diabetes Res. 2015, 2015, 319692. [Google Scholar] [CrossRef] [PubMed]
- Mead, B.; Tomarev, S. Evaluating Retinal Ganglion Cell Loss and Dysfunction. Exp. Eye Res. 2016, 151, 96–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weiner, A.; Ripkin, D.J.; Patel, S.; Kaufman, S.R.; Kohn, H.D.; Weidenthal, D.T. Foveal Dysfunction and Central Visual Field Loss in Glaucoma. Arch. Ophthalmol. 1998, 116, 1169–1174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niyadurupola, N.; Luu, C.D.; Nguyen, D.Q.; Geddes, K.; Tan, G.X.; Wong, C.C.; Tran, T.; Coote, M.A.; Crowston, J.G. Intraocular Pressure Lowering Is Associated with an Increase in the Photopic Negative Response (Phnr) Amplitude in Glaucoma and Ocular Hypertensive Eyes. Investig. Ophthalmol. Vis. Sci. 2013, 54, 1913–1919. [Google Scholar] [CrossRef] [Green Version]
- Kirkiewicz, M.; Lubiński, W.; Penkala, K. Photopic Negative Response of Full-Field Electroretinography in Patients with Different Stages of Glaucomatous Optic Neuropathy. Doc. Ophthalmol. 2016, 132, 57–65. [Google Scholar] [CrossRef] [Green Version]
- Kumar, V. Understanding Retinal Changes after Stroke. Open J. Ophthalmol. 2017, 7, 281–292. [Google Scholar] [CrossRef] [Green Version]
- Grönlund, M.A.; Honarvar, A.K.; Andersson, S.; Moslemi, A.R.; Oldfors, A.; Holme, E.; Tulinius, M.; Darin, N. Ophthalmological Findings in Children and Young Adults with Genetically Verified Mitochondrial Disease. Br. J. Ophthalmol. 2010, 94, 121–127. [Google Scholar] [CrossRef]
- Parisi, V.; Pierelli, F.; Fattapposta, F.; Bianco, F.; Parisi, L.; Restuccia, R.; Malandrini, A.; Ferrari, M.; Carrera, P. Early Visual Function Impairment in Cadasil. Neurology 2003, 60, 2008–2010. [Google Scholar] [CrossRef] [PubMed]
- Katagiri, S.; Nishina, S.; Yokoi, T.; Mikami, M.; Nakayama, Y.; Tanaka, M.; Azuma, N. Retinal Structure and Function in Eyes with Optic Nerve Hypoplasia. Sci. Rep. 2017, 7, 42480. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | Age (Years) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| <10 | 10–20 | 20–30 | 30–40 | 40–50 | 50–60 | 60–70 | 70–80 | >80 | ||
| Diagnosis Group | n (% of Group) | n | n | n | n | n | n | n | n | n |
| Retinal dystrophies | ||||||||||
| Retinitis pigmentosa | 367 (60.8) | 5 | 25 | 38 | 69 | 74 | 71 | 60 | 21 | 4 |
| Macular dystrophy | 85 (14.1) | 3 | 13 | 11 | 12 | 17 | 12 | 12 | 4 | 1 |
| Cone–rod dystrophy | 30 (5.0) | 1 | 4 | 2 | 9 | 4 | 4 | 5 | 1 | 0 |
| Leber’s congenital amaurosis | 29 (4.8) | 18 | 6 | 1 | 2 | 1 | 0 | 1 | 0 | 0 |
| Bietti crystalline dystrophy | 16 (2.6) | 0 | 0 | 0 | 4 | 7 | 4 | 1 | 0 | 0 |
| PPVRCA | 13 (2.2) | 0 | 1 | 1 | 1 | 2 | 3 | 4 | 1 | 0 |
| Family history | 9 (1.5) | 0 | 1 | 2 | 2 | 3 | 1 | 0 | 0 | 0 |
| Cone dystrophy | 8 (1.3) | 4 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 0 |
| Occult macular dystrophy | 8 (1.3) | 0 | 2 | 1 | 2 | 1 | 2 | 0 | 0 | 0 |
| Achromatopsia | 7 (1.2) | 0 | 2 | 2 | 0 | 1 | 1 | 0 | 1 | 0 |
| Choroideremia | 5 (0.8) | 0 | 0 | 2 | 1 | 0 | 1 | 0 | 1 | 0 |
| AZOOR | 4 (0.7) | 0 | 0 | 2 | 1 | 1 | 0 | 0 | 0 | 0 |
| Retinoschisis | 4 (0.7) | 1 | 2 | 1 | 0 | 0 | 0 | 0 | 0 | 0 |
| CSNB | 3 (0.5) | 0 | 1 | 2 | 0 | 0 | 0 | 0 | 0 | 0 |
| Albinism | 2 (0.3) | 0 | 0 | 2 | 0 | 0 | 0 | 0 | 0 | 0 |
| Carrier | 2 (0.3) | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 |
| Other dystrophies | 12 (2.0) | 2 | 0 | 2 | 2 | 2 | 0 | 2 | 2 | 0 |
| Other retinal or macular diseases | ||||||||||
| AMD | 82 (24.6) | 0 | 0 | 0 | 2 | 2 | 20 | 28 | 21 | 9 |
| Vitreomacular disorders | 70 (21.0) | 2 | 5 | 0 | 9 | 10 | 18 | 18 | 6 | 2 |
| Cancer-related | 57 (17.1) | 0 | 0 | 0 | 4 | 14 | 9 | 17 | 9 | 4 |
| Inflammatory disease | 32 (9.6) | 0 | 0 | 4 | 13 | 6 | 5 | 4 | 0 | 0 |
| Myopic degeneration | 30 (9.0) | 1 | 3 | 2 | 5 | 8 | 5 | 2 | 4 | 0 |
| Post-RD operation | 25 (7.5) | 0 | 1 | 1 | 2 | 4 | 9 | 7 | 1 | 0 |
| Diabetic retinopathy | 16 (4.8) | 0 | 0 | 1 | 1 | 1 | 4 | 4 | 5 | 0 |
| Vascular disease | 15 (4.5) | 0 | 0 | 0 | 1 | 1 | 4 | 7 | 2 | 0 |
| Uncertain retinopathy | 7 (2.1) | 0 | 0 | 0 | 1 | 1 | 3 | 2 | 0 | 0 |
| Optic neuropathies | ||||||||||
| Optic neuropathy | 133 (100) | 4 | 10 | 11 | 12 | 30 | 28 | 14 | 16 | 8 |
| Systemic diseases | ||||||||||
| Neurological disease | 98 (89.1) | 5 | 7 | 10 | 11 | 16 | 14 | 19 | 12 | 4 |
| Autoimmune disease | 3 (2.7) | 0 | 0 | 1 | 0 | 1 | 0 | 1 | 0 | 0 |
| Metabolic disease | 3 (2.7) | 0 | 0 | 1 | 1 | 0 | 0 | 1 | 0 | 0 |
| Endocrine disease | 2 (1.8) | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 |
| Mitochondrial disease | 2 (1.8) | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 0 |
| Psuedoxanthoma elasticum | 1 (0.9) | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 |
| Hematology disease | 1 (0.9) | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 |
| Visual complaints | ||||||||||
| Non-specific visual disturbances | 249 (80.8) | 7 | 16 | 31 | 36 | 51 | 53 | 43 | 10 | 2 |
| Suspected night blindness | 27 (8.8) | 0 | 1 | 7 | 6 | 5 | 5 | 2 | 1 | 0 |
| Suspected retina origin amblyopia | 22 (7.1) | 8 | 4 | 5 | 0 | 0 | 2 | 3 | 0 | 0 |
| Malinger tendency | 10 (3.2) | 1 | 2 | 4 | 1 | 0 | 1 | 1 | 0 | 0 |
| Others | ||||||||||
| Clinical study | 79 (47.6) | 0 | 0 | 1 | 3 | 10 | 17 | 31 | 14 | 3 |
| Drug-associated | 67 (40.4) | 0 | 3 | 9 | 6 | 12 | 15 | 13 | 7 | 2 |
| Trauma | 14 (8.4) | 0 | 1 | 1 | 2 | 2 | 0 | 7 | 0 | 1 |
| Pre-cornea transplantation evaluation | 6 (3.6) | 0 | 0 | 0 | 0 | 2 | 1 | 1 | 1 | 1 |
| Total ERG | 1655 | 63 | 112 | 159 | 223 | 292 | 313 | 311 | 141 | 41 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, J.-J.; Huang, C.-H.; Yang, C.-H.; Yang, C.-M.; Lin, C.-W.; Ho, T.-C.; Lin, C.-P.; Hsieh, Y.-T.; Yeh, P.-T.; Lai, T.-T.; et al. The Clinical Contribution of Full-Field Electroretinography and 8-Year Experiences of Application in a Tertiary Medical Center. J. Pers. Med. 2021, 11, 1022. https://doi.org/10.3390/jpm11101022
Yang J-J, Huang C-H, Yang C-H, Yang C-M, Lin C-W, Ho T-C, Lin C-P, Hsieh Y-T, Yeh P-T, Lai T-T, et al. The Clinical Contribution of Full-Field Electroretinography and 8-Year Experiences of Application in a Tertiary Medical Center. Journal of Personalized Medicine. 2021; 11(10):1022. https://doi.org/10.3390/jpm11101022
Chicago/Turabian StyleYang, Jung-Je, Chu-Hsuan Huang, Chang-Hao Yang, Chung-May Yang, Chao-Wen Lin, Tzyy-Chang Ho, Chang-Ping Lin, Yi-Ting Hsieh, Po-Ting Yeh, Tso-Ting Lai, and et al. 2021. "The Clinical Contribution of Full-Field Electroretinography and 8-Year Experiences of Application in a Tertiary Medical Center" Journal of Personalized Medicine 11, no. 10: 1022. https://doi.org/10.3390/jpm11101022