Is Structured Exercise Performed with Supplemental Oxygen a Promising Method of Personalized Medicine in the Therapy of Chronic Diseases?

 , ,
, ,
Abstract
:1. Introduction
2. Methods
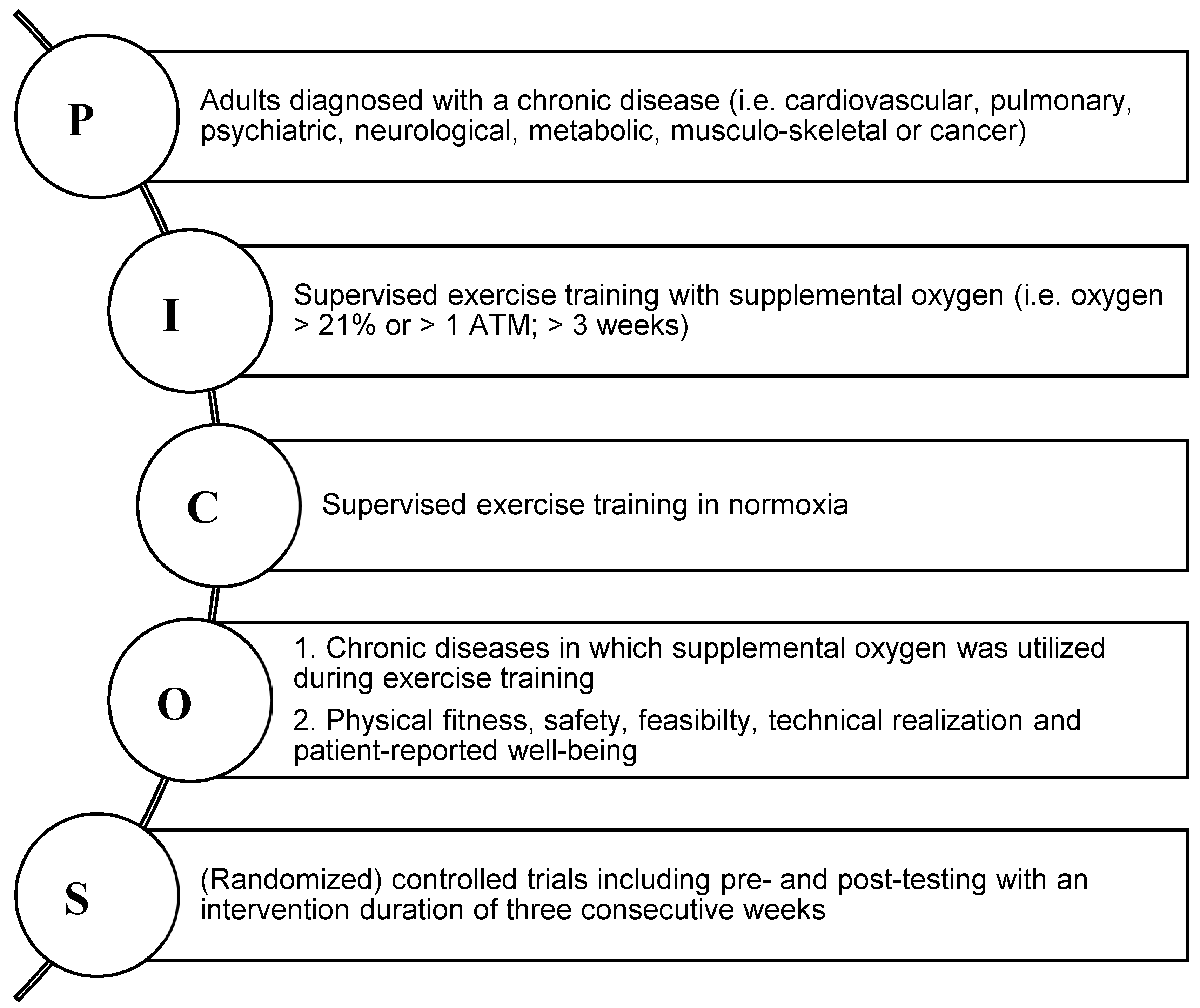
2.1. Eligibility Criteria
2.2. Data Extraction
2.3. Data Synthesis and Analysis
2.4. Assessment of Methodological Quality
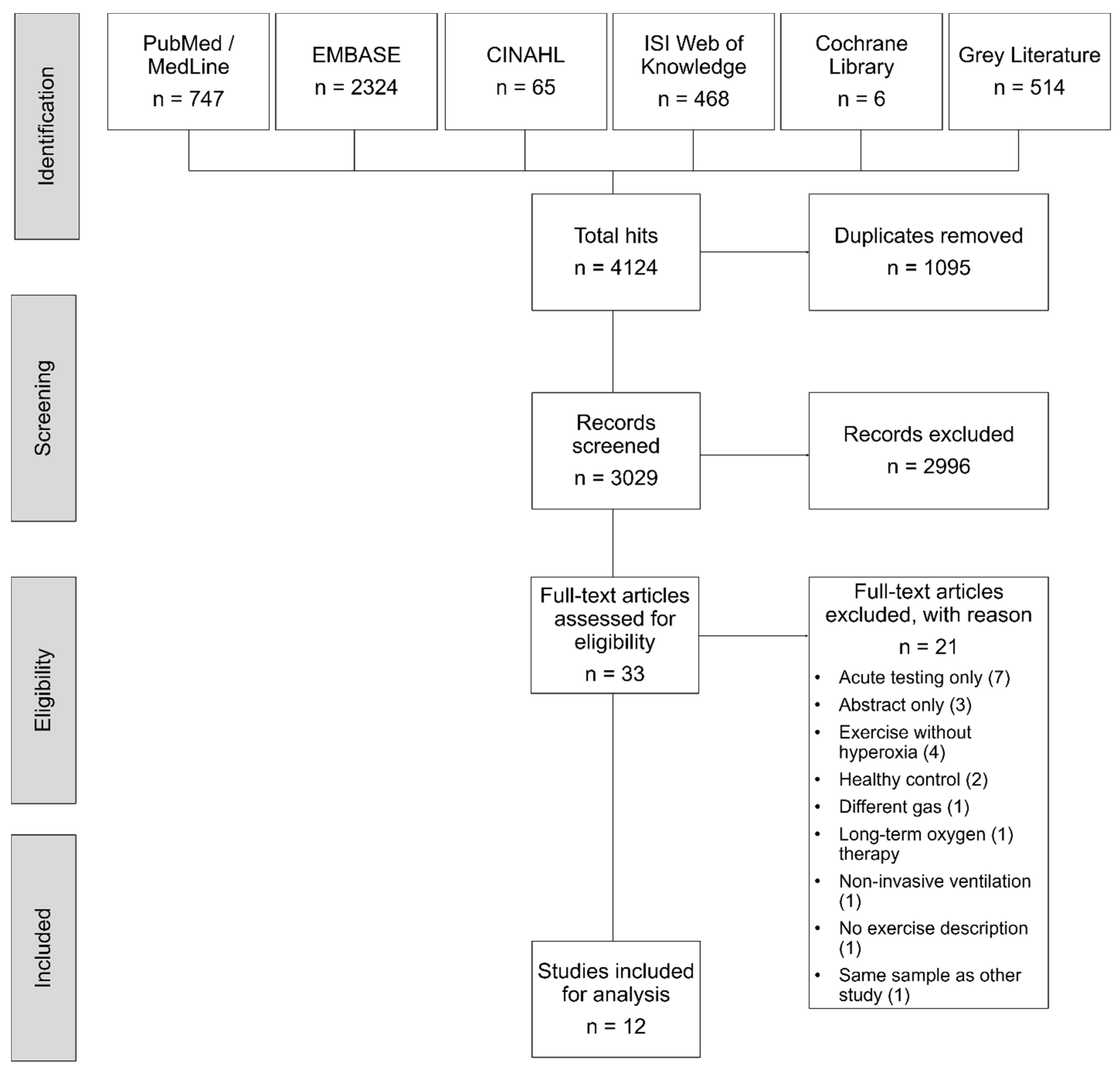
3. Results
3.1. Study and Intervention Characteristics
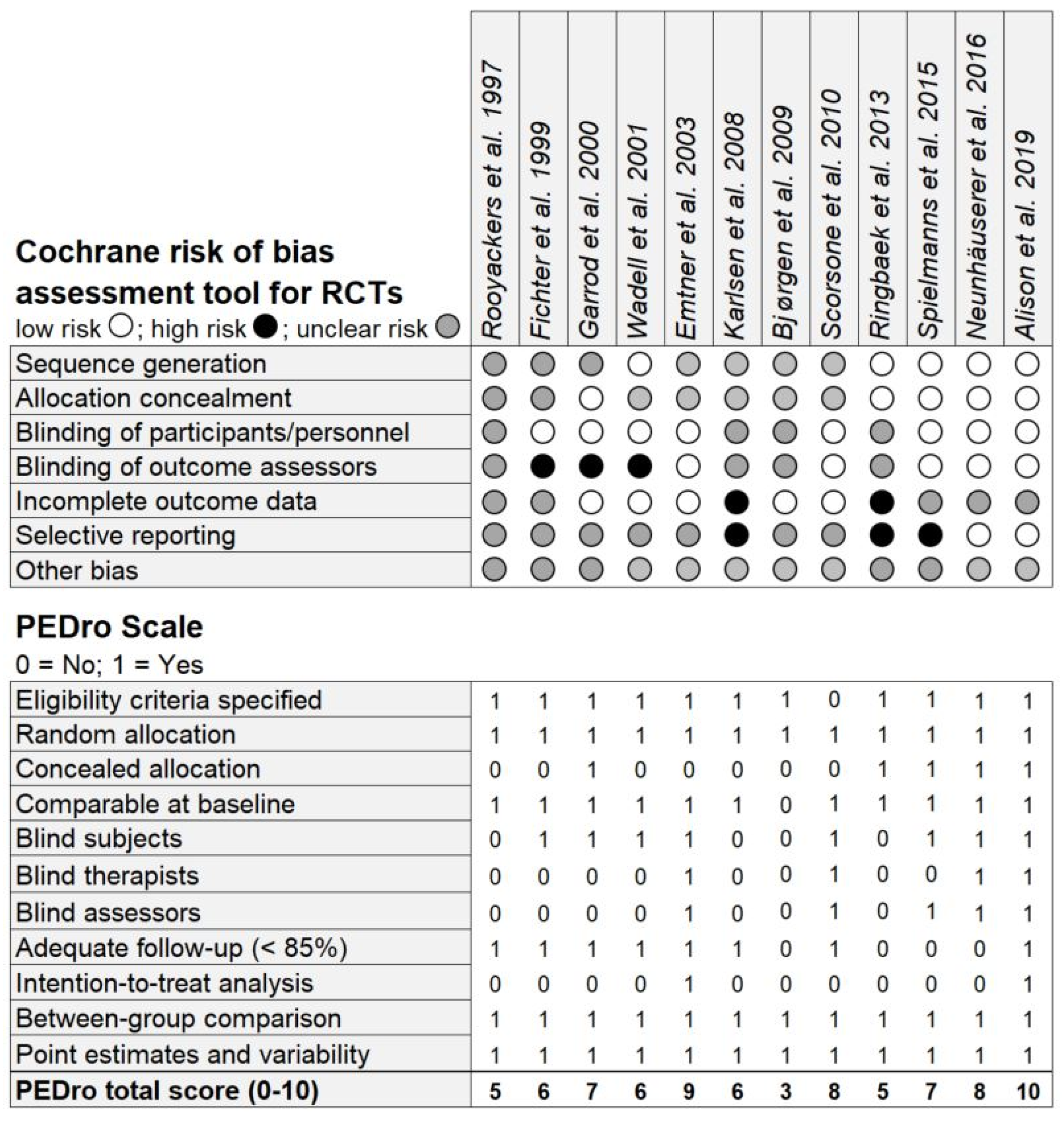
3.2. Risk of Bias Assessment and PEDro Scale Ratings
3.3. Feasibility and Safety
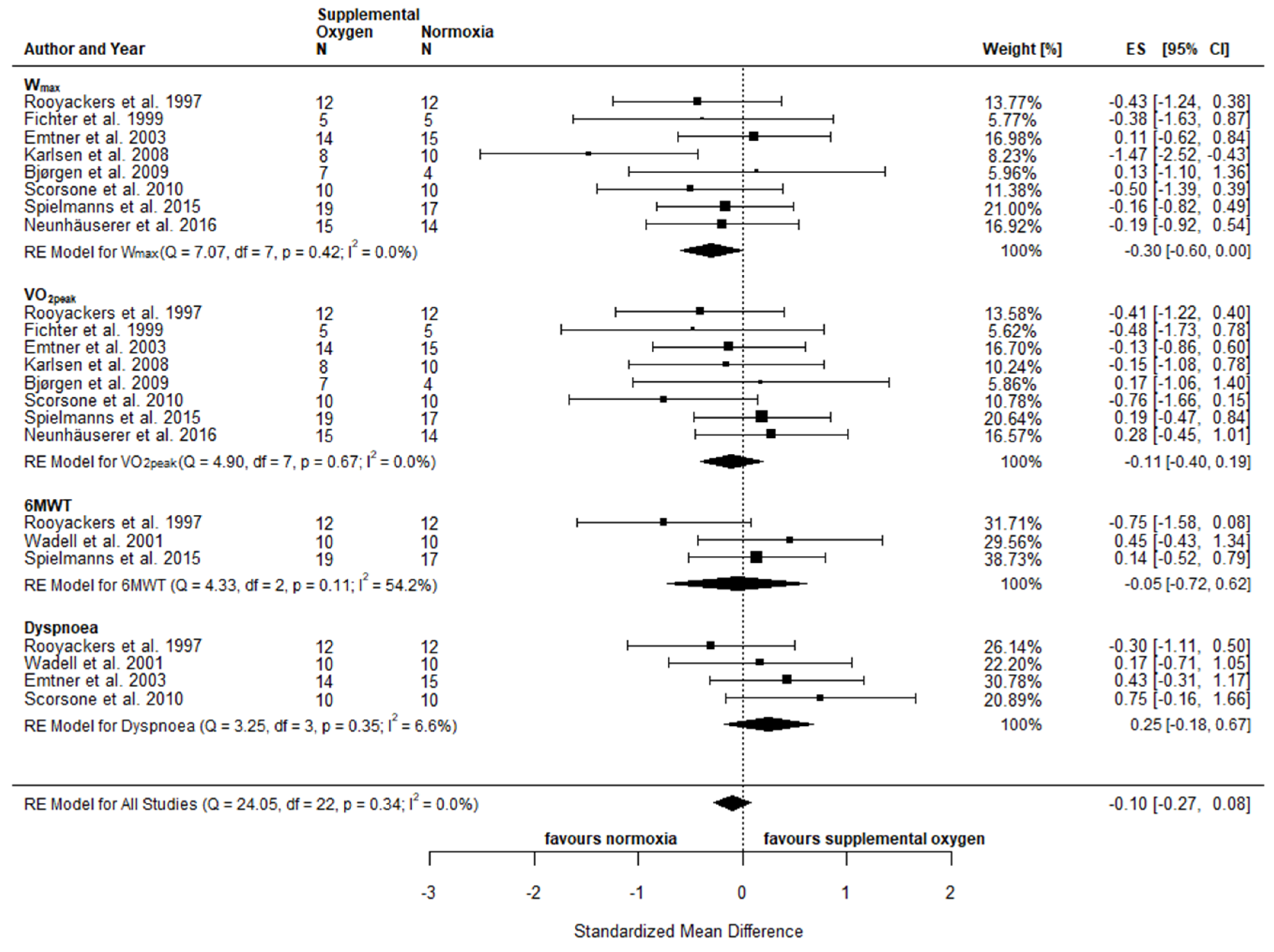
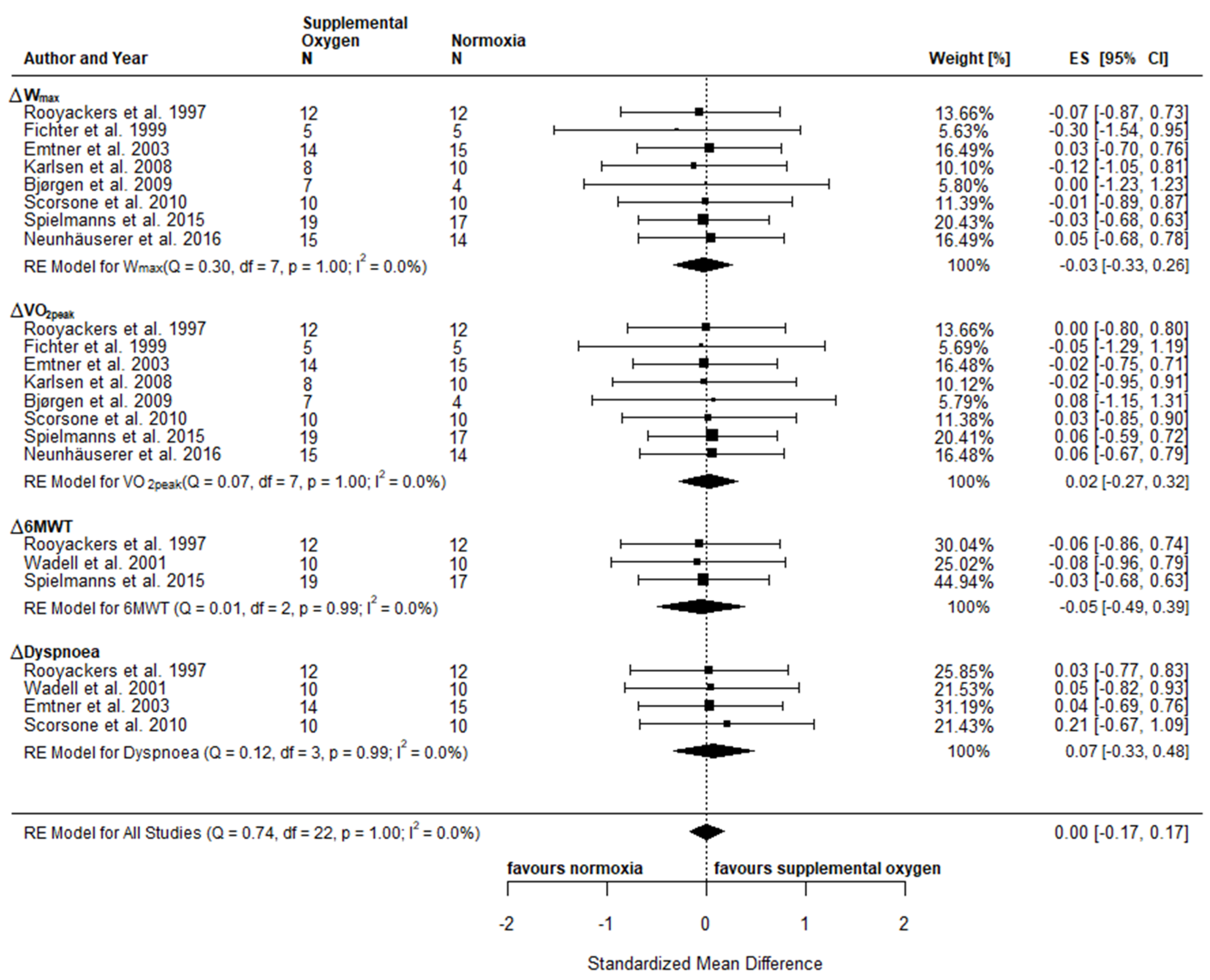
3.4. Intervention Effects and Pooled Analysis
3.4.1. Physical Fitness and Functional Capacity
3.4.2. Patient-Reported Well-Being
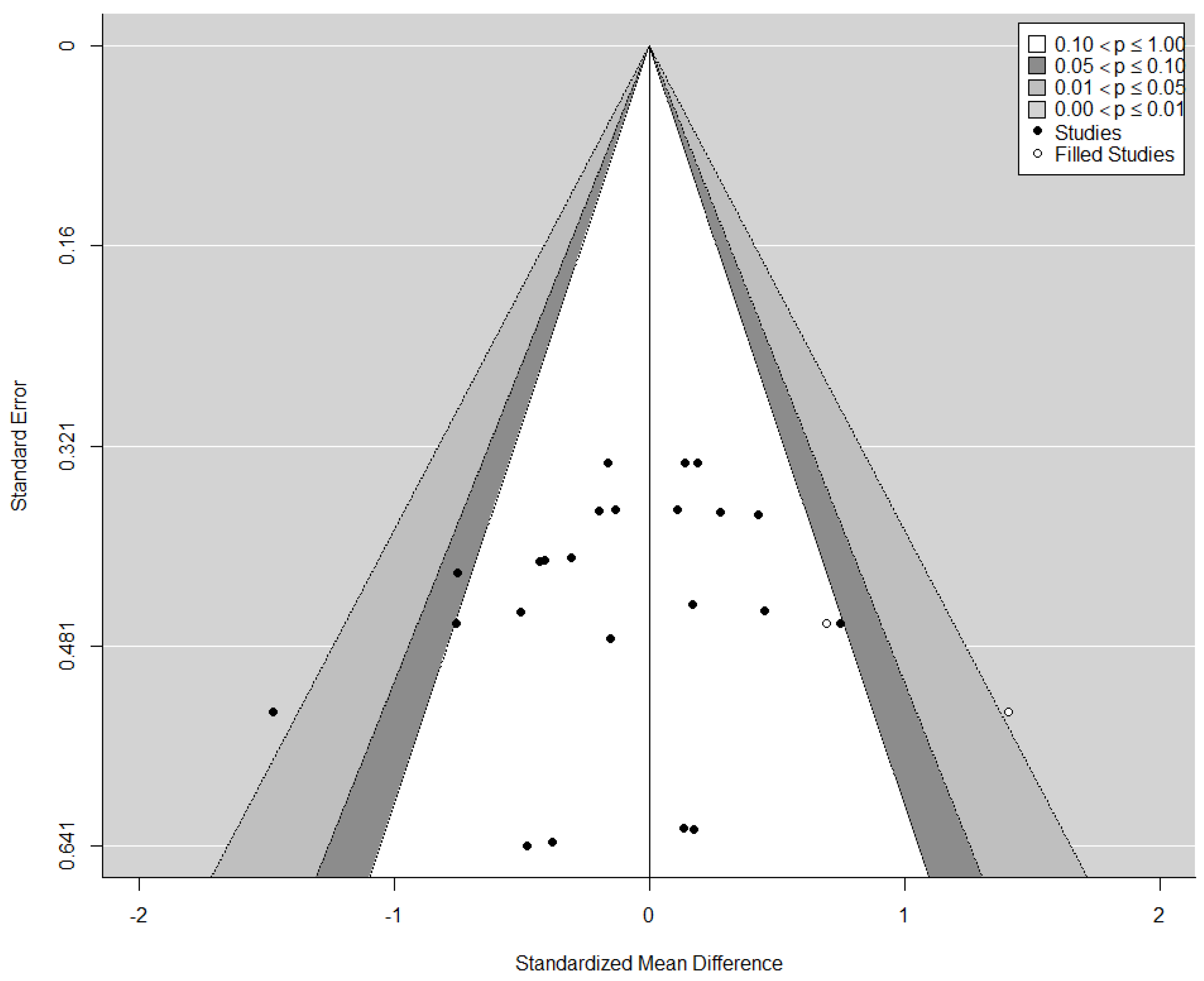
3.4.3. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gore, A.; Muralidhar, M.; Espey, M.G.; Degenhardt, K.; Mantell, L.L. Hyperoxia sensing: From molecular mechanisms to significance in disease. J. Immunotoxicol. 2010, 7, 239–254. [Google Scholar] [CrossRef] [PubMed]
- Grensemann, J.; Fuhrmann, V.; Kluge, S. Oxygen Treatment in Intensive Care and Emergency Medicine. Dtsch. Arztebl. Int. 2018, 115, 455–462. [Google Scholar] [CrossRef] [PubMed]
- Corsonello, A.; Pedone, C.; Scarlata, S.; Zito, A.; Laino, I.; Antonelli-Incalzi, R. The Oxygen Therapy. Curr. Med. Chem. 2013, 20, 1103–1126. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, B.K.; Saltin, B. Exercise as medicine—Evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand. J. Med. Sci. Sports. 2015, 25, 1–72. [Google Scholar] [CrossRef] [Green Version]
- Garvey, C.; Tiep, B.; Carter, R.; Barnett, M.; Hart, M.; Casaburi, R. Severe Exercise-Induced Hypoxemia. Respir. Care 2012, 57, 1154–1160. [Google Scholar] [CrossRef] [Green Version]
- Koerber, D.M.; Rosenbaum, A.N.; Olson, T.P.; Kushwaha, S.; Stulak, J.; Maltais, S.; Behfar, A. Exercise-induced hypoxemia predicts heart failure hospitalization and death in patients supported with left ventricular assist devices. Int. J. Artif. Organs. 2020, 43, 165–172. [Google Scholar] [CrossRef]
- Leermakers, P.A.; Gosker, H.R. Skeletal muscle mitophagy in chronic disease: Implications for muscle oxidative capacity. Curr. Opin. Clin. Nutr. Metab. Care 2016, 19, 427–433. [Google Scholar] [CrossRef] [Green Version]
- Varlotto, J.; Stevenson, M.A. Anemia, tumor hypoxemia, and the cancer patient. Int. J. Radiat. Oncol. Biol. Phys. 2005, 63, 25–36. [Google Scholar] [CrossRef]
- Wedzicha, J.A.; Bestall, J.C.; Garrod, R.; Garnham, R.; Paul, E.A.; Jones, P.W. Randomized controlled trial of pulmonary rehabilitation in severe chronic obstructive pulmonary disease patients, stratified with the MRC dyspnoea scale. Eur. Respir. J. 1998, 12, 363–369. [Google Scholar] [CrossRef]
- Heffner, J.E. The Story of Oxygen. Respir. Care 2013, 58, 18–31. [Google Scholar] [CrossRef] [Green Version]
- Mallette, M.M.; Stewart, D.G.; Cheung, S.S. The Effects of Hyperoxia on Sea-Level Exercise Performance, Training, and Recovery: A Meta-Analysis. Sport Med. 2018, 48, 153–175. [Google Scholar] [CrossRef] [PubMed]
- Cardinale, D.A.; Ekblom, B. Hyperoxia for performance and training. J. Sports Sci. 2018, 36, 1515–1522. [Google Scholar] [CrossRef] [PubMed]
- Sperlich, B.; Zinner, C.; Hauser, A.; Holmberg, H.C.; Wegrzyk, J. The Impact of Hyperoxia on Human Performance and Recovery. Sport Med. 2017, 47, 429–438. [Google Scholar] [CrossRef]
- Brugniaux, J.V.; Coombs, G.B.; Barak, O.F.; Dujic, Z.; Sekhon, M.S.; Ainslie, P.N. Highs and lows of hyperoxia: Physiological, performance, and clinical aspects. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2018, 315, R1–R27. [Google Scholar] [CrossRef] [PubMed]
- Elphick, H.E.; Mallory, G. Oxygen therapy for cystic fibrosis. Cochrane Database Syst. Rev. 2013, 7, CD003884. [Google Scholar] [CrossRef] [PubMed]
- Bradley, J.M.; Lasserson, T.; Elborn, S.; Macmahon, J.; O’neill, B. A Systematic Review of Randomized Controlled Trials Examining the Short-Term Benefit of Ambulatory Oxygen in COPD. Chest 2007, 131, 278–285. [Google Scholar] [CrossRef]
- Bell, E.C.; Cox, N.S.; Goh, N.; Glaspole, I.; Westall, G.P.; Watson, A.; Holland, A.E. Oxygen therapy for interstitial lung disease: A systematic review. Eur. Respir. Rev. 2017, 26, 160080. [Google Scholar] [CrossRef] [Green Version]
- Koshy, A.; Pellicori, P.; Clark, A.L. The effect of Increasing inspired oxygen on exercise performance in patients with chronic heart failure. Heart 2016, 102, 597–601. [Google Scholar] [CrossRef]
- Krop, H.D.; Block, A.J.; Cohen, E.; Croucher, R.; Shuster, J. Neuropsychologic Effects of Continuous Oxygen Therapy in the Aged. Chest 1977, 72, 737–743. [Google Scholar] [CrossRef]
- Nielsen, H.B.; Boushel, R.; Madsen, P.; Secher, N.H. Cerebral desaturation during exercise reversed by O2 supplementation. Am. J. Physiol. 1999, 277 (Pt 2), H1045–H1052. [Google Scholar] [CrossRef]
- Oussaidene, K.; Prieur, F.; Bougault, V.; Borel, B.; Matran, R.; Mucci, P. Cerebral oxygenation during hyperoxia-induced increase in exercise tolerance for untrained men. Eur. J. Appl. Physiol. 2013, 113, 2047–2056. [Google Scholar] [CrossRef] [PubMed]
- Tucker, R.; Kayser, B.; Rae, E.; Rauch, L.; Bosch, A.; Noakes, T. Hyperoxia improves 20 km cycling time trial performance by increasing muscle activation levels while perceived exertion stays the same. Eur. J. Appl. Physiol. 2007, 101, 771–781. [Google Scholar] [CrossRef] [PubMed]
- Goodrich, J.A.; Ryan, B.J.; Byrnes, W.C. The Influence of Oxygen Saturation on the Relationship Between Hemoglobin Mass and VO2max. Sport Med. Int. Open 2018, 2, E98–E104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harms, C.A.; McClaran, S.R.; Nickele, G.A.; Pegelow, D.F.; Nelson, W.B.; Dempsey, J.A. Effect of exercise-induced arterial O2 desaturation on VO2max in women. Med. Sci. Sports Exerc. 2000, 32, 1101–1108. [Google Scholar] [CrossRef] [Green Version]
- Somfay, A.; Porszasz, J.; Lee, S.M.; Casaburi, R. Dose-response effect of oxygen on hyperinflation and exercise endurance in nonhypoxaemic COPD patients. Eur. Respir. J. 2001, 18, 77–84. [Google Scholar] [CrossRef] [Green Version]
- Farber, H.W.; Badesch, D.B.; Benza, R.L.; Elliott, C.G.; Frantz, R.P.; McGoon, M.D.; Selej, M.; Zhao, C.; Frost, A.E. Use of supplemental oxygen in patients with pulmonary arterial hypertension in REVEAL. J. Hear. Lung Transplant. 2018, 37, 948–955. [Google Scholar] [CrossRef] [Green Version]
- Da Silva, A.L.G.; Karnopp, T.E.; Weber, A.F.; da Luz Goulart, C.; de Borba Scheneiders, P.; Cardoso, D.M.; Lisboa Carvalho, L.; Ellwanger, J.H.; Possuelo, L.G.; de Moura Valim, A.R. DNA damage and repair capacity in lymphocyte of chronic obstructive pulmonary diseases patients during physical exercise with oxygen supplementation. Multidiscip Respir. Med. 2016, 11, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Ameer, F.; Carson, K.V.; Usmani, Z.A.; Smith, B.J. Ambulatory oxygen for people with chronic obstructive pulmonary disease who are not hypoxaemic at rest. Cochrane Database Syst. Rev. 2014, 6. [Google Scholar] [CrossRef]
- Allen, P.D.; Pandolf, K.B. Perceived exertion associated with breathing hyperoxic mixtures during submaximal work. Med. Sci. Sports 1977, 9, 122–127. [Google Scholar] [CrossRef]
- Moore, D.P.; Weston, A.R.; Oakley, C.M.; Cleland, J.G.F.; Hughes, J.M.B. Effects of increased inspired oxygen concentrations on exercise performance in chronic heart failure. Lancet 1992, 339, 850–853. [Google Scholar] [CrossRef]
- Mach, W.J.; Thimmesch, A.R.; Pierce, J.T.; Pierce, J.D. Consequences of hyperoxia and the toxicity of oxygen in the lung. Nurs. Res. Pract. 2011, 2011, 260482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bitterman, H. Bench-to bedside. Crit. Care 2009, 13, 205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haque, W.A.; Boehmer, J.; Clemson, B.S.; Leuenberger, U.A.; Silber, D.H.; Sinoway, L.I. Hemodynamic effects of supplemental oxygen administration in congestive heart failure. J. Am. Coll. Cardiol. 1996, 27, 353–357. [Google Scholar] [CrossRef] [Green Version]
- Sperlich, B.; Calbet, J.A.L.; Boushel, R.; Holmberg, H.C. Is the use of hyperoxia in sports effective, safe and ethical? Scand. J. Med. Sci. Sport. 2016, 26, 1268–1272. [Google Scholar] [CrossRef] [PubMed]
- Astorino, T.; Robergs, R.A. Effect of hyperoxia on maximal oxygen uptake, blood acid-base balance, andlimitations to exercise tolerance. J. Exerc. Physiol. Online 2003, 6, 8–20. [Google Scholar]
- Welch, H.G. Hyperoxia and human performance: A brief review. Med. Sci. Sports Exerc. 1982, 14, 253–262. [Google Scholar] [CrossRef]
- Dilektasli, A.G.; Porszasz, J.; Stringer, W.W.; Casaburi, R. Physiologic Effects of Oxygen Supplementation During Exercise in Chronic Obstructive Pulmonary Disease. Clin. Chest Med. 2019, 40, 385–395. [Google Scholar] [CrossRef]
- Bradley, J.M.; O’Neill, B.M. Short-term ambulatory oxygen for chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2005, 4. [Google Scholar] [CrossRef]
- Nonoyama, M.L.; Brooks, D.; Lacasse, Y.; Guyatt, G.H.; Goldstein, R.S. Oxygen therapy during exercise training in chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2007, 2, CD005372. [Google Scholar] [CrossRef]
- Liu, Y.; Gong, F. Determination of whether supplemental oxygen therapy is beneficial during exercise training in patients with COPD: A systematic review and meta-analysis. Exp. Ther. Med. 2019, 18, 4081–4089. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The, P.R.I.SMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing. 2018. Available online: https://www.r-project.org/ (accessed on 17 October 2019).
- Team Rs. 2015. Available online: http://www.rstudio.com/ (accessed on 17 October 2019).
- Viechtbauer, W. Conducting Meta-Analyses in R with the metafor Package. J. Stat. Software 2010, 36, 1–48. [Google Scholar] [CrossRef] [Green Version]
- Viechtbauer, W. Bias and efficiency of meta-analytic variance estimators in the random-effects model. J. Educ. Behav. Stat. 2005, 30, 261–293. [Google Scholar] [CrossRef]
- Cochran, W.G. The Combination of Estimates from Different Experiments. Biometrics 1954, 10, 101. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Riley, R.D.; Higgins, J.P.T.; Deeks, J.J. Interpretation of random effects meta-analyses. BMJ 2011, 342, 964–967. [Google Scholar] [CrossRef] [Green Version]
- Viechtbauer, W.; Cheung, M.W.-L. Outlier and influence diagnostics for meta-analysis. Res. Synth. Methods 2010, 1, 112–125. [Google Scholar] [CrossRef]
- Duval, S.; Tweedie, R. A Nonparametric “Trim and Fill” Method of Accounting for Publication Bias in Meta-Analysis. J. Am. Stat. Assoc. 2000, 95, 89–98. [Google Scholar]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Rothstein, H.R.; Sutton, A.J.; Borenstein, M. Publication Bias in Meta-Analysis: Prevention, Assessment and Adjustments; Wiley: Hoboken, NJ, USA, 2006. [Google Scholar] [CrossRef]
- Begg, C.B.; Mazumdar, M. Operating Characteristics of a Rank Correlation Test for Publication Bias. Biometrics 1994, 50, 1088. [Google Scholar] [CrossRef]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verhagen, A.P.; de Vet, H.C.; de Bie, R.A.; Kessels, A.G.; Boers, M.; Bouter, L.M.; Knipschild, P.G. The Delphi list: A criteria list for quality assessment of randomized clinical trials for conducting systematic reviews developed by Delphi consensus. J. Clin. Epidemiol. 1998, 51, 1235–1241. [Google Scholar] [CrossRef] [Green Version]
- Armijo-Olivo, S.; da Costa, B.R.; Cummings, G.G.; Ha, C.; Fuentes, J.; Saltaji, H.; Egger, M. PEDro or Cochrane to Assess the Quality of Clinical Trials? A Meta-Epidemiological Study. PLoS ONE 2015, 10, e0132634. [Google Scholar] [CrossRef] [Green Version]
- Janaudis-Ferreira, T.; Henriksson-Larsén, K.; Lundgren, R.; Wadell, K. Differences in training effects following training with and without supplemental oxygen in patients with COPD. Adv. Physiother. 2009, 11, 186–192. [Google Scholar] [CrossRef]
- Wadell, K.; Henriksson-Larsen, K.; Lundgren, R. Physical training with and without oxygen in patients with chronic obstructive pulmonary disease and exercise-induced hypoxaemia. J. Rehabil. Med. 2001, 33, 200–205. [Google Scholar]
- Dyer, F.; Callaghan, J.; Cheema, K.; Bott, J. Ambulatory oxygen improves the effectiveness of pulmonary rehabilitation in selected patients with chronic obstructive pulmonary disease. Chron. Respir. Dis. 2012, 9, 83–91. [Google Scholar] [CrossRef] [Green Version]
- Borghi-Silva, A.; Mendes, R.G.; Toledo, A.C.; Malosá Sampaio, L.M.; da Silva, T.P.; Kunikushita, L.N.; de Souza, H.C.D.; Salvini, T.F.; Costa, D. Adjuncts to physical training of patients with severe COPD: Oxygen or noninvasive ventilation? Respir. Care 2010, 55, 885–894. [Google Scholar]
- Rooyackers, J.M.; Dekhuijzen, P.N.; Van Herwaarden, C.L.; Folgering, H.T. Training with supplemental oxygen in patients with COPD and hypoxaemia at peak exercise. Eur. Respir. J. 1997, 10, 1278–1284. [Google Scholar] [CrossRef] [Green Version]
- Fichter, J.; Fleckenstein, J.; Stahl, C.; Sybrecht, G.W. Effect of oxygen (FI02: 0.35) on the aerobic capacity in patients with COPD. Pneumologie 1999, 53, 121–126. [Google Scholar] [PubMed]
- Garrod, R.; Paul, E.A.; Wedzicha, J.A. Supplemental oxygen during pulmonary rehabilitation in patients with COPD with exercise hypoxaemia. Thorax 2000, 55, 539–543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Emtner, M.; Porszasz, J.; Burns, M.; Somfay, A.; Casaburi, R. Benefits of supplemental oxygen in exercise training in nonhypoxemic chronic obstructive pulmonary disease patients. Am. J. Respir. Crit. Care Med. 2003, 168, 1034–1042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karlsen, T.; Hoff, J.; Stoylen, A.; Skovholdt, M.C.; Gulbrandsen Aarhus, K.; Helgerud, J. Aerobic interval training improves VO2peak in coronary artery disease patients; no additional effect from hyperoxia. Scand. Cardiovasc. J. 2008, 42, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Bjørgen, S.; Helgerud, J.; Husby, V.; Steinshamn, S.; Richadson, R.R.; Hoff, J. Aerobic high intensity one-legged interval cycling improves peak oxygen uptake in chronic obstructive pulmonary disease patients; no additional effect from hyperoxia. Int. J. Sports Med. 2009, 30, 872–878. [Google Scholar] [CrossRef] [Green Version]
- Scorsone, D.; Bartolini, S.; Saporiti, R.; Braido, F.; Baroffio, M.; Pellegrino, R.; Brusasco, V.; Crimi, E. Does a low-density gas mixture or oxygen supplementation improve exercise training in COPD? Chest 2010, 138, 1133–1139. [Google Scholar] [CrossRef]
- Ringbaek, T.; Martinez, G.; Lange, P. The long-term effect of ambulatory oxygen in normoxaemic COPD patients: A randomised study. Chron. Respir. Dis. 2013, 10, 77–84. [Google Scholar] [CrossRef]
- Spielmanns, M.; Fuchs-Bergsma, C.; Winkler, A.; Fox, G.; Kruger, S.; Baum, K. Effects of Oxygen Supply During Training on Subjects with COPD Who Are Normoxemic at Rest and During Exercise: A Blinded Randomized Controlled Trial. Respir. Care 2015, 60, 540–548. [Google Scholar] [CrossRef] [Green Version]
- Neunhauserer, D.; Steidle-Kloc, E.; Weiss, G.; Kaiser, B.; Niederseer, D.; Hartl, S.; Tschentscher, M.; Egger, A.; Schönfelder, M.; Lamprecht, B.; et al. Supplemental Oxygen During High-Intensity Exercise Training in Nonhypoxemic Chronic Obstructive Pulmonary Disease. Am. J. Med. 2016, 129, 1185–1193. [Google Scholar] [CrossRef]
- Alison, J.A.; McKeough, Z.J.; Leung, R.W.M.; Holland, A.E.; Hill, K.; Morris, N.R.; Jenkins, S.; Spencer, L.M.; Hill, C.J.; Lee, A.L.; et al. Oxygen compared to air during exercise training in COPD with exercise-induced desaturation. Eur. Respir. J. 2019, 53, 1802429. [Google Scholar] [CrossRef]
- Borg, G. Perceived exertion as an indicator of somatic stress. Scand. J. Rehabil. Med. 1970, 2, 92–98. [Google Scholar] [PubMed]
- Burdon, J.G.W.; Juniper, E.F.; Killian, K.J.; Hargreave, F.E.; Campbell, E.J. The perception of breathlessness in asthma. Am. Rev. Respir Dis. 1982, 126, 825–828. [Google Scholar] [PubMed]
- Perdrizet, G.A. Chronic diseases as barriers to oxygen delivery: A unifying hypothesis of tissue reoxygenation therapy. Adv. Exp. Med. Biol. 2017, 977, 15–20. [Google Scholar] [PubMed]
- Eltzschig, H.K.; Carmeliet, P. Hypoxia and Inflammation. N. Engl. J. Med. 2011, 364, 656–665. [Google Scholar] [CrossRef] [Green Version]
- Chronos, N.; Adams, L.; Guz, A. Effect of hyperoxia and hypoxia on exercise-induced breathlessness in normal subjects. Clin. Sci. 1988, 74, 531–537. [Google Scholar] [CrossRef]
- Schmidt, M.E.; Wiskemann, J.; Armbrust, P.; Schneeweiss, A.; Ulrich, C.M.; Steindorf, K. Effects of resistance exercise on fatigue and quality of life in breast cancer patients undergoing adjuvant chemotherapy: A randomized controlled trial. Int. J. Cancer 2015, 137, 471–480. [Google Scholar] [CrossRef]
- Ekström, M.; Zainab, A.; Bornefalk-Hermansson, A.; Abernethy, A.; Currow, D. Oxygen for Breathlessness in Patients with Chronic Obstructive Pulmonary Disease Who Do Not Qualify for Home Oxygen Therapy. Cochrane Database Sys Rev. 2016, 11. [Google Scholar] [CrossRef] [Green Version]
- Uronis, H.; McCrory, D.C.; Samsa, G.; Currow, D.; Abernethy, A. Symptomatic oxygen for non-hypoxaemic chronic obstructive pulmonary disease. In Cochrane Database of Systematic Reviews; Abernethy, A., Ed.; John Wiley & Sons, Ltd.: Chichester, UK, 2011; p. CD006429. [Google Scholar]
- González-Muniesa, P.; Garcia-Gerique, L.; Quintero, P.; Arriaza, S.; Lopez-Pascual, A.; Martinez, J.A. Effects of hyperoxia on oxygen-related inflammation with a focus on obesity. Oxid. Med. Cell. Longev. 2016, 2016, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Fujimoto, K.; Matsuzawa, Y.; Yamaguchi, S.; Koizumi, T.; Kubo, K. Benefits of oxygen on exercise performance and pulmonary hemodynamics in patients with COPD with mild hypoxemia. Chest 2002, 122, 457–463. [Google Scholar] [CrossRef] [Green Version]
- Somfay, A.; Pórszász, J.; Lee, S.-M.; Casaburi, R. Effect of Hyperoxia on Gas Exchange and Lactate Kinetics Following Exercise Onset in Nonhypoxemic COPD Patients. Chest 2002, 121, 393–400. [Google Scholar] [CrossRef] [Green Version]
- Basch, E.; Reeve, B.B.; Mitchell, S.A.; Clauser, S.B.; Minasian, L.M.; Dueck, A.C.; Mendoza, T.R.; Hay, J.; Atkinson, T.M.; Abernethy, A.P.; et al. Development of the national cancer institute’s patient-reported outcomes version of the common terminology criteria for adverse events (PRO-CTCAE). J. Natl. Cancer Inst. 2014, 106, 244. [Google Scholar] [CrossRef] [PubMed]
- Snider, G.L. Enhancement of Exercise Performance in COPD Patients by Hyperoxia. Chest 2002, 122, 1830–1836. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ambrosino, N.; Strambi, S. New strategies to improve exercise tolerance in chronic obstructive pulmonary disease. Eur. Respir. J. 2004, 24, 313–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wickerson, L. Oxygen administration during pulmonary rehabilitation. Can. J. Respir. Crit. Care. Sleep Med. 2018, 2, 190–193. [Google Scholar] [CrossRef]
- Nixon, P.A.; Orenstein, D.M.; Curtis, S.E.; Ross, E.A. Oxygen supplementation during exercise in cystic fibrosis. Am. Rev. Respir. Dis. 1990, 142, 807–811. [Google Scholar] [CrossRef] [PubMed]
- Rozenberg, R.; Mankowski, R.T.; Van Loon, L.J.C.; Langendonk, J.G.; Sijbrands, E.J.G.; van den Meiracker, A.H.; Stam, H.J.; Praet, S.F.E. Hyperoxia increases arterial oxygen pressure during exercise in type 2 diabetes patients: A feasibility study. Eur. J. Med. Res. 2016, 21, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brinkmann, C.; Metten, A.; Scriba, P.; Tagarakis, C.V.M.; Wahl, P.; Latsch, J.; Brixius, K.; Bloch, W. Hypoxia and Hyperoxia Affect Serum Angiogenic Regulators in T2DM Men during Cycling. Int. J. Sports Med. 2017, 38, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Cotes, J.E.; Gilson, J.C. Effect of Oxygen on Exercise Ability in Chronic Respiratory Insufficiency. Lancet 1956, 267, 872–876. [Google Scholar] [CrossRef]
- Chatila, W.; Nugent, T.; Vance, G.; Gaughan, J.; Criner, G.J. The effects of high-flow vs low-flow oxygen on exercise in advanced obstructive airways disease. Chest 2004, 126, 1108–1115. [Google Scholar] [CrossRef] [Green Version]
- Burgos, C.; Henríquez-Olguín, C.; Andrade, D.C.; Ramírez-Campillo, R.; Araneda, O.F.; White, A.; Cerda-Kohler, H. Effects of exercise training under hyperbaric oxygen on oxidative stress markers and endurance performance in young soccer players: A pilot study. J. Nutr. Metab. 2016, 2016, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Lock, S.H.; Blower, G.; Prynne, M.; Wedzicha, J.A. Comparison of liquid and gaseous oxygen for domiciliary portable use. Thorax 1992, 47, 98–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nasilowski, J.; Przybylowski, T.; Zielinski, J.; Chazan, R. Comparing supplementary oxygen benefits from a portable oxygen concentrator and a liquid oxygen portable device during a walk test in COPD patients on long-term oxygen therapy. Respir. Med. 2008, 102, 1021–1025. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, A.S.; Burns, B.; Goadsby, P.J. High-flow oxygen for treatment of cluster headache: A randomized trial. JAMA J. Am. Med. Assoc. 2009, 302, 2451–2457. [Google Scholar] [CrossRef] [PubMed]
- Dewan, N.A.; Bell, C.W. Effect of low flow and high flow oxygen delivery on exercise tolerance and sensation of dyspnea: A study comparing the transtracheal catheter and nasal prongs. Chest 1994, 105, 1061–1065. [Google Scholar] [CrossRef] [PubMed]
- Davidson, A.C.; Leach, R.; George, R.J.; Geddes, D.M. Supplemental oxygen and exercise ability in chronic obstructive airways disease. Thorax 1988, 43, 965–971. [Google Scholar] [CrossRef] [Green Version]
- Lindholm, P.; Larsson, Å.; Frånberg, O.; Gullstrand, L. A Portable Device for Intermittent Oxygen Supplementation during High-Intensity Exercise. J. Biomed. Sci. Eng. 2017, 10, 304–316. [Google Scholar] [CrossRef] [Green Version]
- Bazuaye, E.A.; Stone, T.N.; Corris, P.A.; Gibson, G.J. Variability of inspired oxygen concentration with nasal cannulas. Thorax 1992, 47, 609–611. [Google Scholar] [CrossRef] [Green Version]
- Katz, I.; Chen, J.; Duong, K.; Zhu, K.; Pichelin, M.; Caillibotte, G.; Martin, A.R. Dose variability of supplemental oxygen therapy with open patient interfaces based on in vitro measurements using a physiologically realistic upper airway model. Respir. Res. 2019, 20, 149. [Google Scholar] [CrossRef] [Green Version]
- Niinimaa, V.; Cole, P.; Mintz, S.; Shephard, R.J. The switching point from nasal to oronasal breathing. Respir. Physiol. 1980, 42, 61–71. [Google Scholar] [CrossRef]
- Neunhäuserer, D.; Steidle-Kloc, E.; Bergamin, M.; Weiss, G.; Ermolao, A.; Lamprecht, B.; Studnicka, M.; Niebauer, J. Role of Breathing Conditions during Exercise Testing on Training Prescription in Chronic Obstructive Pulmonary Disease. Am. J. Phys. Med. Rehabil. 2017, 96, 908–911. [Google Scholar] [CrossRef]
- Owen, J.; McEwan, C.; Nesbitt, H.; Bovornchutichai, P.; Averre, R.; Borden, M.; McHale, A.P.; Callan, J.F.; Stride, E. Reducing tumour hypoxia via oral administration of oxygen nanobubbles. PLoS ONE 2016, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kheir, J.N.; Polizzotti, B.D.; Thomson, L.M.; O’Connel, D.W.; Black, K.J.; Lee, R.W.; Wilking, J.N.; Graham, A.C.; Bell, D.C.; McGowan, F.X. Bulk manufacture of concentrated oxygen gas-filled microparticles for intravenous oxygen delivery. Adv. Healthc Mater. 2013, 2, 1131–1141. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.S.; Hwang, J.; Seo, Y.; Shin, K.; Lee, K.; Park, C.; Choi, Y.; Hong, J.W.; Choi, J. Engineering oxygen nanobubbles for the effective reversal of hypoxia. Artif Cells Nanomedicine Biotechnol. 2018, 46 (Suppl. S3), S318–S327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weston, K.S.; Wisløff, U.; Coombes, J.S. High-intensity interval training in patients with lifestyle-induced cardiometabolic disease: A systematic review and meta-analysis. Br. J. Sports Med. 2014, 48, 1227–1234. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Entity | Design & Blinding | Final Sample & Dropout Rate | Technical Realization | Training Duration & Frequency | Intervention Characteristics | Outcomes of Interest | Conclusion |
|---|---|---|---|---|---|---|---|---|
| Rooyackers et al. 1997 Netherlands | COPD | RCT (parallel) Blinding: not reported | SO n = 2 women and 10 men; Age: 63 ± 5 yrs. Normoxia: n = 2 women and 10 men; Age: 59 ± 13 yrs. Dropouts: not reported | SO: 4 L min−1 via dual prong nasal cannula Normoxia: ambient air | 10 weeks 5 x week | Supervised interval training: 5 times of 2 min active cycling and 2 min rest; rowing for 5 min; dynamic resistance exercise for arms, shoulders, back and legs for 10 min; isometric resistance exercise for 3 min; functional tests/training i.e., stair climbing, chair rise, slalom walk, carrying light weight (1–2 kg) above and below shoulder level for 13 min (workload was increased as tolerated and not to fall below an SaO2 of 90%; warm-up and cool down not specified). Total training time: 51 min | Wmax VO2peak HRpeak 6MWT TTE Dyspnoea Stair climb Weight lifted CRDQ | Supplemental oxygen did not show an advantage compared to normoxia for chronic improvements in QoL, 6MWT, stair-climbing and weight-carrying test. The normoxia condition but not supplemental oxygen led to a statistically significant increase in Wmax without a group difference. |
| Fichter et al. 1999 Germany | COPD | RCT (parallel) Blinding: participants | SO: n = 5 men; Age: 58 ± 11 yrs. Normoxia: n = 5 men; Age: 59 ± 7 yrs. Dropouts: not reported | SO: humidified 35% O2 via mixed chamber Normoxia: humidified decompressed air 21% O2 | 4 weeks 5 x week | Supervised constant cycling with 80% of Wmax for 45 min (warm-up and cool down not specified). Total training time: 45 min | Wmax VO2peak HRpeak BLa | Only the normoxia condition led to a statistically significant higher maximum power output, accompanied by statistically significant lower blood lactate concentrations after the intervention. No statistically significant changes occurred in the supplemental oxygen group. |
| Garrod et al. 2000 England | COPD | RCT (parallel) Blinding: Participants | SO: n = 13; Age: 64.3 (54–77) yrs. Normoxia: n = 12; Age: 71.6 (52–81) yrs. Gender ratio not reported Dropouts: SO = 2 Normoxia = 1 | SO: 4 L min−1 via nasal cannula and conserving device Normoxia: 4 L∙min−1 compressed air | 6 weeks 3 x week | Supervised dynamic resistance exercise with external loads for arms and without external loading for lower limbs; fast walking over 10 m at 80% of VO2peak determined by baseline shuttle walk test; unloaded cycling until intolerance (warm-up and cool down not specified). Total training time: 60 min | ISWT Dyspnoea CRDQ HADS LCADL | Supplemental oxygen led to a statistically significant greater reduction in dyspnoea compared to the normoxia condition. Covered distance of the shuttle walk test and patient-reported outcomes (i.e., hospital anxiety and depression scale, chronic respiratory disease questionnaire and London chest activity of daily living scale) improved during a rehabilitation program of 6 weeks without any statistical differences between the two conditions. |
| Wadell et al. 2001 Sweden | COPD | RCT (parallel) Blinding: participants | SO: n = 6 women and 5 men; Age: 65 (52–73) yrs. Normoxia: n = 6 women and 5 men; Age: 69 (60–72) yrs. Dropouts: SO = 1 Normoxia = 1 | SO: 5 L min−1 via dual prong nasal cannula Normoxia: 5 L min−1 via dual prong nasal cannula of compressed air | 8 weeks 3 x week | Supervised interval training on a motorized treadmill: 5 min warm-up, 2–3 min higher speed separated by 2–3 min lower speed, 2–5 min cool-down; intensity was set to achieve target dyspnoea 7 out of 10 or subjective exertion of 17 on the 6–20 BORG scale; training was paused if SaO2 fall below 90% or values of dyspnoea and exhaustion exceeded target range. Total training time: 30 min | HRpeak BLa 6MWT RPE Dyspnoea | Distance covered in the 6MWT improved statistically significant in both groups with a greater increase in the normoxia condition. Furthermore, only the normoxia group statistically decreased rating for perceived exertion in the 6MWT. |
| Emtner et al. 2003 United States of America | COPD | RCT (parallel) Blinding: Participant, exercise supervisors and analyzing investigators | SO: n = 6 women and 8 men; Age: 66 ± 7 yrs. Normoxia: n = 5 women and 10 men; Age: 67 ± 10 yrs. Dropouts: SO = 1 | SO: 3 L min−1 via nasal cannula Normoxia: 3 L min−1 via nasal cannula of compressed air | 7 weeks 3 x week | Supervised ergometer cycling: 5 min warm-up, 35 min of high-intensity, 5 min cool-down. Exercise intensity during the first week was low and increased to 75% of Wmax (determined by baseline incremental test) in second week. Further adjustments were made according to dyspnoea and fatigue sensation. Total training time: 45 min | Wmax VO2peak HRpeak BLa TTE Dyspnoea Leg fatigue CRDQ SF-36 | Both groups statistically improved exercise tolerance with a higher increase in total work rate in the supplemental oxygen group compared to the normoxia condition. Supplemental oxygen caused a greater tolerance to high-intensity exercise compared to high-intensity loading in ambient condition. |
| Karlsen et al. 2008 Norway | CAD | RCT (parallel) Blinding: not reported | SO: n = 2 women and 6 men; Age: 61.1 ± 7.1 yrs. Normoxia: n = 3 women and 7 men; Age: 63.6 ± 6.5 yrs. Dropouts: SO = 2 Normoxia = 1 | SO: 100% O2 enriched air via Douglas bag connected to a tank via a face mask and three valve system Normoxia: ambient air | 10 weeks 3 x week | Supervised treadmill walking: 5 min warm-up, high-intensity training of 4 × 4 min at 85–95% HRpeak separated by 3 min active rest at 60–70% HRpeak. Treadmill speed and inclination where increased throughout the study period (cool-down not reported). Total training time: 31 min | Wmax VO2peak HRpeak BLa RPE SF-36 Macnew | Exercise performance, VO2peak, maximal ventilation and cardiac output as well as stroke volume increased statistically significant in both groups without a between-group effect. Patient-reported outcomes improved similarly. Supplemental oxygen did not show any additional training effects. |
| Bjørgen et al. 2009 Norway | COPD | RCT (parallel) Blinding: not reported | SO: n = 5 women and 2 men; Age: 61 ± 12 yrs. Normoxia: n = 2 women and 3 men; Age: 61 ± 8 yrs. Dropouts: SO = 1 Normoxia = 2 | SO: 100% O2 via mask connected to a plastic balloon which was constantly refilled Normoxia: ambient air | 8 weeks 3 x week | Supervised one-legged interval cycling: 10 min warm-up (both legs); high-intensity training of 8 × 4 min at 85–95% HRpeak (legs alternating); the resting leg was placed on the bike between the pedals (cool-down not reported). Total training time: 42 min | Wmax VO2peak HRpeak BLa RPE | Exercise performance improved statistically significant in both conditions without a between-group difference. Supplemental oxygen did not show any additional training effects compared to ambient air. |
| Scorsone et al. 2010 Italy | COPD | RCT (parallel) Blinding: participants and exercise supervisors | SO: n = 3 women and 7 men; Age: 67 ± 9 yrs. Normoxia: n = 3 women and 7 men; Age: 68 ± 7 yrs. Dropouts:none | SO: 40% O2 through mouthpiece connected to a Douglas bag Normoxia: humidified room air through mouthpiece connected to a Douglas bag | 8 weeks 3 x week | Supervised ergometer cycling: 5 min warm-up, 30 min high-intensity exercise, 5 min cool-down. Exercise intensity during the first week was 40% of Wmax and increased to 80% of Wmax (determined by baseline incremental test) in second/third week. Adjustments were made according to dyspnoea and fatigue sensation. Total training time: 40 min | Wmax VO2peak HRpeak TTE Dyspnoea Leg fatigue | High-intensity training led to statistically significant improvements of VO2peak, Wmax and time to exhaustion without a between-group difference. Supplemental oxygen did not show any additional training effects compared to humidified normoxic air. |
| Ringbaek et al. 2013 Denmark | COPD | RCT (parallel) Blinding: no | SO: n = 11 women and 11 men; Age: 69.4 ± 9.8 yrs. Normoxia: n = 10 women and 13 men; Age: 68.6 ± 7.8 yrs. Dropouts: Week 0–7 SO = 6 Normoxia = 1 Week 7–20 SO = 1 Normoxia = 1 | SO: 2 L min−1 through a 2.3 kg portable oxygen concentrator including a conserving deviceNormoxia: ambient air | 7 weeks 2 x week Followed by 13 weeks 1 x week | Supervised walking and cycling: 30 min including warm-up and cool-down. Exercise intensity was set to reach 85% of VO2peak (determined by baseline incremental shuttle walk test). Total training time: 30 min | ESWT SGRQ | Both groups improved statistically significant endurance performance assessed via endurance shuttle walk test at 85% VO2peak (predicted through incremental shuttle walk test) and patient-reported outcomes (St. George’s Respiratory Questionnaire) without a between-group effect. Supplemental oxygen showed no additional benefits compared to ambient air. |
| Spielmanns et al. 2015 Germany | COPD | RCT (parallel) Blinding: participants and investigator | SO: n = 9 women and 10 men; Age: 65 ± 8.7 yrs. Normoxia: n = 8 women and 9 men; Age: 64 ± 8.4 yrs. Dropouts: SO = 23 Normoxia = 26 | SO: 4 L min−1 O2 via nasal cannula leading to an FiO2 of approximately 0.35 Normoxia: compressed air at 4 L min−1 via nasal cannula | 24 weeks 3 x week | Supervised ergometer cycling: First 12 weeks included an interval training and the second 12-week period included a continuous loading. Exercise intensity for interval training: weeks 1–3 with 6 × 1 min at 110% Wmax and 4 min at 60% Wmax as active rest; weeks 4–6 with 6 × 1 min at 115% Wmax and 4 min at 65% Wmax; weeks 7–9 with 6 × 1 min at 120% Wmax and 4 min at 70% Wmax; weeks 10–12 with 6 × 1 min at 125% Wmax and 4 min at 75% Wmax. Continuous loading increased every 3 weeks by 5% starting from 70% Wmax to 85% Wmax. Total training time: 30 min | Wmax VO2peak BLa 6MWT SF-36 | Both groups showed statistically significant improvements in QoL, exercise tolerance, VO2peak and distance covered in the 6MWT. Apart from further increase in exercise tolerance, these improvements occurred within the first 12 weeks and were maintained in week 24. Supplemental oxygen did not show any further enhancing effects on outcome values. |
| Neunhäuserer et al. 2016 Austria | COPD | RCT (parallel and cross over †) Blinding: participants and investigator | SO: n = 1 women and 14 men; Age: 63.1 ± 5.4 yrs. Normoxia: n = 7 women and 7 men; Age: 64.1 ± 6.1 yrs. Dropouts before crossover (total): SO = 6 (7) Normoxia = 7 (8) | SO: 10 L min−1 O2 via nasal cannula leading to an FiO2 of approximately 0.6 Normoxia: compressed air at 10 L min−1 via nasal cannula | 6 weeks ‡ 3 x week | Supervised ergometer interval cycling and resistance training: 5-min warm-up; 7 × 1 min at 70–80% Wmax and 2 min at 50% Wmax as active rest; 5 min cool-down. Resistance training included 8 high-intensity exercises performed on machines with 1 set of 8–15 reps to failure: latissimus pull-down, shoulder press, back extension, abdominal crunch, butterfly, reverse butterfly, leg extension and leg flexion. Progression was made if more than 15 reps were performed. Total training time: 31 min without time of resistance training | Wmax VO2peak HRpeak BLa 10-RM § HADS § | Supplemental oxygen showed statistically significant improvements in relative Wmax compared to normoxia. Strength gains increased in both groups without a significant between-group effect. Supplemental oxygen added superior effects on top of the endurance-induced improvements without an effect on muscle strength. |
| Alison et al. 2019 Australia | COPD | RCT (parallel) Blinding: participants, therapists and investigators | SO: n = 28 women and 30 men; Age: 69 ± 7 yrs. Normoxia: n = 22 women and 31 men; Age: 69 ± 8 yrs. Dropouts: SO = 6 Normoxia = 8 | SO: 5 L min−1 via dual prong nasal cannula delivered via an oxygen concentrator producing 90 ± 3 % oxygen Normoxia: 5 L min−1 via dual prong nasal cannula of medical air | 8 weeks 3 x week | Supervised treadmill walking: 20 min at 80% average speed assessed by 6MWT and 10 min cycling at 60% Wmax estimated from 6MWT with progression to 20 min cycling by week 3 leading to a total training time of 40 min. Intensity was modified to keep dyspnoea and RPE between 3 and 4 on the modified BORG scale (0–10). Total training time: 30–40 min | ESWT ISWT CRDQ Dyspnoea-12 | Supplemental oxygen and normoxia statistically improved statistically exercise capacity assessed by ESWT and ISWT as well as quality of life in COPD patients who demonstrated oxygen desaturation during exercise. No statistical between-group difference were observed for dyspnoea, although dyspnoea statistically improved only in the supplemental oxygen group. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Freitag, N.; Doma, K.; Neunhaeuserer, D.; Cheng, S.; Bloch, W.; Schumann, M. Is Structured Exercise Performed with Supplemental Oxygen a Promising Method of Personalized Medicine in the Therapy of Chronic Diseases? J. Pers. Med. 2020, 10, 135. https://doi.org/10.3390/jpm10030135
Freitag N, Doma K, Neunhaeuserer D, Cheng S, Bloch W, Schumann M. Is Structured Exercise Performed with Supplemental Oxygen a Promising Method of Personalized Medicine in the Therapy of Chronic Diseases? Journal of Personalized Medicine. 2020; 10(3):135. https://doi.org/10.3390/jpm10030135
Chicago/Turabian StyleFreitag, Nils, Kenji Doma, Daniel Neunhaeuserer, Sulin Cheng, Wilhelm Bloch, and Moritz Schumann. 2020. "Is Structured Exercise Performed with Supplemental Oxygen a Promising Method of Personalized Medicine in the Therapy of Chronic Diseases?" Journal of Personalized Medicine 10, no. 3: 135. https://doi.org/10.3390/jpm10030135