Roles of ERCP in the Early Diagnosis of Pancreatic Cancer

Abstract
:1. Introduction
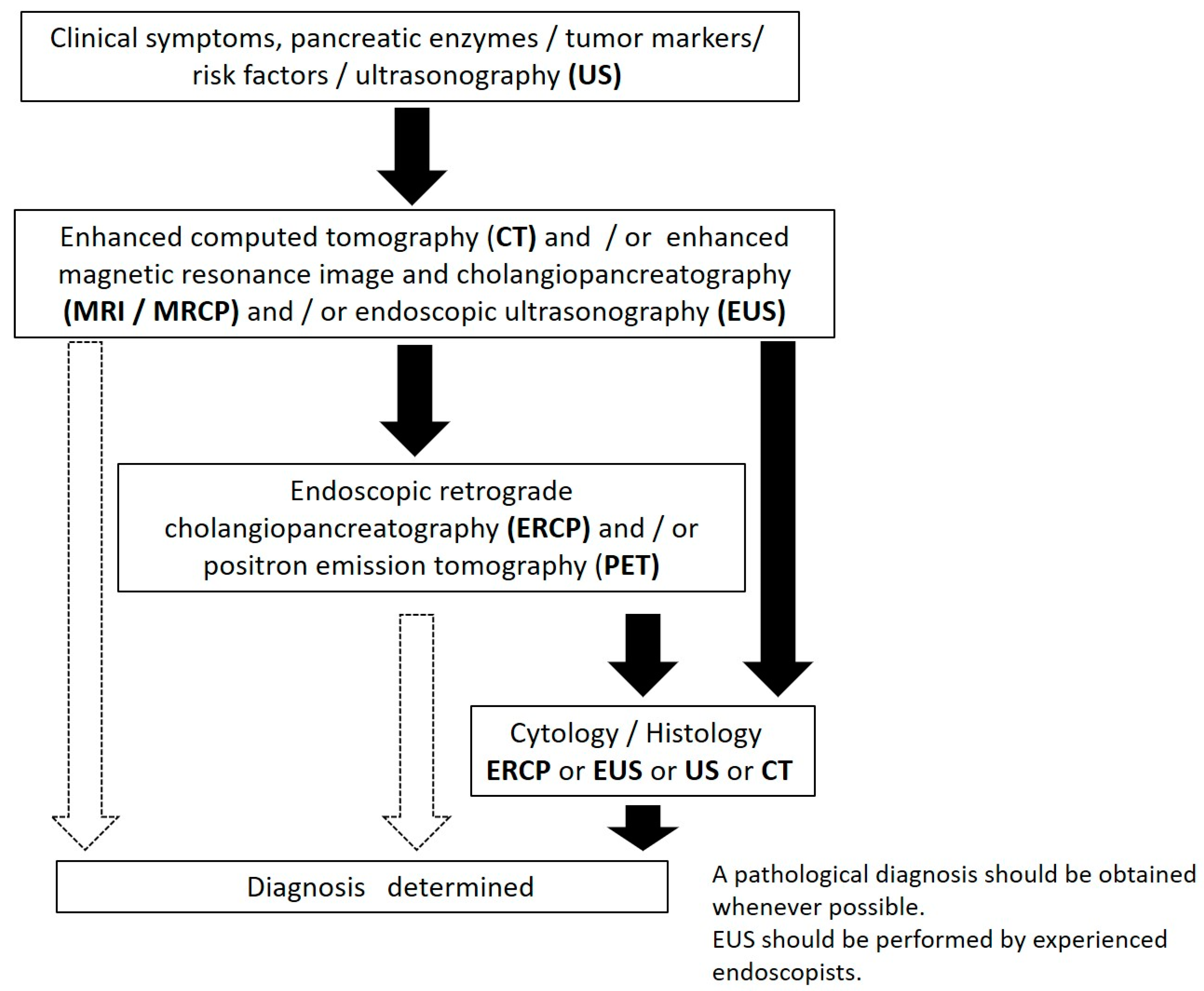
2. Diagnostic Algorithm for Cases of Early-Stage PC in Japan
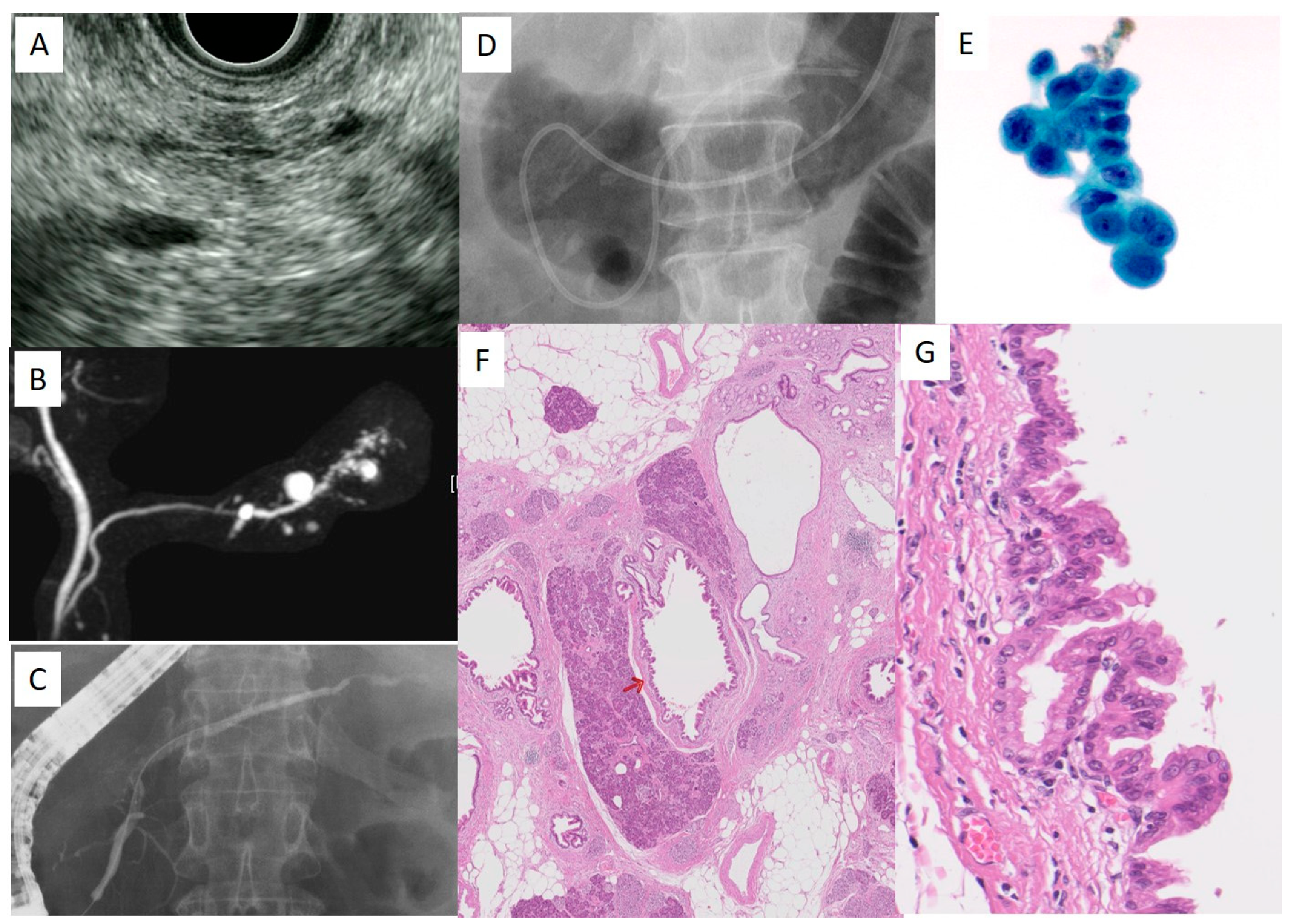
3. Imaging Findings in Cases of Early-Stage PC
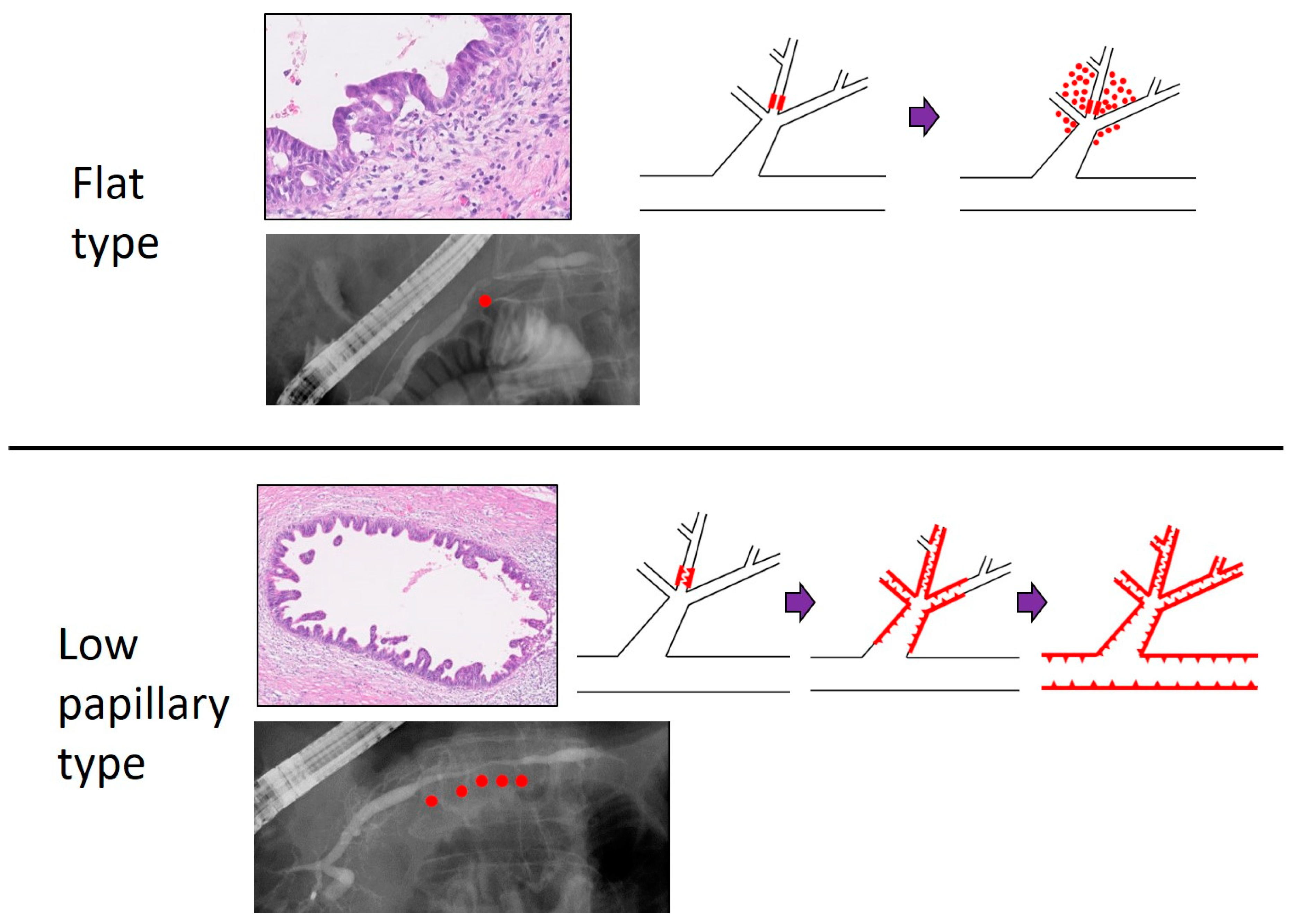
4. Pathologic Findings of PCIS
5. Cytologic Diagnosis of Cases of Early-Stage PC
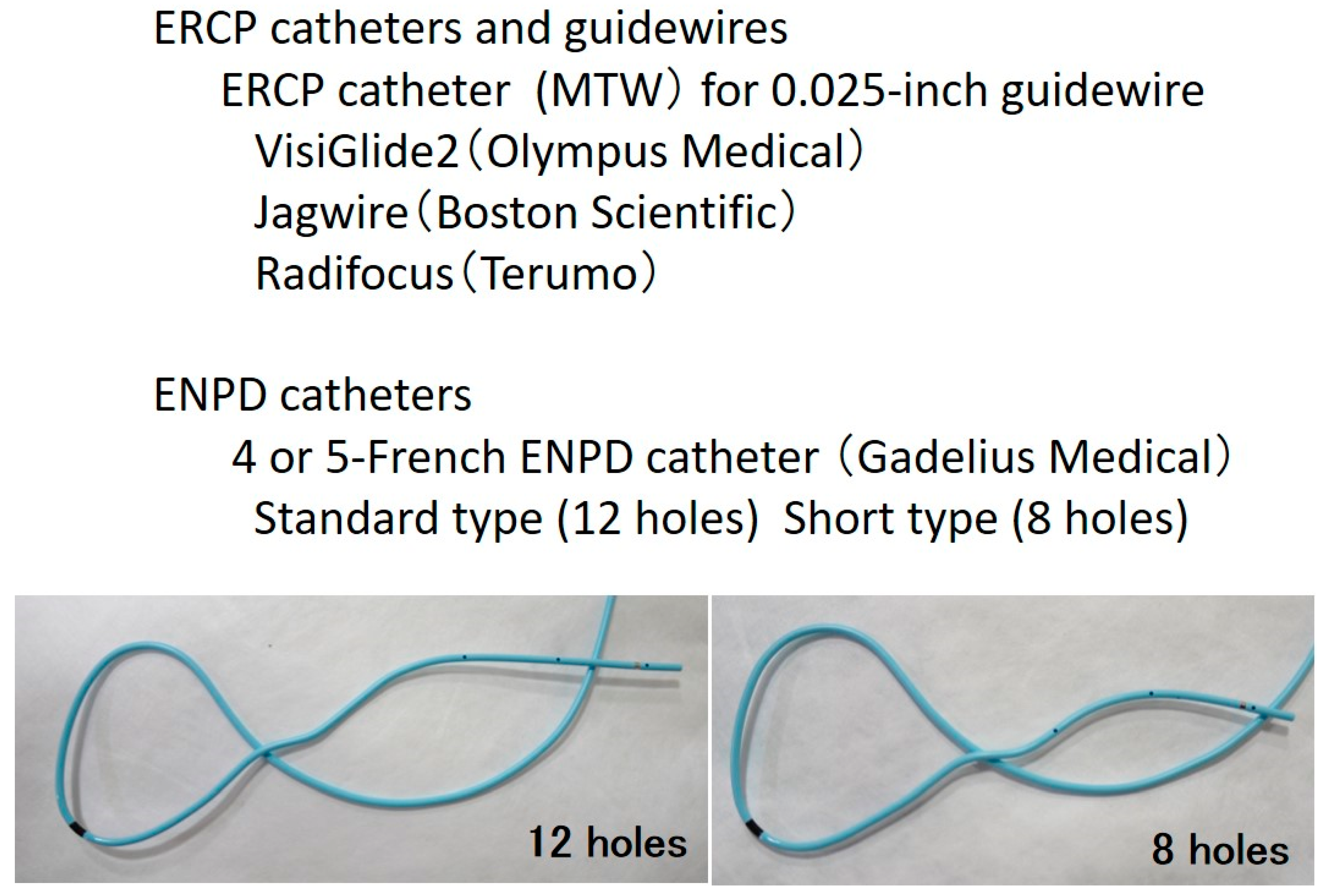
6. A Practical Method of SPACE for Cases of Early-Stage PC
7. Evolutionary SPACE
8. Summary
Funding
Conflicts of Interest
Abbreviations
| CGL | clinical guidelines |
| CT | computed tomography |
| ENPD | endoscopic nasopancreatic drainage |
| ERCP | endoscopic retrograde cholangiopancreatography |
| EUS | endoscopic ultrasonography |
| EUS-FNA | endoscopic ultrasound-guided fine needle aspiration |
| F | flat |
| JEDPAC | Japan Study Group on the Early Detection of Pancreatic Cancer |
| LP | low papillary |
| MRCP | magnetic resonance cholangiopancreatography |
| MPD | main pancreatic duct |
| PC | pancreatic cancer |
| PCIS | pancreatic cancer in situ |
| PEP | post-ERCP pancreatitis |
| SPACE | serial pancreatic juice aspiration cytologic examination |
| US | Ultrasonography |
References
- Warshaw, A.L.; Castillo, C.F. Pancreatic carcinoma. N. Engl. J. Med. 1992, 326, 455–465. [Google Scholar] [CrossRef] [PubMed]
- Rosewicz, S.; Wiedenmann, B. Pancreatic carcinoma. Lancet 1997, 349, 485–489. [Google Scholar] [CrossRef]
- Egawa, S.; Toma, H.; Ohigashi, H.; Okusaka, T.; Nakao, A.; Hatori, T.; Maguchi, H.; Yanagisawa, A.; Tanaka, M. Japan Pancreatic Cancer Registry; 30th Year Anniversary. Pancreas 2012, 41, 985–992. [Google Scholar] [CrossRef] [PubMed]
- Kanno, A.; Masamune, A.; Hanada, K.; Maguchi, H.; Shimizu, Y.; Ueki, T.; Hasebe, O.; Ohtsuka, T.; Nakamura, M.; Takenaka, M.; et al. Multicenter study of early pancreatic cancer in Japan. Pancreatology 2018, 18, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Furuta, K.; Watanaabe, H.; Ikeda, S. Differences between solid and duct-ectatic type of pancreatic ductal carcinoma. Cancer 1992, 69, 1327–1333. [Google Scholar] [CrossRef]
- Ikeda, S.; Maeshiro, K.; Ryu, S.; Ogata, K.; Yasunari, Y.; Nakayama, Y.; Hamada, Y. Diagnosis of small pancreatic cancer by endoscopic balloon-catheter spot pancreatography. An analysis of 29 patients. Pancreas 2009, 38, e102–e113. [Google Scholar] [CrossRef] [PubMed]
- Bhutani, M.S.; Konduru, P.; Joshi, V.; Saxena, P.; Suzuki, R.; Irisawa, A.; Yamao, K. The role of endoscopic ultrasound in pancreatic cancer screening. Endosc. Ultrasound 2016, 5, 8–16. [Google Scholar] [CrossRef] [PubMed]
- Nakaizumi, A.; Tatsuta, M.; Uehara, H.; Yamamoto, R.; Takenaka, A.; Kishigami, Y.; Takemura, K.; Kitamura, T.; Okuda, S. Cytologic examination of pure pancreatic juice in the diagnosis of pancreatic carcinoma. The endoscopic retrograde intraductal catheter aspiration cytologic technique. Cancer 1992, 70, 2610–2614. [Google Scholar] [CrossRef] [Green Version]
- Nakaizumi, A.; Tatsuta, M.; Uehara, H.; Takenaka, A.; Ishii, H.; Kitamura, T.; Ohigashi, H.; Ishikawa, O.; Okuda, S.; Wada, A. Effectiveness of the cytologic examination of pure pancreatic juice in the diagnosis of early neoplasia of the pancreas. Cancer 1995, 76, 750–757. [Google Scholar] [CrossRef]
- Miyata, T.; Takenaka, M.; Omoto, S.; Kamata, K.; Minaga, K.; Yamao, K.; Imai, H.; Kudo, M. A case of pancreatic carcinoma in situ diagnosed by repeated pancreatic juice cytology. Oncology 2017, 93 (Suppl. 1), 98–101. [Google Scholar] [CrossRef] [PubMed]
- Iiboshi, T.; Hanada, K.; Fukuda, T.; Yonehara, S.; Sasaki, T.; Chayama, K. Value of cytodiagnosis using endoscopic nasopancreatic drainage for early diagnosis of pancreatic cancer. Pancreas 2012, 41, 523–529. [Google Scholar] [CrossRef] [PubMed]
- Satoh, T.; Kikuyama, M.; Kawaguchi, S.; Kanemoto, H.; Muro, H.; Hanada, K. Acute pancreatitis-onset carcinoma in situ of the pancreas with focal fat replacement diagnosed using serial pancreatic-juice aspiration cytologic examination (SPACE). Clin. J. Gastroenterol. 2017, 10, 541–545. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, K.; Okusaka, T.; Shimizu, K.; Furuse, J.; Ito, Y.; Hanada, K.; Shimosegawa, T.; Okazaki, K. Clinical Practice Guidelines for Pancreatic Cancer 2016 From the Japan Pancreas Society: A Synopsis. Pancreas 2017, 46, 595–604. [Google Scholar] [CrossRef] [PubMed]
- Hanada, K.; Okazaki, A.; Hirano, N.; Izumi, Y.; Teraoka, Y.; Ikemoto, J.; Kanemitsu, K.; Hino, F.; Fukuda, T.; Yonehara, S. Diagnostic strategies for early pancreatic cancer. J. Gastroenterol. 2015, 50, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Seki, M.; Ninomiya, E.; Takano, K.; Fujita, R.; Aruga, A.; Yamada, K.; Tanaka, H.; Matsueda, K.; Mikami, K.; Hiki, N.; et al. Pancreatogram findings for carcinoma in situ (CIS) of the pancreas seen on endoscopic retrograde cholangiopancreatography and postoperative pancreatography of resected specimens: Can CIS be diagnosed preoperatively? Pancreatology 2008, 8, 142–152. [Google Scholar] [CrossRef] [PubMed]
- Kikuyama, M.; Hanada, K.; Ueki, T. Pancreatic carcinoma in situ presenting prominent fatty change of the pancreatic body on CT: experiences from 3 cases. Suizo 2015, 30, 626–632, (In Japanese with English Abstract). [Google Scholar] [CrossRef]
- Ikeda, M.; Yanagisawa, A.; Seki, M.; Sasaki, K.; Takano, K.; Kato, Y. The early state of invasive pancreatic ductal adenocarcinomas. Characteristics of the low papillary type and flat type intraductal carcinoma. Pancreas 2006, 33, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Fukuhara, M.; Hanada, K.; Yano, S.; Mori, H.; Maruyama, H.; Shimizu, A.; Minami, T.; Hirano, N.; Amano, H.; Abe, T.; et al. Comparison of flat type and low papillary type of pancreatic carcinoma in situ. Gastroenterology 2018, 154, S-521. [Google Scholar] [CrossRef]
- Athanassiadou, P.; Graspa, D. Value of endoscopic retrograde cholangiopancreatography-guided brushings in preoperavite assessment of pancreatobiliary stricture.: What’s new? Acta Cytol. 2008, 52, 24–34. [Google Scholar] [CrossRef] [PubMed]
- Shindo, H.; Fukasawa, M.; Takano, S.; Kadokura, M.; Takahashi, E.; Yokota, Y.; Hirose, S.; Sato, T.; Kawada, H.; Itakura, J.; et al. A case of carcinoma in situ of the pancreas concomitant with branch duct intraductal papillary mucinous neoplasm. Suizo 2014, 29, 742–748, (In Japanese with English Abstract). [Google Scholar] [CrossRef] [Green Version]
- Mikata, R.; Ishihara, T.; Tada, M.; Tawada, K.; Saito, M.; Kurosawa, J.; Sugiyama, H.; Sakai, Y.; Tsuyuguchi, T.; Miyazaki, M.; et al. Clinical usefulness of repeated pancreatic juice cytology via endoscopic naso-pancreatic drainage tube in patients with pancreatic cancer. J. Gastroenterol. 2013, 48, 866–873. [Google Scholar] [CrossRef] [PubMed]
- Maehira, H.; Sugiura, T.; Kanemoto, H.; Okamura, Y.; Itoh, T.; Kuribara, T.; Ashida, R.; Sasaki, K.; Uesaka, K. A case of carcinoma in situ of the pancreas with s surrounding fibrotic region. Suizo 2014, 29, 919–925, (In Japanese with English Abstract). [Google Scholar] [CrossRef]
- Ohtsubo, K.; Mouri, H.; Yamashita, K.; Makino, I.; Tajima, H.; Ohta, T.; Inoue, D.; Gabata, T.; Ikeda, H.; Zen, Y.; et al. Resection of carcinoma in situ and minimally invasive carcinoma of the pancreas in a patient presenting with stenosis and post-stenotic dilatation of the main pancreatic duct on endoscopic ultrasonography and positive serial pancreatic juice aspiration cytology. Nihon Shokakibyo Gakkai Zasshi 2017, 114, 700–709, (In Japanese with English Abstract). [Google Scholar] [PubMed]
- Kaneko, J.; Matsushita, M.; Tanaka, Y.; Nagasawa, M.; Ishibashi, K.; Watanabe, S.; Kanayama, H.; Morishita, M.; Ashizawa, N.; Kamimura, K.; et al. Evaluation of EUS and serial pancreatic juice aspiration cytological examination in a case of pancreatic carcinoma in situ. Suizo 2017, 32, 821–828, (In Japanese with English Abstract). [Google Scholar] [CrossRef]
- Minami, T.; Hanada, K.; Hirano, N.; Okazaki, A.; Ikemoto, J.; Fukuhara, M. Diagnosis of pancreatic cancer in situ. Suizo 2017, 32, 50–55, (In Japanese with English Abstract). [Google Scholar] [CrossRef]
- Kimura, K.; Furukawa, Y.; Yamasaki, S.; Kagawa, K.; Sakano, A.; Hananoki, M.; Kurushima, H.; Matsumoto, N.; Yamamoto, M.; Tsujita, E.; et al. A study of the usefullness of pancreatic juice cytology obtained via an endoscopic nasal pancreatic drainage (ENPD) tube. Nihon Shokakibyo Gakkai Zasshi 2011, 108, 928–936, (In Japanese with English Abstract). [Google Scholar] [PubMed]
- Mouri, T.; Sasaki, T.; Serikawa, M.; Ishigaki, T.; Ishii, Y.; Shimizu, A.; Tsuboi, T.; Kurihara, K.; Tatsukawa, Y.; Miyaki, E.; et al. A comparison of 4-Fr with 5-Fr endoscopic nasopancreatic drainage catheters: A randomized controlled trial. J. Gastroenterol. Hepatol. 2016, 31, 1783–1789. [Google Scholar] [CrossRef] [PubMed]
- Hanada, K. Fundamental technique and pitfalls of endoscopic transpapillary biopsy and cytology. Gastroenterol. Endosc. 2018, 60, 260–269, (In Japanese with English Abstract). [Google Scholar]
- Sasaki, K.; Sugiyama, K.; Koda, M.; Yonehara, S. Cytological differentiation of pancreatic intraepithelial neoplasia by cytologic diagnosis of pancreatic juice obtained by endoscopic nasopancreatic drainage. J. Jpn. Soc. Clin. Cytol. 2017, 56, 1–8, (In Japanese with English Abstract). [Google Scholar] [CrossRef]
- Yokode, M.; Akita, M.; Fujikura, K.; Kim, M.J.; Morinaga, Y.; Yoshikawa, S.; Terada, T.; Matsukiyo, H.; Tajiri, T.; Abe-Suzuki, S.; et al. High-grade PanIN presenting with localised stricture of the main pancreatic duct: A clinicopathological and molecular study of 10 cases suggests a clue for the early detection of pancreatic cancer. Histopathology 2018, 73, 247–258. [Google Scholar] [CrossRef] [PubMed]
- Hosoda, W.; Chianchiano, P.; Griffin, J.F.; Pittman, M.E.; Brosens, L.A.; Noë, M.; Yu, J.; Shindo, K.; Suenaga, M.; Rezaee, N.; et al. Genetic analysis of isolated high-grade pancreatic intraepithelial neoplasia (HG-PanIN) reveal paucity of alternations in TP53 and SMAD4. J. Pathol. 2017, 242, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Raimondo, M.; Guha, S.; Chen, J.; Diao, L.; Dong, X.; Wallace, M.B.; Killary, A.M.; Frazier, M.L.; Woodward, T.A.; et al. Circulating microRNAs in pancreatic juice as candidate biomarkers of pancreatic cancer. J. Cancer 2014, 5, 696–705. [Google Scholar] [CrossRef] [PubMed]
- Kisiel, J.B.; Raimomdo, M.; Taylor, W.R.; Yab, T.C.; Mahoney, D.W.; Sun, Z.; Middha, S.; Baheti, S.; Zou, H.; Smyrk, T.C.; et al. New DNA methylation markers for pancreatic cancer: discovery, tissue validation, and pilot testing in pancreatic juice. Clin Cancer Res. 2015, 21, 4473–4481. [Google Scholar] [CrossRef] [PubMed]
- Hata, T.; Ishida, M.; Motoi, F.; Yamaguchi, T.; Naitoh, T.; Katayose, Y.; Egawa, S.; Unno, M. Telomerase activity in pancreatic juice differentiates pancreatic cancer from chronic pancreatitis: a meta-analysis. Pancreatology 2016, 16, 372–381. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Modalities | Findings | All Cases (%) | Stage 0 (%) (n = 51) | Stage I (%) (n = 149) |
|---|---|---|---|---|
| US | 135/200 (67.5) | 34/51 (66.7) | 101/149 (67.8) | |
| Findings | MPD dilatation | 101/135 (74.8) | 26/34 (76.5) | 75/101 (74.3) |
| MPD stenosis | 27/135 (20) | 2/34 (5.9) | 25/101 (24.8) | |
| Tumors | 71/135 (52.6) | 3/34 (8.8) | 68/101 (67.3) | |
| CT | 196/200 (98) | 50/51 (98) | 146/149 (98) | |
| Findings | MPD dilatation | 156/196 (79.6) | 36/50 (72) | 120/146 (82.2) |
| Tumor | 101/196 (51.5) | 5/50 (10) | 96/146 (65.8) | |
| Focal fatty changes | 82/196 (41.8) | 21/50 (42) | 61/146 (41.8) | |
| MRI | 173/200 (86.5) | 46/51 (90.2) | 127/149 (85.2) | |
| Findings | MPD dilatation | 143/173 (82.7) | 34/46 (73.9) | 109/127 (85.8) |
| Tumor | 78/173 (45.1) | 5/46 (10.9) | 73/127 (57.5) | |
| EUS | 173/200 (86.5) | 41/51 (80.4) | 132/149 (88.6) | |
| Findings | MPD dilatation | 153/173 (88.4) | 35/41 (85.4) | 118/132 (89.4) |
| MPD stenosis | 98/173 (56.6) | 28/41 (68.3) | 70/132 (53) | |
| Tumor | 132/173 (76.3) | 10/41 (24.4) | 122/132 (92.4) | |
| ERCP | 141/200 (70.5) | 47/51 (92.2) | 94/149 (63.1) | |
| Findings | MPD dilatation | 114/141 (80.9) | 39/47 (83) | 75/94 (79.8) |
| MPD stenosis | 112/141 (79.4) | 39/47 (83) | 73/94 (77.7) | |
| FDG-PET | 61/200 (30.5) | 11/51 (21.6) | 50/149 (33.6) | |
| FDG accumulation | 31/61 (50.8) | 1/11 (9.1) | 30/50 (60) |
| Cytology | All Cases (n = 200) | Stage 0 (n = 51) | Stage I (n = 149) | |
|---|---|---|---|---|
| Cytology by ERCP | 79/141 (56) | 36/47 (77) | 48/94 (51) | |
| Confirmation of Malignancy | Brush | 30/62 (48) | 6/14 (43) | 24/43 (56) |
| ENPD | 55/79 (70) | 26/36 (72) | 29/48 (60) | |
| Cytology by EUS-FNA | 69/200 (35) | 6/51 (12) | 63/149 (42) | |
| Confirmation of Malignancy | 54/69 (78) | 1/6 (17) | 53/63 (84) |
| Authors/Years | Number of Cases | Depiction of Tumor | MPD Findings | Methods of Collection of Pancreatic Juice | Number of Collection of Pancreatic Juice | Pathological Stage |
|---|---|---|---|---|---|---|
| Kimura et al. 2011 [26] | 3 | No | Stenosis and distal dilatation | ENPD | 3 | PCIS |
| Iiboshi et al. 2012 [11] | 7 | No | Stenosis and dilatation | ENPD | 6 | PCIS |
| Mikata et al. 2013 [21] | 2 | No | Stenosis and distal dilatation | ENPD | 6 | PCIS |
| Shindo et al. 2014 [20] | 1 | No | Stenosis and distal dilatation | ERCP brushing and ENPD | 4 | PCIS |
| Maehira et al. 2014 [22] | 1 | No | Stenosis and distal dilatation | ERCP brushing and ENPD | 2 | PCIS |
| Kikuyama et al. 2015 [16] | 2 | No | Stenosis and dilatation | ENPD | 6 | PCIS |
| Ohtsubo et al. 2017 [23] | 1 | No | Stenosis and distal dilatation | ENPD | 6 | PCIS and minimally invasion |
| Kaneko et al. 2017 [24] | 1 | No | Stenosis and distal dilatation | ENPD | 6 | PCIS |
| Minami et al. 2017 [25] | 11 | No | Stenosis and distal dilatation | ENPD | 6 | PCIS |
| Miyata et al. 2017 [10] | 1 | No | Stenosis and distal dilatation | ENPD | 6 | PCIS |
| Sato et al. 2017 [12] | 1 | No | Stenosis and distal dilatation | ENPD | 6 | PCIS |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hanada, K.; Minami, T.; Shimizu, A.; Fukuhara, M.; Yano, S.; Sasaki, K.; Koda, M.; Sugiyama, K.; Yonehara, S.; Yanagisawa, A. Roles of ERCP in the Early Diagnosis of Pancreatic Cancer. Diagnostics 2019, 9, 30. https://doi.org/10.3390/diagnostics9010030
Hanada K, Minami T, Shimizu A, Fukuhara M, Yano S, Sasaki K, Koda M, Sugiyama K, Yonehara S, Yanagisawa A. Roles of ERCP in the Early Diagnosis of Pancreatic Cancer. Diagnostics. 2019; 9(1):30. https://doi.org/10.3390/diagnostics9010030
Chicago/Turabian StyleHanada, Keiji, Tomoyuki Minami, Akinori Shimizu, Motomitsu Fukuhara, Shigeki Yano, Kenji Sasaki, Masanori Koda, Kayo Sugiyama, Shuji Yonehara, and Akio Yanagisawa. 2019. "Roles of ERCP in the Early Diagnosis of Pancreatic Cancer" Diagnostics 9, no. 1: 30. https://doi.org/10.3390/diagnostics9010030