Advances in Early Detection of Pancreatic Cancer

 ,
, 
Abstract
: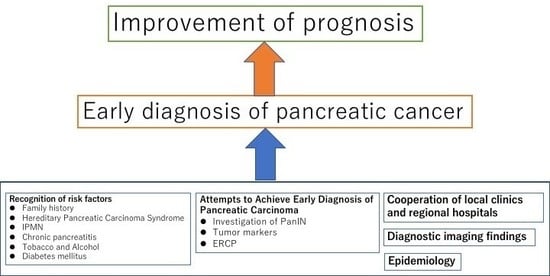
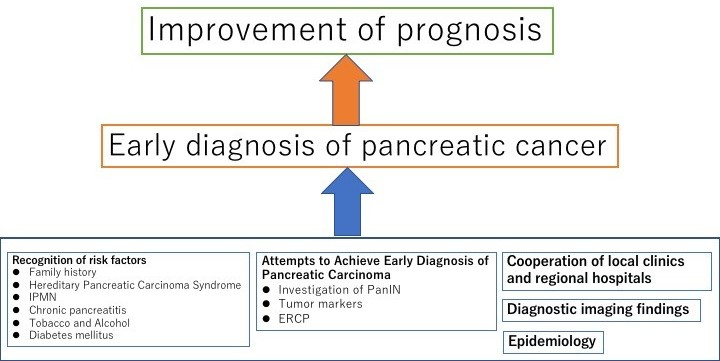
1. Introduction
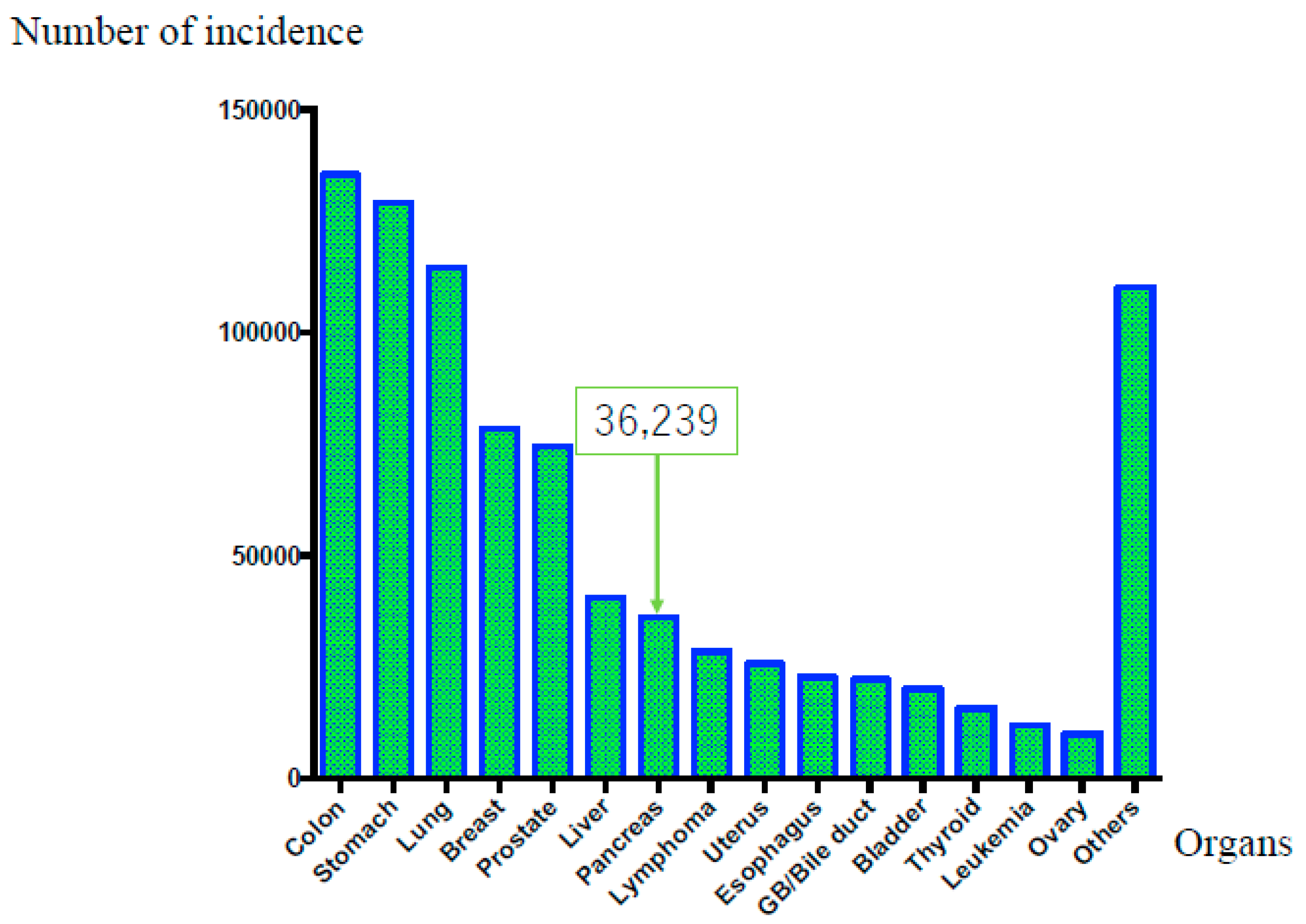
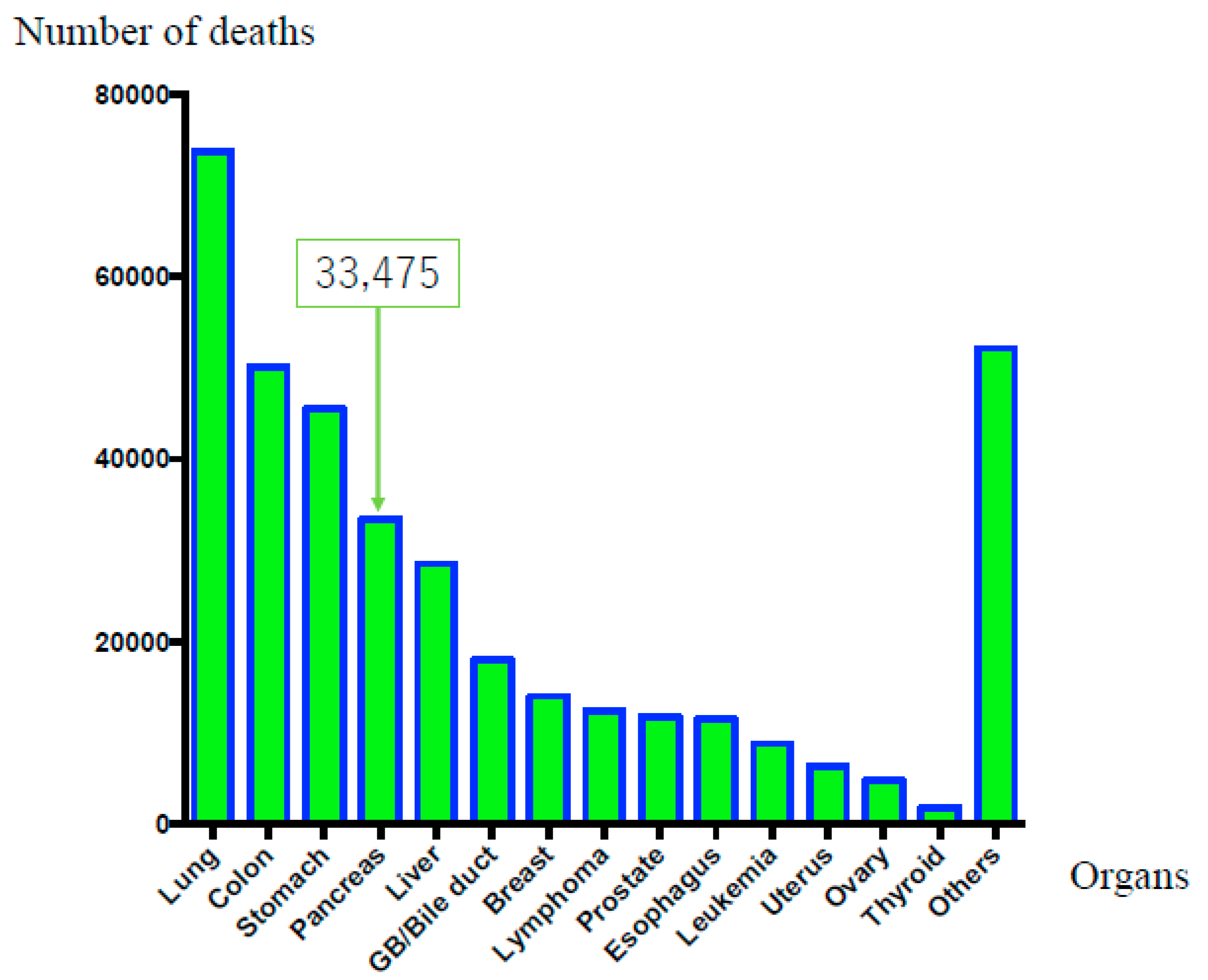
2. Epidemiology
3. Risk Factors
3.1. Family History or Hereditary Pancreatic Carcinoma Syndrome
3.2. IPMN
3.3. Chronic Pancreatitis
3.4. Tobacco and Alcohol
3.5. Diabetes Mellitus
4. Attempts to Achieve Early Diagnosis of Pancreatic Carcinoma
4.1. PanIN
4.2. microRNA and Cancer-Derived Exosomes
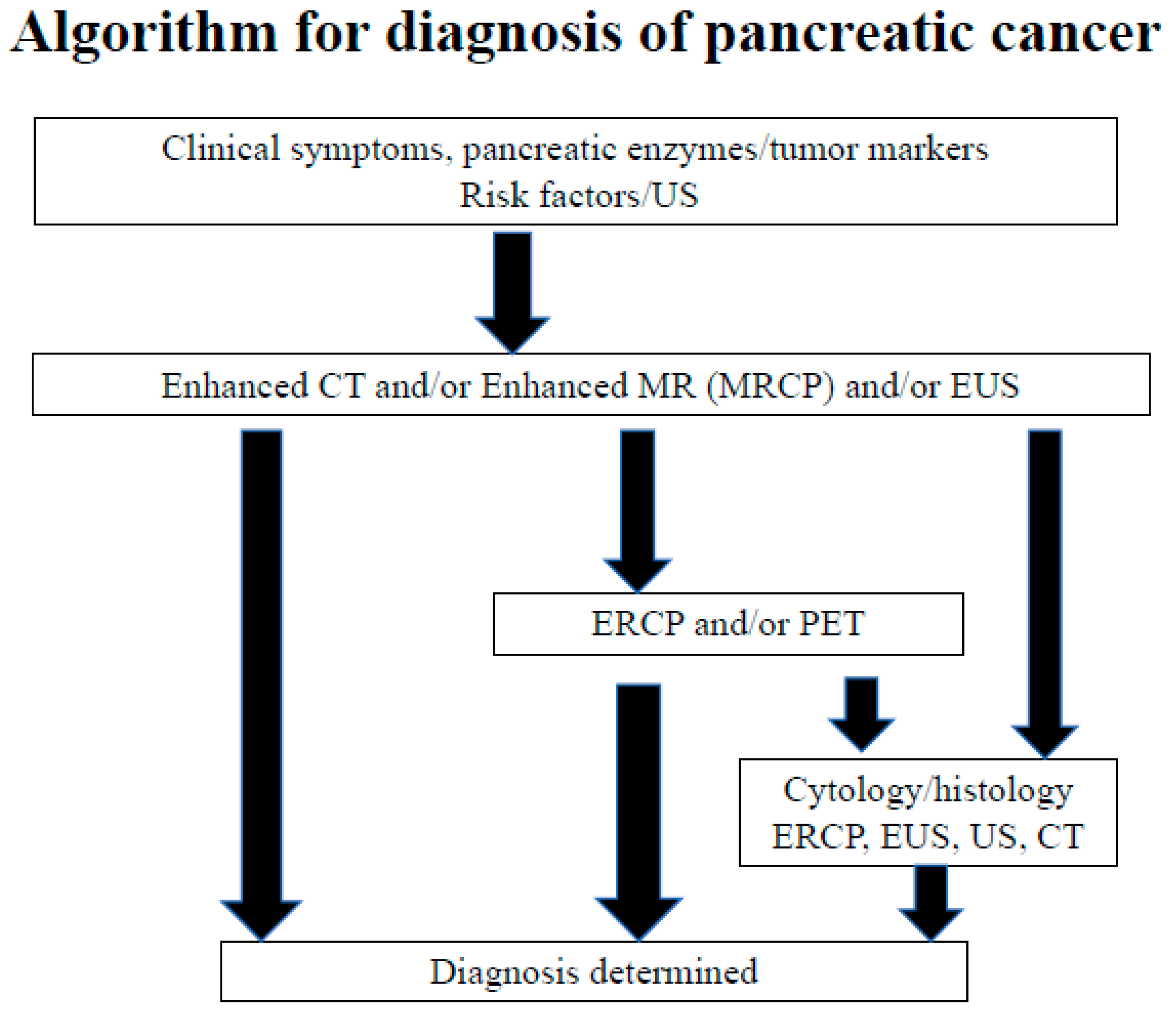
4.3. Hematological and Biochemical Tests and Tumor Markers
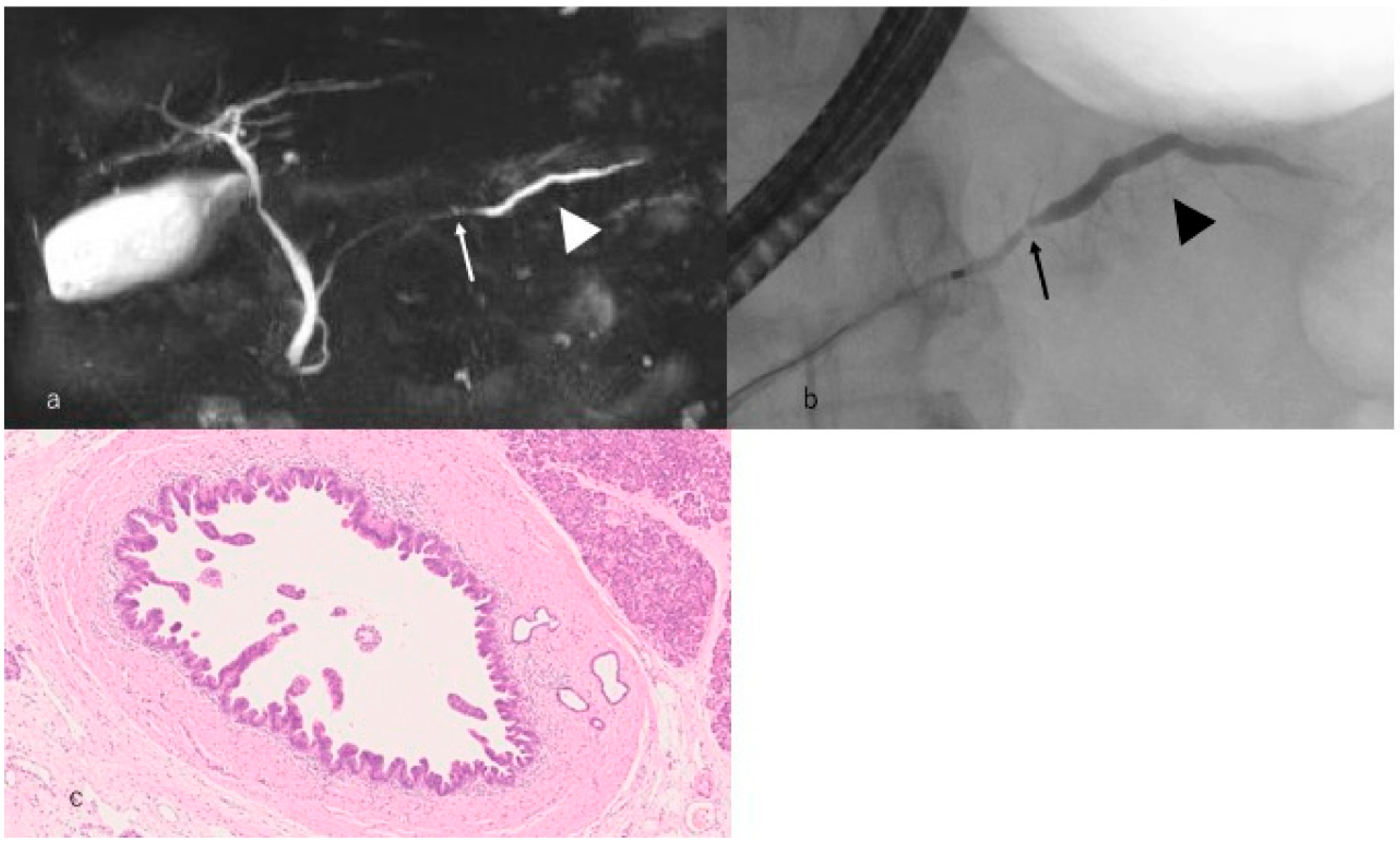
4.4. Importance of Endoscopic Retrograde Cholangiopancreatography (ERCP) for Early Diagnosis of Pancreatic Carcinoma
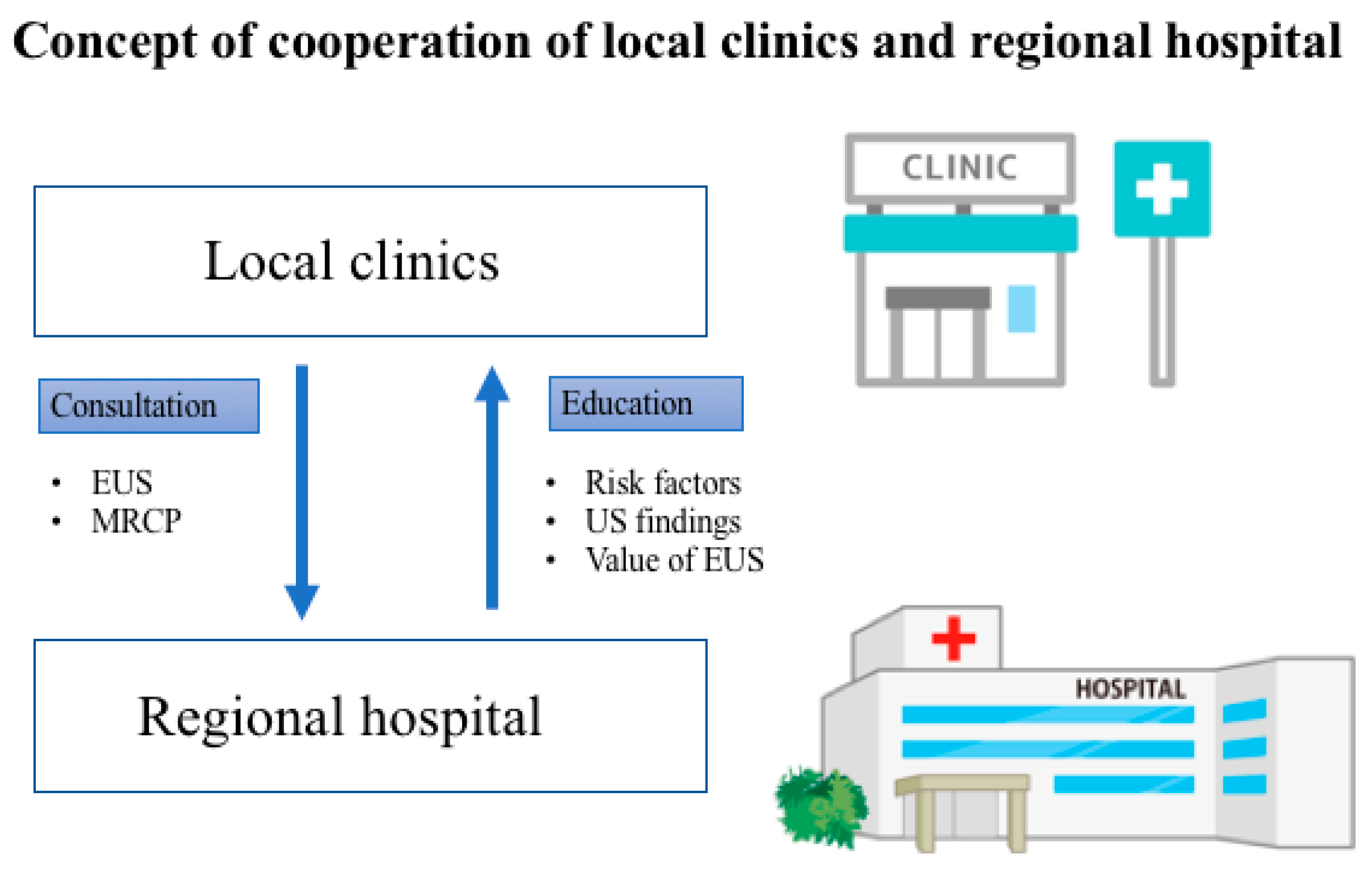
4.5. Cooperation of Local Clinics and Regional Hospitals
4.6. Japan Study Group on the Early Detection of Pancreatic Cancer (JEDPAC)
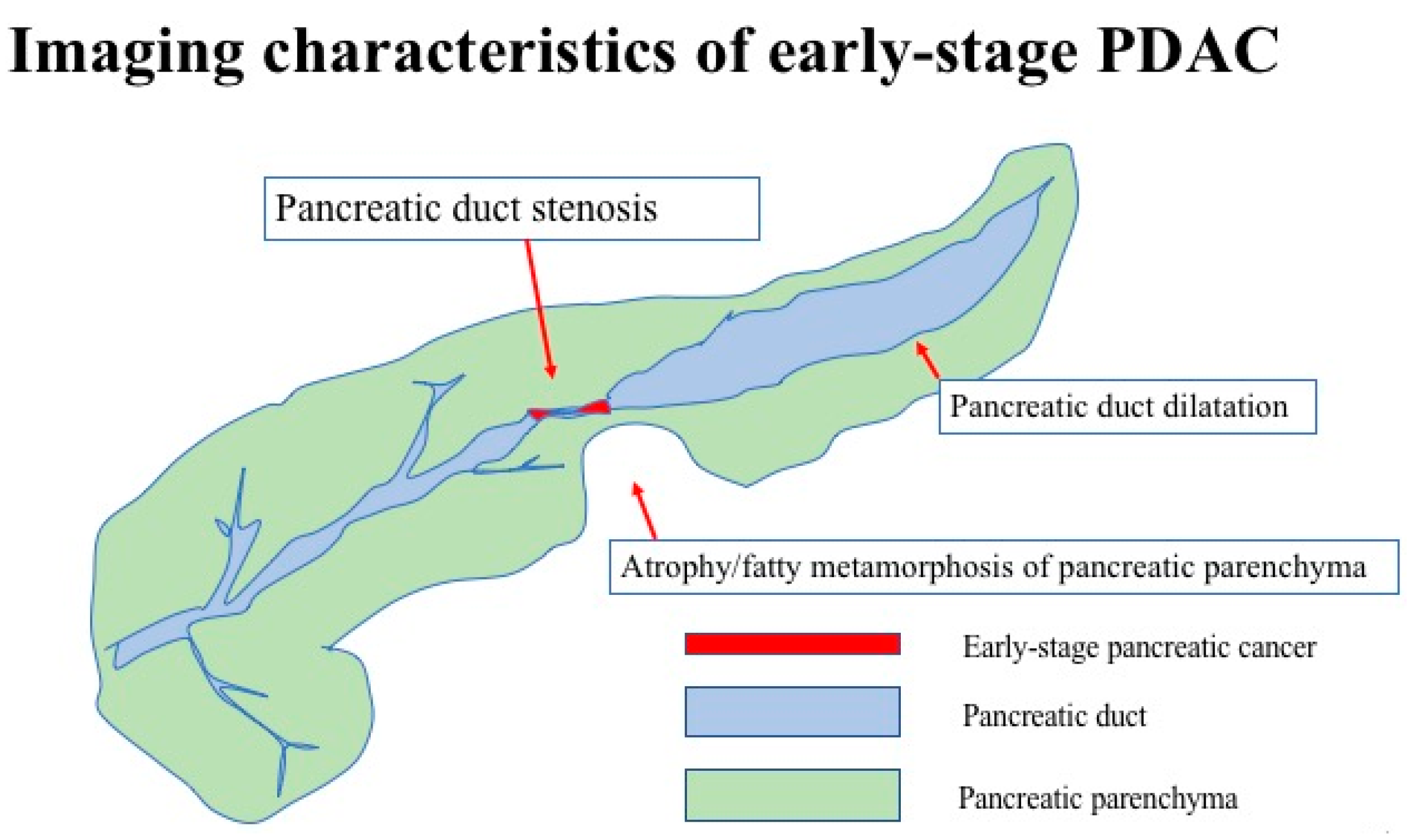
5. Current Status of Pancreatic Carcinoma Diagnosed in the Early Stages
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| CT | computed tomography |
| DM | diabetes mellitus |
| ENPD | endoscopic nasopancreatic duct drainage |
| ERCP | endoscopic retrograde cholangiopancreatography |
| EUS | endoscopic ultrasonography |
| FNA | fine needle aspiration |
| IPMN | intraductal papillary mucinous neoplasm |
| MRI | magnetic resonance imaging |
| PDAC | pancreatic ductal adenocarcinoma |
| US | ultrasonography |
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2018. CA Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Pourhoseingholi, M.A.; Ashtari, S.; Hajizadeh, N.; Fazeli, Z.; Zali, M.R. Systematic review of pancreatic cancer epidemiology in Asia-Pacific Region: Major patterns in GLOBACON 2012. Gastroenterol. Hepatol. Bed Bench 2017, 10, 245–257. [Google Scholar] [PubMed]
- Ministry of Health, Labour and Welfare. Available online: http://www.mhlw.go.jp/toukei/saikin/hw/jinkou/suikei15/ (accessed on 10 January 2019).
- Japanese Association of Clinical Cancer Centers. Available online: http://www.gunma-cc.jp/sarukihan/seizonritu/seizonritu2007.html (accessed on 10 January 2019).
- Egawa, S.; Toma, H.; Ohigashi, H.; Okusaka, T.; Hatori, T.; Maguchi, H.; Yanagisawa, A.; Tanaka, M. Japan Pancreatic Cancer Registry; 30th year anniversary: Japan Pancreas Society. Pancreas 2012, 41, 985–992. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, K.; Okusaka, T.; Shimizu, K.; Furuse, J.; Ito, Y.; Hanada, K.; Shimosegawa, T.; Okazaki, K. Clinical Practice Guidelines for Pancr Committee for Revision of Clinical Guidelines for Pancreatic Cancer of the Japan Pancreas Society. eatic Cancer 2016 From the Japan Pancreas Society: A Synopsis. Pancreas 2017, 46, 595–604. [Google Scholar] [CrossRef] [PubMed]
- Permuth-Wey, J.; Egan, K.M. Family history is a significant risk factor for pancreatic cancer: Results from a systematic review and meta-analysis. Fam. Cancer 2009, 8, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Klein, A.P.; Brune, K.A.; Petersen, G.M.; Goggins, M.; Tersmette, A.C.; Offerhaus, G.J.; Griffin, C.; Cameron, J.L.; Yeo, C.J.; Kern, S.; et al. Prospective risk of pancreatic cancer in familial pancreatic cancer kindreds. Cancer Res. 2004, 64, 2634–2638. [Google Scholar] [CrossRef] [PubMed]
- Shi, C.; Hruban, R.H.; Klein, A.P. Familial pancreatic cancer. Arch. Pathol. Lab. Med. 2009, 133, 365–374. [Google Scholar] [PubMed]
- Canto, M.I.; Hruban, R.H.; Fishman, E.K.; Kamel, I.R.; Schulick, R.; Zhang, Z.; Topazian, M.; Takahashi, N.; Fletcher, J.; Petersen, G.; et al. Frequent detection of pancreatic lesions in asymptomatic high-risk individuals. Gastroenterology 2012, 142, 796–804. [Google Scholar] [CrossRef] [PubMed]
- Canto, M.I.; Almario, J.A.; Schulick, R.D.; Yeo, C.J.; Klein, A.; Blackford, A.; Shin, E.J.; Sanyal, A.; Yenokyan, G.; Lennon, A.M. Risk of Neoplastic Progression in Individuals at High Risk for Pancreatic Cancer Undergoing Long-term Surveillance. Gastroenterology 2018, 155, 740–751. [Google Scholar] [CrossRef] [PubMed]
- Harinck, F.; Konings, I.C.; Kluijt, I.; Kluijt, I.; Poley, J.W.; van Hooft, J.E.; van Dullemen, H.M.; Nio, C.Y.; Krak, N.C.; Hermans, J.J.; et al. A multicentre comparative prospective blinded analysis of EUS and MRI for screening of pancreatic cancer in high-risk individuals. Gut 2016, 65, 1505–1513. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, M. Intraductal Papillary Mucinous Neoplasm of the Pancreas as the Main Focus for Early Detection of Pancreatic Adenocarcinoma. Pancreas 2018, 47, 544–550. [Google Scholar] [CrossRef] [PubMed]
- Kamata, K.; Kitano, M.; Kudo, M.; Sakamoto, H.; Kadosaka, K.; Miyata, T.; Imai, H.; Maekawa, K.; Chikugo, T.; Kumano, M.; et al. Value of EUS in early detection of pancreatic ductal adenocarcinomas in patients with intraductal papillary mucinous neoplasms. Endoscopy 2014, 46, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Ueda, J.; Tanaka, M.; Ohtsuka, T.; Tokunaga, S.; Shimosegawa, T.; Research Committee of Intractable Diseases of the Pancreas. Surgery for chronic pancreatitis decreases the risk for pancreatic cancer: A multicenter retrospective analysis. Surgery 2013, 153, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Shimosegawa, T.; Kataoka, K.; Kamisawa, T.; Miyakawa, H.; Ohara, H.; Ito, T.; Naruse, S.; Sata, N.; Suda, K.; Hirota, M.; et al. The revised Japanese clinical diagnostic criteria for chronic pancreatitis. J. Gastroenterol. 2010, 45, 584–591. [Google Scholar] [CrossRef] [PubMed]
- Sarner, M.; Cotton, P.B. Classification of pancreatitis. Gut 1984, 25, 756–759. [Google Scholar] [CrossRef] [PubMed]
- Catalano, M.F.; Sahai, A.; Levy, M.; Romagnuolo, J.; Wiersema, M.; Brugge, W.; Freeman, M.; Yamao, K.; Canto, M.; Hernandez, L.V. EUS-based criteria for the diagnosis of chronic pancreatitis: The Rosemont classification. Gastrointest. Endosc. 2009, 69, 1251–1261. [Google Scholar] [CrossRef] [PubMed]
- Rashid, S.; Singh, N.; Gupta, S.; Rashid, S.; Nalika, N.; Sachdev, V.; Bal, C.S.; Datta Gupta, S.; Chauhan, S.S.; Saraya, A. Progression of Chronic Pancreatitis to Pancreatic Cancer: Is There a Role of Gene Mutations as a Screening Tool? Pancreas 2018, 47, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Korc, M.; Jeon, C.Y.; Edderkaoui, M.; Pandol, S.J.; Petrov, M.S. Consortium for the Study of Chronic Pancreatitis, Diabetes, and Pancreatic Cancer (CPDPC). Tobacco and alcohol as risk factors for pancreatic cancer. Best Pract. Res. Clin. Gastroenterol. 2017, 31, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Illés, D.; Terzin, V.; Holzinger, G.; Kosár, K.; Róka, R.; Zsóri, G.; Ábrahám, G.; Czakó, L. New-onset type 2 diabetes mellitus—A high-risk group suitable for the screening of pancreatic cancer? Pancreatology 2016, 16, 266–271. [Google Scholar] [CrossRef] [PubMed]
- Khadka, R.; Tian, W.; Hao, X.; Koirala, R. Risk factor, early diagnosis and overall survival on outcome of association between pancreatic cancer and diabetes mellitus: Changes and advances, a review. Int. J. Surg. 2018, 52, 342–346. [Google Scholar] [CrossRef] [PubMed]
- Ben, Q.; Xu, M.; Ning, X.; Liu, J.; Hong, S.; Huang, W.; Zhang, H.; Li, Z. Diabetes mellitus and risk of pancreatic cancer: A meta-analysis of cohort studies. Eur. J. Cancer 2011, 47, 1928–1937. [Google Scholar] [CrossRef] [PubMed]
- Maitra, A.; Sharma, A.; Brand, R.E.; Van Den Eeden, S.K.; Fisher, W.E.; Hart, P.A.; Hughes, S.J.; Mather, K.J.; Pandol, S.J.; Park, W.G.; et al. A Prospective Study to Establish a New-Onset Diabetes Cohort: From the Consortium for the Study of Chronic Pancreatitis, Diabetes, and Pancreatic Cancer. Pancreas 2018, 47, 1244–1248. [Google Scholar] [CrossRef] [PubMed]
- Iiboshi, T.; Hanada, K.; Fukuda, T.; Yonehara, S.; Sasaki, T.; Chayama, K. Value of cytodiagnosis using endoscopic nasopancreatic drainage for early diagnosis of pancreatic cancer: Establishing a new method for the early detection of pancreatic carcinoma in situ. Pancreas 2012, 41, 523–529. [Google Scholar] [CrossRef] [PubMed]
- Hanada, K.; Okazaki, A.; Hirano, N.; Izumi, Y.; Teraoka, Y.; Ikemoto, J.; Kanemitsu, K.; Hino, F.; Fukuda, T.; Yonehara, S. Diagnostic strategies for early pancreatic cancer. J. Gastroenterol. 2015, 50, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Okada, T.; Motoi, F.; Kanno, A.; Masamune, A.; Ishida, K.; Fujishima, F.; Rikiyama, T.; Katayose, Y.; Egawa, S.; Shimosegawa, T.; et al. Pancreatic intraepithelial neoplasia-3 with localized acute pancreatitis in the main pancreatic duct. Clin. J. Gastroenterol. 2013, 6, 164–168. [Google Scholar] [CrossRef] [PubMed]
- Kanno, A.; Masamune, A.; Hanada, K.; Maguchi, H.; Shimizu, Y.; Ueki, T.; Hasebe, O.; Ohtsuka, T.; Nakamura, M.; Takenaka, M.; et al. Multicenter study of early pancreatic cancer in Japan. Pancreatology 2018, 18, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.K.; Brand, R.E.; Mehla, K. MicroRNAs in pancreatic cancer metabolism. Nat. Rev. Gastroenterol. Hepatol. 2012, 9, 334–344. [Google Scholar] [CrossRef] [PubMed]
- Raposo, G.; Stoorvogel, W. Extracellular vesicles: Exosomes, microvesicles, and friends. J. Cell Biol. 2013, 200, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Madhavan, B.; Yue, S.; Galli, U.; Rana, S.; Gross, W.; Müller, M.; Giese, N.A.; Kalthoff, H.; Becker, T.; Büchler, M.W.; et al. Combined evaluation of a panel of protein and miRNA serum-exosome biomarkers for pancreatic cancer diagnosis increases sensitivity and specificity. Int. J. Cancer 2015, 136, 2616–2627. [Google Scholar] [CrossRef] [PubMed]
- Lin, A.; Feller, E.R. Pancreatic carcinoma as a cause of unexplained pancreatitis: Report of ten cases. Ann. Intern. Med. 1990, 113, 166–167. [Google Scholar] [CrossRef] [PubMed]
- Hansson, G.C.; Karlsson, K.A.; Larson, G.; McKibbin, J.M.; Blaszczyk, M.; Herlyn, M.; Steplewski, Z.; Koprowski, H. Mouse monoclonal antibodies against human cancer cell lines with specificities for blood group and related antigens. Characterization by antibody binding to glycosphingolipids in a chromatogram binding assay. J. Biol. Chem. 1983, 258, 4091–4097. [Google Scholar] [PubMed]
- Yamaguchi, T.; Shirai, Y.; Nakamura, N.; Sudo, K.; Nakamura, K.; Hironaka, S.; Hara, T.; Denda, T. Usefulness of brush cytology combined with pancreatic juice cytology in the diagnosis of pancreatic cancer: Significance of pancreatic juice cytology after brushing. Pancreas 2012, 41, 1225–1229. [Google Scholar] [CrossRef] [PubMed]
- Loperfido, S.; Angelini, G.; Benedetti, G.; Chilovi, F.; Costan, F.; De Berardinis, F.; De Bernardin, M.; Ederle, A.; Fina, P.; Fratton, A. Major early complications from diagnostic and therapeutic ERCP: A prospective multicenter study. Gastrointest. Endosc. 1998, 48, 1–10. [Google Scholar] [CrossRef]
- Mine, T.; Morizane, T.; Kawaguchi, Y.; Akashi, R.; Hanada, K.; Ito, T.; Kanno, A.; Kida, M.; Miyagawa, H.; Yamaguchi, T.; et al. Clinical practice guideline for post-ERCP pancreatitis. J. Gastroenterol. 2017, 52, 1013–1022. [Google Scholar] [CrossRef] [PubMed]
- Hanada, K.; Okazaki, A.; Hirano, N.; Izumi, Y.; Minami, T.; Ikemoto, J.; Kanemitsu, K.; Hino, F. Effective screening for early diagnosis of pancreatic cancer. Best Pract. Res. Clin. Gastroenterol. 2015, 29, 929–939. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Incidence and Mortality Rate of Pancreatic Cancer | Worldwide | Japan |
|---|---|---|
| Incidence rate (male/female) (/100,000) | 4.9/3.6 | 10.6/6.7 |
| Mortality rate(male/female) (/100,000) | 4.8/3.4 | 8.4/6.1 |
| Sex (Male/Female) | 111/89 |
| Age, mean ± SD (range), years | 68.8 ± 9.5 (38–88) |
| Stage (0/1), number of cases | 51/149 |
| Observation period, mean (range), days | 1240.8 (66–3635) |
| Location, head/body/tail, number of cases (%) | 86 (43.0)/103 (51.5)/11 (5.5) |
| Risk Factors (Including Overlapping Cases) | Number of Cases (%) |
|---|---|
| Diabetes | 64 (32.0) |
| Smoking | 62 (31.0) |
| Intraductal papillary mucinous neoplasm | 52 (26.0) |
| Heavy Alcohol consumption | 30 (15.0) |
| Chronic pancreatitis | 26 (13.0) |
| Obesity | 13 (6.5) |
| Family history of pancreatic carcinoma | 9 (4.5) |
| Diagnostic Imaging Modalities and Findings | Number of Patients (%) | |
|---|---|---|
| Abdominal ultrasound | 135/200 (67.5) | |
| Findings (some overlapping cases) | Pancreatic duct dilatation | 101/135 (74.8) |
| Pancreatic duct stenosis | 27/135 (20.0) | |
| Pancreatic tumors | 71/135 (52.6) | |
| Computed tomography | 196/200 (98.0) | |
| Findings (some overlapping cases) | Pancreatic duct dilatation | 156/196 (79.6) |
| Pancreatic tumors | 101/196 (51.5) | |
| Atrophy/fatty metamorphosis of pancreatic parenchyma | 82/196 (41.8) | |
| Magnetic resonance imaging | 173/200 (86.5) | |
| Findings (some overlapping cases) | Pancreatic duct dilatation | 143/173 (82.7) |
| Pancreatic tumors | 78/1733 (45.1) | |
| Endoscopic ultrasonography | 173/200 (86.5) | |
| Findings (some overlapping cases) | Pancreatic duct dilatation | 153/173 (88.4) |
| Pancreatic duct stenosis | 98/173 (56.6) | |
| Pancreatic tumors | 132/173 (76.3) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kanno, A.; Masamune, A.; Hanada, K.; Kikuyama, M.; Kitano, M. Advances in Early Detection of Pancreatic Cancer. Diagnostics 2019, 9, 18. https://doi.org/10.3390/diagnostics9010018
Kanno A, Masamune A, Hanada K, Kikuyama M, Kitano M. Advances in Early Detection of Pancreatic Cancer. Diagnostics. 2019; 9(1):18. https://doi.org/10.3390/diagnostics9010018
Chicago/Turabian StyleKanno, Atsushi, Atsushi Masamune, Keiji Hanada, Masataka Kikuyama, and Masayuki Kitano. 2019. "Advances in Early Detection of Pancreatic Cancer" Diagnostics 9, no. 1: 18. https://doi.org/10.3390/diagnostics9010018