
Comparison of Transient Elastography and Point Shear Wave Elastography for Analysis of Liver Stiffness: A Prospective Study
 , ,
, ,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Patients’ Characteristics
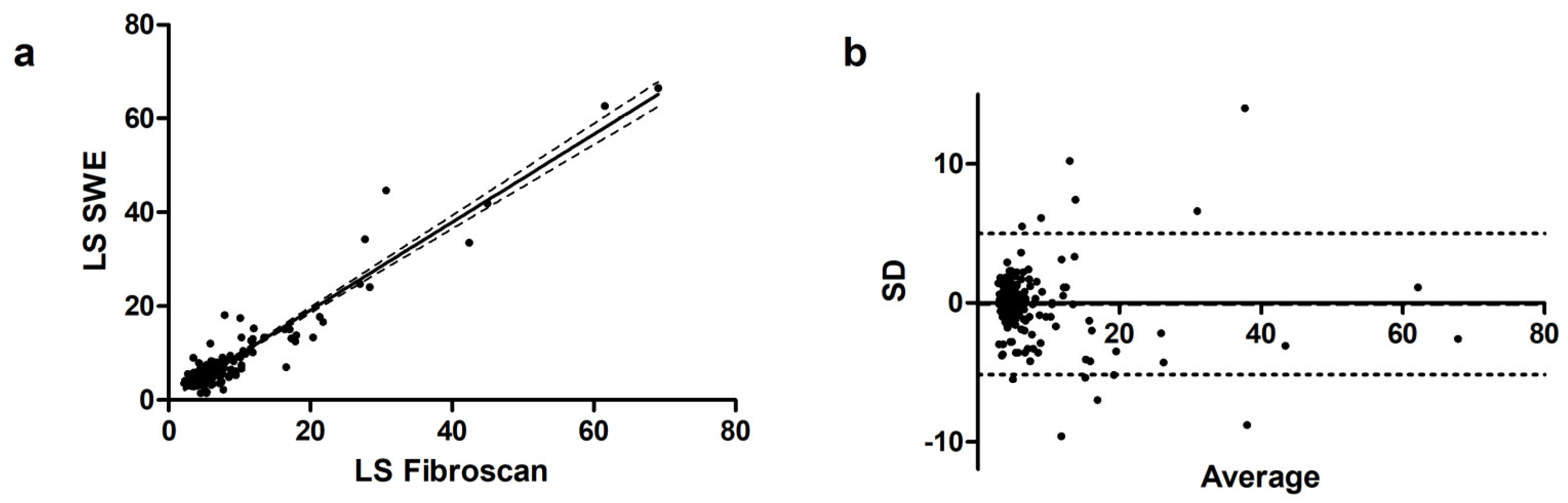
3.2. Overall Correlation
3.3. Sub-Analysis According to Liver Stiffness
3.4. Sub-Analysis According to Etiology
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Udompap, P.; Kim, D.; Kim, W.R. Current and Future Burden of Chronic Nonmalignant Liver Disease. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2015, 13, 2031–2041. [Google Scholar] [CrossRef] [PubMed]
- Horowitz, J.M.; Venkatesh, S.K.; Ehman, R.L.; Jhaveri, K.; Kamath, P.; Ohliger, M.A.; Samir, A.E.; Silva, A.C.; Taouli, B.; Torbenson, M.S.; et al. Evaluation of hepatic fibrosis: A review from the society of abdominal radiology disease focus panel. Abdom. Radiol. N. Y. 2017, 42, 2037–2053. [Google Scholar] [CrossRef]
- Castera, L. Invasive and non-invasive methods for the assessment of fibrosis and disease progression in chronic liver disease. Best Pract. Res. Clin. Gastroenterol. 2011, 25, 291–303. [Google Scholar] [CrossRef]
- Regev, A.; Berho, M.; Jeffers, L.J.; Milikowski, C.; Molina, E.G.; Pyrsopoulos, N.T.; Feng, Z.Z.; Reddy, K.R.; Schiff, E.R. Sampling error and intraobserver variation in liver biopsy in patients with chronic HCV infection. Am. J. Gastroenterol. 2002, 97, 2614–2618. [Google Scholar] [CrossRef] [PubMed]
- Bravo, A.A.; Sheth, S.G.; Chopra, S. Liver biopsy. N. Engl. J. Med. 2001, 344, 495–500. [Google Scholar] [CrossRef]
- Lupșor-Platon, M.; Badea, R.; Gersak, M.; Maniu, A.; Rusu, I.; Suciu, A.; Vicas, C.; Stefănescu, H.; Urs, R.; Al Hajjar, N. Noninvasive Assessment of Liver Diseases using 2D Shear Wave Elastography. J. Gastrointest. Liver Dis. JGLD 2016, 25, 525–532. [Google Scholar] [CrossRef]
- Ferraioli, G.; Filice, C.; Castera, L.; Choi, B.I.; Sporea, I.; Wilson, S.R.; Cosgrove, D.; Dietrich, C.F.; Amy, D.; Bamberet, J.C.; et al. WFUMB guidelines and recommendations for clinical use of ultrasound elastography: Part 3: Liver. Ultrasound Med. Biol. 2015, 41, 1161–1179. [Google Scholar] [CrossRef] [PubMed]
- de Lédinghen, V.; Vergniol, J. Transient elastography (FibroScan). Gastroenterol. Clin. Biol. 2008, 32, 58–67. [Google Scholar] [CrossRef]
- Ferraioli, G.; Wong, V.W.; Castera, L.; Berzigotti, A.; Sporea, I.; Dietrich, C.F.; Choi, B.I.; Wilson, S.R.; Kudo, M.; Barr, R.G. Liver Ultrasound Elastography: An Update to the World Federation for Ultrasound in Medicine and Biology Guidelines and Recommendations. Ultrasound Med. Biol. 2018, 44, 2419–2440. [Google Scholar] [CrossRef]
- Saadi, T.; Khoury, J.; Toukan, W.; Krimasky, R.; Veitsman, E.; Baruch, Y.; Gaitini, D.; Beck-Razi, N. Point Shear Wave Elastography for Assessing Liver Stiffness in Chronic Liver Diseases of Different Etiologies Compared to Biopsy. Isr. Med. Assoc. J. IMAJ 2021, 23, 223–228. [Google Scholar]
- Ferraioli, G.; Tinelli, C.; Lissandrin, R.; Zicchetti, M.; Dal Bello, B.; Filice, G.; Filice, C. Point shear wave elastography method for assessing liver stiffness. World J. Gastroenterol. 2014, 20, 4787–4796. [Google Scholar] [CrossRef]
- Ferraioli, G.; Tinelli, C.; Dal Bello, B.; Zicchetti, M.; Lissandrin, R.; Filice, G.; Filice, C.; Above, E.; Barbarini, G.; Brunetti, E.; et al. Performance of liver stiffness measurements by transient elastography in chronic hepatitis. World J. Gastroenterol. 2013, 19, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Barone, M.; Iannone, A.; Brunetti, N.D.; Sebastiani, F.; Cecere, O.; Berardi, E.; Antonica, G.; Di Leo, A. Liver stiffness and portal blood flow modifications induced by a liquid meal consumption: Pathogenetic mechanisms and clinical relevance. Scand. J. Gastroenterol. 2015, 50, 560–566. [Google Scholar] [CrossRef] [PubMed]
- Bedossa, P.; Poynard, T. An algorithm for the grading of activity in chronic hepatitis C. The METAVIR Cooperative Study Group. Hepatol. Baltim. Md 1996, 24, 289–293. [Google Scholar] [CrossRef]
- Pár, A.; Pár, G. The 43rd Annual Meeting of the European Association for the Study of the Liver (EASL), Milan, Italy (April 23–27, 2008). Orv. Hetil. 2008, 149, 1329–1332. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, C.F.; Bamber, J.; Berzigotti, A.; Bota, S.; Cantisani, V.; Castera, L.; Cosgrove, D.; Ferraioli, G.; Friedrich-Rust, M.; Gilja, O.H.; et al. EFSUMB Guidelines and Recommendations on the Clinical Use of Liver Ultrasound Elastography, Update 2017 (Long Version). Ultraschall Med. 2017, 38, e16–e47. [Google Scholar]
- De Franchis, R.; Bosch, J.; Garcia-Tsao, G.; Reiberger, T.; Ripoll, C.; Abraldes, J.G.; Albillos, A.; Baiges, A.; Bajaj, J.; Bañares, R.; et al. Baveno VII-Renewing consensus in portal hypertension. J. Hepatol. 2022, 76, 959–974. [Google Scholar] [CrossRef] [PubMed]
- Cassinotto, C.; Lapuyade, B.; Mouries, A.; Hiriart, J.B.; Vergniol, J.; Gaye, D.; Castain, C.; Le Bail, B.; Chermak, F.; Foucher, J.; et al. Non-invasive assessment of liver fibrosis with impulse elastography: Comparison of Supersonic Shear Imaging with ARFI and FibroScan®. J. Hepatol. 2014, 61, 550–557. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.J.; Lee, J.M.; Chang, W.; Lee, S.M.; Kang, H.J.; Yang, H.; Yoon, J.H.; Park, S.J.; Han, J.K. Prospective Validation of Intra- and Interobserver Reproducibility of a New Point Shear Wave Elastographic Technique for Assessing Liver Stiffness in Patients with Chronic Liver Disease. Korean J. Radiol. 2017, 18, 926–935. [Google Scholar] [CrossRef]
- Joo, I.; Kim, S.Y.; Park, H.S.; Kang, H.J.; Lee, J.M. Validation of a New Point Shear-Wave Elastography Method for Noninvasive Assessment of Liver Fibrosis: A Prospective Multicenter Study. Korean J. Radiol. 2019, 20, 1527–1535. [Google Scholar] [CrossRef]
- European Association for Study of Liver & Asociacion Latinoamericana para el Estudio del Higado. EASL-ALEH Clinical Practice Guidelines: Non-invasive tests for evaluation of liver disease severity and prognosis. J. Hepatol. 2015, 63, 237–264. [Google Scholar] [CrossRef] [PubMed]
- Valente, G.; Rinaldi, L.; Moggio, G.; Piai, G. Point shear wave elastography and vibration controlled transient elastography for estimating liver fibrosis in a cohort of liver transplant patients. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 7357–7365. [Google Scholar] [CrossRef]
- Foncea, C.G.; Popescu, A.; Lupusoru, R.; Fofiu, R.; Sirli, R.; Danila, M.; Sporea, I. Comparative study between pSWE and 2D-SWE techniques integrated in the same ultrasound machine, with Transient Elastography as the reference method. Med. Ultrason. 2020, 22, 13–19. [Google Scholar] [CrossRef]
- Roccarina, D.; Iogna Prat, L.; Pallini, G.; Guerrero Misas, M.; Buzzetti, E.; Saffioti, F.; Aricò, F.M.; Mantovani, A.; Koutli, E.; Goyale, A.; et al. Comparison of point-shear wave elastography (ElastPQ) and transient elastography (FibroScan) for liver fibrosis staging in patients with non-alcoholic fatty liver disease. Liver Int. 2022, 42, 2195–2203. [Google Scholar] [CrossRef]
- Bamber, J.; Cosgrove, D.; Dietrich, C.F.; Fromageau, J.; Bojunga, J.; Calliada, F.; Cantisani, V.; Correas, J.M.; D’Onofrio, M.; Drakonaki, E.E.; et al. EFSUMB guidelines and recommendations on the clinical use of ultrasound elastography. Part 1: Basic principles and technology. Ultraschall Med. 2013, 34, 169–184. [Google Scholar] [CrossRef]
- Ozturk, A.; Olson, M.C.; Samir, A.E.; Venkatesh, S.K. Liver fibrosis assessment: MR and US elastography. Abdom. Radiol. 2022, 47, 3037–3050. [Google Scholar] [CrossRef] [PubMed]
- Park, C.C.; Nguyen, P.; Hernandez, C.; Bettencourt, R.; Ramirez, K.; Fortney, L.; Hooker, J.; Sy, E.; Savides, M.T.; Alquiraish, M.H.; et al. Magnetic Resonance Elastography vs. Transient Elastography in Detection of Fibrosis and Noninvasive Measurement of Steatosis in Patients with Biopsy-Proven Nonalcoholic Fatty Liver Disease. Gastroenterology 2017, 152, 598–607.e2. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Population characteristics | Mean ± SD or n (%) |
| Age | 56.9 ± 12.5 |
| Male/female ratio | 107/77 |
Liver disease etiology
| 29 (15.8%) 21 (11.4%) 61 (33.1%) 16 (8.7%) 11 (6.0%) 7 (3.8%) 18 (9.8%) 21 (11.4) |
| Median Stiffness Measured by | Correlation | Bias | ||||
|---|---|---|---|---|---|---|
| TE | pSWE | r | 95% CI | p | ||
| HBV | 4.3 | 4.9 | 0.67 | 0.39–0.84 | <0.001 | 0.21 |
| ALD | 8.7 | 9.5 | 0.99 | 0.91–0.99 | <0.001 | −1.18 |
| HCV | 6.8 | 6.7 | 0.91 | 0.77–0.96 | <0.001 | 1.12 |
| NASH | 5.2 | 5.6 | 0.62 | 0.43–0.76 | <0.001 | −0.57 |
| PBC/PSC | 4.85 | 5.0 | 0.72 | 0.31–0.89 | 0.002 | 0.45 |
| AIH | 4.9 | 4.6 | 0.50 | 0.10–0.78 | 0.11 | −0.24 |
| Hypertransaminasemia of unknown origin | 4.9 | 4.65 | 0.53 | 0.06–0.80 | 0.02 | 0.06 |
| Other causes | 5.7 | 5.3 | 0.67 | 0.33–0.86 | 0.008 | −0.53 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Losurdo, G.; Ditonno, I.; Novielli, D.; Celiberto, F.; Iannone, A.; Castellaneta, A.; Dell’Aquila, P.; Ranaldo, N.; Rendina, M.; Barone, M.; et al. Comparison of Transient Elastography and Point Shear Wave Elastography for Analysis of Liver Stiffness: A Prospective Study. Diagnostics 2024, 14, 604. https://doi.org/10.3390/diagnostics14060604
Losurdo G, Ditonno I, Novielli D, Celiberto F, Iannone A, Castellaneta A, Dell’Aquila P, Ranaldo N, Rendina M, Barone M, et al. Comparison of Transient Elastography and Point Shear Wave Elastography for Analysis of Liver Stiffness: A Prospective Study. Diagnostics. 2024; 14(6):604. https://doi.org/10.3390/diagnostics14060604
Chicago/Turabian StyleLosurdo, Giuseppe, Ilaria Ditonno, Domenico Novielli, Francesca Celiberto, Andrea Iannone, Antonino Castellaneta, Paola Dell’Aquila, Nunzio Ranaldo, Maria Rendina, Michele Barone, and et al. 2024. "Comparison of Transient Elastography and Point Shear Wave Elastography for Analysis of Liver Stiffness: A Prospective Study" Diagnostics 14, no. 6: 604. https://doi.org/10.3390/diagnostics14060604