
Performance Evaluation of the STANDARD i-Q COVID-19 Ag Test with Nasal and Oral Swab Specimens from Symptomatic Patients

Abstract
:1. Introduction
2. Materials and Methods
2.1. Samples
2.2. Procedure
2.3. Statistical Analysis
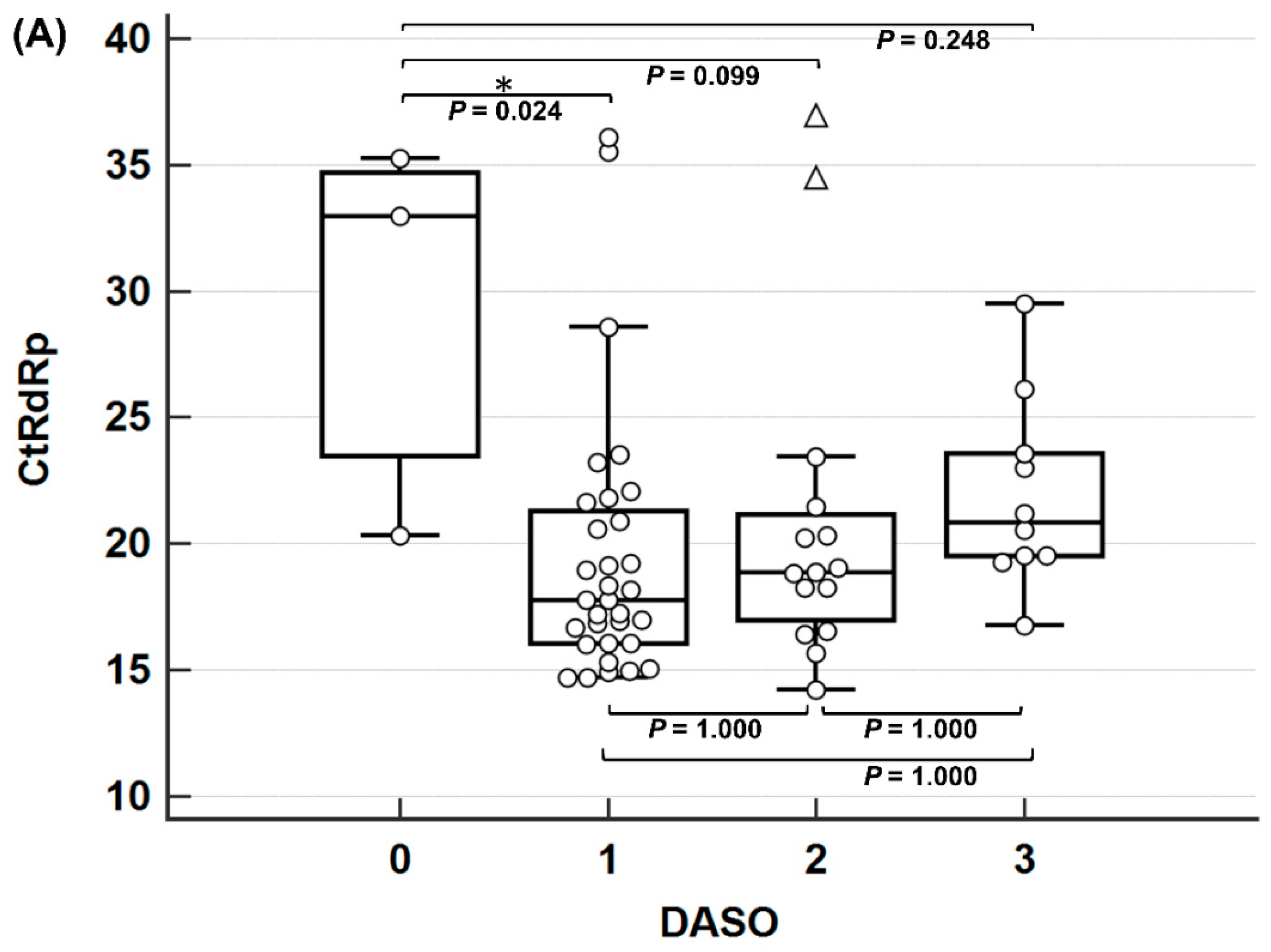
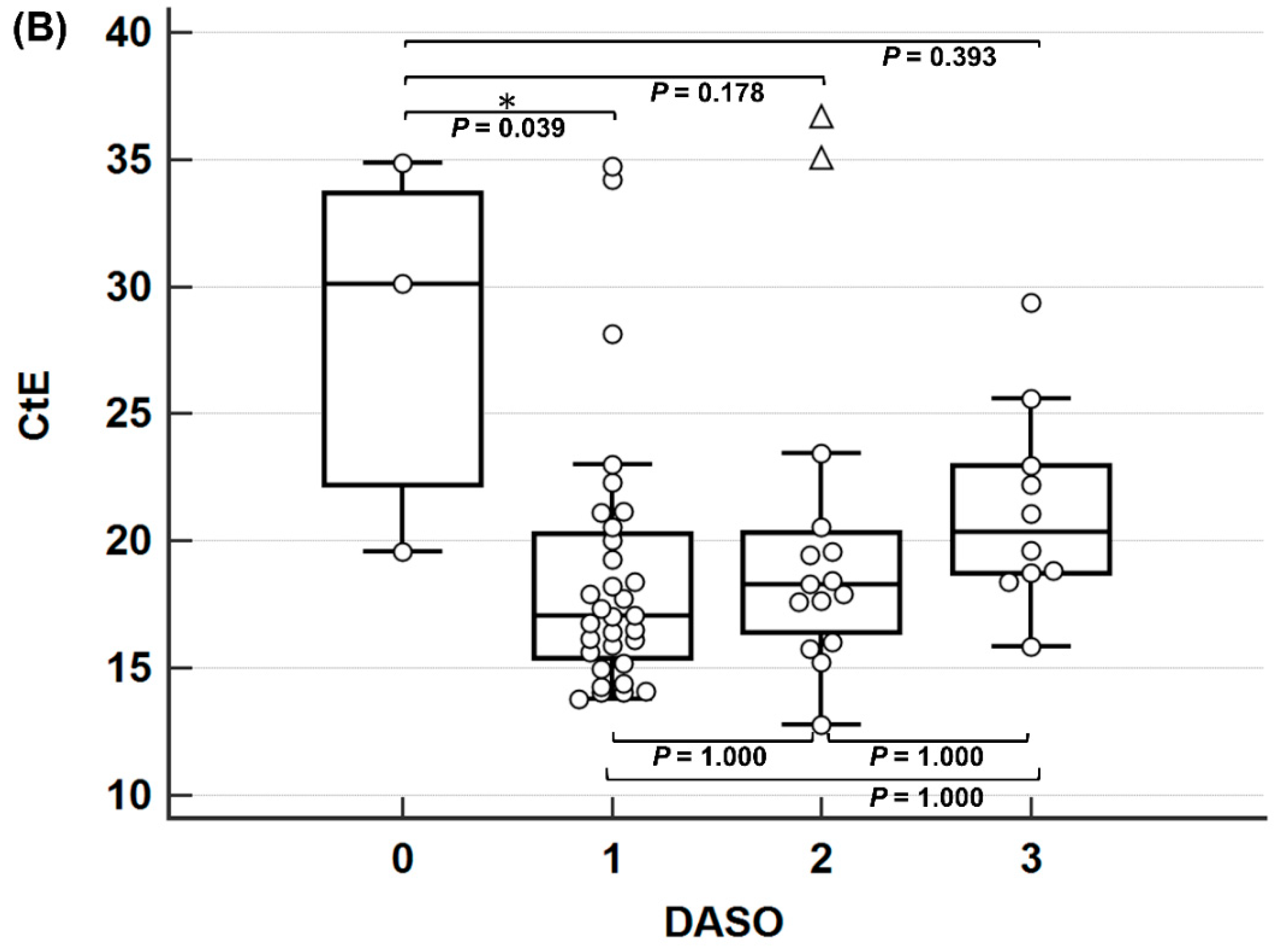
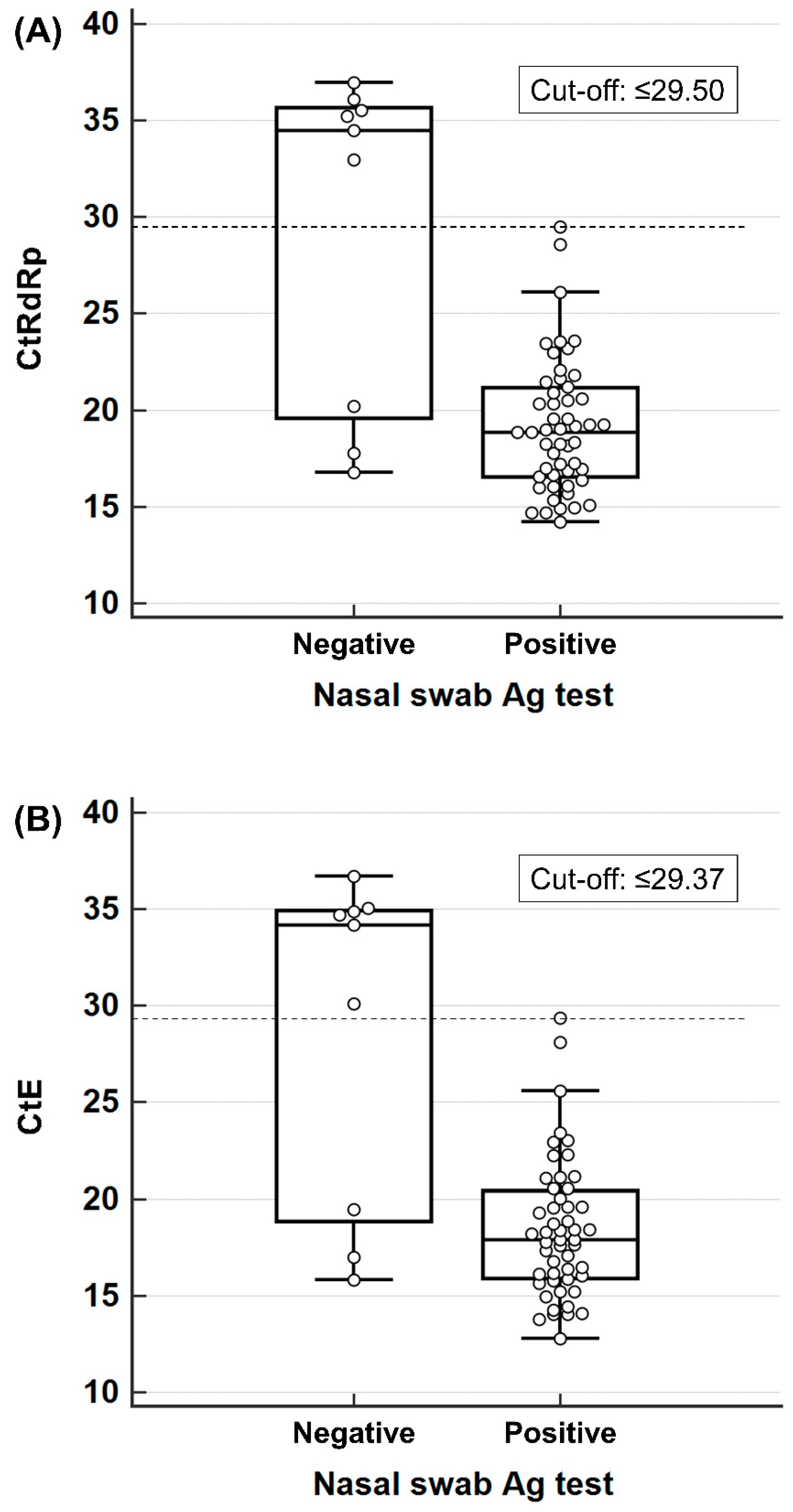
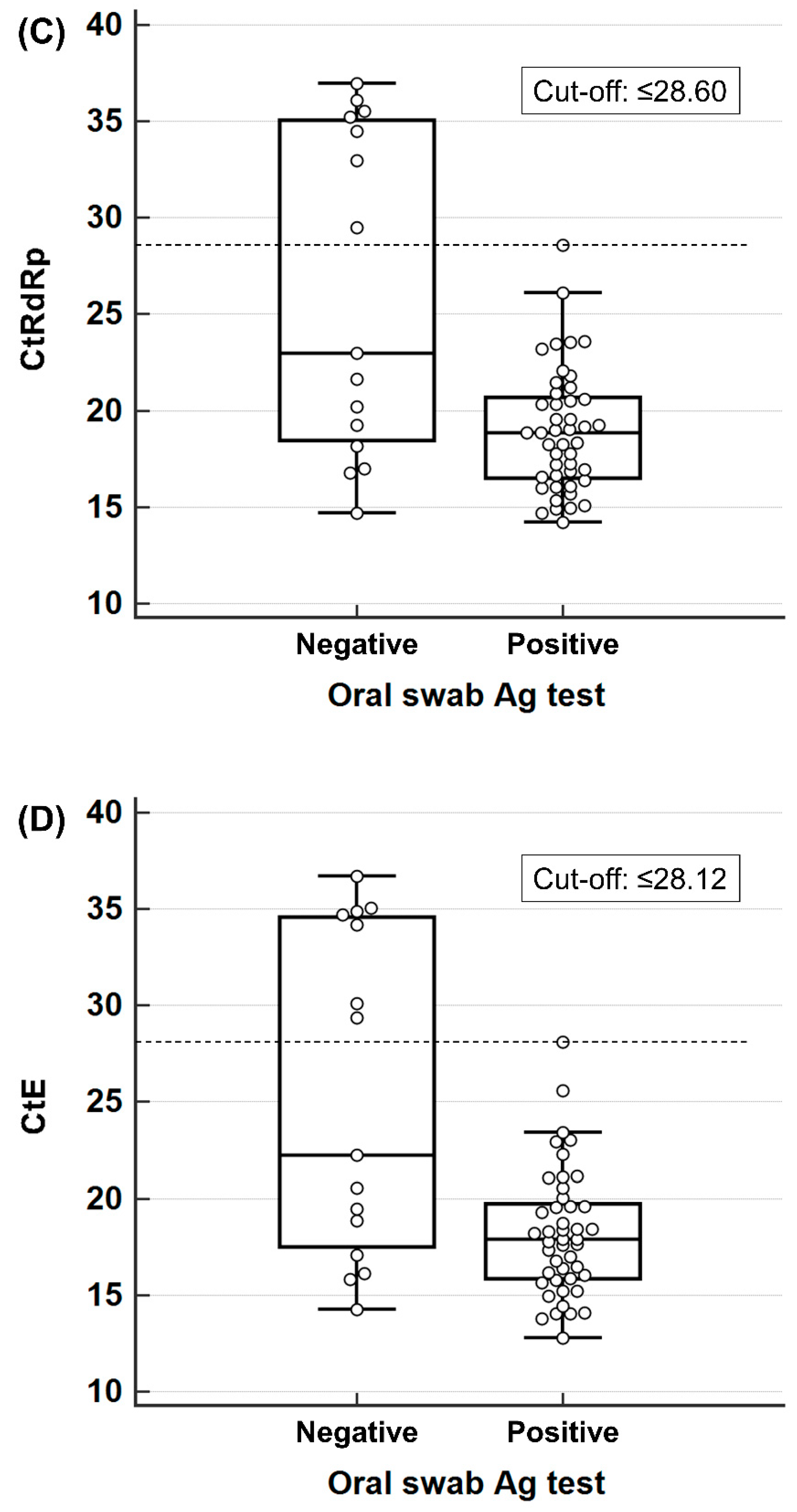
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Weekly Epidemiological Update on COVID-19, 141st ed.; World Health Organization: Geneva, Switzerland, 2023. [Google Scholar]
- National Institutes of Health. Testing for SARS-CoV-2 Infection. Available online: https://www.covid19treatmentguidelines.nih.gov/overview/sars-cov-2-testing/ (accessed on 8 May 2023).
- Centers for Disease Control and Prevention. Nucleic Acid Amplification Tests (NAATs). Available online: https://www.cdc.gov/coronavirus/2019-ncov/lab/naats.html (accessed on 3 May 2023).
- Roberts, A.; Chouhan, R.S.; Shahdeo, D.; Shrikrishna, N.S.; Kesarwani, V.; Horvat, M.; Gandhi, S. A Recent Update on Advanced Molecular Diagnostic Techniques for COVID-19 Pandemic: An Overview. Front. Immunol. 2021, 12, 732756. [Google Scholar] [CrossRef]
- Oh, S.M.; Lee, J.S.; Jo, H.J.; Kim, D.; Park, D.; Hwang, Y.H.; Choi, Y.; Lee, C.M.; Lee, S.; Chang, E.; et al. Clinical application of the Panbio COVID-19 Ag rapid test device and SSf-COVID19 kit for the detection of SARS-CoV-2 infection. BMC Res. Notes 2022, 15, 357. [Google Scholar] [CrossRef]
- Younes, N.; Al-Sadeq, D.W.; Al-Jighefee, H.; Younes, S.; Al-Jamal, O.; Daas, H.I.; Yassine, H.M.; Nasrallah, G.K. Challenges in Laboratory Diagnosis of the Novel Coronavirus SARS-CoV-2. Viruses 2020, 12, 582. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Guidance for Antigen Testing for SARS-CoV-2 for Healthcare Providers Testing Individuals in the Community. Available online: https://www.cdc.gov/coronavirus/2019-ncov/lab/resources/antigen-tests-guidelines.html (accessed on 29 April 2023).
- Hayden, M.K.; Hanson, K.E.; Englund, J.A.; Lee, F.; Lee, M.J.; Loeb, M.; Morgan, D.J.; Patel, R.; El Alayli, A.; El Mikati, I.K.; et al. The Infectious Diseases Society of America Guidelines on the Diagnosis of COVID-19: Antigen Testing. Clin. Infect. Dis. 2023, ciad032. [Google Scholar] [CrossRef]
- Cai, X.F.; Chen, J.; Li Hu, J.; Long, Q.X.; Deng, H.J.; Liu, P.; Fan, K.; Liao, P.; Liu, B.Z.; Wu, G.C.; et al. A Peptide-Based Magnetic Chemiluminescence Enzyme Immunoassay for Serological Diagnosis of Coronavirus Disease 2019. J. Infect. Dis. 2020, 222, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Yi, Y.; Luo, X.; Xiong, N.; Liu, Y.; Li, S.; Sun, R.; Wang, Y.; Hu, B.; Chen, W. Development and clinical application of a rapid IgM-IgG combined antibody test for SARS-CoV-2 infection diagnosis. J. Med. Virol. 2020, 92, 1518–1524. [Google Scholar] [CrossRef] [PubMed]
- Lassaunière, R.; Frische, A.; Harboe, Z.B.; Nielsen, A.C.; Fomsgaard, A.; Krogfelt, K.A.; Jørgensen, C.S. Evaluation of nine commercial SARS-CoV-2 immunoassays. medRxiv 2020. [Google Scholar] [CrossRef]
- Montesinos, I.; Gruson, D.; Kabamba, B.; Dahma, H.; Van den Wijngaert, S.; Reza, S.; Carbone, V.; Vandenberg, O.; Gulbis, B.; Wolff, F.; et al. Evaluation of two automated and three rapid lateral flow immunoassays for the detection of anti-SARS-CoV-2 antibodies. J. Clin. Virol. 2020, 128, 104413. [Google Scholar] [CrossRef] [PubMed]
- Yuce, M.; Filiztekin, E.; Ozkaya, K.G. COVID-19 diagnosis -A review of current methods. Biosens. Bioelectron. 2021, 172, 112752. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.-L.; Tseng, W.-P.; Lin, C.-H.; Lee, T.-F.; Chung, M.-Y.; Huang, C.-H.; Chen, S.-Y.; Hsueh, P.-R.; Chen, S.-C. Four point-of-care lateral flow immunoassays for diagnosis of COVID-19 and for assessing dynamics of antibody responses to SARS-CoV-2. J. Infect. 2020, 81, 435–442. [Google Scholar] [CrossRef] [PubMed]
- Mak, G.C.; Cheng, P.K.; Lau, S.S.; Wong, K.K.; Lau, C.; Lam, E.T.; Chan, R.C.; Tsang, D.N. Evaluation of rapid antigen test for detection of SARS-CoV-2 virus. J. Clin. Virol. 2020, 129, 104500. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Point-of-Care & Rapid Testing. Available online: https://www.cdc.gov/coronavirus/2019-ncov/lab/point-of-care-testing.html (accessed on 29 April 2023).
- World Health Organization. Antigen-Detection in the Diagnosis of SARS-CoV-2 Infection: Interim Guidance; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Korean Ministry of Food and Drug Safety. Guideline on the Review and Approval of In Vitro Diagnostic Devices for COVID-19. Available online: https://www.mfds.go.kr/eng/brd/m_40/view.do?seq=72625&srchFr=&srchTo=&srchWord=&srchTp=&itm_seq_1=0&itm_seq_2=0&multi_itm_seq=0&company_cd=&company_nm=&page=1 (accessed on 24 April 2023).
- Pray, I.W.; Ford, L.; Cole, D.; Lee, C.; Bigouette, J.P.; Abedi, G.R.; Bushman, D.; Delahoy, M.J.; Currie, D.; Cherney, B.; et al. Performance of an Antigen-Based Test for Asymptomatic and Symptomatic SARS-CoV-2 Testing at Two University Campuses—Wisconsin, September–October 2020. MMWR. Morb. Mortal. Wkly. Rep. 2021, 69, 1642–1647. [Google Scholar] [CrossRef] [PubMed]
- Pascarella, G.; Strumia, A.; Piliego, C.; Bruno, F.; Del Buono, R.; Costa, F.; Scarlata, S.; Agro, F.E. COVID-19 diagnosis and management: A comprehensive review. J. Intern. Med. 2020, 288, 192–206. [Google Scholar] [CrossRef] [PubMed]
- Parvu, V.; Gary, D.S.; Mann, J.; Lin, Y.-C.; Mills, D.; Cooper, L.; Andrews, J.C.; Manabe, Y.C.; Pekosz, A.; Cooper, C.K. Factors that influence the reported sensitivity of rapid antigen testing for SARS-CoV-2. Front. Microbiol. 2021, 12, 2611. [Google Scholar] [CrossRef] [PubMed]
- Berger, A.; Nsoga, M.T.N.; Perez-Rodriguez, F.J.; Aad, Y.A.; Sattonnet-Roche, P.; Gayet-Ageron, A.; Jaksic, C.; Torriani, G.; Boehm, E.; Kronig, I. Diagnostic accuracy of two commercial SARS-CoV-2 antigen-detecting rapid tests at the point of care in community-based testing centers. PLoS ONE 2021, 16, e0248921. [Google Scholar] [CrossRef] [PubMed]
- Jääskeläinen, A.; Ahava, M.J.; Jokela, P.; Szirovicza, L.; Pohjala, S.; Vapalahti, O.; Lappalainen, M.; Hepojoki, J.; Kurkela, S. Evaluation of three rapid lateral flow antigen detection tests for the diagnosis of SARS-CoV-2 infection. J. Clin. Virol. 2021, 137, 104785. [Google Scholar] [CrossRef] [PubMed]
- Ryu, H.; Oh, E.; Cha, K.; Kim, K.; Kim, S.; Minn, D. Clinical Evaluation of an Antigen Home Test Using Surface-Enhanced Raman Spectroscopy and Stacking Pad for SARS-CoV-2 Screening with Nasal and Salivary Swab Samples. Diagnostics 2023, 13, 880. [Google Scholar] [CrossRef]
- Jung, E.J.; Lee, S.K.; Shin, S.H.; Kim, J.S.; Woo, H.; Cho, E.J.; Hyun, J.; Kim, J.S.; Kim, H.S. Comparison of Nasal Swabs, Nasopharyngeal Swabs, and Saliva Samples for the Detection of SARS-CoV-2 and other Respiratory Virus Infections. Ann. Lab. Med. 2023, 43, 434–442. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PCR+ (n = 60) | PCR− (n = 100) | Sensitivity (95% CI) | Specificity (95% CI) | |||
|---|---|---|---|---|---|---|
| Ag+ | Ag− | Ag+ | Ag− | |||
| Oral swab | 45 | 15 | 0 | 100 | 75.0 (62.1–85.3) | 100.0 (96.4–100.0) |
| Nasal swab | 51 | 9 | 2 | 98 | 85.0 (73.4–92.9) | 98.0 (93.0–99.8) |
| PCR+ | PCR− | Sensitivity (95% CI) | Specificity (95% CI) | |||
|---|---|---|---|---|---|---|
| Ag+ | Ag− | Ag+ | Ag− | |||
| Oral swab | ||||||
| CtRdRp | ||||||
| ≤20 | 30 | 5 | 85.7 (69.7–95.2) | |||
| 20 < ≤ 25 | 13 | 3 | 81.3 (54.4–96.0) | |||
| 25 < ≤ 30 | 2 | 1 | 66.7 (9.4–99.2) | |||
| 30< | 0 | 6 | 0 | 100 | 0.0 (0.0–45.9) | 100.0 (96.4–100.0) |
| CtE | ||||||
| ≤20 | 34 | 6 | 85.0 (70.2–94.3) | |||
| 20 < ≤ 25 | 9 | 2 | 81.8 (48.2–97.7) | |||
| 25 < ≤ 30 | 2 | 1 | 66.7 (9.4–99.2) | |||
| 30< | 0 | 6 | 0 | 100 | 0.00 (0.0–45.9) | 100.0 (96.4–100.0) |
| Nasal swab | ||||||
| CtRdRp | ||||||
| ≤20 | 33 | 2 | 94.3 (80.8–99.3) | |||
| 20 < ≤ 25 | 15 | 1 | 93.8 (69.8–99.8) | |||
| 25 < ≤ 30 | 3 | 0 | 100.0 (29.2–100.0) | |||
| 30< | 0 | 6 | 2 | 98 | 0.0 (0.0–84.2) | 94.2 (87.9–97.9) |
| CtE | ||||||
| ≤20 | 37 | 3 | 92.55 (79.6–98.4) | |||
| 20 < ≤ 25 | 11 | 0 | 100.0 (71.5–100.0) | |||
| 25 < ≤ 30 | 3 | 0 | 100.0 (29.2–100.0) | |||
| 30< | 0 | 6 | 2 | 98 | 0.0 (0.0–45.9) | 98.0 (93.0–99.8) |
| PCR+ | PCR− | Sensitivity (95% CI) | Specificity (95% CI) | |||
|---|---|---|---|---|---|---|
| Ag+ | Ag− | Ag+ | Ag− | |||
| Oral swab | ||||||
| DASO | ||||||
| ≤1 | 27 | 8 | 0 | 50 | 77.1 (59.9–89.6) | 100.0 (92.9–100.0) |
| 2–3 | 18 | 7 | 0 | 41 | 72.0 (50.6–87.9) | 97.6 (87.4–99.9) |
| 4–6 | 0 | 9 | 100.0 (66.4–100.0) | |||
| Nasal swab | ||||||
| DASO | ||||||
| ≤1 | 30 | 5 | 1 | 49 | 85.7 (69.7–95.2) | 98.0 (89.4–99.9) |
| 2–3 | 21 | 4 | 0 | 41 | 84.0 (63.9–95.5) | 100.0 (91.4–100.0) |
| 4–6 | 1 | 8 | 88.9 (51.8–99.7) | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seo, J.D.; Moon, H.-W.; Shin, E.; Kim, J.Y.; Choi, S.-G.; Lee, J.A.; Choi, J.H.; Yun, Y.-M. Performance Evaluation of the STANDARD i-Q COVID-19 Ag Test with Nasal and Oral Swab Specimens from Symptomatic Patients. Diagnostics 2024, 14, 231. https://doi.org/10.3390/diagnostics14020231
Seo JD, Moon H-W, Shin E, Kim JY, Choi S-G, Lee JA, Choi JH, Yun Y-M. Performance Evaluation of the STANDARD i-Q COVID-19 Ag Test with Nasal and Oral Swab Specimens from Symptomatic Patients. Diagnostics. 2024; 14(2):231. https://doi.org/10.3390/diagnostics14020231
Chicago/Turabian StyleSeo, Jong Do, Hee-Won Moon, Eunju Shin, Ji Young Kim, Sang-Gyu Choi, Ju Ae Lee, Jeong Hwa Choi, and Yeo-Min Yun. 2024. "Performance Evaluation of the STANDARD i-Q COVID-19 Ag Test with Nasal and Oral Swab Specimens from Symptomatic Patients" Diagnostics 14, no. 2: 231. https://doi.org/10.3390/diagnostics14020231