
Integrating Point-of-Care Bacterial Fluorescence Imaging-Guided Care with Continued Wound Measurement for Enhanced Wound Area Reduction Monitoring
Abstract
:1. Introduction
2. Materials and Methods
2.1. Aims
2.2. Inclusion and Exclusion Criteria
2.3. Data Collection
2.4. Patient Assessment and Care Protocol
2.5. Manual Wound Measurement
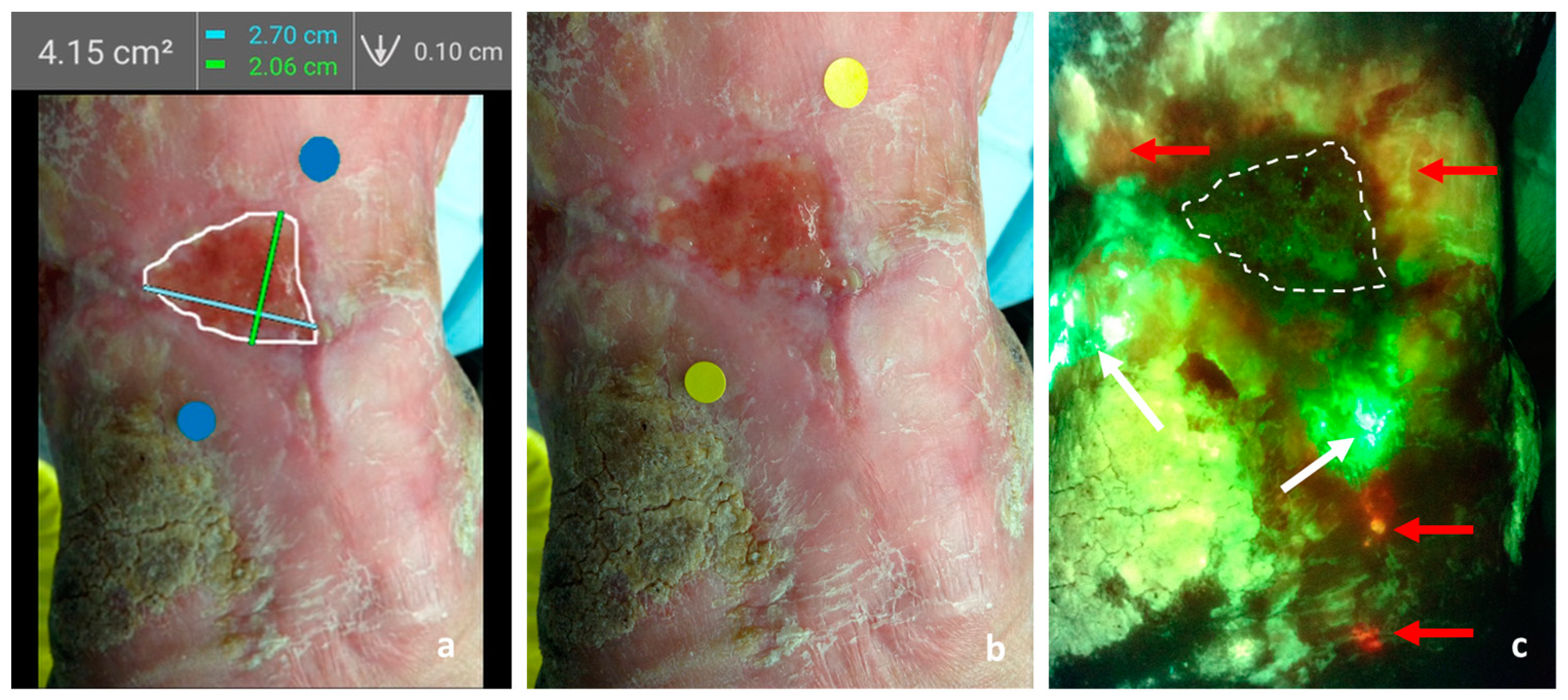
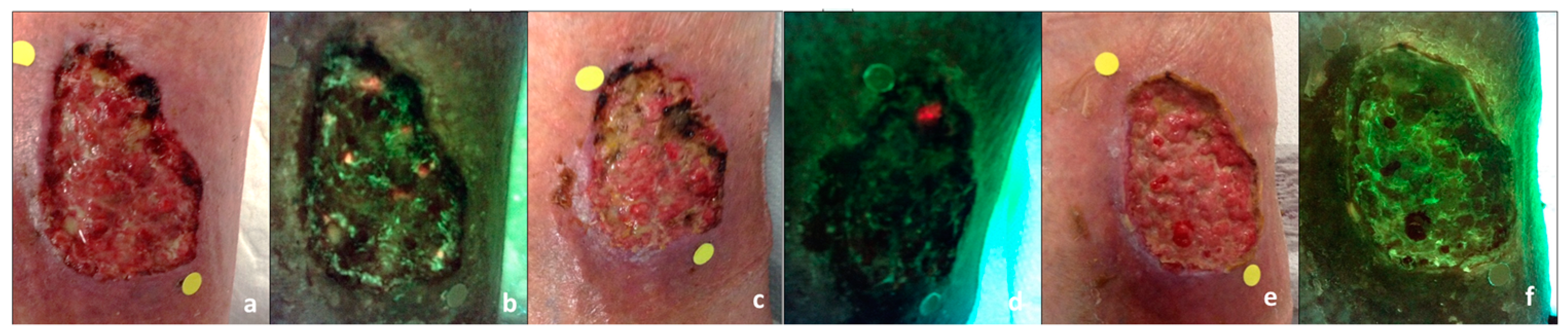
2.6. Digital Wound Measurement and Fluorescence Imaging
2.7. Statistical Analysis
3. Results
3.1. Description of the Study Population
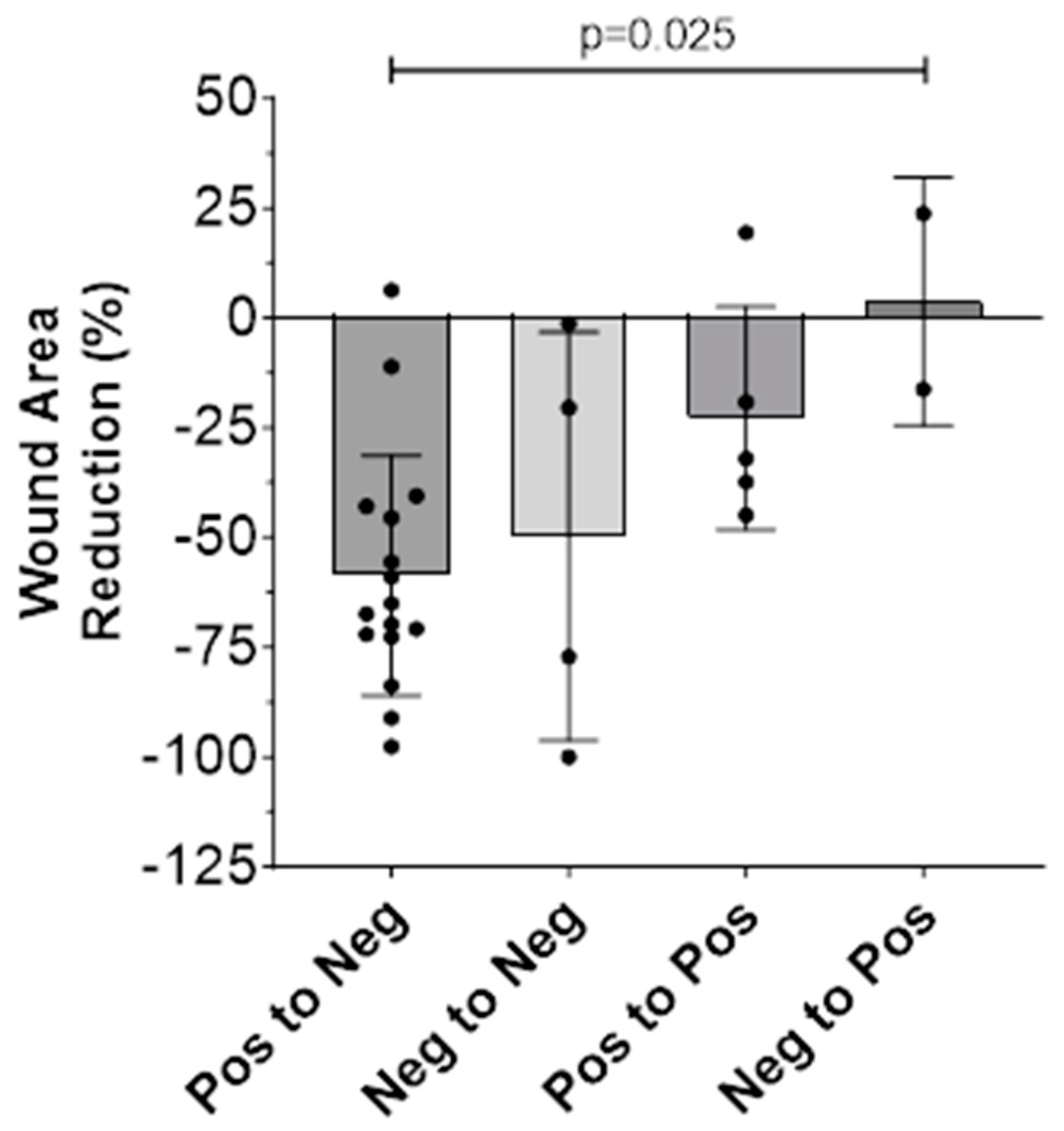
3.2. Wound Area Reduction (WAR)
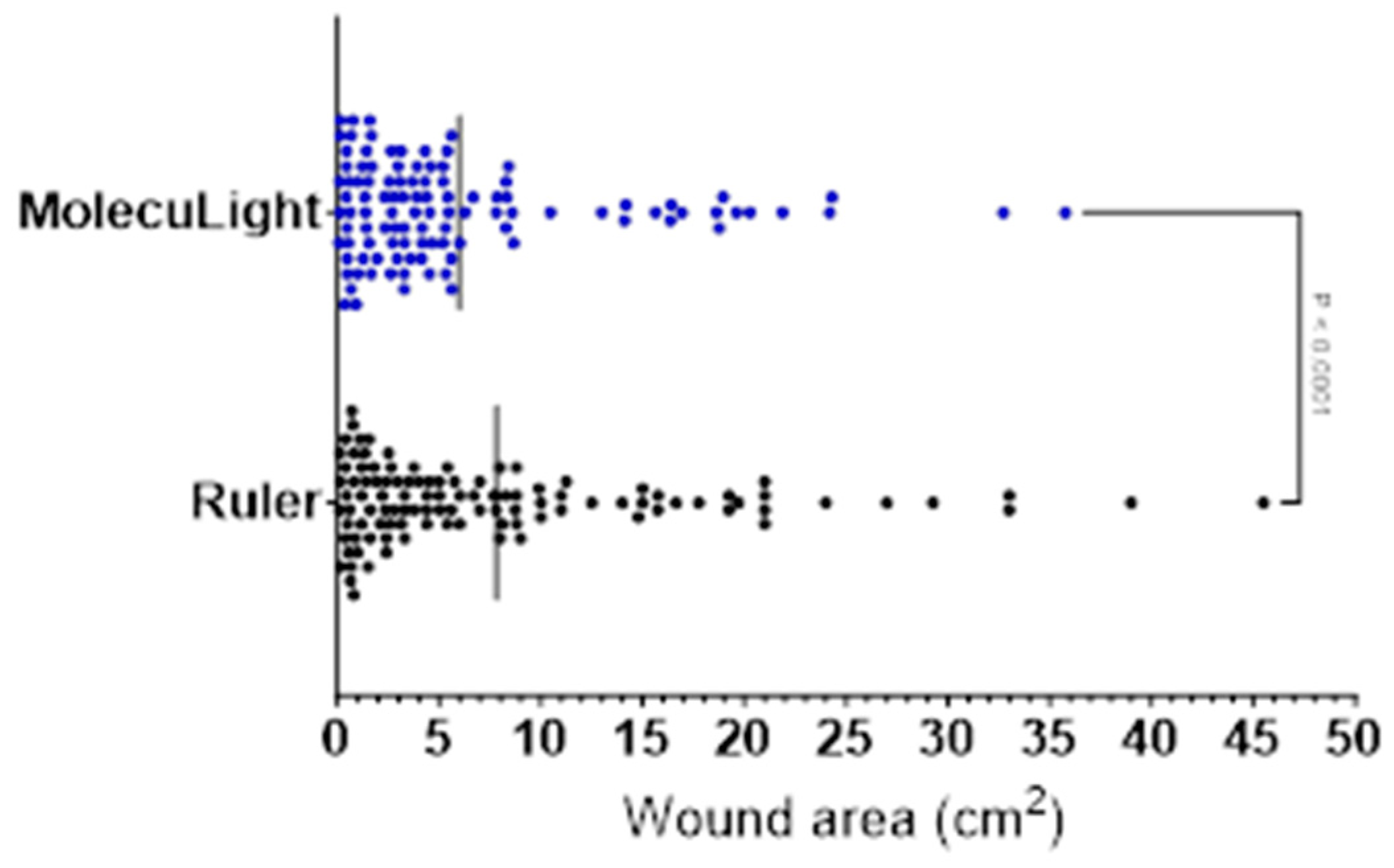
3.3. Wound Measurement Manual (Ruler) versus Digital (MolecuLight i:X)
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Marques, R.; Lopes, M.; Ramos, P.; Neves-Amado, J.; Alves, P. Prognostic factors for delayed healing of complex wounds in adults: A scoping review. Int. Wound J. 2023, 20, 2869–2886. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, M.C.; Tuma, P.; Carvalho, V.F.; Kamamoto, F. Complex Wounds. Clinics 2006, 61, 571–578. [Google Scholar] [CrossRef] [PubMed]
- Park, H.; Copeland, C.; Henry, S.; Barbul, A. Complex Wounds and Their Management. Surg. Clin. N. Am. 2010, 90, 1181–1194. [Google Scholar] [CrossRef] [PubMed]
- Guest, J.F.; Ayoub, N.; McIlwraith, T.; Uchegbu, I.; Gerrish, A.; Weidlich, D.; Vowden, K.; Vowden, P. Health economic burden that wounds impose on the National Health Service in the UK. BMJ Open 2015, 5, e009283. [Google Scholar] [CrossRef] [PubMed]
- Sen, C.K. Human Wound and Its Burden: Updated 2020 Compendium of Estimates. Adv. Wound Care 2021, 10, 281–292. [Google Scholar] [CrossRef] [PubMed]
- Järbrink, K.; Ni, G.; Sönnergren, H.; Schmidtchen, A.; Pang, C.; Bajpai, R.; Car, J. Prevalence and incidence of chronic wounds and related complications: A protocol for a systematic review. Syst. Rev. 2016, 5, 152. [Google Scholar] [CrossRef] [PubMed]
- Gottrup, F.; Henneberg, E.; Trangbæk, R.; Bækmark, N.; Zøllner, K.; Sørensen, J. Point prevalence of wounds and cost impact in the acute and community setting in Denmark. J. Wound Care 2013, 22, 413–422. [Google Scholar] [CrossRef]
- Sen, C.K. Human Wounds and Its Burden: Updated 2022 Compendium of Estimates. Adv. Wound Care 2023, 12, 657–670. [Google Scholar] [CrossRef]
- Guest, J.F.; Vowden, K.; Vowden, P. The health economic burden that acute and chronic wounds impose on an average clinical commissioning group/health board in the UK. J. Wound Care 2017, 26, 292–303. [Google Scholar] [CrossRef]
- Guest, J.F.; Ayoub, N.; McIlwraith, T.; Uchegbu, I.; Gerrish, A.; Weidlich, D.; Vowden, K.; Vowden, P. Health economic burden that different wound types impose on the UK’s National Health Service. Int. Wound J. 2017, 14, 322–330. [Google Scholar] [CrossRef]
- Olsson, M.; Järbrink, K.; Divakar, U.; Bajpai, R.; Upton, Z.; Schmidtchen, A.; Car, J. The humanistic and economic burden of chronic wounds: A systematic review. Wound Repair Regen. 2019, 27, 114–125. [Google Scholar] [CrossRef] [PubMed]
- Nussbaum, S.R.; Carter, M.J.; Fife, C.E.; DaVanzo, J.; Haught, R.; Nusgart, M.; Cartwright, D. An Economic Evaluation of the Impact, Cost, and Medicare Policy Implications of Chronic Nonhealing Wounds. Value Health 2018, 21, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Rahim, K.; Saleha, S.; Zhu, X.; Huo, L.; Basit, A.; Franco, O.L. Bacterial Contribution in Chronicity of Wounds. Microb. Ecol. 2017, 73, 710–721. [Google Scholar] [CrossRef] [PubMed]
- Bowler, P.G. The 10(5) bacterial growth guideline: Reassessing its clinical relevance in wound healing. Ostomy Wound Manag. 2003, 49, 44–53. Available online: https://www.ncbi.nlm.nih.gov/pubmed/12532033 (accessed on 3 August 2021).
- Bowler, P.G.; Duerden, B.I.; Armstrong, D.G. Wound microbiology and associated approaches to wound management. Clin. Microbiol. Rev. 2001, 14, 244–269. [Google Scholar] [CrossRef]
- Le, L.; Baer, M.; Briggs, P.; Bullock, N.; Cole, W.; DiMarco, D.; Hamil, R.; Harrell, K.; Kasper, M.; Li, W.; et al. Diagnostic Accuracy of Point-of-Care Fluorescence Imaging for the Detection of Bacterial Burden in Wounds: Results from the 350-Patient FLAAG Trial. Adv. Wound Care 2021, 10, 123–136. [Google Scholar] [CrossRef]
- Derwin, R.; Patton, D.; Strapp, H.; Moore, Z. The effect of inflammation management on pH, temperature, and bacterial burden. Int. Wound J. 2023, 20, 1118–1129. [Google Scholar] [CrossRef]
- Xu, L.; McLennan, S.V.; Lo, L.; Natfaji, A.; Bolton, T.; Liu, Y.; Twigg, S.M.; Yue, D.K. Bacterial load predicts healing rate in neuropathic diabetic foot ulcers. Diabetes Care 2007, 30, 378–380. [Google Scholar] [CrossRef]
- Armstrong, D.G.; Edmonds, M.E.; Serena, T.E. Point-of-care fluorescence imaging reveals extent of bacterial load in diabetic foot ulcers. Int. Wound J. 2023, 20, 554–566. [Google Scholar] [CrossRef]
- Attinger, C.; Wolcott, R. Clinically Addressing Biofilm in Chronic Wounds. Adv. Wound Care 2012, 1, 127–132. [Google Scholar] [CrossRef]
- Swanson, T.; Ousey, K.; Haesler, E.; Bjarnsholt, T.; Carville, K.; Idensohn, P.; Kalan, L.; Keast, D.H.; Larsen, D.; Percival, S.; et al. IWII Wound Infection in Clinical Practice consensus document: 2022 update. J. Wound Care 2022, 31, S10–S21. [Google Scholar] [CrossRef] [PubMed]
- Schultz, G.; Bjarnsholt, T.; James, G.A.; Leaper, D.J.; McBain, A.J.; Malone, M.; Stoodley, P.; Swanson, T.; Tachi, M.; Wolcott, R.D.; et al. Consensus guidelines for the identification and treatment of biofilms in chronic nonhealing wounds. Wound Repair Regen. 2017, 25, 744–757. [Google Scholar] [CrossRef] [PubMed]
- Stallard, Y. When and How to Perform Cultures on Chronic Wounds? J. Wound Ostomy Cont. Nurs. 2018, 45, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Bonham, P.A. Swab Cultures for Diagnosing Wound Infections. J. Wound Ostomy Cont. Nurs. 2009, 36, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Gardner, S.E.; Frantz, R.A.; Saltzman, C.L.; Hillis, S.L.; Park, H.; Scherubel, M. Diagnostic validity of three swab techniques for identifying chronic wound infection. Wound Repair Regen. 2006, 14, 548–557. [Google Scholar] [CrossRef] [PubMed]
- Serena, T.E.; Bowler, P.G.; Schultz, G.S.; D’souza, A.; Rennie, M.Y. Are Semi-Quantitative Clinical Cultures Inadequate? Comparison to Quantitative Analysis of 1053 Bacterial Isolates from 350 Wounds. Diagnostics 2021, 11, 1239. [Google Scholar] [CrossRef] [PubMed]
- Serena, T. Lack of Reliability of Clinical/Visual Assessment of Chronic Wound Infection: The Incidence of Biopsy-Proven Infection in Venous Leg Ulcers. Wounds 2006, 18, 5. [Google Scholar]
- Lipsky, B.A.; Berendt, A.R.; Deery, H.G.; Embil, J.M.; Joseph, W.S.; Karchmer, A.W.; LeFrock, J.L.; Lew, D.P.; Mader, J.T.; Norden, C.; et al. Diagnosis and treatment of diabetic foot infections. Clin. Infect. Dis. 2004, 39, 885–910. [Google Scholar] [CrossRef]
- Jones, L.M.; Dunham, D.; Rennie, M.Y.; Kirman, J.; Lopez, A.J.; Keim, K.C.; Little, W.; Gomez, A.; Bourke, J.; Ng, H.; et al. In vitro detection of porphyrin-producing wound bacteria with real-time fluorescence imaging. Futur. Microbiol. 2020, 15, 319–332. [Google Scholar] [CrossRef]
- Lopez, A.J.; Jones, L.M.; Reynolds, L.; Diaz, R.C.; George, I.K.; Little, W.; Fleming, D.; D’Souza, A.; Rennie, M.Y.; Rumbaugh, K.P.; et al. Detection of bacterial fluorescence from in vivo wound biofilms using a point-of-care fluorescence imaging device. Int. Wound J. 2021, 18, 626–638. [Google Scholar] [CrossRef]
- Raizman, R.; Little, W.; Smith, A.C. Rapid Diagnosis of Pseudomonas aeruginosa in Wounds with Point-of-Care Fluorescence Imaing. Diagnostics 2021, 11, 280. [Google Scholar] [CrossRef] [PubMed]
- Rennie, M.Y.; Dunham, D.; Lindvere-Teene, L.; Raizman, R.; Hill, R.; Linden, R. Understanding Real-Time Fluorescence Signals from Bacteria and Wound Tissues Observed with the MolecuLight i:XTM. Diagnostics 2019, 9, 22. [Google Scholar] [CrossRef] [PubMed]
- Rahma, S.; Woods, J.; Brown, S.; Nixon, J.; Russell, D. The Use of Point-of-Care Bacterial Autofluorescence Imaging in the Management of Diabetic Foot Ulcers: A Pilot Randomized Controlled Trial. Diabetes Care 2022, 45, 1601–1609. [Google Scholar] [CrossRef] [PubMed]
- Price, N. Routine Fluorescence Imaging to Detect Wound Bacteria Reduces Antibiotic Use and Antimicrobial Dressing Expenditure While Improving Healing Rates: Retrospective Analysis of 229 Foot Ulcers. Diagnostics 2020, 10, 927. [Google Scholar] [CrossRef] [PubMed]
- Okeahialam, N.A.; Thakar, R.; Sultan, A.H. Bacterial autofluorescence in infected perineal wounds: A prospective cohort study. Diagn. Microbiol. Infect. Dis. 2023, 105, 115831. [Google Scholar] [CrossRef]
- Jacob, A.; Jones, L.M.; Abdo, R.J.; Cruz-Schiavone, S.F.; Skerker, R.; Caputo, W.J.; Krehbiel, N.; Moyer-Harris, A.K.; McAtee, A.; Baker, I.; et al. Lights, fluorescence, action—Influencing wound treatment plans including debridement of bacteria and biofilms. Int. Wound J. 2023, 20, 3279–3288. [Google Scholar] [CrossRef]
- Lavery, L.A.; Barnes, S.A.; Keith, M.S.; Seaman, J.W.; Armstrong, D.G. Prediction of healing for postoperative diabetic foot wounds based on early wound area progression. Diabetes Care 2008, 31, 26–29. [Google Scholar] [CrossRef]
- Cardinal, M.; Eisenbud, D.E.; Phillips, T.; Harding, K. Early healing rates and wound area measurements are reliable predictors of later complete wound closure. Wound Repair Regen. 2008, 16, 19–22. [Google Scholar] [CrossRef]
- Sheehan, P.; Jones, P.; Caselli, A.; Giurini, J.M.; Veves, A. Percent Change in Wound Area of Diabetic Foot Ulcers over a 4-Week Period Is a Robust Predictor of Complete Healing in a 12-Week Prospective Trial. Diabetes Care 2003, 26, 1879–1882. [Google Scholar] [CrossRef]
- Jørgensen, L.B.; Sørensen, J.A.; Jemec, G.B.; Yderstræde, K.B. Methods to assess area and volume of wounds—A systematic review. Int. Wound J. 2016, 13, 540–553. [Google Scholar] [CrossRef]
- Rogers, L.C.; Bevilacqua, N.J.; Armstrong, D.G.; Andros, G. Digital planimetry results in more accurate wound measurements: A comparison to standard ruler measurements. J. Diabetes Sci. Technol. 2010, 4, 799–802. [Google Scholar] [CrossRef] [PubMed]
- Shetty, R.; Sreekar, H.; Lamba, S.; Gupta, A.K. A novel and accurate technique of photographic wound measurement. Indian J. Plast. Surg. 2012, 45, 425–429. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [PubMed]
- Nursing and Midwifery Board of Ireland. Code of Professional Conduct and Ethics for Registered Nurses and Registered Midwives; Nursing and Midwifery Board of Ireland: Dublin, Ireland, 2014. [Google Scholar]
- Derwin, R.; Patton, D.; Strapp, H.; Moore, Z. Wound pH and temperature as predictors of healing: An observational study. J. Wound Care 2023, 32, 302–310. [Google Scholar] [CrossRef] [PubMed]
- HSE National Wound Management Guidelines 2018 Clinical Strategy and Programmes Division. Available online: https://healthservice.hse.ie/filelibrary/onmsd/hse-wound-management-guidelines-2018.pdf (accessed on 7 November 2023).
- Snyder, R.J.; Fife, C.; Moore, Z. Components and Quality Measures of DIME (Devitalized Tissue, Infection/Inflammation, Moisture Balance, and Edge Preparation) in Wound Care. Adv. Ski. Wound Care 2016, 29, 205–215. [Google Scholar] [CrossRef] [PubMed]
- Leaper, D.J.; Schultz, G.; Carville, K.; Fletcher, J.; Swanson, T.; Drake, R. Extending the TIME concept: What have we learned in the past 10 years? Int. Wound J. 2012, 9 (Suppl. S2), 1–19. [Google Scholar] [CrossRef] [PubMed]
- Vidal, A.; Zerón, H.M.; Giacaman, I.; Romero, M.d.S.C.; López, S.P.; Trillo, L.E.M.; Pérez, D.A.P.; Concha, M.; Torres-Gallegos, C.; Orellana, S.L.; et al. A Simple Mathematical Model for Wound Closure Evaluation. J. Am. Coll. Clin. Wound Spéc. 2015, 7, 40–49. [Google Scholar] [CrossRef]
- Jessup, R.L. What is the Best Method for Assessing the Rate of Wound Healing? Adv. Ski. Wound Care 2006, 19, 138–147. [Google Scholar] [CrossRef]
- Raizman, R.; Dunham, D.; Lindvere-Teene, L.; Jones, L.M.; Tapang, K.; Linden, R.; Rennie, M.Y. Use of a bacterial fluorescence imaging device: Wound measurement, bacterial detection and targeted debridement. J. Wound Care 2019, 28, 824–834. [Google Scholar] [CrossRef]
- Siddiqui, A.R.; Bernstein, J.M. Chronic wound infection: Facts and controversies. Clin. Dermatol. 2010, 28, 519–526. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | Acute (%) | Chronic (%) | |
|---|---|---|---|
| Number of patients | 26 | 16 (61.5) | 10 (38.5) |
| Number of wounds | 27 | 16 (59.3) | 11 (40.7) |
| Age—mean (SD) | 47.1 (19.5) | 44.7 (19.6) | 50.9 (19.7) |
| Gender (%) | |||
| Male | 5 (19.2) | 2 (12.5) | 3 (30.0) |
| Female | 21 (80.8) | 14 (87.5) | 7 (70.7) |
| Comorbidities | |||
| >1 * | 17 (65.4) | 10 (62.5) | 7 (70.0) |
| Diabetes | 6 (23.1) | 3 (18.8) | 3 (30.0) |
| COPD | 1 (3.8) | 0 | 1 (10.0) |
| Peripheral vascular disease | 2 (7.7) | 0 | 2 (20.0) |
| Kidney disease | 1 (3.8) | 1 (6.3) | 0 |
| Hypertension | 6 (23.1) | 4 (25.0) | 2 (20.0) |
| Smoking | 11 (42.3) | 9 (56.3) | 2 (20.0) |
| Wound Location (%) | |||
| Buttocks | 5 (18.5) | 2 (12.5) | 3 (27.3) |
| Abdomen | 5 (18.5) | 3 (18.8) | 2 (18.2) |
| Lower leg | 5 (18.5) | 2 (12.5) | 3 (27.3) |
| Thigh | 2 (7.4) | 2 (12.5) | 0 |
| Foot | 6 (22.2) | 3 18.8) | 3 (27.3) |
| Back | 2 (7.4) | 2 (12.5) | 0 |
| Other | 2 (7.4) | 2 (12.5) | 0 |
| Visit 1 Avg Wound Area (cm2) | Visit 4 Avg Wound Area (cm2) | ∆ Wound Area cm2 | ∆ Wound Area % | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Type | n | % | RULER | DIGITAL * | RULER | DIGITAL * | RULER | DIGITAL * | RULER | DIGITAL * |
| All | 27 | - | 9.74 | 7.30 | 5.94 | 4.68 | −3.80 | −2.62 | −46.87 | −46.05 |
| Acute | 16 | 59.3 | 8.85 | 6.11 | 4.56 | 3.57 | −4.29 | −2.55 | −49.76 | −45.80 |
| Chronic | 11 | 40.7 | 11.03 | 9.04 | 7.94 | 6.31 | −3.09 | −2.73 | −42.67 | −46.40 |
| Visit 1 Avg Wound Area | Visit 4 Avg Wound Area | ∆ Wound Area cm2 | ∆ Wound Area % | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Classification Visit 1–Visit 4 | n | % | Manual | Digital * | Manual | Digital * | Manual | Digital * | Manual | Digital * |
| pos-pos | 5 | 19 | 20.28 | 17.37 | 16.73 | 13.48 | −3.55 | −3.89 | −16.66 | −22.81 |
| pos-neg | 16 | 59 | 8.11 | 5.45 | 3.46 | 2.44 | −4.65 | −3.02 | −62.07 | −58.63 |
| neg-pos | 2 | 7 | 4.20 | 4.04 | 4.50 | 3.91 | 0.31 | −0.13 | 19.24 | 3.77 |
| neg-neg | 4 | 15 | 5.82 | 3.78 | 3.09 | 3.07 | −2.73 | −0.71 | −56.89 | −49.69 |
| Acute and Chronic | Ruler (Wound Area in cm2) | Digital (Wound Area in cm2) | Difference (Absolute) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Visit | N | Avg | MIN | MAX | Avg | MIN | MAX | ∆ cm2 | MIN | MAX |
| 1 | 27 | 9.74 | 0.54 | 45.50 | 7.30 | 0.48 | 35.76 | 2.65 | 0.01 | 12.58 |
| 2 | 27 | 8.20 | 0.16 | 39.00 | 6.23 | 0.14 | 32.72 | 2.14 | 0.02 | 10.59 |
| 3 | 27 | 7.11 | 0.14 | 33.00 | 5.54 | 0.10 | 24.2 | 1.68 | 0.00 | 8.8 |
| 4 | 26 | 6.17 | 0.10 | 33.00 | 4.86 | 0.07 | 24.3 | 1.41 | 0.02 | 8.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Derwin, R.; Patton, D.; Strapp, H.; Moore, Z. Integrating Point-of-Care Bacterial Fluorescence Imaging-Guided Care with Continued Wound Measurement for Enhanced Wound Area Reduction Monitoring. Diagnostics 2024, 14, 2. https://doi.org/10.3390/diagnostics14010002
Derwin R, Patton D, Strapp H, Moore Z. Integrating Point-of-Care Bacterial Fluorescence Imaging-Guided Care with Continued Wound Measurement for Enhanced Wound Area Reduction Monitoring. Diagnostics. 2024; 14(1):2. https://doi.org/10.3390/diagnostics14010002
Chicago/Turabian StyleDerwin, Rosemarie, Declan Patton, Helen Strapp, and Zena Moore. 2024. "Integrating Point-of-Care Bacterial Fluorescence Imaging-Guided Care with Continued Wound Measurement for Enhanced Wound Area Reduction Monitoring" Diagnostics 14, no. 1: 2. https://doi.org/10.3390/diagnostics14010002