
The Fluoroless Future in Electrophysiology: A State-of-the-Art Review
 , , and
, , and
Abstract
:1. Introduction
2. Radiation-Related Risks
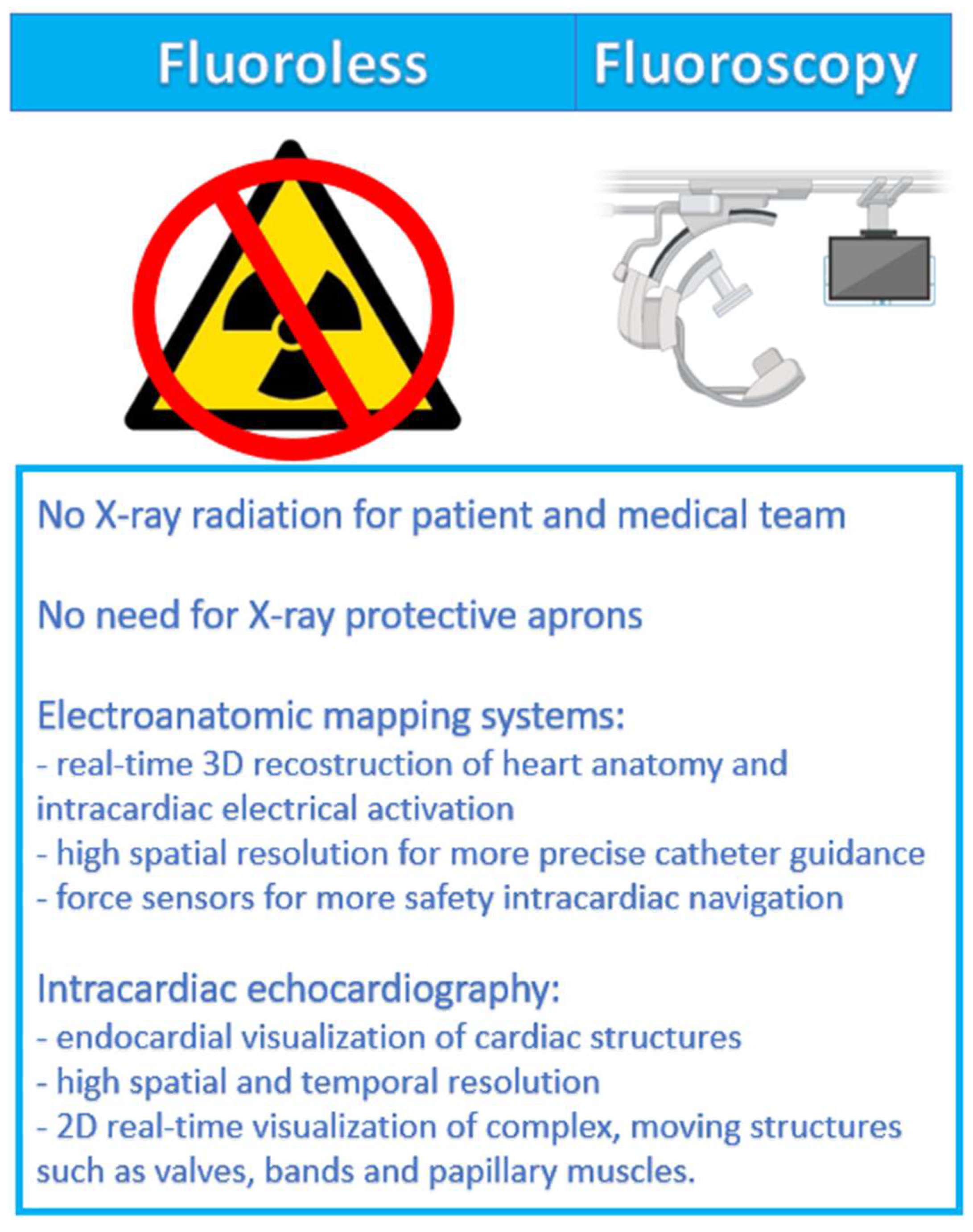
3. Non-Fluoroscopic Technologies
3.1. Three-Dimensional Electroanatomic Mapping Systems
3.2. Intracardiac Echocardiography
4. Fluoroless Procedures in EP Labs
4.1. Paroxysmal Supraventricular Tachycardias
4.2. Atrial Fibrillation and Atrial Flutter
4.3. Ventricular Tachycardia and Premature Ventricular Contraction
5. Device Implantation and Other Possible Use of Zero-Fluoroscopy
6. Cost-Effectiveness
7. Limitations and Future Perspectives
8. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Picano, E.; Vañó, E.; Rehani, M.M.; Cuocolo, A.; Mont, L.; Bodi, V.; Bar, O.; Maccia, C.; Pierard, L.; Sicari, R.; et al. The appropriate and justified use of medical radiation in cardiovascular imaging: A position document of the ESC Associations of Cardiovascular Imaging, Percutaneous Cardiovascular Interventions and Electrophysiology. Eur. Heart J. 2014, 35, 665–672. [Google Scholar] [CrossRef] [PubMed]
- Fazel, R.; Gerber, T.C.; Balter, S.; Brenner, J.D.; Jeffrey Carr, J.; Cerqueira, M.D.; Chen, J.; Einstein, A.J.; Krumholz, H.M.; Manesh, M.; et al. Approaches to enhancing radiation safety in cardiovascular imaging: A scientific statement from the American Heart Association. Circulation 2014, 130, 1730–1748. [Google Scholar] [CrossRef]
- Klein, L.W.; Miller, D.L.; Balter, S.; Laskey, W.; Haines, D.; Norbash, A.; Mauro, M.A.; Goldstein, J.A. Occupational health hazards in the interventional laboratory: Time for a safer environment. Heart Rhythm. 2009, 6, 439–444. [Google Scholar] [CrossRef] [PubMed]
- Jones, C.G. The US Nuclear Regulatory Commission radiation protection policy and opportunities for the future. J. Radiol. Prot. 2019, 39, R51–R62. [Google Scholar] [CrossRef] [PubMed]
- Debreceni, D.; Janosi, K.; Bocz, B.; Turcsan, M.; Lukacs, R.; Simor, T.; Antolic, B.; Vamos, M.; Komocsi, A.; Kupo, P. Zero fluoroscopy catheter ablation for atrial fibrillation: A systematic review and meta-analysis. Front. Cardiovasc. Med. 2023, 10, 1178783. [Google Scholar] [CrossRef]
- Kipp, R.T.; Boynton, J.R.; Field, M.E.; Wang, J.F.; Bares, A.; Leal, M.A.; VON Bergen, N.H.; Eckhardt, L.L. Outcomes During Intended Fluoroscopy-free Ablation in Adults and Children. J. Innov. Card. Rhythm. Manag. 2018, 9, 3305–3311. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.D.; Abid, Q.U.A.; Ravi, V.; Sharma, P.; Larsen, T.; Krishnan, K.; Trohman, R.G. Meta-analysis of pulmonary vein isolation ablation for atrial fibrillation conventional vs low- and zero-fluoroscopy approaches. J. Cardiovasc. Electrophysiol. 2020, 31, 1403–1412. [Google Scholar] [CrossRef]
- Gaita, F.; Guerra, P.G.; Battaglia, A.; Anselmino, M. The dream of near-zero X-rays ablation comes true. Eur. Heart J. 2016, 37, 2749–2755. [Google Scholar] [CrossRef]
- Kim, Y.H.; Chen, S.A.; Ernst, S.; Guzman, C.E.; Han, S.; Kalarus, Z.; Labadet, C.; Lin, Y.-J.; Lo, L.W.; Nogami, A.; et al. 2019 APHRS expert consensus statement on three-dimensional mapping systems for tachycardia developed in collaboration with HRS, EHRA, and LAHRS. J. Arhythmia 2020, 36, 215–270. [Google Scholar] [CrossRef]
- Enriquez, A.; Saenz, L.C.; Rosso, R.; Silvestry, F.E.; Callans, D.; Marchlinski, E.; Garcia, F. Use of Intracardiac Echocardiography in Interventional Cardiology. Circulation 2018, 137, 2278–2294. [Google Scholar] [CrossRef]
- Debreceni, D.; Janosi, K.; Vamos, M.; Komocsi, A.; Simor, T.; Kupo, P. Zero and Minimal Fluoroscopic Approaches during Ablation of Supraventricular Tachycardias: A Systematic Review and Meta-Analysis. Front. Cardiovasc. Med. 2022, 9, 856145. [Google Scholar] [CrossRef] [PubMed]
- Sarkozy, A.; De Potter, T.; Heidbuchel, H.; Ernst, S.; Kosiuk, J.; Vano, E.; Picano, E.; Arbelo, E.; Tedrow, U. Occupational radiation exposure in the electrophysiology laboratory with a focus on personnel with reproductive potential and during pregnancy: A European Heart Rhythm Association (EHRA) consensus document endorsed by the Heart Rhythm Society (HRS). Europace 2017, 19, 1909–1922. [Google Scholar] [CrossRef] [PubMed]
- Ector, J.; Dragusin, O.; Adriaenssens, B.; Huybrechts, W.; Willems, R.; Ector, H.; Heidbüchel, H. Obesity is a major determinant of radiation dose in patients undergoing pulmonary vein isolation for atrial fibrillation. J. Am. Coll. Cardiol. 2007, 50, 234–242. [Google Scholar] [CrossRef] [PubMed]
- Hirshfeld, J.W.; Ferrari, V.A.; Bengel, F.M.; Bergersen, L.; Chambers, C.E.; Einstein, A.J.; Eisenberg, M.J.; Fogel, M.A.; Gerber, T.C.; Haines, D.E.; et al. 2018 ACC/HRS/NASCI/SCAI/SCCT Expert Consensus Document on Optimal Use of Ionizing Radiation in Cardiovascular Imaging-Best Practices for Safety and Effectiveness, Part 2: Radiological Equipment Operation, Dose-Sparing Methodologies, Patient and Medical Personnel Protection: A Report of the American College of Cardiology Task Force on Expert Consensus Decision Pathways. J. Am. Coll. Cardiol. 2018, 71, 2829–2855. [Google Scholar] [CrossRef] [PubMed]
- Mascia, G.; Giaccardi, M. A New Era in Zero X-ray Ablation. Arhythm. Electrophysiol. Rev. 2020, 9, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Prolic Kalinsek, T.; Sorli, J.; Jan, M.; Šinkovec, M.; Antolič, B.; Klemen, L.; Žižek, D.; Pernat, A. Conventional fluoroscopy-guided vs zero-fluorscopy catheter ablation of supraventricular tachycardias. Europace 2022, 24 (Suppl. 1), euac053.307. [Google Scholar] [CrossRef]
- Al Kharji, S.; Connell, T.; Bernier, M.; Eisenberg, M.J. Ionizing Radiation in Interventional Cardiology and Electrophysiology. Can. J. Cardiol. 2019, 35, 535–538. [Google Scholar] [CrossRef]
- Perisinakis, K.; Damilakis, J.; Theocharopoulos, N.; Manios, E.; Vardas, P.; Gourtsoyiannis, N. Accurate assessment of patient effective radiation dose and associated detriment risk from radiofrequency catheter ablation procedures. Circulation 2001, 104, 58–62. [Google Scholar] [CrossRef]
- Qin, D.; Ptaszek, L.M. A Practical Guide to Ultrasound-guided Venous Access During Implantation of Pacemakers and Defibrillators. J. Innov. Card. Rhythm. Manag. 2022, 13, 4873–4877. [Google Scholar] [CrossRef]
- Nagaraju, L.; Menon, D.; Aziz, P.F. Use of 3D Electroanatomical Navigation (CARTO-3) to Minimize or Eliminate Fluoroscopy Use in the Ablation of Pediatric Supraventricular Tachyarrhythmias. Pacing Clin. Electrophysiol. 2016, 39, 574–580. [Google Scholar] [CrossRef]
- Philip Saul, J.; Kanter, R.J.; Writing Committee; Abrams, D.; Asirvatham, S.; Bar-Cohen, Y.; Blaufox, A.D.; Cannon, B.; Clark, J.; Dick, M.; et al. PACES/HRS expert consensus statement on the use of catheter ablation in children and patients with congenital heart disease: Developed in partnership with the Pediatric and Congenital Electrophysiology Society (PACES) and the Heart Rhythm Society (HRS). Endorsed by the governing bodies of PACES, HRS, the American Academy of Pediatrics (AAP), the American Heart Association (AHA), and the Association for European Pediatric and Congenital Cardiology (AEPC). Heart Rhythm. 2016, 13, e251–e289. [Google Scholar] [CrossRef] [PubMed]
- Andreassi, M.G.; Picano, E. Reduction of radiation to children: Our responsibility to change. Circulation 2014, 130, 135–137. [Google Scholar] [CrossRef] [PubMed]
- Andreassi, M.G.; Piccaluga, E.; Guagliumi, G.; Del Greco, M.; Gaita, F.; Picano, E. Occupational Health Risks in Cardiac Catheterization Laboratory Workers. Circ. Cardiovasc. Interv. 2016, 9, e003273. [Google Scholar] [CrossRef]
- Roguin, A.; Goldstein, J.; Bar, O.; Goldstein, J.A. Brain and neck tumors among physicians performing interventional procedures. Am. J. Cardiol. 2013, 111, 1368–1372. [Google Scholar] [CrossRef] [PubMed]
- Marazziti, D.; Tomaiuolo, F.; Dell’Osso, L.; Demi, V.; Campana, S.; Piccaluga, E.; Guagliumi, G.; Conversano, C.; Baroni, S.; Andreassi, M.G.; et al. Neuropsychological Testing in Interventional Cardiology Staff after Long-Term Exposure to Ionizing Radiation. J. Int. Neuropsychol. Soc. 2015, 21, 670–676. [Google Scholar] [CrossRef]
- Marinskis, G.; Bongiorni, M.G.; Dagres, N.; Lewalter, T.; Pison, L.; Blomstrom-Lundqvist, C. X-ray exposure hazards for physicians performing ablation procedures and device implantation: Results of the European Heart Rhythm Association survey. Europace 2013, 15, 444–446. [Google Scholar] [CrossRef]
- Pelz, D.M. Low back pain, lead aprons, and the angiographer. AJNR Am. J. Neuroradiol. 2000, 21, 1364. [Google Scholar]
- Bhakta, D.; Miller, J.M. Principles of electroanatomic mapping. Indian. Pacing Electrophysiol. J. 2008, 8, 32–50. [Google Scholar]
- Elgendy, A.Y.; Mahmoud, A.N.; Khan, M.S.; Sheikh, M.R.; Mojadidi, M.K.; Omer, M.; Elgendy, I.Y.; Bavry, A.A.; Ellenbogen, K.A.; Miles, W.M.; et al. Meta-Analysis Comparing Catheter-Guided Ablation Versus Conventional Medical Therapy for Patients with Atrial Fibrillation and Heart Failure with Reduced Ejection Fraction. Am. J. Cardiol. 2018, 122, 806–813. [Google Scholar] [CrossRef]
- Bergonti, M.; Dello Russo, A.; Sicuso, R.; Ribatti, V.; Compagnucci, P.; Catto, V.; Gasperetti, A.; Zucchetti, M.; Cellucci, S.; Vettor, G.; et al. Long-Term Outcomes of Near-Zero Radiation Ablation of Paroxysmal Supraventricular Tachycardia: A Comparison with Fluoroscopy-Guided Approach. JACC Clin. Electrophysiol. 2021, 7, 1108–1117. [Google Scholar] [CrossRef]
- Purtell, C.S.; Kipp, R.T.; Eckhardt, L.L. Into a Fluoroless Future: An Appraisal of Fluoroscopy-Free Techniques in Clinical Cardiac Electrophysiology. Curr. Cardiol. Rep. 2021, 23, 28. [Google Scholar] [CrossRef] [PubMed]
- Borlich, M.; Sommer, P. Cardiac Mapping Systems: Rhythmia, Topera, EnSite Precision, and CARTO. Card. Electrophysiol. Clin. 2019, 11, 449–458. [Google Scholar] [CrossRef] [PubMed]
- Kautzner, J.; Peichl, P. Mapping and Ablation of Unmappable Ventricular Tachycardia, Ventricular Tachycardia Storm, and Those in Acute Myocardial Infarction. Card. Electrophysiol. Clin. 2019, 11, 675–688. [Google Scholar] [CrossRef] [PubMed]
- Andreu, D.; Berruezo, A.; Ortiz-Pérez, J.T.; Silva, E.; Mont, L.; Borras, R.; de Caralt, T.M.; Peres, R.J.; Fernandez-Arment, J.; Zeliko, H.; et al. Integration of 3D Electroanatomic Maps and Magnetic Resonance Scar Characterization Into the Navigation System to Guide Ventricular Tachycardia Ablation. Circ. Arrhythmia Electrophysiol. 2011, 4, 674–683. [Google Scholar] [CrossRef] [PubMed]
- Hawson, J.; Joshi, S.; Al-Kaisey, A.; Das, S.K.; Anderson, R.D.; Morton, J.; Kumar, S.; Kristler, P.; Kalman, J.; Lee, G. Utility of cardiac imaging in patients with ventricular tachycardia. Indian Pacing Electrophysiol. J. 2023, 23, 63–76. [Google Scholar] [CrossRef]
- Stoks, J.; Hermans, B.J.M.; Boukens, B.J.D.; Holtackers, R.J.; Gommers, S.; Kaya, Y.S.; Vernooy, K.; Cluitmans, M.J.M.; Volders, P.G.A.; Ter Bekke, R.M.A. High-resolution structural-functional substrate-trigger characterization: Future roadmap for catheter ablation of ventricular tachycardia. Front. Cardiovasc. Med. 2023, 10, 1112980. Available online: https://www.frontiersin.org/articles/10.3389/fcvm.2023.1112980 (accessed on 18 August 2023). [CrossRef]
- Koutalas, E.; Rolf, S.; Dinov, B.; Richeter, S.; Arya, A.; Bollmann, A.; Hindricks, G.; Sommer, P. Contemporary Mapping Techniques of Complex Cardiac Arrhythmias—Identifying and Modifying the Arrhythmogenic Substrate. Arrhythm. Electrophysiol. Rev. 2015, 4, 19–27. [Google Scholar] [CrossRef]
- Mantziari, L.; Butcher, C.; Kontogeorgis, A.; Panikker, S.; Roy, K.; Markides, V.; Wong, T. Utility of a Novel Rapid High-Resolution Mapping System in the Catheter Ablation of Arrhythmias: An Initial Human Experience of Mapping the Atria and the Left Ventricle. JACC Clin. Electrophysiol. 2015, 1, 411–420. [Google Scholar] [CrossRef]
- Casella, M.; Dello Russo, A.; Pelargonio, G.; Del Greco, M.; Zingarini, G.; Piacenti, M.; Di Cori, A.; Casula, V.; Marini, M.; Pizzamiglio, F.; et al. Near zerO fluoroscopic exPosure during catheter ablAtion of supRavenTricular arrhYthmias: The NO-PARTY multicentre randomized trial. Europace 2016, 18, 1565–1572. [Google Scholar] [CrossRef]
- Mah, D.Y.; Miyake, C.Y.; Sherwin, E.D.; Walsh, A.; Anderson, M.J.; Western, K.; Abrams, D.J.; Alexander, M.E.; Cecchin, F.; Walsh, E.P.; et al. The use of an integrated electroanatomic mapping system and intracardiac echocardiography to reduce radiation exposure in children and young adults undergoing ablation of supraventricular tachycardia. Europace 2014, 16, 277–283. [Google Scholar] [CrossRef]
- Gist, K.; Tigges, C.; Smith, G.; Clark, J. Learning Curve for Zero-Fluoroscopy Catheter Ablation of AVNRT: Early versus Late Experience. Pacing Clin. Electrophysiol. 2011, 34, 264–268. [Google Scholar] [CrossRef] [PubMed]
- Mhanna, M.; Beran, A.; Al-Abdouh, A.; Sajdeya, O.; Barbarawi, M.; Alsaiqali, M.; Jabri, A.; Aò-Aaraj, A.; Alharbi, A.; Chacko, P. Steerable versus nonsteerable sheath technology in atrial fibrillation ablation: A systematic review and meta-analysis. J. Arrhythmia 2022, 38, 570–579. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, N.; Mittal, A.; Galvin, J.; Jauvert, G.; Keaney, J.; Keelan, E.; O’Brien, J.; Sźeplaki, G. The impact of steerable sheath visualization during catheter ablation for atrial fibrillation. Europace 2023, 25, 1345–1351. [Google Scholar] [CrossRef] [PubMed]
- Janosi, K.; Debreceni, D.; Janosa, B.; Bocz, B.; Simor, T.; Kupo, P. Visualizable vs. standard, non-visualizable steerable sheath for pulmonary vein isolation procedures: Randomized, single-centre trial. Front. Cardiovasc. Med. 2022, 9, 1033755. Available online: https://www.frontiersin.org/articles/10.3389/fcvm.2022.1033755 (accessed on 7 January 2024). [CrossRef] [PubMed]
- Guo, P.; Qiu, J.; Wang, Y.; Chen, G.; Proietti, R.; Fadhle, A.S.; Zhao, C.; Wang, D.W. Zero-fluoroscopy permanent pacemaker implantation using Ensite NavX system: Clinical viability or fanciful technique? Pacing Clin. Electrophysiol. 2018, 41, 122–127. [Google Scholar] [CrossRef] [PubMed]
- Luani, B.; Zrenner, B.; Basho, M.; Genz, C.; Rauwolf, T.; Tanev, I.; Schmeisser, A.; Braun-Dullaeus, R.C. Zero-fluoroscopy cryothermal ablation of atrioventricular nodal re-entry tachycardia guided by endovascular and endocardial catheter visualization using intracardiac echocardiography (Ice&ICE Trial). J. Cardiovasc. Electrophysiol. 2018, 29, 160–166. [Google Scholar] [CrossRef]
- Asvestas, D.; Xenos, T.; Tzeis, S. The contribution of intracardiac echocardiography in catheter ablation of ventricular arrhythmias. Rev. Cardiovasc. Med. 2022, 23, 25. [Google Scholar] [CrossRef]
- Vitulano, N.; Pazzano, V.; Pelargonio, G.; Narducci, M.L. Technology update: Intracardiac echocardiography—A review of the literature. Med. Devices Evid. Res. 2015, 8, 231–239. [Google Scholar] [CrossRef]
- Kautzner, J.; Haskova, J.; Lehar, F. Intracardiac Echocardiography to Guide Non-fluoroscopic Electrophysiology Procedures. Card. Electrophysiol. Clin. 2021, 13, 399–408. [Google Scholar] [CrossRef]
- Kupo, P.; Saghy, L.; Bencsik, G.; Kohari, M.; Makai, A.; Vamos, M.; Benak, A.; Miklos, M.; Raileanu, G.; Schvartz, N.; et al. Randomized trial of intracardiac echocardiography-guided slow pathway ablation. J. Interv. Card. Electrophysiol. 2022, 63, 709–714. [Google Scholar] [CrossRef]
- Ponti, R.D. Reduction of radiation exposure in catheter ablation of atrial fibrillation: Lesson learned. World J. Cardiol. 2015, 7, 442–448. [Google Scholar] [CrossRef] [PubMed]
- Marini, M.; Martin, M.; Ravanelli, D.; Del Greco, M.; Quintarelli, S.; Guarracini, F.; Coser, A.; Valentinelli, A.; Bonmassari, R. Extensive Use of 3D Nonfluoroscopic Mapping Systems for Reducing Radiation Exposure during Catheter Ablation Procedures: An Analysis of 10 Years of Activity. BioMed Res. Int. 2019, 2019, e4217076. [Google Scholar] [CrossRef] [PubMed]
- Žižek, D.; Antolič, B.; Prolič Kalinšek, T.; Štublar, J.; Kajdič, N.; Jelenc, M.; Jan, M. Intracardiac echocardiography-guided transseptal puncture for fluoroless catheter ablation of left-sided tachycardias. J. Interv. Card. Electrophysiol. 2021, 61, 595–602. [Google Scholar] [CrossRef] [PubMed]
- Tahin, T.; Riba, A.; Nemeth, B.; Arvai, F.; Lupkovics, G.; Szeplaki, G.; Geller, L. Implementation of a zero fluoroscopic workflow using a simplified intracardiac echocardiography guided method for catheter ablation of atrial fibrillation, including repeat procedures. BMC Cardiovasc. Disord. 2021, 21, 407. [Google Scholar] [CrossRef] [PubMed]
- Page, R.L.; Joglar, J.A.; Caldwell, M.A.; Calkins, H.; Conti, J.B.; Deal, B.J.; Estes, N.A.M., 3rd; Field, M.E.; Goldberg, Z.D.; Hammil, S.C.; et al. 2015 ACC/AHA/HRS Guideline for the Management of Adult Patients with Supraventricular Tachycardia: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation 2016, 133, e506–e574. [Google Scholar] [CrossRef]
- Brugada, J.; Katritsis, D.G.; Arbelo, E.; Arribas, F.; Bax, J.J.; Blomstrőm-Lundqvist, C.; Calkins, H.; Corrado, D.; Deftereos, S.G.; Diller, G.P.; et al. 2019 ESC Guidelines for the management of patients with supraventricular tachycardiaThe Task Force for the management of patients with supraventricular tachycardia of the European Society of Cardiology (ESC). Eur. Heart J. 2020, 41, 655–720. [Google Scholar] [CrossRef] [PubMed]
- Orejarena, L.A.; Vidaillet, H.; DeStefano, F.; Nordstrom, D.L.; Vierkant, R.A.; Smith, P.N.; Hayes, J.J. Paroxysmal supraventricular tachycardia in the general population. J. Am. Coll. Cardiol. 1998, 31, 150–157. [Google Scholar] [CrossRef]
- Shotan, A.; Ostrzega, E.; Mehra, A.; Johnson, J.V.; Elkayam, U. Incidence of arrhythmias in normal pregnancy and relation to palpitations, dizziness, and syncope. Am. J. Cardiol. 1997, 79, 1061–1064. [Google Scholar] [CrossRef]
- Katritsis, D.G.; Zografos, T.; Katritsis, G.D.; Giazitzoglou, E.; Vachliotis, V.; Paxinos, G.; Camm, A.J.; Josephson, M.E. Catheter ablation vs. antiarrhythmic drug therapy in patients with symptomatic atrioventricular nodal re-entrant tachycardia: A randomized, controlled trial. Europace 2017, 19, 602–606. [Google Scholar] [CrossRef]
- Yang, L.; Sun, G.; Chen, X.; Chen, G.; Yang, S.; Guo, P.; Wang, Y.; Wang, D.W. Meta-Analysis of Zero or Near-Zero Fluoroscopy Use During Ablation of Cardiac Arrhythmias. Am. J. Cardiol. 2016, 118, 1511–1518. [Google Scholar] [CrossRef]
- Di Cori, A.; Zucchelli, G.; Segreti, L.; Barletta, V.; Viani, S.; Paperini, L.; Della Tommasina, V.; Cellamaro, T.; Vecchi, A.; Soldati, E.; et al. Predictors of zero X ray procedures in supraventricular arrhythmias ablation. Int. J. Cardiovasc. Imaging. 2020, 36, 1599–1607. [Google Scholar] [CrossRef] [PubMed]
- Stec, S.; Śledź, J.; Mazij, M.; Raś, M.; Ludwik, B.; Chrabaszcz, M.; Šledź, A.; Banasik, M.; Bzymek, M.; Mlynarczyk, K.; et al. Feasibility of implementation of a “simplified, No-X-Ray, no-lead apron, two-catheter approach” for ablation of supraventricular arrhythmias in children and adults. J. Cardiovasc. Electrophysiol. 2014, 25, 866–874. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Wang, Y.; Proietti, R.; Wang, X.; Ouyang, F.; Ma, C.S.; Yu, R.H.; Zhao, C.; Ma, K.; Qiu, J.; et al. Zero-fluoroscopy approach for ablation of supraventricular tachycardia using the Ensite NavX system: A multicenter experience. BMC Cardiovasc. Disord. 2020, 20, 48. [Google Scholar] [CrossRef] [PubMed]
- Kochar, A.; Ahmed, T.; Donnellan, E.; Wazni, O.; Tchou, P.; Chung, R. Operator learning curve and clinical outcomes of zero fluoroscopy catheter ablation of atrial fibrillation, supraventricular tachycardia, and ventricular arrhythmias. J. Interv. Card. Electrophysiol. 2021, 61, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Fadhle, A.; Hu, M.; Wang, Y. The safety and efficacy of zero-fluoroscopy ablation versus conventional ablation in patients with supraventricular tachycardia. Kardiol. Pol. 2020, 78, 552–558. [Google Scholar] [CrossRef]
- Silversides, C.K.; Harris, L.; Haberer, K.; Sermer, M.; Colman, J.M.; Siu, S.C. Recurrence rates of arrhythmias during pregnancy in women with previous tachyarrhythmia and impact on fetal and neonatal outcomes. Am. J. Cardiol. 2006, 97, 1206–1212. [Google Scholar] [CrossRef]
- You, J.; Pagan, E.; Mitra, R. Comparison of minimal versus zero-fluoroscopic catheter ablation in gestational supraventricular arrhythmias. J. Interv. Card. Electrophysiol. 2022, 66, 1423–1429. [Google Scholar] [CrossRef]
- Chen, G.; Sun, G.; Xu, R.; Chen, X.; Yang, L.; Bai, Y.; Yang, S.; Guo, P.; Zhang, Y.; Zhao, C.; et al. Zero-fluoroscopy catheter ablation of severe drug-resistant arrhythmia guided by Ensite NavX system during pregnancy: Two case reports and literature review. Medicine 2016, 95, e4487. [Google Scholar] [CrossRef]
- Kwong, W.; Neilson, A.L.; Chiu, C.C.; Gorss, G.J.; Hamilton, R.M.; Soucie, L.; Stephenson, E.A.; Kirsh, J.A. The effect of NavX on fluoroscopy times in pediatric catheter ablation. J. Interv. Card. Electrophysiol. 2012, 33, 123–126. [Google Scholar] [CrossRef]
- Koca, S.; Paç, F.A.; Eriş, D.; Zabun, M.M.; Özeke, Ö.; Özcan, F. Electroanatomic mapping-guided pediatric catheter ablation with limited/zero fluoroscopy. Anatol. J. Cardiol. 2018, 20, 159–164. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomstrőm-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef] [PubMed]
- Blomström-Lundqvist, C.; Gizurarson, S.; Schwieler, J.; Jensen, S.M.; Bergfeldt, L.; Kennebäck, G.; Rubulis, A.; Malmborg, H.; Raatikainen, P.; Lönnerholm, S.; et al. Effect of Catheter Ablation vs Antiarrhythmic Medication on Quality of Life in Patients with Atrial Fibrillation: The CAPTAF Randomized Clinical Trial. JAMA 2019, 321, 1059–1068. [Google Scholar] [CrossRef] [PubMed]
- Mark, D.B.; Anstrom, K.J.; Sheng, S.; Piccini, J.-P.-; Baloch, K.N.; Monahan, K.H.; Daniels, M.R.; Bahnson, T.D.; Poole, J.E.; Rosenberg, Y.; et al. Effect of Catheter Ablation vs Medical Therapy on Quality of Life Among Patients with Atrial Fibrillation: The CABANA Randomized Clinical Trial. JAMA 2019, 321, 1275–1285. [Google Scholar] [CrossRef] [PubMed]
- Gerber, T.C.; Carr, J.J.; Arai, A.E.; Dixon, R.L.; Ferrari, V.A.; Gomes, A.S.; Heller, G.V.; McCollough, C.H.; McNitt-Gray, M.F.; Metteler, F.A.; et al. Ionizing radiation in cardiac imaging: A science advisory from the American Heart Association Committee on Cardiac Imaging of the Council on Clinical Cardiology and Committee on Cardiovascular Imaging and Intervention of the Council on Cardiovascular Radiology and Intervention. Circulation 2009, 119, 1056–1065. [Google Scholar] [CrossRef] [PubMed]
- Metzner, A.; Straube, F.; Tilz, R.R.; Kuniss, M.; Noelker, G.; Tebbenjohanns, J.; Andresen, D.; Wieneke, H.; Stellbrink, C.; Franke, J.; et al. Electrophysiology lab efficiency comparison between cryoballoon and point-by-point radiofrequency ablation: A German sub-analysis of the FREEZE Cohort study. BMC Cardiovasc. Disord. 2023, 23, 8. [Google Scholar] [CrossRef]
- Ferguson, J.D.; Helms, A.; Mangrum, J.M.; Mahapatra, S.; Mason, P.; Bilchick, K.; McDaniel, G.; Wiggins, D.; DiMarco, J.P. Catheter ablation of atrial fibrillation without fluoroscopy using intracardiac echocardiography and electroanatomic mapping. Circ. Arrhythm. Electrophysiol. 2009, 2, 611–619. [Google Scholar] [CrossRef]
- Lurie, A.; Amit, G.; Divakaramenon, S.; Acosta, J.G.; Healey, J.S.; Wong, J.A. Outcomes and Safety of Fluoroless Catheter Ablation for Atrial Fibrillation. CJC Open 2021, 3, 303–310. [Google Scholar] [CrossRef]
- Khaykin, Y.; Oosthuizen, R.; Zarnett, L.; Wulffhart, Z.A.; Whaley, B.; Hill, C.; Giewercer, D.; Verma, A. CARTO-guided vs. NavX-guided pulmonary vein antrum isolation and pulmonary vein antrum isolation performed without 3-D mapping: Effect of the 3-D mapping system on procedure duration and fluoroscopy time. J. Interv. Card. Electrophysiol. 2011, 30, 233–240. [Google Scholar] [CrossRef]
- Alyesh, D.; Venkataraman, G.; Stucky, A.; Joyner, J.; Choe, W.; Sundaram, S. Acute Safety and Efficacy of Fluoroless Cryoballoon Ablation for Atrial Fibrillation. J. Innov. Card. Rhythm. Manag. 2021, 12, 4413–4420. [Google Scholar] [CrossRef]
- Ahn, J.; Shin, D.G.; Han, S.J.; Lim, H.E. Safety and efficacy of intracardiac echocardiography-guided zero-fluoroscopic cryoballoon ablation for atrial fibrillation: A prospective randomized controlled trial. Europace 2023, 25, euad086. [Google Scholar] [CrossRef]
- Spector, P.; Reynolds, M.R.; Calkins, H.; Sondhi, M.; Xu, Y.; Martin, A.; William, C.J.; Sledge, I. Meta-analysis of ablation of atrial flutter and supraventricular tachycardia. Am. J. Cardiol. 2009, 104, 671–677. [Google Scholar] [CrossRef] [PubMed]
- Ko Ko, N.L.; Sriramoju, A.; Khetarpal, B.K.; Srivathsan, K. Atypical atrial flutter: Review of mechanisms, advances in mapping and ablation outcomes. Curr. Opin. Cardiol. 2022, 37, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Willems, S.; Kautzner, J.; De Chillou, C.; Wiedemann, M.; Schepel, S.; Piorkowski, C.; Risius, T.; Kottkamp, H.; EuroFlutter Investigators. Effect of electroanatomically guided versus conventional catheter ablation of typical atrial flutter on the fluoroscopy time and resource use: A prospective randomized multicenter study. J. Cardiovasc. Electrophysiol. 2009, 20, 734–740. [Google Scholar] [CrossRef] [PubMed]
- Willems, S.; Weiss, C.; Ventura, R.; Rüppel, R.; Risius, T.; Hoffmann, M.; Meinertz, T. atheter ablation of atrial flutter guided by electroanatomic mapping (CARTO): A randomized comparison to the conventional approach. J. Cardiovasc. Electrophysiol. 2000, 11, 1223–1230. [Google Scholar] [CrossRef]
- Bencsik, G.; Pap, R.; Makai, A.; Kalusz, G.; Chadaide, S.; Traykov, V.; Forster, T.; Sághy, L. Randomized trial of intracardiac echocardiography during cavotricuspid isthmus ablation. J. Cardiovasc. Electrophysiol. 2012, 23, 996–1000. [Google Scholar] [CrossRef]
- Turcsan, M.; Janosi, K.F.; Debreceni, D.; Toth, D.; Bocz, B.; Simor, T.; Kupo, P. Intracardiac Echocardiography Guidance Improves Procedural Outcomes in Patients Undergoing Cavotricuspidal Isthmus Ablation for Typical Atrial Flutter. J. Clin. Med. 2023, 12, 6277. [Google Scholar] [CrossRef] [PubMed]
- Herman, D.; Osmancik, P.; Zdarska, J.; Prochazkova, R. Routine use of intracardiac echocardiography for atrial flutter ablation is associated with reduced fluoroscopy time, but not with a reduction of radiofrequency energy delivery time. J. Atr. Fibrillation. 2017, 10, 1553. [Google Scholar] [CrossRef]
- Jacinto, S.; Silva Cunha, P.; Portugal, G.; Valente, B.; Coutinho Cruz, M.; Lousinha, A.; Veiga, J.; Delgago, A.S.; Bras, M.; Paulo, M.; et al. Fluoroless cavotricuspid isthmus radiofrequency ablation of typical atrial flutter achieves success with zero radiation and shorter procedural duration. Europace 2022, 24 (Suppl. 1), euac053.066. [Google Scholar] [CrossRef]
- Zeppenfeld, K.; Tfelt-Hansen, J.; de Riva, M.; Winkel, B.G.; Behr, E.R.; Blom, N.A.; Charron, P.; Corrado, D.; Dagres, N.; de Chillou, C.; et al. 2022 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur. Heart J. 2022, 43, 3997–4126. [Google Scholar] [CrossRef]
- Rivera, S.; Vecchio, N.; Ricapito, P.; Ayala-Paredes, F. Non-fluoroscopic catheter ablation of arrhythmias with origin at the summit of the left ventricle. J. Interv. Card. Electrophysiol. 2019, 56, 279–290. [Google Scholar] [CrossRef]
- Lamberti, F.; Di Clemente, F.; Remoli, R.; Bellini, C.; De Santins, A.; Mercurio, M.; Dottori, S.; Gasparone, A. Catheter ablation of idiopathic ventricular tachycardia without the use of fluoroscopy. Int. J. Cardiol. 2015, 190, 338–343. [Google Scholar] [CrossRef]
- Sadek, M.M.; Ramirez, F.D.; Nery, P.B.; Golian, M.; Redpath, C.J.; Nair, G.M.; Birnie, D.H. Completely nonfluoroscopic catheter ablation of left atrial arrhythmias and ventricular tachycardia. J. Cardiovasc. Electrophysiol. 2019, 30, 78–88. [Google Scholar] [CrossRef] [PubMed]
- Alyesh, D.; Choe, W.; Demo, H.; Razminia, M.; Sundaram, S. The Advanced Application of Intracardiac Echocardiography for Cardiac Electrophysiology Ablation Procedures. Curr. Cardiol. Rep. 2022, 24, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Ozyilmaz, I.; Ergul, Y.; Akdeniz, C.; Ozturk, E.; Tanidir, I.C.; Tuzcu, V. Catheter ablation of idiopathic ventricular tachycardia in children using the EnSite NavX system with/without fluoroscopy. Cardiol. Young. 2014, 24, 886–892. [Google Scholar] [CrossRef] [PubMed]
- Kloosterman, E.M.; Yamamura, K.; Alba, J.; Mitrani, R.D.; Myerburg, R.J.; Interian, A. An innovative application of anatomic electromagnetic voltage mapping in a patient with Ebstein’s anomaly undergoing permanent pacemaker implantation. J. Cardiovasc. Electrophysiol. 2000, 11, 99–101. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Granell, R.; Ferrero, A.; Morell-Cabedo, S.; Martinez-Brotons, A.; Bertomeu, V.; Llacer, A.; Garcia-Civera, R. Implantation of single-lead atrioventricular permanent pacemakers guided by electroanatomic navigation without the use of fluoroscopy. Europace 2008, 10, 1048–1051. [Google Scholar] [CrossRef]
- Ruiz-Granell, R.; Morell-Cabedo, S.; Ferrero-De-Loma, A.; García-Civera, R. Atrioventricular node ablation and permanent ventricular pacemaker implantation without fluoroscopy: Use of an electroanatomic navigation system. J. Cardiovasc. Electrophysiol. 2005, 16, 793–795. [Google Scholar] [CrossRef]
- Del Greco, M.; Marini, M.; Bonmassari, R. Implantation of a biventricular implantable cardioverter-defibrillator guided by an electroanatomic mapping system. Europace 2012, 14, 107–111. [Google Scholar] [CrossRef]
- Attanasio, P.; Mirdamadi, M.; Wielandts, J.Y.; Pieske, B.; Blaschke, F.; Boldt, L.H.; Jais, P.; Haverkamp, W.; Huemer, M. Safety and efficacy of applying a low-dose radiation fluoroscopy protocol in device implantations. Europace 2017, 19, 1364–1368. [Google Scholar] [CrossRef]
- Attanasio, P.; Schreiber, T.; Parwani, A.; Lacour, P.; Pieske, B.; Haverkamp, W.; Blaschke, F.; Huemer, M. The effect of an ultra-low frame rate and antiscatter grid-less radiation protocol for cardiac device implantations. Pacing Clin. Electrophysiol. 2017, 40, 1380–1383. [Google Scholar] [CrossRef]
- Liang, J.J.; Hebl, V.B.; DeSimone, C.V.; Madhavan, M.; Nanda, S.; Kapa, S.; Maleszewski, J.J.; Edwards, W.D.; Reeder, G.; Cooper, L.T.; et al. Electrogram guidance: A method to increase the precision and diagnostic yield of endomyocardial biopsy for suspected cardiac sarcoidosis and myocarditis. JACC Heart Fail. 2014, 2, 466–473. [Google Scholar] [CrossRef] [PubMed]
- Casella, M.; Dello Russo, A.; Bergonti, M.; Catto, V.; Conte, E.; Sommariva, E.; Gasperetti, A.; Vettor, G.; Tundo, F.; Sicuso, R.; et al. Diagnostic Yield of Electroanatomic Voltage Mapping in Guiding Endomyocardial Biopsies. Circulation 2020, 142, 1249–1260. [Google Scholar] [CrossRef]
- Blomström Lundqvist, C.; Auricchio, A.; Brugada, J.; Boriani, G.; Bremerich, J.; Cabrera, J.A.; Frank, H.; Gutberlet, M.; Hedbuchel, H.; Kuck, K.H.; et al. The use of imaging for electrophysiological and devices procedures: A report from the first European Heart Rhythm Association Policy Conference, jointly organized with the European Association of Cardiovascular Imaging (EACVI), the Council of Cardiovascular Imaging and the European Society of Cardiac Radiology. Europace 2013, 15, 927–936. [Google Scholar] [CrossRef] [PubMed]
- Marini, M.; Ravanelli, D.; Guarracini, F.; Del Greco, M.; Quintarelli, S.; Cima, A.; Coser, A.; Martin, M.; Valentini, A.; Bonmassari, R. A Cost-Effective Analysis of Systematically Using Mapping Systems During Catheter Ablation Procedures in Children and Teenagers. Pediatr. Cardiol. 2018, 39, 1581–1589. [Google Scholar] [CrossRef] [PubMed]
- Marini, M.; Ravanelli, D.; Martin, M.; Del Greco, M.; Guarracini, F.; Quintarelli, S.; Coser, A.; Valentini, A.; Bonmassari, R. An Economic Analysis of the Systematic Use of Mapping Systems during Catheter Ablation Procedures: Single Center Experience. Biomed. Res. Int. 2019, 2019, 2427015. [Google Scholar] [CrossRef] [PubMed]
- Velagic, V.; Mugnai, G.; Prepolec, I.; Pasara, V.; Milinković, A.; Nekić, A.; Bogdanic, J.E.; Posavec, J.P.; Puljević, D.; de Asmundis, C.; et al. Feasibility and safety of reprocessing of intracardiac echocardiography catheters for electrophysiology procedures—A large single center experience. Cardiovasc. Ultrasound 2023, 21, 20. [Google Scholar] [CrossRef] [PubMed]
- Kuniyoshi, R.R.; Sternick, E.B.; Nadalin, E.; Hachul, D.T. Reprocessing of Medical Products in Electrophysiology. Arq. Bras. Cardiol. 2017, 108, 169–172. [Google Scholar] [CrossRef]
- Kosiuk, J.; Fiedler, L.; Ernst, S.; Duncker, D.; Pavlović, N.; Guarguagli, S.; Stegmann, C.; Miskowiec, D.; Garcia, R.; Russo, V.; et al. Fluoroscopy usage in contemporary interventional electrophysiology: Insights from a European registry. Clin. Cardiol. 2021, 44, 36–42. [Google Scholar] [CrossRef]
- De Ponti, R.; Marazzi, R.; Doni, L.A.; Tamborini, C.; Ghiringhelli, S.; Salerno-Uriarte, J.A. Simulator training reduces radiation exposure and improves trainees’ performance in placing electrophysiologic catheters during patient-based procedures. Heart Rhythm. 2012, 9, 1280–1285. [Google Scholar] [CrossRef]
- Percell, R.L.; Pike, J.L.; Olmsted, R.K.; Beideck, J.E.; Nunes, H.L.; Johnson, K.N.; Schaffer, M.; Vachock, L.B.; Sveen, S.M.; Keim, E.J.; et al. The Grand SANS FLUORO (SAy No Series to FLUOROsopy) Study: Examining Fluoroscopy Use in More than 1,000 Ablation Procedures. J. Innov. Card. Rhythm. Manag. 2020, 11, 4224–4232. [Google Scholar] [CrossRef]


{kind=link}
| CARTO | Ensite NavX | RHYTHMIA | |
|---|---|---|---|
| Company | Biosense Webster | Abbott | Boston Scientific |
| Location method | Magnetic field | Electrical and magnetic field | Electrical field |
| Mapping technique | Point-to-point | Point-to-point | Non-contact |
| Compatibility with any catheter | No | Yes | No |
| Patient movement sensibility | High | Low | Low |
| Need for intracardiac reference catheter | No | Yes | Yes |
| Contact-sensing catheters | Force | Electromagnetic | Impedance |
| CT–CMR integration | Yes | Yes | No |
| ICE integration | Yes | No | No |
| Pros |
|
|
|
| Cons |
|
|
|
| Reference | Arrhythmia Treated | No. of Patients (Fluoroless vs. Conventional Fluoroscopy) | Main Findings |
|---|---|---|---|
| Di Cori et al. [61] | SVT/AFL | 93 vs. 116 |
|
| Kalinsek et al. [16] | SVT | 294 vs. 280 |
|
| Bergonti et al. [30] | SVT | 206 vs. 412 |
|
| Casella et al. [39] | SVT | 134 vs. 128 |
|
| Stec et al. [62] | SVT | 179 vs. 714 |
|
| Chen et al. [63] | SVT | 1020 vs. 2040 |
|
| Fadhle et al. [65] | SVT | 100 (Carto) vs. 100 (Ensite) vs. 100 |
|
| Ferguson et al. [76] | AF | 21 |
|
| Lurie et al. [77] | AF | 147 vs. 176 |
|
| Khaykin et al. [78] | AF | 71 (Carto) vs. 165 (Ensite) vs. 197 |
|
| Rivera et al. [90] | TV/PVC | 27 |
|
| Lamberti et al. [91] | TV/PVC | 52 |
|
| Sadek et al. [92] | AF/AFL/VT | 80 |
|
| Alyesh et al. [79] | AF | 50 vs. 50 |
|
| Jinhee et al. [80] | AF | 50 vs. 50 |
|
| Turcsan et al. [86] | AFL | 219 vs. 151 |
|
| Jacinto et al. [88] | AFL | 31 vs. 191 |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Preda, A.; Bonvicini, E.; Coradello, E.; Testoni, A.; Gigli, L.; Baroni, M.; Carbonaro, M.; Vargiu, S.; Varrenti, M.; Colombo, G.; et al. The Fluoroless Future in Electrophysiology: A State-of-the-Art Review. Diagnostics 2024, 14, 182. https://doi.org/10.3390/diagnostics14020182
Preda A, Bonvicini E, Coradello E, Testoni A, Gigli L, Baroni M, Carbonaro M, Vargiu S, Varrenti M, Colombo G, et al. The Fluoroless Future in Electrophysiology: A State-of-the-Art Review. Diagnostics. 2024; 14(2):182. https://doi.org/10.3390/diagnostics14020182
Chicago/Turabian StylePreda, Alberto, Eleonora Bonvicini, Elena Coradello, Alessio Testoni, Lorenzo Gigli, Matteo Baroni, Marco Carbonaro, Sara Vargiu, Marisa Varrenti, Giulia Colombo, and et al. 2024. "The Fluoroless Future in Electrophysiology: A State-of-the-Art Review" Diagnostics 14, no. 2: 182. https://doi.org/10.3390/diagnostics14020182