1. Introduction
A large proportion of patients presenting with typical chest pain and signs of myocardial ischemia is found with non-obstructing epicardial disease, but coronary microvascular dysfunction (CMD) may be present. However, CMD represents a diagnostic challenge; therefore, the purpose of this review is to describe the pathophysiological mechanisms of CMD and the available invasive diagnostic modalities.
Two different invasive tools are currently available for the assessment of coronary microcirculation: Doppler-based and thermodilution-derived tools. For each of them, we will discuss the measurement principles, advantages, and limitations. Finally, we will provide the readers with an overview of the currently available evidence for their use in clinical practice.
2. The Coronary Circulation
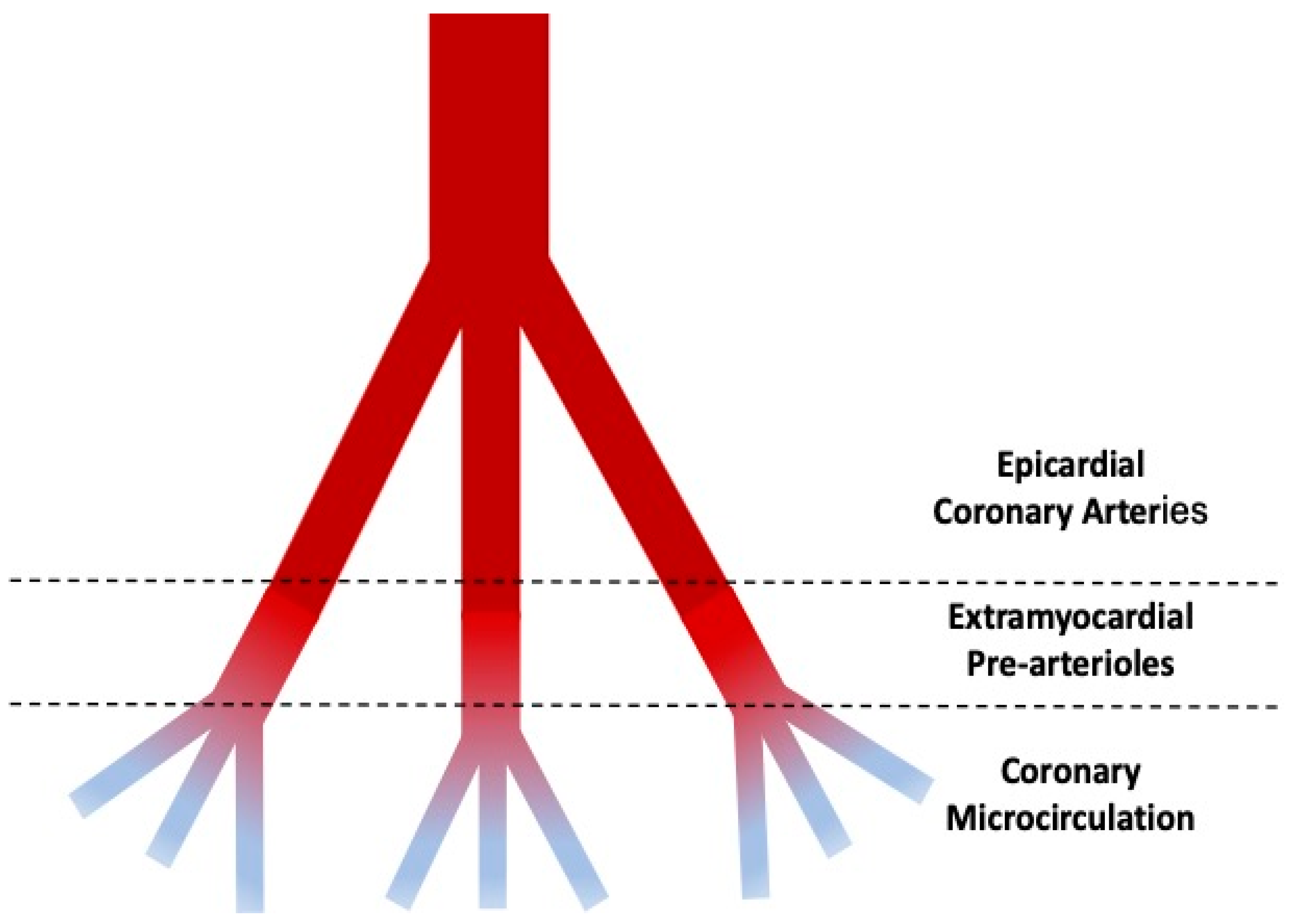
The coronary tree may be virtually divided into three compartments with decreasing size and different functions (
Figure 1) [
1].
The proximal compartment is represented by the epicardial coronary arteries, with a diameter ranging from 5 mm up to 0.5 mm, acting as adaptive vessels and offering just a little resistance to the flow. The intermediate compartment, including pre-arteriolar and arteriolar vessels with a diameter ranging from 0.5 to 0.1 mm, offers the most relevant part of resistance to the flow. The distal compartment is represented by capillaries, with a diameter < 0.1 mm and the function of providing oxygen to the myocardial wall. Intramyocardial pre-arterioles, arterioles, and capillaries constitute the coronary microcirculation.
3. Coronary Microcirculatory Dysfunction
CMD is emerging as a major cause of myocardial ischemia in symptomatic patients without obstructive coronary artery disease (INOCA). It is caused by several disorders affecting the structure and the function of the coronary microcirculation, leading to an inadequate blood supply, finally resulting in myocardial ischemia [
2,
3].
Functional mechanisms responsible for CMD may be related to the presence of an imbalance between vasodilative and constrictor forces acting on the coronary microcirculation. Impaired vasodilation can be caused by endothelium-dependent and/or endothelium-independent mechanisms [
2,
3,
4,
5]. While these latter are probably caused by an impairment of vascular smooth muscle cells (VSMCs) relaxation because of the increased release of vasoconstrictor agonists or the enhanced sensibility to normal vasoconstrictor stimuli, the former is related to endothelial dysfunction, particularly sensible to the cardiovascular risk factors, which may be responsible for a reduced production and/or enhanced degradation of NO and other endothelial-derived relaxation factors, resulting in blunted coronary flow increase or vasoconstriction. Vasomotor abnormalities can be unmasked only during invasive coronary angiography through the administration of intracoronary boluses of acetylcholine. CMD may also be a consequence of diffuse structural alterations such as luminal narrowing of the arterioles and capillaries, perivascular fibrosis, and capillary rarefaction [
3]. In this case, CMD presents with impaired blood flow and increased coronary microvascular resistance during drug-mediated hyperemia. Of note, in some patients, structural remodeling and vasomotor disorders may concur and can even be present in the context of patients presenting with obstructive coronary artery disease. The main endotypes, with their pathophysiological mechanism, are described in
Table 1.
4. The Functional Coronary Angiography
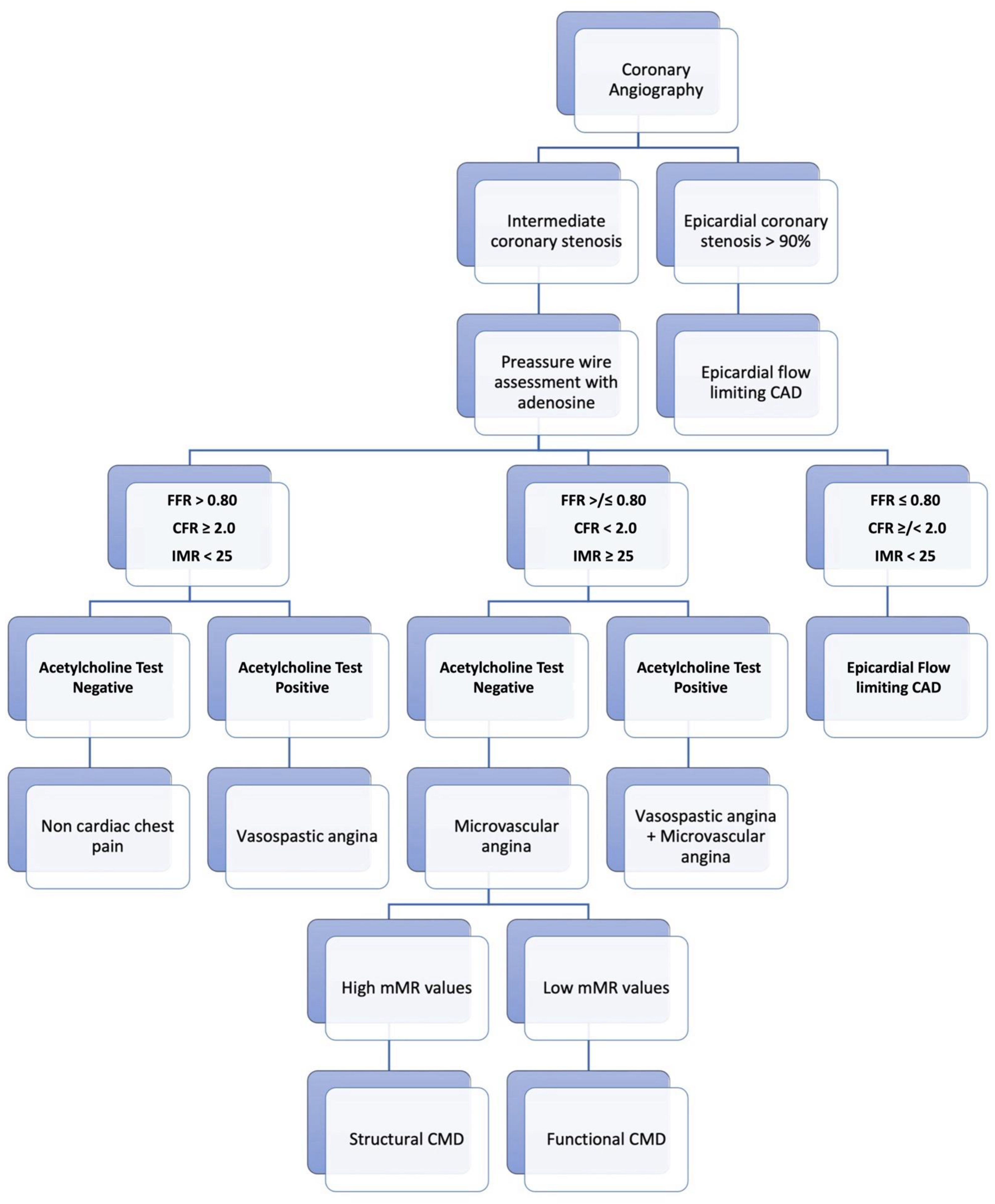
While invasive coronary angiography relies on the visual estimation of the coronary tree, including sometimes the use of quantitative tools such as quantitative coronary angiography (QCA), functional coronary angiography (FCA) requires a direct invasive assessment of both the epicardial disease and the microcirculation, using different tools in combination with a pharmacological reactivity test, according to a “full physiology” approach (
Figure 2) [
6].
Blood flow through the coronary tree is continuously regulated with the aim of delivering an adequate blood and oxygen supply to the myocardium, either at rest or during exercise. The ability of the entire coronary bed to adequately respond to any increased myocardial oxygen demand, maintaining stable myocardial perfusion across a range of perfusion pressures, is called “autoregulation”, and the coronary flow reserve (CFR) describes the ratio by which coronary blood flow can be augmented by exercise, stress, or microcirculatory vasodilation [
7]. Thereby, the measurement of the CFR allows for a comprehensive assessment of both epicardial and microvascular compartments. Of note, when a reduced CFR value is found, either the impaired microcirculation and/or the presence of myocardial bridging, as well as obstructive CAD, can be responsible [
8]. For this reason, several indexes have been proposed to specifically assess the microcirculation, regardless of the presence of any disease of the epicardial compartment. This latter can also be assessed with specific tools able to hemodynamically evaluate the ischemic potential of coronary artery stenoses. The fractional flow reserve (FFR) is a well-validated diagnostic tool for invasively assessing the ischemic potential of the epicardial compartment, and it represents the gold standard for the functional assessment of intermediate coronary artery stenosis [
9,
10,
11,
12,
13,
14]. Functionally significant coronary artery stenosis can be identified with an FFR value ≤ 0.80. Of note, several non-hyperemic indexes requiring no administration of any hyperemic drugs, such as the instantaneous wave-free ratio (iFR) or the resting full-cycle ratio (RFR), have been recently introduced to simplify invasive functional evaluation and enhance clinical adoption [
15,
16,
17,
18]. Although with some limitations, a functionally significant epicardial coronary artery disease can be identified with a value < 0.90 [
19,
20,
21].
In the presence of endothelial dysfunction, a dysregulation of the vasodilatory cascade in coronary resistance vessels may occur. Thus, when myocardial oxygen demands increase, the presence of endothelial dysfunction can be responsible for impaired vasodilation and even paradoxical vasoconstriction of upstream arteries and arterioles. A vasoreactivity test can be performed during FCA to highlight this phenomenon. The most established approach is represented by intracoronary infusion of acetylcholine, which influences coronary vascular tone via muscarinic receptors on endothelial and vascular smooth muscle cells [
22,
23,
24,
25]. Acetylcholine test is currently recommended by the ESC guidelines [
26]. A standard approach involves sequential intracoronary administration of acetylcholine at concentrations increasing from 20 μg up to 200 μg [
22]. However, some limitations associated with provocative tests should be acknowledged, as also clearly indicated by Lanza G.A. et al.: (1) Acetylcholine is normally used to assess endothelium-dependent dilatation; however, it has been shown that it also has a direct constrictor effect on SMCs, potentially contributing to abnormal coronary microvascular responses; (2) A global impairment of SMC relaxation in response to vasodilator substances can lead to a misdiagnosis of endothelium-dependent dilatation. Thereby, in some cases, it might be difficult to definitively attribute CMD to a specific mechanism [
27].
A clinical diagnosis to rule in or rule out microvascular or epicardial spasm is made according to well-established criteria (
Table 2 and
Table 3) [
23,
28].
5. Assessment of Coronary Flow Reserve and Microcirculation
A comprehensive evaluation of the coronary physiology, namely the combination of epicardial and microcirculatory conduits, can be performed by measuring CFR, while several indexes can be measured to evaluate the microcirculation isolated from the upstream epicardial conduit. Although initially used for research purposes only, it is nowadays more often measured, particularly in patients with non-flow-limiting epicardial stenosis. Coronary flow reserve and microcirculation can be assessed using different tools and techniques: Doppler-based tools and thermodilution-based tools.
6. Doppler-Based Tools
Coronary flow velocity measurement by ultrasonic Doppler systems has provided crucial information to modern theories of coronary hemodynamics. A catheter-based Doppler system was previously introduced in the early 1970s by Benchimol, Hartley, and Cole [
29,
30,
31]. Since then, many improvements have been made. The currently used device is a 0.018–0.014” flexible and steerable guidewire with a 12 MHz piezoelectric ultrasound transducer integrated onto its tip and a forward-directed ultrasound beam. It measures flow velocity in a sample volume of 2.25 mm in diameter, at 5.2 mm from its transducer. After the wire crosses the epicardial stenosis, it can assess flow velocity in small and distal branches of the coronary tree. This wire is proximally connected to a real-time spectrum analyzer, which records flow velocity during the whole cardiac cycle. Simultaneously, it can record additional parameters such as ECG track, aortic pressure (Pa), instantaneous spectral peak velocity, and the time average of spectral peak flow velocity (APV—cm/s). Velocity measurements are continuously displayed on the FloMap monitor in a gray-scale spectral pattern. Functional assessment is usually performed in the left anterior descending coronary artery (LAD) since it supplies a larger myocardial mass.
Douchette et al. and Labovitz et al. have previously validated the use of Doppler flow wire for the functional assessment of coronary hemodynamics in vivo by deriving quantitative coronary flow from the product of vessel cross-sectional area and mean velocity, assuming that a linear correlation between the average peak flow velocity (APV) and blood flow exists in straight vessels [
32,
33]. Doppler FloWire has also been used to measure CFR to assess the ischemic potential of intermediate coronary stenosis. CFR is calculated as the ratio between the hyperemic (hyp) APV, measured during drug-induced maximal hyperemia, and resting (rest) coronary flow velocity (APV
hyp/APV
rest). Maximal hyperemia is achieved by i.v. adenosine administration (140 µg/Kg/min). CFR values ≤ 2.5 are considered abnormal, with a negative prognostic value, predicting major cardiovascular events at long-term follow-up [
34,
35].
Doppler flow wire has also been used to directly assess the hyperemic microvascular resistance (HMR—mmHg·cm
−1·s), a microvascular-specific index. This is defined as the ratio between the distal coronary pressure (Pd) and the APV during maximal hyperemia [
36]. Of note, this formula needs to be corrected for collateral flow in case of the presence of obstructive CAD [
37].
However, the cutoff value of HMR for prediction of CMD is still a matter of debate. A study including symptomatic patients with non-obstructive CAD proposed an HMR value ≥ 2.5 to identify patients with CMD [
38].
Minimal microvascular resistance (mMR—mmHg·cm
−1·s) is another Doppler-based invasive method for the assessment of coronary microvascular resistance, and it is calculated by assessing both Pd and APV during the diastolic wave-free (WF) period and during maximal hyperemia, using the following formula:
It has been developed to overcome the limitations of HMR in the presence of obstructive CAD. In this setting, HMR can overestimate microvascular resistance. De Waard et al. showed that mMR provides a reliable evaluation of the coronary microcirculation status, regardless of the presence of epicardial stenosis [
39]. For this reason, mMR can be useful in assessing microvascular disease in patients presenting with either obstructive or non-obstructive coronary artery disease. Moreover, mMR might be used with CFR to discriminate structural from functional CMD. Low CFR and increased mMR values indicate structural CMD. On the contrary, low CFR and reduced mMR values allow the identification of functional CMD [
40].
7. Advantages and Limitations of Doppler-Based Tools
Doppler-based tools provide numerous advantageous features: low operator dependency, low risk for the patient, and high diagnostic accuracy. Doppler devices are also relatively widely available in catheterization laboratories.
Furthermore, the employment of Doppler guidewires results in a minor degree of obstruction in small vessels, causing only a negligible disturbance of Doppler flow velocity profiles. Additionally, when performing percutaneous coronary intervention (PCI), the Doppler wire may serve as both a diagnostic and intervention tool [
32].
Beyond their many advantages, Doppler-based tools require overcoming some limitations. In general terms, both the quality of the Doppler signal and the value of peak velocity are particularly dependent on the correct positioning of the wire, which may limit the use of a Doppler device in large vessels or in segments with variable luminal caliber [
32]. Values obtained with this technique may also differ because of loading conditions (i.e., heart rate, blood pressure, left ventricular contractility) [
38].
When compared to thermodilution-based CFR, Doppler-derived CFR has the advantage of having a greater agreement with oxygen-15-labeled water PET-derived CFR, which is considered to be the gold standard for the quantification of CFR [
41]. The use of HMR is limited by the lack of a determined cutoff value. As previously stated, it is still unclear whether the HMR reference value should be ≥ 1.9 or ≥2.5 [
38]. Both CFR and HMR require adenosine-induced hyperemia. In contrast, i.v.-infused and i.c.-injected adenosine may cause several side effects ranging from negligible to significant. The advantages and limitations of Doppler-based tools are summarized in
Table 4.
8. Clinical Evidence in Non-Acute Scenarios
Myocardial ischemia is due to both epicardial stenoses and microvascular dysfunction, which is emerging as a new pathogenic mechanism responsible for non-obstructive coronary artery disease and several other conditions, including non-ischemic cardiomyopathies, takotsubo syndrome, and heart failure, particularly with preserved or mildly reduced ejection fraction. FloWire can be used to measure both CFR and HMR in order to assess microvascular function when the epicardial compartment is free from obstructive disease [
42]. Increased microvascular resistance is considered a marker of coronary microvascular dysfunction and is associated with worse clinical outcomes.
Feenstra et al. enrolled a cohort of 41 patients presenting with angina, non-obstructive coronary artery disease (<50% luminal obstruction on angiography), FFR > 0.80, and CFR > 2.5 undergoing vasomotor function test. They aimed to establish a reference range for Doppler flow velocity-derived index HMR, and they documented that values equal to or higher than 2.5 mmHg/cm/s can identify increased microvascular resistance and, therefore, microvascular dysfunction, regardless of patients’ clinical features [
43].
Both Doppler wire-derived CFR (CFR
doppler) and HMR have been respectively compared with thermodilution-derived CFR (CFR
thermo) and IMR. Demir et al. enrolled 250 vessels (149 patients) in their study. A modest correlation was found between CFR
thermo and CFR
doppler (r
2 = 0.36;
p < 0.0001). In particular, CFR
thermo overestimates CFR
doppler (mean 2.59 ± 1.46 vs. 2.05 ± 0.89;
p < 0.0001). In addition, a CFR
thermo threshold of 2.0 had poor sensitivity for identifying vessels with diminished CFR, but using the same Doppler threshold (<2.5), diagnostic accuracy increased [
44]. Williams et al. compared HMR vs. IMR and both with independent measurements of CMD. A total of 54 patients (61 ± 10 years) who underwent cardiac catheterization for stable coronary artery disease (
n = 10) or acute myocardial infarction (
n = 44) were enrolled. They found that an HMR of ≥2.5 mmHg/cm/sec and an IMR from 21.5 to 24 were optimal thresholds to define CMD compared to the average values of CFR
thermo and CFR
doppler and cardiac magnetic resonance (CMR) [
38]. Moreover, HMR showed better diagnostic accuracy compared to IMR, CFR (both CFR
doppler and CFR
thermo), and CMR in detecting CMD.
9. Clinical Evidence in Acute Scenarios
In the setting of acute coronary syndromes (ACS), up to 50% of patients presenting with ST segment elevation myocardial infarction (STEMI) develop microvascular injury (MVI) despite angiographically successful primary percutaneous coronary intervention (PCI). Different pathogenic mechanisms after coronary revascularization play a role, such as distal embolization of the thrombus, endothelial dysfunction, reperfusion injury, and intramyocardial hemorrhage.
In this setting, Doppler FloWire can be used to detect patients who still have impaired flow at the myocardial microcirculatory and after percutaneous revascularization. Microvascular obstruction (MVO) occurs with reduced coronary flow velocity reserve, systolic flow velocity reversal, and a short diastolic deceleration time. A correct diagnosis of MVO could lead these patients to benefit from adjunctive therapy after primary PCI.
Teunissen et al. demonstrated that in patients presenting with STEMI, HMR values > 2.5 mmHg/cm/s correlate with MVI (as assessed by CMR) and with decreased PET myocardial blood flow after primary PCI. Microvascular resistance indexes can be immediately performed in a catheterization laboratory, allowing for an early risk stratification and management of microvascular damage, whereas CMR and PET are usually only performed after the index procedure. The role of HMR on long-term clinical outcomes in patients with STEMI undergoing PCI was investigated for the first time by Jin et al. In this study, HMR was found to be a strong predictor of long-term major adverse cardiovascular events [
45].
An additional study by de Waard et al. demonstrated that HMR is more reliable in identifying patients with ACS and high risk of adverse clinical events immediately after primary percutaneous revascularization, compared to CFR
doppler. Indeed, HMR > 3.0 mmHg/cm/s had a predictive value for the composite end point (HR 7.0; 95% CI 1.5 to 33.7) as well as both individual components (death and hospitalization for heart failure), whereas CFR
doppler only had it for the composite endpoint (HR 7.0; 95% CI 1.5 to 33.7) [
46].
Finally, in a recent metanalysis by Canu et al., it was confirmed that severe CMD, defined as IMR > 40 mmHg or HMR > 3 mmHg/cm/s, was associated with increased risk of long-term adverse cardiovascular events in patients with STEMI, suggesting that both IMR and HMR can have an important prognostic role and guide therapeutic approach [
47].
10. Thermodilution-Based Tools
Indicator-dilution theory and the “Stewart-Hamilton” equation represent the basis for measuring the flow in a human district [
48,
49]. The “indicator” can be represented by a traceable substance with physical properties (i.e., temperature, pH) that can be measured while diluted with blood. In addition, a specific device is also required to measure the “passage” of the indicator during time. This theory is normally applied for the assessment of the cardiac output, which is measured with a Swan–Ganz catheter placed in the pulmonary artery, which can measure the variations of blood temperature during the time and allows injecting saline at room temperature as a “colder than blood” indicator.
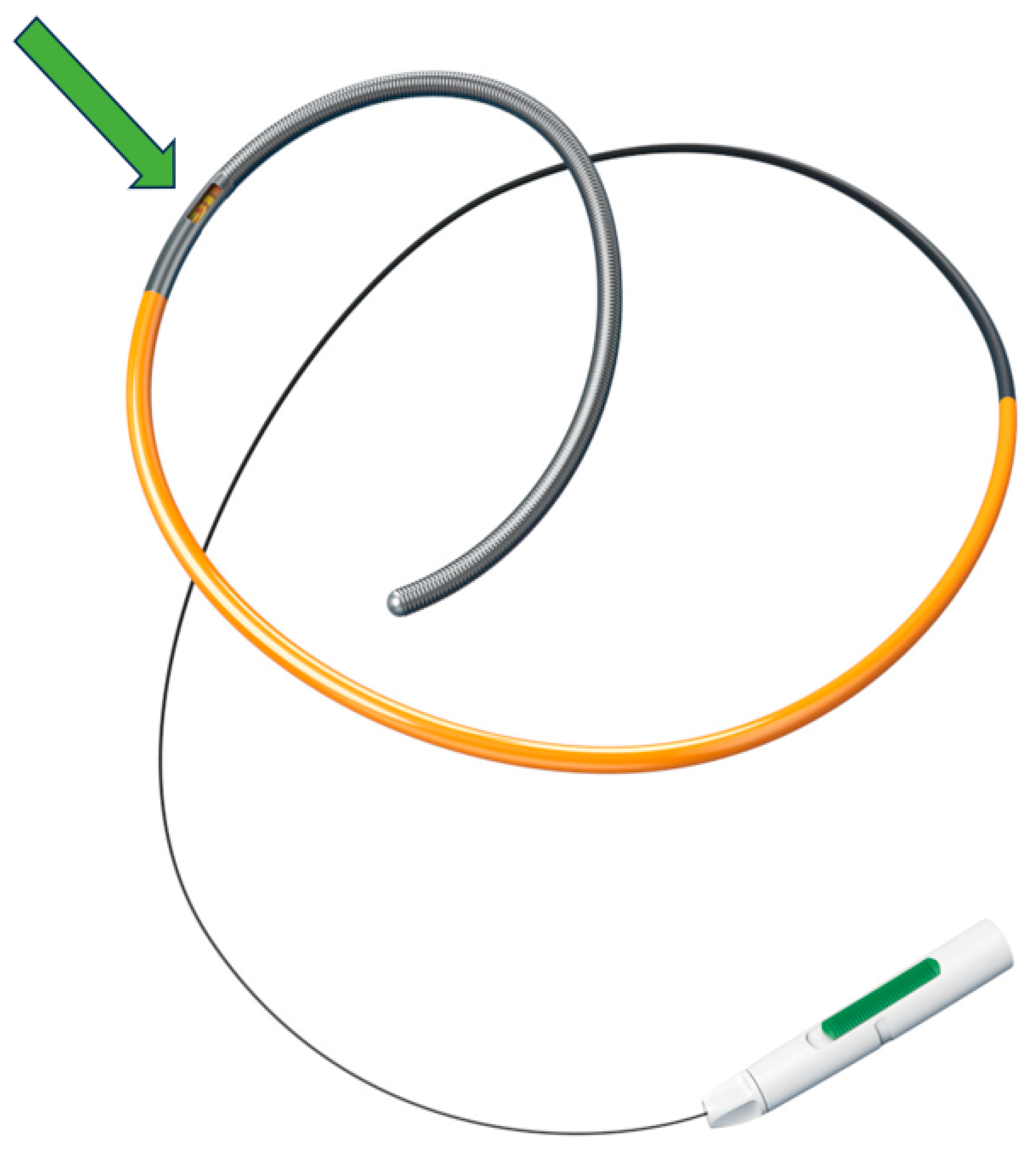
In the coronary system, the colder-than-blood indicator can be administered either as a bolus injection or continuous infusion. In both cases, a specific pressure–temperature coronary wire must be used to detect both the distal coronary pressure and the temperature difference while the indicator is diluted (
Figure 3).
11. Thermodilution by Bolus Injection
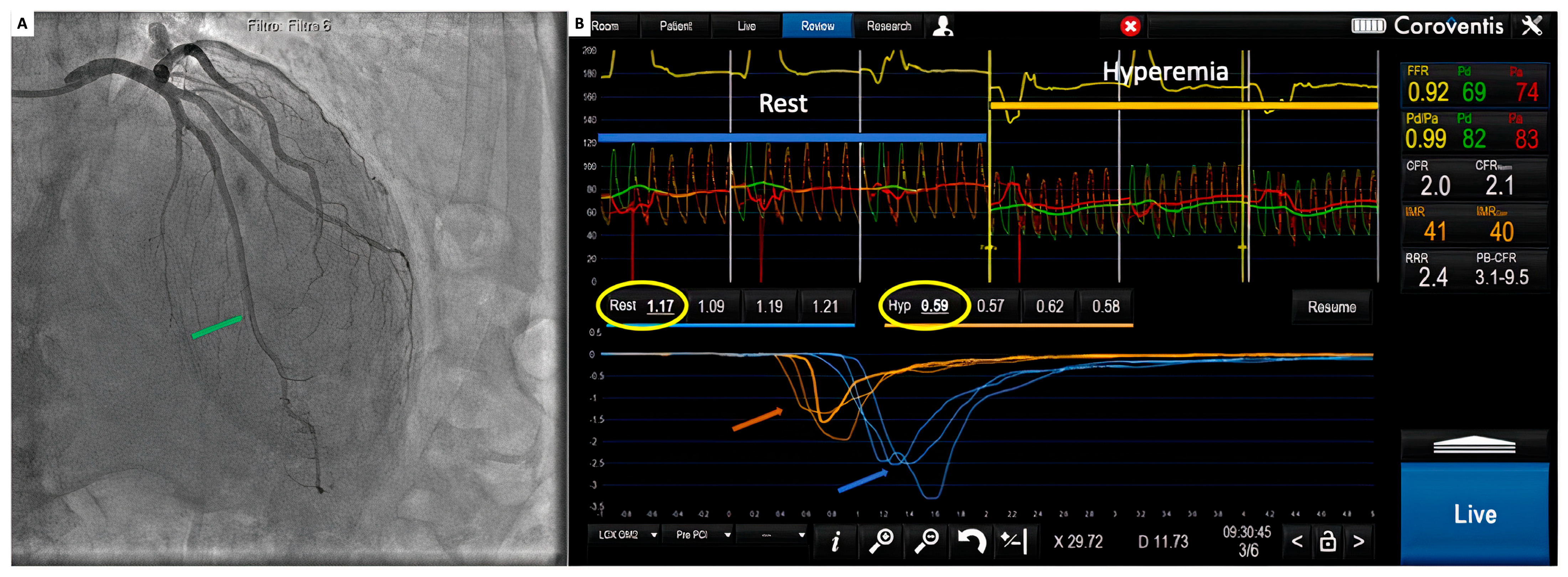
With a 6 Fr guiding catheter positioned in the coronary ostium, a 0.014″ floppy pressure–temperature coronary guidewire is advanced through the coronary artery, after equalization, and located as distal as possible into the target vessel. Thermodilution curves can be obtained with a short manual injection of 3 to 5 mL of saline at room temperature, and a time-based temperature change can be recorded in the distal part of the artery (
Figure 4).
Because of the low reproducibility, measurements must be performed three times, taking care not to move the wire during the injections, during two different periods: at baseline and during maximal hyperemia [
50].
When bolus thermodilution is used to assess coronary flow, the exact volume of the indicator is not known. In fact, a portion of the injected saline can go lost in the aorta during bolus injection. In this case, the coronary flow (Q−mL/s) can be approximately calculated by dividing the vascular volume (V−in mL) by the mean transit time of the indicator (Tmn; in seconds):
However, vascular volume (V) is also unknown, but it can be considered constant during consecutive measurements and under hyperemic conditions. In this case, Tmn can be considered inversely proportional to Q:
The mean transit time (Tmn) can be finally calculated from thermodilution curves and, as the index of flow, when measured both at rest and during maximal hyperemia, it can be used to calculate coronary flow reserve (CFR):
Experimental models have previously found a significant agreement between bolus thermodilution-based CFR and Doppler-based CFR [
50,
51]. Furthermore, CFR
thermo is also technically easier to perform than CFR
doppler [
52].
Commonly, a value lower than 2 is considered abnormal, providing also a prognostic role. However, more recently, some authors suggested using a cutoff of 2.5, which is similar to the one suggested for the CFR
Doppler in order to improve the diagnostic accuracy [
35].
Bolus thermodilution can also be used to directly evaluate the microvascular compartment through the assessment of the index of microcirculatory resistance (IMR), which is defined as the ratio of the distal coronary pressure and the inverse of Tmn during maximal hyperemia:
This index was introduced to specifically evaluate the microvascular resistance as a single compartment independent of the epicardial section, thereby specific for coronary microcirculation regardless of the presence of epicardial disease. In an animal model, Fearon and colleagues showed a suitable correlation between IMR and true microcirculatory resistance (TMR), defined as distal coronary pressure divided by absolute coronary flow during maximal hyperemia. In addition, IMR was able to distinguish between normal and abnormal microcirculatory function, this latter simulated using embolized microspheres [
53].
12. Catheterization Protocol
With a 6 Fr guiding catheter placed in the coronary ostium, a 0.014″ floppy pressure–temperature guidewire is connected to the pressure analyzer and calibrated outside the body, then it is advanced to the tip of the guiding catheter to check the equality of pressure signals. The guide catheter is flushed with saline, clearing all contrast, and after the equalization, the temperature signal is calibrated so the temperature at the coronary ostium is taken as a reference for measurements. Next, the wire is advanced into the coronary artery and located as distally as possible in the target vessel. At this point, three boluses of 3 to 5 mL of saline at room temperature are injected both at baseline and during maximal hyperemia, normally obtained with intravenous infusion of adenosine. In this way, two couples of triple thermodilution curves can be produced, representing each of them the mean transit time values obtained three times at baseline and during hyperemia. At the same time, both Pa and Pd are recorded at rest and during maximal hyperemia. In this way, FFR, CFR, and IMR are all measured at the same time, allowing the operator to contemporarily assess the epicardial compartment and the coronary microcirculation [
51,
53,
54].
13. Advantages and Limitations of Bolus Thermodilution
Thermodilution-derived CFR tends to incorporate the same limitations of Doppler-derived CFR: containing resting flow in its mathematical formula, any hemodynamic change, such as different loading conditions or epicardial coronary artery disease, may result in a lack of reproducibility and a greater degree of variability [
54].
Both CFR and IMR require adenosine-induced hyperemia, with the potential side effects already mentioned. Unlike CFR, IMR values are not altered by different hemodynamic states.
Although being performed through manual indicator injections, IMR values measurement remain consistent, with remarkable intraoperator and interoperator reproducibility. Furthermore, Tmn persists to be stable regardless of the indicator temperature or volume injected [
41].
Unless subocclusive, epicardial coronary stenosis results in a negligible alteration of IMR values. In this case, due to an underestimation of coronary flow, IMR measurements obtained may be falsely higher. To overcome this limitation, it is necessary to take into account collateral flow by assessing coronary wedge pressure (Pw) and integrating the result in a new formula, as follows:
Lastly, Tmn can vary according to the distance of the thermistor from the ostium of the coronary artery; hence, movement of the sensor greater than 2 cm might disrupt Tmn evaluation [
54]. The advantages and limitations of bolus thermodilution are summarized in
Table 4.
14. Clinical Evidence in Non-Acute Scenarios
Patients experiencing chest pain often show non-obstructive epicardial coronary artery disease during invasive coronary angiography (ICA). These patients may present with exertional angina; noninvasive tests positive for the evidence of inducible ischemia; or either no epicardial stenosis, as previously stated, or mild to moderate stenosis (ranging from 40 to 60%) unfolded by ICA or computed tomography angiography (CTA), that are accounted to be functionally not significant [
26].
In this subset of patients, CMD is strikingly prevalent [
41]. This condition is mainly linked to women [
55], associated with poor clinical outcomes, and deserves targeted therapy. In 2003, Fearon et al. established the index of microvascular resistance as the first index to assess specifically the microcirculation [
53]. In apparently healthy subjects, several examinations suggested that normal IMR reference values are generally lower than 25 [
54,
55].
In 2015, Lee et al. [
56] assessed IMR in 1096 patients, demonstrating different cutoff values for each major coronary artery: 22.0 for the left anterior descending (LAD) coronary artery, 24.0 in the circumflex coronary artery, and 28.0 in the right coronary artery (RCA). The greater value detected in the RCA might be related either to the longer length of the vessel (and consequently to a longer mean transit time) or the smaller amount of subtended myocardial mass [
57].
Medical therapy, stratified according to an invasive physiologic assessment consisting of IMR and CFR, can improve typical chest pain relief after 6 months in patients with angina and non-obstructive coronary artery disease compared with standard care [
25].
In addition, IMR can serve as a predictor of myocardial injury after percutaneous coronary intervention. In patients presenting with chronic coronary syndrome, higher IMR values (detected pre- and post-PCI) are strong predictors of the occurrence of type 4a myocardial infarction [
58].
15. Clinical Evidence in Acute Scenarios
When employed in acute scenarios, such as STEMI, and performed after a successful primary PCI, IMR can predict the presence of MVO, the extension of the infarct size, and which patients are at risk of major cardiac complications within 30 days [
41]. MVO is the leading mechanism of no reflow, causing the persistence of deteriorated myocardial perfusion in patients presenting with STEMI who have already undergone a successful epicardial recanalization of the culprit coronary artery [
59].
CMR is often regarded as the gold standard for assessing MVO but is not always easily available and performed after the acute phase. It may provide the proper information but not right after the coronary revascularization, i.e., when it is most needed [
60]. On the other hand, IMR can be readily measured in the catheterization laboratory and could allow for earlier administration of adjunctive therapy [
54].
Ahn et al. investigated the predictive accuracy of invasive microvascular indexes, such as IMR and CFR
thermo, for identifying MVO versus CMR in patients presenting with STEMI undergoing primary PCI. IMR and CFR
thermo were assessed in 40 STEMI patients soon after successful primary PCI and compared with CMR assessed within 7 days. The investigators found that high IMR values and low CFR
thermo values were associated with MVO. In contrast, low IMR values and high CFR
thermo values suggested preserved microvascular function. The combination of both indexes performed better than the use of one of them [
61].
16. Thermodilution by Continuous Infusion
The assessment of microvascular resistance based on actual coronary blood flow measurements has recently become possible by continuous thermodilution with intracoronary saline infusion, using a pressure–temperature guidewire and an infusion microcatheter. The method was validated in vitro, in animals, and in humans [
62,
63].
Recent improvements in hardware and software enabled the technique to be introduced into routine clinical practice [
64,
65]. The basic principle of continuous thermodilution has been recently validated and proved to be operator independent; furthermore, it is not necessary to use pharmacological agents to induce maximal hyperemia [
66]. In fact, a recent study indicates that saline-induced hyperemia is mediated by hemolysis, either by rupture or deformation of red blood cells (RBCs), and suggests that vasodilatory compounds, including ATP and NO, are released locally from RBCs and are ultimately responsible for maximal steady-state vasodilation [
67].
Absolute blood flow can be calculated with the following equation:
where Q represents the hyperemic coronary blood flow (mL/min);
represents the indicator flow (saline at room temperature—mL/min); T represents the difference in temperature in °C between body temperature (calibrated to 0) and the mixture of blood and saline, and it is measured by the pressure wire in the distal part of the coronary artery;
represents the difference in temperature in °C between body temperature and saline only, and it measured when the pressure wire is pulled back in the infusion catheter. The constant 1.08 accounts for the densities and specific heat of blood and saline [
41]. Pd is also recorded simultaneously, so microvascular resistance (R) can be calculated by dividing distal pressure and flow according to the following equation:
All signals are instantaneously recorded by a dedicated software (Coroflow
® v3.0 Coroventis, Uppsala, Sweden), which can measure all pressure parameters, fractional flow reserve as well as absolute blood flow in mL/min and microvascular resistance in mmHg/L/min or wood units (WU) (
Figure 5).
Moreover, continuous thermodilution with infusion of saline at the low rate of 10/mL allows for the assessment of CFR (CFR
abs) and microvascular resistance reserve (MRR). CFR
abs is calculated by dividing Q during maximal hyperemia (Q
h) and Q at rest (Q
r):
MRR is calculated according to the formula shown by De Bruyne et al., as follows:
and it can be assessed both with bolus and continuous thermodilution methods. However, hyperemic Pa (Pa
hyp) can be lower when assessed by bolus thermodilution because of adenosine administration, as compared with continuous infusion. Thereby, an overestimation of the MRR values might occur with bolus thermodilution [
68].
Interestingly, Jansen et al. demonstrated that, unlike bolus thermodilution-derived CFR and MRR, absolute flow measurements correlate well with angina severity and overall quality of life [
69].
17. Catheterization Protocol
Cardiac catheterization and FFR measurement can be performed as usual by either radial or femoral access. Guiding catheters and a pressure/temperature wire (Pressure wire X™, Abbott, Saint Paul, MN, USA) can be manipulated as a regular practice. After the intracoronary administration of 200 micrograms of nitroglycerin and proper equalization of pressures, the pressure wire can be advanced into the coronary artery. A dedicated monorail infusion catheter (Rayflow™, Hexacath, Paris, France) can be advanced over the pressure wire and positioned with its tip at the proximal part of the coronary artery [
70]. This infusion catheter (2.5 French) consists of a 25 cm long rapid exchange inner monorail lumen for the 0.014″ wire, and it is equipped with four infusion holes guaranteeing rapid and complete mixing of saline with blood in the coronary artery. In addition, the infusion catheter has two inner side holes, which allow the recording of the temperature of saline at the site where it enters the coronary artery. Before saline infusion starts, the temperature is calibrated, and body temperature is set to “zero” (reference temperature); thereafter, all changes in temperature are related to this reference temperature (
Figure 5). During the measurement, the pressure–temperature sensor of the pressure wire is positioned in the distal part of the coronary artery. Then, saline infusion is started at the rate of 10 to 20 mL/min, inducing maximal hyperemia within 10–20 s. After obtaining a steady state, the temperature of the completely mixed blood and saline (T) is measured in the distal coronary artery; the pressure/temperature wire is pulled back into the tip of the infusion catheter to measure the saline temperature (Ti) [
71].
18. Advantages and Limitations of Continuous Thermodilution
The continuous thermodilution method showed several advantages over other coronary assessment techniques. Primarily, it has been demonstrated to be safe and reproducible [
72]. Xaplanteris et al. observed no significant periprocedural adverse events in 203 absolute coronary blood flow (Q) and resistance (R) measurements in 135 patients undergoing clinically indicated coronary angiography [
65]. A small percentage (8.1%) of patients experienced transient bradycardia and concomitant atrioventricular block, which were reversed immediately upon interruption of the infusion.
Keulards et al. observed one catheter-induced coronary dissection requiring percutaneous coronary intervention in 467 absolute Q and R measurements from 100 consecutive patients undergoing clinically indicated invasive fractional flow reserve measurements [
73]. They observed only 2.6% cases of bradycardia and atrioventricular block and two patients experiencing transient chest discomfort during infusion without electrocardiographic abnormalities. Xaplanteris et al. also assessed reproducibility in their cohort [
65]. Duplicate measurements were performed in 80 patients, which had a strong correlation both for Q (ρ = 0.841;
p < 0.001; ICC: 0.89;
p < 0.001) and R (ρ = 0.780;
p < 0.001; ICC: 0.89;
p < 0.001). This methodology is operator independent, and it does not require adenosine infusion because saline infusion directly induces maximal hyperemia. Of note, differently from adenosine-induced hyperemia, the one induced by saline infusion does not cause chest discomfort in most patients [
73]. Another strength of continuous thermodilution is that it has been validated against the current gold standard for flow assessment, PET-TC [
74].
However, there are limitations associated with this microvascular assessment method, the most important of which is that there is significant interpatient variability in Q and R during hyperemia owing to the difference in the vascular territory supplied and, hence, correction for myocardial mass using computed tomography may be needed, and no well-accepted normal values are available [
74,
75]. Moreover, the clinical impact of the hemolysis process is yet to be fully assessed.
In a recent sub-study by Jansen et al., 73 patients underwent coronary functional tests (acetylcholine test, CFR
thermo, IMR, Q, and R) at baseline and after 6 weeks. Continuous thermodilution-derived Q and R show better reproducibility than CFR and IMR [
76]. The advantages and limitations of this technique are summarized in
Table 4.
19. Clinical Evidence in Non-Acute Scenarios
Konst et al. have explored the relation between Q and R and CFR and IMR and the relation with self-reported angina. In 84 enrolled patients, they found that the absolute R value was higher in patients with CMD, defined as abnormal CFR or IMR, than in the control group (495 WU vs. 374 WU); absolute Q was not different between these groups (191 mL/min vs. 208 mL/min) [
77].
Furthermore, they observed that low Q (<198 mL/min) and high R (>416 WU) were associated with the severity of angina. Therefore, continuous thermodilution-derived measurements correlated with microvascular dysfunction and angina but were not associated with endothelium-dependent coronary spasm during acetylcholine testing.
Similarly, Rivero et al. demonstrated that Rmicro derived from continuous intracoronary thermodilution represents an accurate technique to assess the microvascular function and correlates well with IMR. An Rmicro value above 500 WU measured in the proximal LAD accurately predicts the presence of CMD. However, the reference values for absolute Q and R need to be validated in larger studies and correlated with clinical outcomes, potentially representing a future guide in patient-tailored therapy and an essential tool for the INOCA diagnostic workup [
71].
Scarsini et al. used MRR to assess CMD in patients with severe aortic stenosis undergoing transcatheter aortic valve implantation (TAVI). They assessed coronary microcirculation at baseline and promptly after the TAVI procedure and found that CMD correlated with a low-flow phenotype and with extra-valvular cardiac damage (EVCD) related to severe aortic stenosis [
78].
20. Clinical Evidence in Acute Scenarios
Recently, Wijnbergen et al. demonstrated that continuous thermodilution, using an intracoronary infusion of saline, permits safe and feasible measurement of absolute coronary blood flow and microvascular resistance during primary PCI in STEMI patients. This technique may allow better exploration and understanding of microvascular dysfunction in the early phase of STEMI. Absolute blood flow per gram of tissue of myocardium at risk correlates well with IMR. During the first couple of days, absolute flow increases and resistance decreases in a significant number of patients, indicating recovery of microvascular dysfunction over time. Larger studies are required to evaluate the clinical use of continuous thermodilution-derived indexes in acute settings [
79].
21. Conclusions
With the advancement of technology, numerous tools are available to assess the microcirculation. Although microvascular angina benefits from its own definite therapy, the techniques for diagnosing it are often overlooked and underemployed. Contrarily, the use of these methods should be implemented in the diagnostic workup of INOCA patients to promptly establish an appropriate therapeutic regimen. At last, larger randomized clinical trials are necessary to appraise the clinical use of the latest and most advanced continuous thermodilution techniques.
Author Contributions
Conceptualization, L.D.S., P.C., G.E., L.C. and S.M.; methodology, L.D.S. and L.C.; writing—original draft preparation, L.D.S., P.C., G.E., L.C., L.M., M.L.D.R., C.C., F.S.R., S.M. and M.S.; writing—review and editing, L.D.S. and L.C.; visualization, L.D.S., L.C.; supervision, L.D.S., P.C. and G.E. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
Di Serafino reports consultant fees from Abbott Vascular, Menarini, Boston, and Hexacath outside the submitted work. Cirillo reports consultant fees from Astra-Zeneca and Chiesi. Esposito reports consultant fees from Abbott Vascular, Amgen, Boehringer Ingelheim, Edwards Lifesciences, Terumo, and Sanofi outside the submitted work and research grants to the institution from Alvimedica, Boston Scientific, and Medtronic. The other authors have no conflicts of interest to declare.
References
- Del Buono, M.G.; Montone, R.A.; Camilli, M.; Carbone, S.; Narula, J.; Lavie, C.J.; Niccoli, G.; Crea, F. Coronary Microvascular Dysfunction Across the Spectrum of Cardiovascular Diseases: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2021, 78, 1352–1371. [Google Scholar] [CrossRef] [PubMed]
- Kaski, J.C.; Crea, F.; Gersh, B.J.; Camici, P.G. Reappraisal of Ischemic Heart Disease. Circulation 2018, 138, 1463–1480. [Google Scholar] [CrossRef] [PubMed]
- Camici, P.G.; Crea, F. Coronary microvascular dysfunction. N. Engl. J. Med. 2007, 356, 830–840. [Google Scholar] [CrossRef] [PubMed]
- Crea, F.; Camici, P.G.; Bairey Merz, C.N. Coronary microvascular dysfunction: An update. Eur. Heart J. 2014, 35, 1101–1111. [Google Scholar] [CrossRef] [PubMed]
- Pries, A.R.; Badimon, L.; Bugiardini, R.; Camici, P.G.; Dorobantu, M.; Duncker, D.J.; Escaned, J.; Koller, A.; Piek, J.J.; de Wit, C. Coronary vascular regulation, remodelling, and collateralization: Mechanisms and clinical implications on behalf of the working group on coronary pathophysiology and microcirculation. Eur. Heart J. 2015, 36, 3134–3146. [Google Scholar] [CrossRef] [PubMed]
- Scarsini, R.; Campo, G.; DI Serafino, L.; Zanon, S.; Rubino, F.; Monizzi, G.; Biscaglia, S.; Ancona, M.; Polimeni, A.; Niccoli, G.; et al. #FullPhysiology: A systematic step-by-step guide to implement intracoronary physiology in daily practice. Minerva Cardiol. Angiol. 2023, 71, 504–514. [Google Scholar] [CrossRef] [PubMed]
- Kelshiker, M.A.; Seligman, H.; Howard, J.P.; Rahman, H.; Foley, M.; Nowbar, A.N.; Rajkumar, C.A.; Shun-Shin, M.J.; Ahmad, Y.; Sen, S.; et al. Coronary flow reserve and cardiovascular outcomes: A systematic review and meta-analysis. Eur. Heart J. 2022, 43, 1582–1593. [Google Scholar] [CrossRef]
- Guerra, E.; Bergamaschi, L.; Tuttolomondo, D.; Pizzi, C.; Sartorio, D.; Gaibazzi, N. Contrast Stress Echocardiography Findings in Myocardial Bridging Compared to Normal Coronary Course, With and Without Coronary Artery Disease. J. Am. Soc. Echocardiogr. 2023, 36, 1092–1099. [Google Scholar] [CrossRef]
- Barbato, E.; Toth, G.G.; Johnson, N.P.; Pijls, N.H.; Fearon, W.F.; Tonino, P.A.; Curzen, N.; Piroth, Z.; Rioufol, G.; Jüni, P.; et al. A Prospective Natural History Study of Coronary Atherosclerosis Using Fractional Flow Reserve. J. Am. Coll. Cardiol. 2016, 68, 2247–2255. [Google Scholar] [CrossRef]
- De Bruyne, B.; Pijls, N.H.; Kalesan, B.; Barbato, E.; Tonino, P.A.; Piroth, Z.; Jagic, N.; Möbius-Winkler, S.; Mobius-Winckler, S.; Rioufol, G.; et al. Fractional flow reserve-guided PCI versus medical therapy in stable coronary disease. N. Engl. J. Med. 2012, 367, 991–1001. [Google Scholar] [CrossRef]
- Tonino, P.A.; De Bruyne, B.; Pijls, N.H.; Siebert, U.; Ikeno, F.; van’t Veer, M.; Klauss, V.; Manoharan, G.; Engstrøm, T.; Oldroyd, K.G.; et al. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N. Engl. J. Med. 2009, 360, 213–224. [Google Scholar] [CrossRef] [PubMed]
- Di Serafino, L.; De Bruyne, B.; Mangiacapra, F.; Bartunek, J.; Agostoni, P.; Vanderheyden, M.; Scognamiglio, G.; Heyndrickx, G.R.; Wijns, W.; Barbato, E. Long-term clinical outcome after fractional flow reserve- versus angio-guided percutaneous coronary intervention in patients with intermediate stenosis of coronary artery bypass grafts. Am. Heart J. 2013, 166, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Johnson, N.P.; Tóth, G.G.; Lai, D.; Zhu, H.; Açar, G.; Agostoni, P.; Appelman, Y.; Arslan, F.; Barbato, E.; Chen, S.-L.; et al. Prognostic value of fractional flow reserve: Linking physiologic severity to clinical outcomes. J. Am. Coll. Cardiol. 2014, 64, 1641–1654. [Google Scholar] [CrossRef] [PubMed]
- Mangiacapra, F.; Di Serafino, L.; Barbato, E. The role of fractional flow reserve to guide stent implantation. Minerva Cardioangiol. 2011, 59, 39–48. [Google Scholar] [PubMed]
- Davies, J.E.; Sen, S.; Dehbi, H.M.; Al-Lamee, R.; Petraco, R.; Nijjer, S.S.; Bhindi, R.; Lehman, S.J.; Walters, D.; Sapontis, J.; et al. Use of the Instantaneous Wave-free Ratio or Fractional Flow Reserve in PCI. N. Engl. J. Med. 2017, 376, 1824–1834. [Google Scholar] [CrossRef] [PubMed]
- Götberg, M.; Christiansen, E.H.; Gudmundsdottir, I.J.; Sandhall, L.; Danielewicz, M.; Jakobsen, L.; Olsson, S.E.; Öhagen, P.; Olsson, H.; Omerovic, E.; et al. Instantaneous Wave-free Ratio versus Fractional Flow Reserve to Guide PCI. N. Engl. J. Med. 2017, 376, 1813–1823. [Google Scholar] [CrossRef] [PubMed]
- Ligthart, J.; Masdjedi, K.; Witberg, K.; Mastik, F.; van Zandvoort, L.; Lemmert, M.E.; Wilschut, J.; Diletti, R.; de Jaegere, P.; Zijlstra, F.; et al. Validation of Resting Diastolic Pressure Ratio Calculated by a Novel Algorithm and Its Correlation with Distal Coronary Artery Pressure to Aortic Pressure, Instantaneous Wave-Free Ratio, and Fractional Flow Reserve. Circ. Cardiovasc. Interv. 2018, 11, e006911. [Google Scholar] [CrossRef]
- Svanerud, J.; Ahn, J.M.; Jeremias, A.; van’t Veer, M.; Gore, A.; Maehara, A.; Crowley, A.; Pijls, N.H.J.; De Bruyne, B.; Johnson, N.P.; et al. Validation of a novel non-hyperaemic index of coronary artery stenosis severity: The Resting Full-cycle Ratio (VALIDATE RFR) study. EuroIntervention 2018, 14, 806–814. [Google Scholar] [CrossRef]
- Kobayashi, Y.; Johnson, N.P.; Berry, C.; De Bruyne, B.; Gould, K.L.; Jeremias, A.; Oldroyd, K.G.; Pijls, N.H.J.; Fearon, W.F.; Investigators, C.S. The Influence of Lesion Location on the Diagnostic Accuracy of Adenosine-Free Coronary Pressure Wire Measurements. JACC Cardiovasc. Interv. 2016, 9, 2390–2399. [Google Scholar] [CrossRef]
- Petraco, R.; Park, J.J.; Sen, S.; Nijjer, S.S.; Malik, I.S.; Echavarría-Pinto, M.; Asrress, K.N.; Nam, C.W.; Macías, E.; Foale, R.A.; et al. Hybrid iFR-FFR decision-making strategy: Implications for enhancing universal adoption of physiology-guided coronary revascularisation. EuroIntervention 2013, 8, 1157–1165. [Google Scholar] [CrossRef]
- Di Serafino, L.; Barbato, E.; Serino, F.; Svanerud, J.; Scalamogna, M.; Cirillo, P.; Petitto, M.; Esposito, M.; Silvestri, T.; Franzone, A.; et al. Myocardial mass affects diagnostic performance of non-hyperemic pressure-derived indexes in the assessment of coronary stenosis. Int. J. Cardiol. 2023, 370, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Kunadian, V.; Chieffo, A.; Camici, P.G.; Berry, C.; Escaned, J.; Maas, A.H.E.M.; Prescott, E.; Karam, N.; Appelman, Y.; Fraccaro, C.; et al. An EAPCI Expert Consensus Document on Ischaemia with Non-Obstructive Coronary Arteries in Collaboration with European Society of Cardiology Working Group on Coronary Pathophysiology & Microcirculation Endorsed by Coronary Vasomotor Disorders International Study Group. Eur. Heart J. 2020, 41, 3504–3520. [Google Scholar] [CrossRef] [PubMed]
- Beltrame, J.F.; Crea, F.; Kaski, J.C.; Ogawa, H.; Ong, P.; Sechtem, U.; Shimokawa, H.; Bairey Merz, C.N.; Coronary Vasomotion Disorders International Study Group (COVADIS). International standardization of diagnostic criteria for vasospastic angina. Eur. Heart J. 2017, 38, 2565–2568. [Google Scholar] [CrossRef] [PubMed]
- Ford, T.J.; Stanley, B.; Sidik, N.; Good, R.; Rocchiccioli, P.; McEntegart, M.; Watkins, S.; Eteiba, H.; Shaukat, A.; Lindsay, M.; et al. 1-Year Outcomes of Angina Management Guided by Invasive Coronary Function Testing (CorMicA). JACC Cardiovasc Interv 2020, 13, 33–45. [Google Scholar] [CrossRef] [PubMed]
- Ford, T.J.; Stanley, B.; Good, R.; Rocchiccioli, P.; McEntegart, M.; Watkins, S.; Eteiba, H.; Shaukat, A.; Lindsay, M.; Robertson, K.; et al. Stratified Medical Therapy Using Invasive Coronary Function Testing in Angina: The CorMicA Trial. J. Am. Coll. Cardiol. 2018, 72, 2841–2855. [Google Scholar] [CrossRef] [PubMed]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef]
- Lanza, G.A.; Morrone, D.; Pizzi, C.; Tritto, I.; Bergamaschi, L.; De Vita, A.; Villano, A.; Crea, F. Diagnostic approach for coronary microvascular dysfunction in patients with chest pain and no obstructive coronary artery disease. Trends Cardiovasc. Med. 2022, 32, 448–453. [Google Scholar] [CrossRef]
- Ong, P.; Camici, P.G.; Beltrame, J.F.; Crea, F.; Shimokawa, H.; Sechtem, U.; Kaski, J.C.; Bairey Merz, C.N.; COVADIS. International standardization of diagnostic criteria for microvascular angina. Int. J. Cardiol. 2018, 250, 16–20. [Google Scholar] [CrossRef]
- Hartley, C.J. Review of intracoronary Doppler catheters. Int. J. Card. Imaging 1989, 4, 159–168. [Google Scholar] [CrossRef]
- Hartley, C.J.; Cole, J.S. An ultrasonic pulsed Doppler system for measuring blood flow in small vessels. J. Appl. Physiol. 1974, 37, 626–629. [Google Scholar] [CrossRef]
- Cole, J.S.; Hartley, C.J. The pulsed Doppler coronary artery catheter preliminary report of a new technique for measuring rapid changes in coronary artery flow velocity in man. Circulation 1977, 56, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Doucette, J.W.; Corl, P.D.; Payne, H.M.; Flynn, A.E.; Goto, M.; Nassi, M.; Segal, J. Validation of a Doppler guide wire for intravascular measurement of coronary artery flow velocity. Circulation 1992, 85, 1899–1911. [Google Scholar] [CrossRef] [PubMed]
- Labovitz, A.J.; Anthonis, D.M.; Cravens, T.L.; Kern, M.J. Validation of volumetric flow measurements by means of a Doppler-tipped coronary angioplasty guide wire. Am. Heart J. 1993, 126, 1456–1461. [Google Scholar] [CrossRef] [PubMed]
- AlBadri, A.; Bairey Merz, C.N.; Johnson, B.D.; Wei, J.; Mehta, P.K.; Cook-Wiens, G.; Reis, S.E.; Kelsey, S.F.; Bittner, V.; Sopko, G.; et al. Impact of Abnormal Coronary Reactivity on Long-Term Clinical Outcomes in Women. J. Am. Coll. Cardiol. 2019, 73, 684–693. [Google Scholar] [CrossRef] [PubMed]
- van de Hoef, T.P.; van Lavieren, M.A.; Damman, P.; Delewi, R.; Piek, M.A.; Chamuleau, S.A.; Voskuil, M.; Henriques, J.P.; Koch, K.T.; de Winter, R.J.; et al. Physiological basis and long-term clinical outcome of discordance between fractional flow reserve and coronary flow velocity reserve in coronary stenoses of intermediate severity. Circ. Cardiovasc. Interv. 2014, 7, 301–311. [Google Scholar] [CrossRef]
- Travieso, A.; Jeronimo-Baza, A.; Faria, D.; Shabbir, A.; Mejia-Rentería, H.; Escaned, J. Invasive evaluation of coronary microvascular dysfunction. J. Nucl. Cardiol. 2022, 29, 2474–2486. [Google Scholar] [CrossRef]
- Nolte, F.; van de Hoef, T.P.; Meuwissen, M.; Voskuil, M.; Chamuleau, S.A.; Henriques, J.P.; Verberne, H.J.; van Eck-Smit, B.L.; Koch, K.T.; de Winter, R.J.; et al. Increased hyperaemic coronary microvascular resistance adds to the presence of myocardial ischaemia. EuroIntervention 2014, 9, 1423–1431. [Google Scholar] [CrossRef]
- Williams, R.P.; de Waard, G.A.; De Silva, K.; Lumley, M.; Asrress, K.; Arri, S.; Ellis, H.; Mir, A.; Clapp, B.; Chiribiri, A.; et al. Doppler Versus Thermodilution-Derived Coronary Microvascular Resistance to Predict Coronary Microvascular Dysfunction in Patients with Acute Myocardial Infarction or Stable Angina Pectoris. Am. J. Cardiol. 2018, 121, 1–8. [Google Scholar] [CrossRef]
- de Waard, G.A.; Nijjer, S.S.; van Lavieren, M.A.; van der Hoeven, N.W.; Petraco, R.; van de Hoef, T.P.; Echavarría-Pinto, M.; Sen, S.; van de Ven, P.M.; Knaapen, P.; et al. Invasive minimal Microvascular Resistance Is a New Index to Assess Microcirculatory Function Independent of Obstructive Coronary Artery Disease. J. Am. Heart Assoc. 2016, 5, e004482. [Google Scholar] [CrossRef]
- Boerhout, C.K.M.; de Waard, G.A.; Lee, J.M.; Mejia-Renteria, H.; Lee, S.H.; Jung, J.H.; Hoshino, M.; Echavarria-Pinto, M.; Meuwissen, M.; Matsuo, H.; et al. Prognostic value of structural and functional coronary microvascular dysfunction in patients with non-obstructive coronary artery disease; from the multicentre international ILIAS registry. EuroIntervention 2022, 18, 719–728. [Google Scholar] [CrossRef]
- Candreva, A.; Gallinoro, E.; van’t Veer, M.; Sonck, J.; Collet, C.; Di Gioia, G.; Kodeboina, M.; Mizukami, T.; Nagumo, S.; Keulards, D.; et al. Basics of Coronary Thermodilution. JACC Cardiovasc. Interv. 2021, 14, 595–605. [Google Scholar] [CrossRef]
- Akasaka, T.; Yamamuro, A.; Kamiyama, N.; Koyama, Y.; Akiyama, M.; Watanabe, N.; Neishi, Y.; Takagi, T.; Shalman, E.; Barak, C.; et al. Assessment of coronary flow reserve by coronary pressure measurement: Comparison with flow- or velocity-derived coronary flow reserve. J. Am. Coll. Cardiol. 2003, 41, 1554–1560. [Google Scholar] [CrossRef]
- Feenstra, R.G.T.; Seitz, A.; Boerhout, C.K.M.; de Winter, R.J.; Ong, P.; Beijk, M.A.M.; Piek, J.J.; Sechtem, U.; van de Hoef, T.P. Reference values for intracoronary Doppler flow velocity-derived hyperaemic microvascular resistance index. Int. J. Cardiol. 2023, 371, 16–20. [Google Scholar] [CrossRef]
- Demir, O.M.; Boerhout, C.K.M.; de Waard, G.A.; van de Hoef, T.P.; Patel, N.; Beijk, M.A.M.; Williams, R.; Rahman, H.; Everaars, H.; Kharbanda, R.K.; et al. Comparison of Doppler Flow Velocity and Thermodilution Derived Indexes of Coronary Physiology. JACC Cardiovasc. Interv. 2022, 15, 1060–1070. [Google Scholar] [CrossRef]
- Jin, X.; Yoon, M.H.; Seo, K.W.; Tahk, S.J.; Lim, H.S.; Yang, H.M.; Choi, B.J.; Choi, S.Y.; Hwang, G.S.; Shin, J.H.; et al. Usefulness of Hyperemic Microvascular Resistance Index as a Predictor of Clinical Outcomes in Patients with ST-Segment Elevation Myocardial Infarction. Korean Circ. J. 2015, 45, 194–201. [Google Scholar] [CrossRef]
- de Waard, G.A.; Fahrni, G.; de Wit, D.; Kitabata, H.; Williams, R.; Patel, N.; Teunissen, P.F.; van de Ven, P.M.; Umman, S.; Knaapen, P.; et al. Hyperaemic microvascular resistance predicts clinical outcome and microvascular injury after myocardial infarction. Heart 2018, 104, 127–134. [Google Scholar] [CrossRef]
- Canu, M.; Khouri, C.; Marliere, S.; Vautrin, E.; Piliero, N.; Ormezzano, O.; Bertrand, B.; Bouvaist, H.; Riou, L.; Djaileb, L.; et al. Prognostic significance of severe coronary microvascular dysfunction post-PCI in patients with STEMI: A systematic review and meta-analysis. PLoS ONE 2022, 17, e0268330. [Google Scholar] [CrossRef]
- Zierler, K. Indicator dilution methods for measuring blood flow, volume, and other properties of biological systems: A brief history and memoir. Ann. Biomed. Eng. 2000, 28, 836–848. [Google Scholar] [CrossRef]
- Miller, D.E.; Gleason, W.L.; McIntosh, H.D. A comparison of the cardiac output determination by the direct Fick method and the dye-dilution method using indocyanine green dye and a cuvette densitometer. J. Lab. Clin. Med. 1962, 59, 345–350. [Google Scholar]
- De Bruyne, B.; Pijls, N.H.; Smith, L.; Wievegg, M.; Heyndrickx, G.R. Coronary thermodilution to assess flow reserve: Experimental validation. Circulation 2001, 104, 2003–2006. [Google Scholar] [CrossRef]
- Pijls, N.H.; De Bruyne, B.; Smith, L.; Aarnoudse, W.; Barbato, E.; Bartunek, J.; Bech, G.J.; Van De Vosse, F. Coronary thermodilution to assess flow reserve: Validation in humans. Circulation 2002, 105, 2482–2486. [Google Scholar] [CrossRef]
- Barbato, E.; Aarnoudse, W.; Aengevaeren, W.R.; Werner, G.; Klauss, V.; Bojara, W.; Herzfeld, I.; Oldroyd, K.G.; Pijls, N.H.; De Bruyne, B.; et al. Validation of coronary flow reserve measurements by thermodilution in clinical practice. Eur. Heart J. 2004, 25, 219–223. [Google Scholar] [CrossRef]
- Fearon, W.F.; Balsam, L.B.; Farouque, H.M.; Caffarelli, A.D.; Robbins, R.C.; Fitzgerald, P.J.; Yock, P.G.; Yeung, A.C. Novel index for invasively assessing the coronary microcirculation. Circulation 2003, 107, 3129–3132. [Google Scholar] [CrossRef]
- Fearon, W.F.; Kobayashi, Y. Invasive Assessment of the Coronary Microvasculature: The Index of Microcirculatory Resistance. Circ. Cardiovasc. Interv. 2017, 10, e005361. [Google Scholar] [CrossRef]
- Taqueti, V.R.; Shaw, L.J.; Cook, N.R.; Murthy, V.L.; Shah, N.R.; Foster, C.R.; Hainer, J.; Blankstein, R.; Dorbala, S.; Di Carli, M.F. Excess Cardiovascular Risk in Women Relative to Men Referred for Coronary Angiography Is Associated with Severely Impaired Coronary Flow Reserve, Not Obstructive Disease. Circulation 2017, 135, 566–577. [Google Scholar] [CrossRef]
- Lee, J.M.; Layland, J.; Jung, J.H.; Lee, H.J.; Echavarria-Pinto, M.; Watkins, S.; Yong, A.S.; Doh, J.H.; Nam, C.W.; Shin, E.S.; et al. Integrated physiologic assessment of ischemic heart disease in real-world practice using index of microcirculatory resistance and fractional flow reserve: Insights from the International Index of Microcirculatory Resistance Registry. Circ. Cardiovasc. Interv. 2015, 8, e002857. [Google Scholar] [CrossRef]
- Echavarría-Pinto, M.; van de Hoef, T.P.; Nijjer, S.; Gonzalo, N.; Nombela-Franco, L.; Ibañez, B.; Sen, S.; Petraco, R.; Jimenez-Quevedo, P.; Nuñez-Gil, I.J.; et al. Influence of the amount of myocardium subtended to a coronary stenosis on the index of microcirculatory resistance. Implications for the invasive assessment of microcirculatory function in ischaemic heart disease. EuroIntervention 2017, 13, 944–952. [Google Scholar] [CrossRef]
- Mangiacapra, F.; Bressi, E.; Di Gioia, G.; Pellicano, M.; Di Serafino, L.; Peace, A.J.; Bartunek, J.; Morisco, C.; Wijns, W.; De Bruyne, B.; et al. Coronary microcirculation and peri-procedural myocardial injury during elective percutaneous coronary intervention. Int. J. Cardiol. 2020, 306, 42–46. [Google Scholar] [CrossRef]
- Niccoli, G.; Scalone, G.; Lerman, A.; Crea, F. Coronary microvascular obstruction in acute myocardial infarction. Eur. Heart J. 2016, 37, 1024–1033. [Google Scholar] [CrossRef]
- De Maria, G.L.; Alkhalil, M.; Wolfrum, M.; Fahrni, G.; Borlotti, A.; Gaughran, L.; Dawkins, S.; Langrish, J.P.; Lucking, A.J.; Choudhury, R.P.; et al. Index of Microcirculatory Resistance as a Tool to Characterize Microvascular Obstruction and to Predict Infarct Size Regression in Patients with STEMI Undergoing Primary PCI. JACC Cardiovasc. Imaging 2019, 12, 837–848. [Google Scholar] [CrossRef]
- Ahn, S.G.; Hung, O.Y.; Lee, J.W.; Lee, J.H.; Youn, Y.J.; Ahn, M.S.; Kim, J.Y.; Yoo, B.S.; Lee, S.H.; Yoon, J.; et al. Combination of the Thermodilution-Derived Index of Microcirculatory Resistance and Coronary Flow Reserve Is Highly Predictive of Microvascular Obstruction on Cardiac Magnetic Resonance Imaging After ST-Segment Elevation Myocardial Infarction. JACC Cardiovasc. Interv. 2016, 9, 793–801. [Google Scholar] [CrossRef]
- van’t Veer, M.; Geven, M.C.; Rutten, M.C.; van der Horst, A.; Aarnoudse, W.H.; Pijls, N.H.; van de Vosse, F.N. Continuous infusion thermodilution for assessment of coronary flow: Theoretical background and in vitro validation. Med. Eng. Phys. 2009, 31, 688–694. [Google Scholar] [CrossRef]
- Aarnoudse, W.; Van’t Veer, M.; Pijls, N.H.; Ter Woorst, J.; Vercauteren, S.; Tonino, P.; Geven, M.; Rutten, M.; van Hagen, E.; de Bruyne, B.; et al. Direct volumetric blood flow measurement in coronary arteries by thermodilution. J. Am. Coll. Cardiol. 2007, 50, 2294–2304. [Google Scholar] [CrossRef]
- van’t Veer, M.; Adjedj, J.; Wijnbergen, I.; Tóth, G.G.; Rutten, M.C.; Barbato, E.; van Nunen, L.X.; Pijls, N.H.; De Bruyne, B. Novel monorail infusion catheter for volumetric coronary blood flow measurement in humans: In vitro validation. EuroIntervention 2016, 12, 701–707. [Google Scholar] [CrossRef]
- Xaplanteris, P.; Fournier, S.; Keulards, D.C.J.; Adjedj, J.; Ciccarelli, G.; Milkas, A.; Pellicano, M.; Van’t Veer, M.; Barbato, E.; Pijls, N.H.J.; et al. Catheter-Based Measurements of Absolute Coronary Blood Flow and Microvascular Resistance: Feasibility, Safety, and Reproducibility in Humans. Circ. Cardiovasc. Interv. 2018, 11, e006194. [Google Scholar] [CrossRef]
- Gutiérrez-Barrios, A.; Izaga-Torralba, E.; Rivero Crespo, F.; Gheorghe, L.; Cañadas-Pruaño, D.; Gómez-Lara, J.; Silva, E.; Noval-Morillas, I.; Zayas Rueda, R.; Calle-Pérez, G.; et al. Continuous Thermodilution Method to Assess Coronary Flow Reserve. Am. J. Cardiol. 2021, 141, 31–37. [Google Scholar] [CrossRef]
- Gallinoro, E.; Candreva, A.; Colaiori, I.; Kodeboina, M.; Fournier, S.; Nelis, O.; Di Gioia, G.; Sonck, J.; van’t Veer, M.; Pijls, N.H.J.; et al. Thermodilution-derived volumetric resting coronary blood flow measurement in humans. EuroIntervention 2021, 17, e672–e679. [Google Scholar] [CrossRef]
- De Bruyne, B.; Pijls, N.H.J.; Gallinoro, E.; Candreva, A.; Fournier, S.; Keulards, D.C.J.; Sonck, J.; Van’t Veer, M.; Barbato, E.; Bartunek, J.; et al. Microvascular Resistance Reserve for Assessment of Coronary Microvascular Function: JACC Technology Corner. J. Am. Coll. Cardiol. 2021, 78, 1541–1549. [Google Scholar] [CrossRef] [PubMed]
- Jansen, T.P.J.; de Vos, A.; Paradies, V.; Dimitriu-Leen, A.; Crooijmans, C.; Elias-Smale, S.; Rodwell, L.; Maas, A.H.E.M.; Smits, P.C.; Pijls, N.; et al. Continuous Versus Bolus Thermodilution-Derived Coronary Flow Reserve and Microvascular Resistance Reserve and Their Association with Angina and Quality of Life in Patients with Angina and Nonobstructive Coronaries: A Head-to-Head Comparison. J. Am. Heart Assoc. 2023, 12, e030480. [Google Scholar] [CrossRef] [PubMed]
- Keulards, D.C.J.; El Farissi, M.; Tonino, P.A.L.; Teeuwen, K.; Vlaar, P.J.; van Hagen, E.; Wijnbergen, I.F.; de Vos, A.; Brueren, G.R.G.; Van’t Veer, M.; et al. Thermodilution-Based Invasive Assessment of Absolute Coronary Blood Flow and Microvascular Resistance: Quantification of Microvascular (Dys)Function? J. Interv. Cardiol. 2020, 2020, 5024971. [Google Scholar] [CrossRef] [PubMed]
- Rivero, F.; Gutiérrez-Barrios, A.; Gomez-Lara, J.; Fuentes-Ferrer, M.; Cuesta, J.; Keulards, D.C.J.; Pardo-Sanz, A.; Bastante, T.; Izaga-Torralba, E.; Gomez-Hospital, J.A.; et al. Coronary microvascular dysfunction assessed by continuous intracoronary thermodilution: A comparative study with index of microvascular resistance. Int. J. Cardiol. 2021, 333, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Mangiacapra, F.; Viscusi, M.M.; Verolino, G.; Paolucci, L.; Nusca, A.; Melfi, R.; Ussia, G.P.; Grigioni, F. Invasive Assessment of Coronary Microvascular Function. J. Clin. Med. 2021, 11, 228. [Google Scholar] [CrossRef] [PubMed]
- Keulards, D.C.J.; Van’t Veer, M.; Zelis, J.M.; El Farissi, M.; Zimmermann, F.M.; de Vos, A.; Teeuwen, K.; Brueren, G.R.G.; Wijnbergen, I.F.; Vlaar, P.J.; et al. Safety of absolute coronary flow and microvascular resistance measurements by thermodilution. EuroIntervention 2021, 17, 229–232. [Google Scholar] [CrossRef] [PubMed]
- Everaars, H.; de Waard, G.A.; Schumacher, S.P.; Zimmermann, F.M.; Bom, M.J.; van de Ven, P.M.; Raijmakers, P.G.; Lammertsma, A.A.; Götte, M.J.; van Rossum, A.C.; et al. Continuous thermodilution to assess absolute flow and microvascular resistance: Validation in humans using [15O]H2O positron emission tomography. Eur. Heart J. 2019, 40, 2350–2359. [Google Scholar] [CrossRef] [PubMed]
- Fournier, S.; Keulards, D.C.J.; van’t Veer, M.; Colaiori, I.; Di Gioia, G.; Zimmermann, F.M.; Mizukami, T.; Nagumo, S.; Kodeboina, M.; El Farissi, M.; et al. Normal values of thermodilution-derived absolute coronary blood flow and microvascular resistance in humans. EuroIntervention 2021, 17, e309–e316. [Google Scholar] [CrossRef] [PubMed]
- Jansen, T.P.J.; de Vos, A.; Paradies, V.; Damman, P.; Teerenstra, S.; Konst, R.E.; Dimitriu-Leen, A.; Maas, A.H.E.M.; Smits, P.C.; Elias-Smale, S.E.; et al. Absolute Flow and Resistance Have Superior Repeatability as Compared to CFR and IMR: EDIT-CMD Substudy. JACC Cardiovasc. Interv. 2023, 16, 872–874. [Google Scholar] [CrossRef]
- Konst, R.E.; Elias-Smale, S.E.; Pellegrini, D.; Hartzema-Meijer, M.; van Uden, B.J.C.; Jansen, T.P.J.; Vart, P.; Gehlmann, H.; Maas, A.H.E.M.; van Royen, N.; et al. Absolute Coronary Blood Flow Measured by Continuous Thermodilution in Patients With Ischemia and Nonobstructive Disease. J. Am. Coll. Cardiol. 2021, 77, 728–741. [Google Scholar] [CrossRef]
- Scarsini, R.; Gallinoro, E.; Ancona, M.B.; Portolan, L.; Paolisso, P.; Springhetti, P.; Della Mora, F.; Mainardi, A.; Belmonte, M.; Moroni, F.; et al. Characterisation of coronary microvascular dysfunction in patients with severe aortic stenosis undergoing TAVI. EuroIntervention 2023, 19, EIJ-D-23-00735. [Google Scholar] [CrossRef]
- Wijnbergen, I.; van’t Veer, M.; Lammers, J.; Ubachs, J.; Pijls, N.H. Absolute coronary blood flow measurement and microvascular resistance in ST-elevation myocardial infarction in the acute and subacute phase. Cardiovasc. Revasc. Med. 2016, 17, 81–87. [Google Scholar] [CrossRef]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).

 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}