
Feasibility of Ultrasound-Guided Axillary Vein Puncture under Valsalva Maneuver for Diagnostic and Cardiovascular Interventional Purposes: Pacemaker and Cardioverter-Defibrillator Implantation


Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting and Ethics
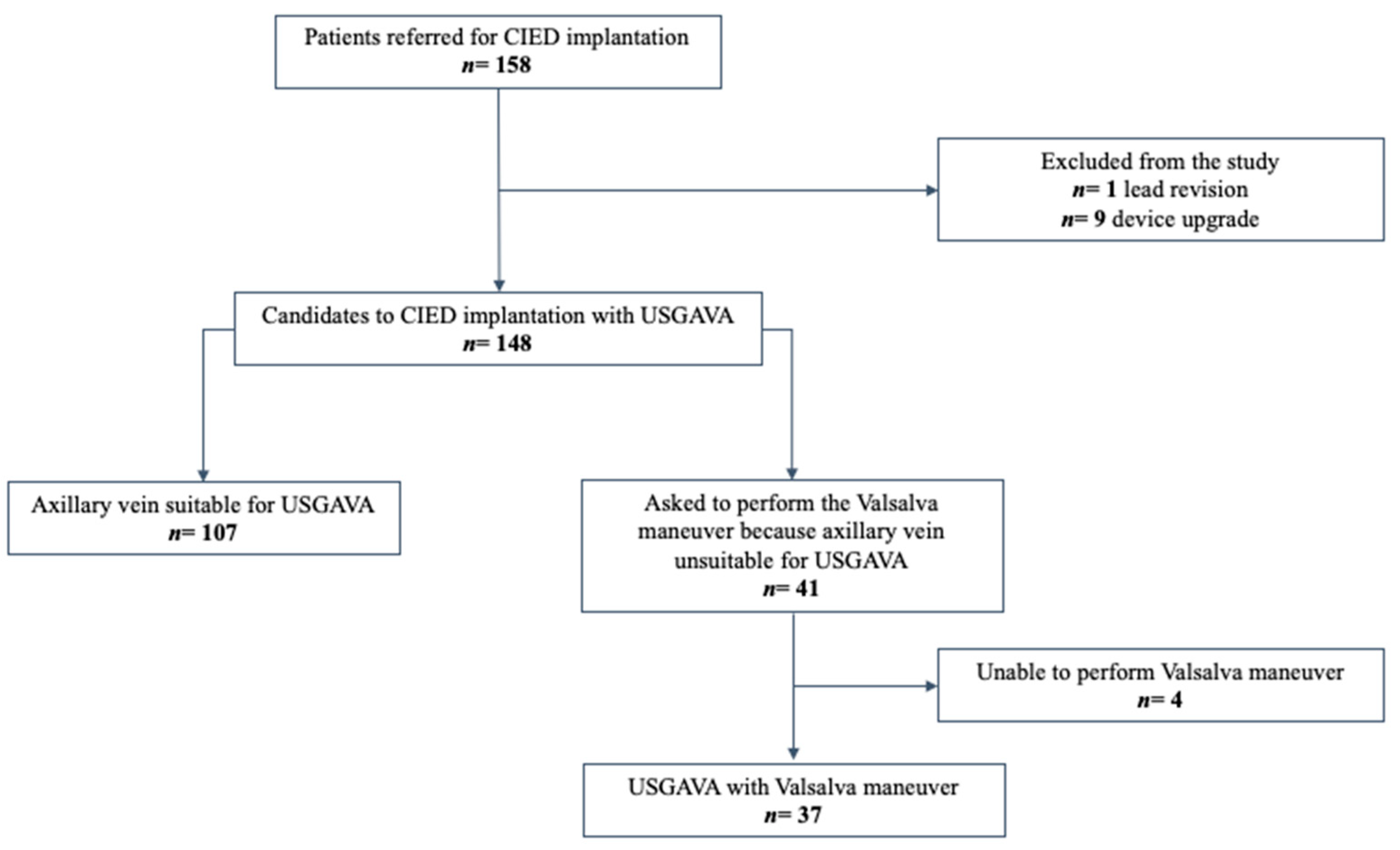
2.2. Patient Selection
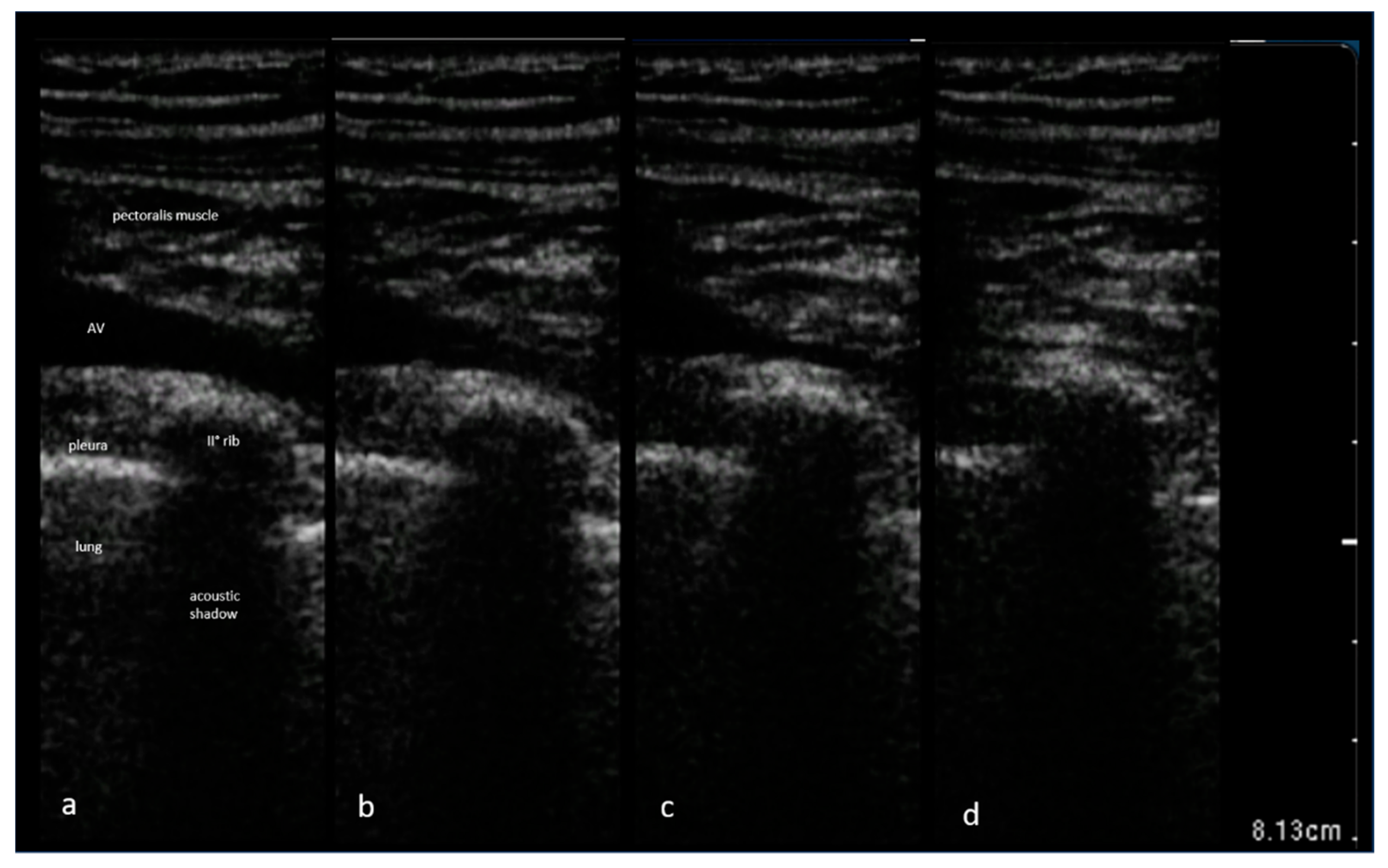
2.3. Technique for Axillary Vein Access Guided by Ultrasound
2.4. Routine Maneuvers to Increase Filling of Axillary Vein
2.5. Use of the Valsalva Maneuver
2.6. Variables and Definitions
2.7. Study Endpoints
2.8. Statistical Analyses
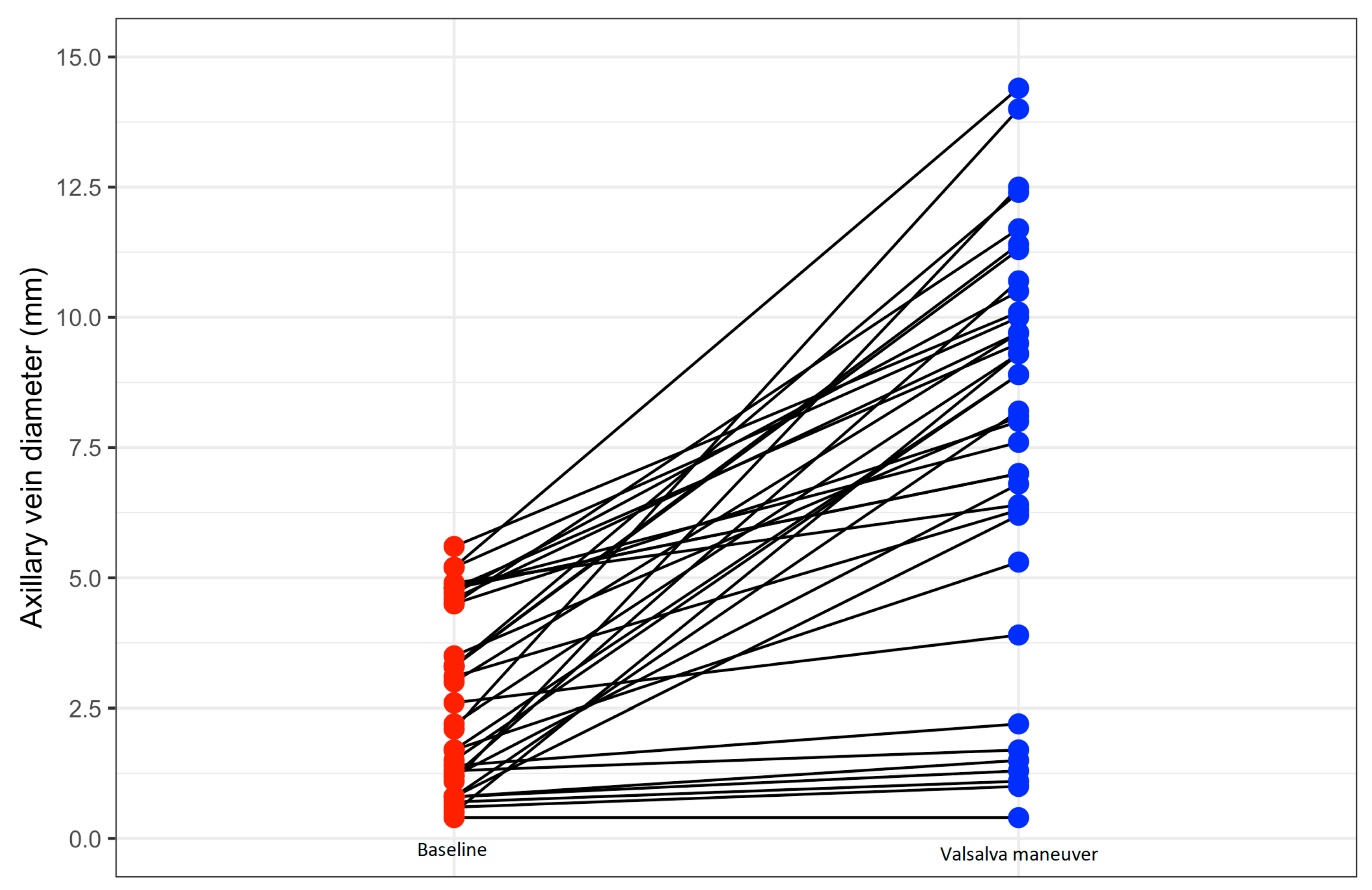
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bongiorni, M.G.; Proclemer, A.; Dobreanu, D.; Marinskis, G.; Pison, L.; Blomstrom-Lundqvist, C. Preferred tools and techniques for implantation of cardiac electronic devices in Europe: Results of the European Heart Rhythm Association survey. Europace 2013, 15, 1664–1668. [Google Scholar] [CrossRef]
- Lin, Y.S.; Hung, S.P.; Chen, P.R.; Yang, C.H.; Wo, H.T.; Chang, P.C.; Wang, C.C.; Chou, C.C.; Wen, M.S.; Chung, C.M.; et al. Risk factors influencing complications of cardiac implantable electronic device implantation: Infection, pneumothorax and heart perforation: A nationwide population-based cohort study. Medicine 2014, 93, e213. [Google Scholar] [CrossRef]
- Parsonnet, V.; Bernstein, A.; Lindsay, B. Pacemaker-implantation complication rates: An analysis of some contributing factors. J. Am. Coll. Cardiol. 1989, 13, 917–921. [Google Scholar] [CrossRef]
- Aggarwal, R.K.; Connelly, D.T.; Ray, S.G.; Ball, J.; Charles, R.G. Early complications of permanent pacemaker implantation: No difference between dual and single chamber systems. Br. Heart J. 1995, 73, 571–575. [Google Scholar] [CrossRef] [PubMed]
- Kirkfeldt, R.E.; Johansen, J.B.; Nohr, E.A.; Moller, M.; Arnsbo, P.; Nielsen, J.C. Pneumothorax in cardiac pacing: A population-based cohort study of 28,860 Danish patients. Europace 2012, 14, 1132–1138. [Google Scholar] [CrossRef] [PubMed]
- Antonelli, D.; Rosenfeld, T.; Freedberg, N.A.; Palma, E.; Gross, J.N.; Furman, S. Insulation Lead Failure: Is it a Matter of Insulation Coating, Venous Approach, or both? Pacing Clin. Electrophysiol. 1998, 21, 418–421. [Google Scholar] [CrossRef] [PubMed]
- Altun, A.; Erdogan, O. Pacemaker lead failure suggestive of crush injury. Cardiol. Rev. 2003, 11, 256. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, D.M.; Fink, A.S.; Miller, R.P.; Anderson, W.R.; McVenes, R.D.; Lessar, J.F.; Cobian, K.E.; Staffanson, D.B.; Upton, J.E.; Bubrick, M.P. Anatomical and morphological evaluation of pacemaker lead compression. Pacing Clin. Electrophysiol. 1993, 16, 434–444. [Google Scholar] [CrossRef]
- Roelke, M.; O’Nunain, S.S.; Osswald, S.; Garan, H.; Harthorne, J.W.; Ruskin, J.N. Subclavian crush syndrome complicating transvenous cardioverter defibrillator systems. Pacing Clin. Electrophysiol. 1995, 18, 973–979. [Google Scholar] [CrossRef]
- King, S.M.; Arrington, J.O.; Dalton, M.L. Permanent transvenous cardiac pacing via the left cephalic vein. Ann. Thorac. Surg. 1968, 5, 469–473. [Google Scholar] [CrossRef] [PubMed]
- Furman, S. Venous cutdown for pacemaker implantation. Ann. Thorac. Surg. 1986, 41, 438–439. [Google Scholar] [CrossRef] [PubMed]
- Shimada, H.; Hoshino, K.; Yuki, M.; Sakurai, S.; Owa, M. Percutaneous cephalic vein approach for permanent pacemaker implantation. Pacing Clin. Electrophysiol. 1999, 22, 1499–1501. [Google Scholar] [CrossRef] [PubMed]
- Lau, E.W. Upper body venous access for transvenous lead placement? Review of existent techniques. Pacing Clin. Electrophysiol. 2007, 30, 901–909. [Google Scholar] [CrossRef]
- Gallik, D.M.; Ben-Zur, U.M.; Gross, J.N.; Furman, S. Lead fracture in cephalic versus subclavian approach with transvenous implantable cardioverter defibrillator systems. Pacing Clin. Electrophysiol. 1996, 19, 1089–1094. [Google Scholar] [CrossRef]
- Calkins, H.; Ramza, B.M.; Brinker, J.; Atiga, W.; Donahue, K.; Nsah, E.; Taylor, E.; Halperin, H.; Lawrence, J.H.; Tomaselli, G.; et al. Prospective randomized comparison of the safety and effectiveness of placement of endocardial pacemaker and defibrillator leads using the extrathoracic subclavian vein guided by contrast venography versus the cephalic approach. Pacing Clin. Electrophysiol. 2001, 24, 456–464. [Google Scholar] [CrossRef]
- Tse, H.F.; Lau, C.P.; Leung, S.K. A cephalic vein cutdown and venography technique to facilitate pacemaker and defibrillator lead implantation. Pacing Clin. Electrophysiol. 2001, 24, 469–473. [Google Scholar] [CrossRef]
- Belott, P. How to access the axillary vein. Heart Rhythm 2006, 3, 366–369. [Google Scholar] [CrossRef] [PubMed]
- Sassone, B.; Valzania, C.; Laffi, M.; Virzì, S.; Luzi, M. Axillary vein access for antiarrhythmic cardiac device implantation: A literature review. J. Cardiovasc. Med. 2021, 22, 237–245. [Google Scholar] [CrossRef] [PubMed]
- Magney, J.E.; Staplin, D.H.; Flynn, D.M.; Hunter, D.W. A new approach to percutaneous subclavian venipuncture to avoid lead fracture or central venous catheter occlusion. Pacing Clin. Electrophysiol. 1993, 16, 2133–2142. [Google Scholar] [CrossRef]
- Chan, N.Y.; Kwong, N.P.; Cheong, A.P. Venous access and long-term pacemaker lead failure: Comparing contrast-guided axillary vein puncture with subclavian puncture and cephalic cutdown. Europace 2017, 19, 1193–1197. [Google Scholar] [CrossRef]
- Garcia-Rinaldi, R.F. Insertion of the lead of a permanent transvenous pacemaker utilizing an axillary approach: A solution to the unsuitable cephalic vein. Chest 1978, 73, 561. [Google Scholar] [CrossRef]
- Al-Hadithi, A.B.; Do, D.H.; Boyle, N.G. Vein management for cardiac device implantation. Card. Electrophysiol. Clin. 2018, 10, 561–571. [Google Scholar] [CrossRef]
- Watanabe, M.; Yokoshiki, H.; Mitsuyama, H.; Mizukami, K.; Tenma, T.; Kamada, R.; Takahashi, M.; Matsui, Y.; Anzai, T. Long-term reliability of the defibrillator lead inserted by the extrathoracic subclavian puncture. J. Arrhythmia 2018, 34, 541–547. [Google Scholar] [CrossRef]
- Kim, K.H.; Park, K.M.; Nam, G.B.; Kim, D.K.; Oh, M.; Choi, H.O.; Hong, T.J.; Park, B.M.; Seo, G.W.; Song, P.S.; et al. Comparison of the axillary venous approach and subclavian venous approach for efficacy of permanent pacemaker implantation. Circ. J. 2014, 78, 865–871. [Google Scholar] [CrossRef] [PubMed]
- Ramza, B.M.; Rosenthal, L.; Hui, R.; Nsah, E.; Savader, S.; Lawrence, J.H.; Tomaselli, G.; Berger, R.; Brinker, J.; Calkins, H. Safety and effectiveness of placement of pacemaker and defibrillator leads in the axillary vein guided by contrast venography. Am. J. Cardiol. 1997, 80, 892–896. [Google Scholar] [CrossRef] [PubMed]
- Byrd, C.L. Clinical experience with the extrathoracic introducer insertion technique. Pacing Clin. Electrophysiol. 1993, 16, 1781–1784. [Google Scholar] [CrossRef]
- Antonelli, D.; Feldman, A.; Freedberg, N.A.; Turgeman, Y. Axillary vein puncture without contrast venography for pacemaker and defibrillator leads implantation. Pacing Clin. Electrophysiol. 2013, 36, 1107–1110. [Google Scholar] [CrossRef] [PubMed]
- Seto, A.H.; Jolly, A.; Salcedo, J. Ultrasound-guided venous access for pacemakers and defibrillators. J. Cardiovasc. Electrophysiol. 2013, 24, 370–374. [Google Scholar] [CrossRef] [PubMed]
- Liccardo, M.; Nocerino, P.; Gaia, S.; Ciardiello, C. Efficacy of ultrasound-guided axillary/subclavian venous approaches for pacemaker and defibrillator lead implantation: A randomized study. J. Interv. Card. Electrophysiol. 2018, 51, 153–160. [Google Scholar] [CrossRef]
- Tagliari, A.P.; Kochi, A.N.; Mastella, B.; Saadi, R.P.; di Leoni Ferrari, A.; Saadi, E.K.; Polanczyk, C.A. Axillary vein puncture guided by ultrasound versus cephalic vein dissection in pacemaker and defibrillator implant: A multicenter randomized clinical trial. Heart Rhythm 2020, 17, 1554–1560. [Google Scholar] [CrossRef]
- Ravindran, C.; Thiyagarajan, S.; Velraj, J.; Murugesan, R. Arm position and collapsibility of infraclavicular axillary vein during voluntary breathing: An ultrasound-guided observational study. J. Vasc. Access 2020, 21, 39–44. [Google Scholar] [CrossRef]
- Nagalingam, S.; Sivashanmugam, T.; Ravindran, C.; Ponnusamy, R. Influence of arm position on the first pass success rates of ultrasound-guided infraclavicular axillary vein cannulation in spontaneously breathing patients: A randomised clinical trial. J. Vasc. Access. 2023, 11297298231152631. [Google Scholar] [CrossRef]
- Hightower, D.R.; Gooding, G.A. Sonographic evaluation of the normal response of subclavian veins to respiratory maneuvers. Investig. Radiol. 1985, 20, 517–520. [Google Scholar] [CrossRef] [PubMed]
- Lim, K.J.; Lee, J.M.; Byon, H.J.; Kim, H.S.; Kim, C.S.; Lee, S.K.; Kim, J.T. The Effect of full expiration on the position and size of the subclavian vein in spontaneously breathing adults. Anesth. Analg. 2013, 117, 109–113. [Google Scholar] [CrossRef] [PubMed]
- Sassone, B.; Bertagnin, E.; Simeti, G.; Santo, V. Handheld ultrasound device-guided axillary vein access for pacemaker and defibrillator implantation. Veins Lymphat. 2023, 12. [Google Scholar] [CrossRef]
- Fortune, J.B.; Feustel, P. Effect of patient position on size and location of the subclavian vein for percutaneous puncture. Arch. Surg. 2003, 138, 996–1000. [Google Scholar] [CrossRef] [PubMed]
- Clenaghan, S.; McLaughlin, R.E.; Martyn, C.; McGovern, S.; Bowra, J. Relationship between Trendelenburg tilt and internal jugular vein diameter. Emerg. Med. J. 2005, 22, 867–868. [Google Scholar] [CrossRef]
- Beddy, P.; Geoghegan, T.; Ramesh, N.; Buckley, O.; O’Brien, J.; Colville, J.; Torreggiani, W.C. Valsalva and gravitational variability of the internal jugular vein and common femoral vein: Ultrasound assessment. Eur. J. Radiol. 2006, 53, 654–658. [Google Scholar] [CrossRef]
- Bellazzini, M.A.; Rankin, P.M.; Gangnon, R.E.; Bjoernsen, L.P. Ultrasound validation of maneuvers to increase internal jugular vein cross-sectional area and decrease compressibility. Am. J. Emerg. Med. 2009, 27, 454–459. [Google Scholar] [CrossRef]
- Ford, D.R.; Witting, M.D.; Vora, M.V.; Sommerkamp, S.K.; Euerle, B.D. No effect of Valsalva maneuver or Trendelenburg angle on axillary vein size. J. Emerg. Med. 2013, 45, 452–457. [Google Scholar] [CrossRef]
- Sassone, B.; Simeti, G.; Virzì, S.; Pasanisi, G.; Muser, G. The Use of a Handheld Ultrasound Device to Guide the Axillary Vein Access during Pacemaker and Cardioverter-Defibrillator Implantation. A Feasibility Study. Rev. Cardiovasc. Med. 2022, 23, 258. [Google Scholar] [CrossRef]
- Berczi, V.; Molnar, A.A.; Apor, A.; Kovacs, V.; Rusics, C.; Varallyay, C.; Huttl, K.; Monos, E.; Nadasy, G.L. Non-invasive assessment of human large vein diameter, capacity, distensibility and ellipticity in situ: Dependence on anatomical location, age, body position and pressure. Eur. J. Appl. Physiol. 2005, 95, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Jones, M.R.; Prabhakar, A.; Viswanath, O.; Urits, I.; Green, J.B.; Kendrick, J.B.; Brunk, A.J.; Eng, M.R.; Orhurhu, V.; Cornett, E.M.; et al. Thoracic Outlet Syndrome: A Comprehensive Review of Pathophysiology, Diagnosis, and Treatment. Pain Ther. 2019, 8, 5–18. [Google Scholar] [CrossRef] [PubMed]
- Kaziród-Wolski, K.; Zając, P.; Sielski, J.K. Temporary transvenous cardiac pacing in patient with thoracic outlet syndrome technical difficulties. Folia Cardiol. 2022, 17, 180–182. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | n = 148 1 |
|---|---|
| Age (year) | 78 (8) |
| Male gender | 104 (70%) |
| BMI (kg/m2) | 26.8 (3.9) |
| BSA (m2) | 1.9 (0.2) |
| LVEF (%) | 50.6 (14.5) |
| Diabetes mellitus | 30 (20%) |
| Coronary artery disease | 40 (27%) |
| Chronic obstructive pulmonary disease | 16 (11%) |
| Hypertension | 105 (71%) |
| History of cardiac surgery | 17 (11%) |
| Creatinine (mg/dL) | 1.0 (0.4) |
| Use of diuretic therapy | 45 (30%) |
| Antithrombotic therapy | |
| No antithrombotic therapy | 35 (24%) |
| Oral anticoagulant | 70 (47%) |
| Single antiplatelet therapy | 36 (24%) |
| Dual antiplatelet therapy | 2 (1.4%) |
| Oral anticoagulant + antiplatelet therapy | 5 (3.4%) |
| Device type | |
| Single-chamber pacemaker | 29 (20%) |
| Dual-chamber pacemaker | 69 (47%) |
| Biventricular pacemaker | 23 (16%) |
| Single-chamber cardioverter-defibrillator | 13 (8.8%) |
| Dual-chamber cardioverter-defibrillator | 2 (1.4%) |
| Biventricular cardioverter-defibrillator | 12 (8.1%) |
| Success rate of ultrasound-guided axillary vein access | 137 (93%) |
| Complications | 2 (1.4%) |
| Total number of implanted leads | 273 (0) |
| Average number of leads per patient | 1.8 (0.6) |
| Procedural time (min) | 68.1 (32.5) |
| X-ray time (min) | 2.8 (1.6, 6.2) |
| Axillary vein depth (mm) | 21.7 (6.6) |
| Axillary vein diameter (mm) | 7.5 (4.1) |
| Characteristic | Without Valsalva n = 111 1 | With Valsalva n = 37 1 | p-Value 2 |
|---|---|---|---|
| Age (year) | 79 (8) | 76 (10) | 0.075 |
| Male gender | 75 (68%) | 29 (78%) | 0.213 |
| BMI (kg/m2) | 26.3 (3.7) | 28.6 (4.2) | 0.007 |
| BSA (m2) | 1.8 (0.2) | 1.9 (0.2) | 0.009 |
| LVEF (%) | 51.2 (13.4) | 48.6 (17.3) | 0.545 |
| Diabetes mellitus | 22 (20%) | 8 (22%) | 0.813 |
| Coronary artery disease | 30 (27%) | 10 (27%) | 1.000 |
| Chronic obstructive pulmonary disease | 11 (9.9%) | 5 (14%) | 0.548 |
| Hypertension | 82 (74%) | 23 (62%) | 0.174 |
| History of cardiac surgery | 13 (12%) | 4 (11%) | 1.000 |
| Creatinine (mg/dl) | 1.0 (0.4) | 1.0 (0.4) | 0.372 |
| Use of diuretic therapy | 30 (27%) | 15 (41%) | 0.122 |
| Antithrombotic therapy | 0.011 | ||
| No antithrombotic therapy | 19 (17%) | 16 (43%) | |
| Oral anticoagulant | 58 (52%) | 12 (32%) | |
| Single antiplatelet therapy | 28 (25%) | 8 (22%) | |
| Dual antiplatelet therapy | 1 (0.9%) | 1 (2.7%) | |
| Oral anticoagulant + antiplatelet therapy | 5 (4.5%) | 0 (0%) | |
| Device type | 0.212 | ||
| Single-chamber pacemaker | 24 (22%) | 5 (14%) | |
| Dual-chamber pacemaker | 50 (45%) | 19 (51%) | |
| Biventricular pacemaker | 20 (18%) | 3 (8.1%) | |
| Single-chamber cardioverter-defibrillator | 7 (6.3%) | 6 (16%) | |
| Dual-chamber cardioverter-defibrillator | 1 (0.9%) | 1 (2.7%) | |
| Biventricular cardioverter-defibrillator | 9 (8.1%) | 3 (8.1%) | |
| Success rate of ultrasound-guided axillary vein access | 107 (96%) | 30 (81%) | 0.006 |
| Complications | 2 (1.8%) | 0 (0%) | 1.000 |
| Average number of leads per patient | 1.9 (0.6) | 1.8 (0.5) | 0.371 |
| Procedural time (min) | 70.6 (33.7) | 60.4 (27.7) | 0.128 |
| X-ray time (min) | 3.2 (1.6, 6.2) | 2.4 (1.6, 5.5) | 0.647 |
| Axillary vein depth (mm) | 21.4 (6.8) | 22.5 (6.2) | 0.356 |
| Axillary vein diameter (mm) | 9.1 (3.3) | 2.7 (1.7) | <0.0001 |
| Characteristic | Unsuccessful n = 7 1 | Successful n = 30 1 | p-Value 2 |
|---|---|---|---|
| Age (year) | 70 (13) | 77 (9) | 0.095 |
| Male gender | 6 (86%) | 23 (77%) | 1.000 |
| BMI (kg/m2) | 31.3 (4.3) | 28.0 (4.0) | 0.062 |
| BSA (m2) | 1.9 (0.2) | 1.9 (0.1) | 0.790 |
| LVEF (%) | 48.6 (19.3) | 48.6 (17.2) | 0.997 |
| Diabetes mellitus | 2 (29%) | 6 (20%) | 0.631 |
| Coronary artery disease | 2 (29%) | 8 (27%) | 1.000 |
| Chronic obstructive pulmonary disease | 0 (0%) | 5 (17%) | 0.560 |
| Hypertension | 5 (71%) | 18 (60%) | 0.687 |
| History of cardiac surgery | 0 (0%) | 4 (13%) | 0.570 |
| Creatinine (mg/dL) | 0.8 (0.1) | 1.1 (0.4) | 0.069 |
| Use of diuretic therapy | 3 (43%) | 12 (40%) | 1.000 |
| Antithrombotic therapy | 0.189 | ||
| No antithrombotic therapy | 4 (57%) | 12 (40%) | |
| Oral anticoagulant | 1 (14%) | 11 (37%) | |
| Single antiplatelet therapy | 1 (14%) | 7 (23%) | |
| Dual antiplatelet therapy | 1 (14%) | 0 (0%) | |
| Oral anticoagulant + antiplatelet therapy | 0 (0%) | 0 (0%) | |
| Device type | 0.355 | ||
| Single-chamber pacemaker | 0 (0%) | 5 (17%) | |
| Dual-chamber pacemaker | 5 (71%) | 14 (47%) | |
| Biventricular pacemaker | 0 (0%) | 3 (10%) | |
| Single-chamber cardioverter-defibrillator | 1 (14%) | 5 (17%) | |
| Dual-chamber cardioverter-defibrillator | 1 (14%) | 0 (0%) | |
| Biventricular cardioverter-defibrillator | 0 (0%) | 3 (10%) | |
| Complications | 0 (0%) | 0 (0%) | 1.000 |
| Total number of implanted leads | 13 (0) | 52 (0) | |
| Average number of leads per patient | 1.9 (0.4) | 1.7 (0.6) | 0.597 |
| Procedural time (min) | 62.9 (15.3) | 59.8 (30.1) | 0.797 |
| X-ray time (min) | 2.0 (1.8, 3.3) | 2.5 (1.7, 6.2) | 0.575 |
| Axillary vein depth (mm) | 21.6 (6.1) | 22.8 (6.3) | 0.659 |
| Axillary vein diameter with tidal breathing (mm) | 0.9 (0.4) | 3.2 (1.6) | 0.001 |
| Axillary vein diameter with Valsalva maneuver (mm) | 1.3 (0.6) | 9.2 (2.5) | <0.0001 |
| Axillary vein diameter increase with Valsalva maneuver (mm) | 0.5 (0.3) | 6.0 (2.8) | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sassone, B.; Bertagnin, E.; Virzì, S.; Simeti, G.; Tolomeo, P. Feasibility of Ultrasound-Guided Axillary Vein Puncture under Valsalva Maneuver for Diagnostic and Cardiovascular Interventional Purposes: Pacemaker and Cardioverter-Defibrillator Implantation. Diagnostics 2023, 13, 3274. https://doi.org/10.3390/diagnostics13203274
Sassone B, Bertagnin E, Virzì S, Simeti G, Tolomeo P. Feasibility of Ultrasound-Guided Axillary Vein Puncture under Valsalva Maneuver for Diagnostic and Cardiovascular Interventional Purposes: Pacemaker and Cardioverter-Defibrillator Implantation. Diagnostics. 2023; 13(20):3274. https://doi.org/10.3390/diagnostics13203274
Chicago/Turabian StyleSassone, Biagio, Enrico Bertagnin, Santo Virzì, Giuseppe Simeti, and Paolo Tolomeo. 2023. "Feasibility of Ultrasound-Guided Axillary Vein Puncture under Valsalva Maneuver for Diagnostic and Cardiovascular Interventional Purposes: Pacemaker and Cardioverter-Defibrillator Implantation" Diagnostics 13, no. 20: 3274. https://doi.org/10.3390/diagnostics13203274