
MMP-13, VEGF, and Disease Activity in a Cohort of Rheumatoid Arthritis Patients
 , , ,
, , ,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects and Clinical Assessment
2.2. Sample Collection
2.3. Immunological Investigations
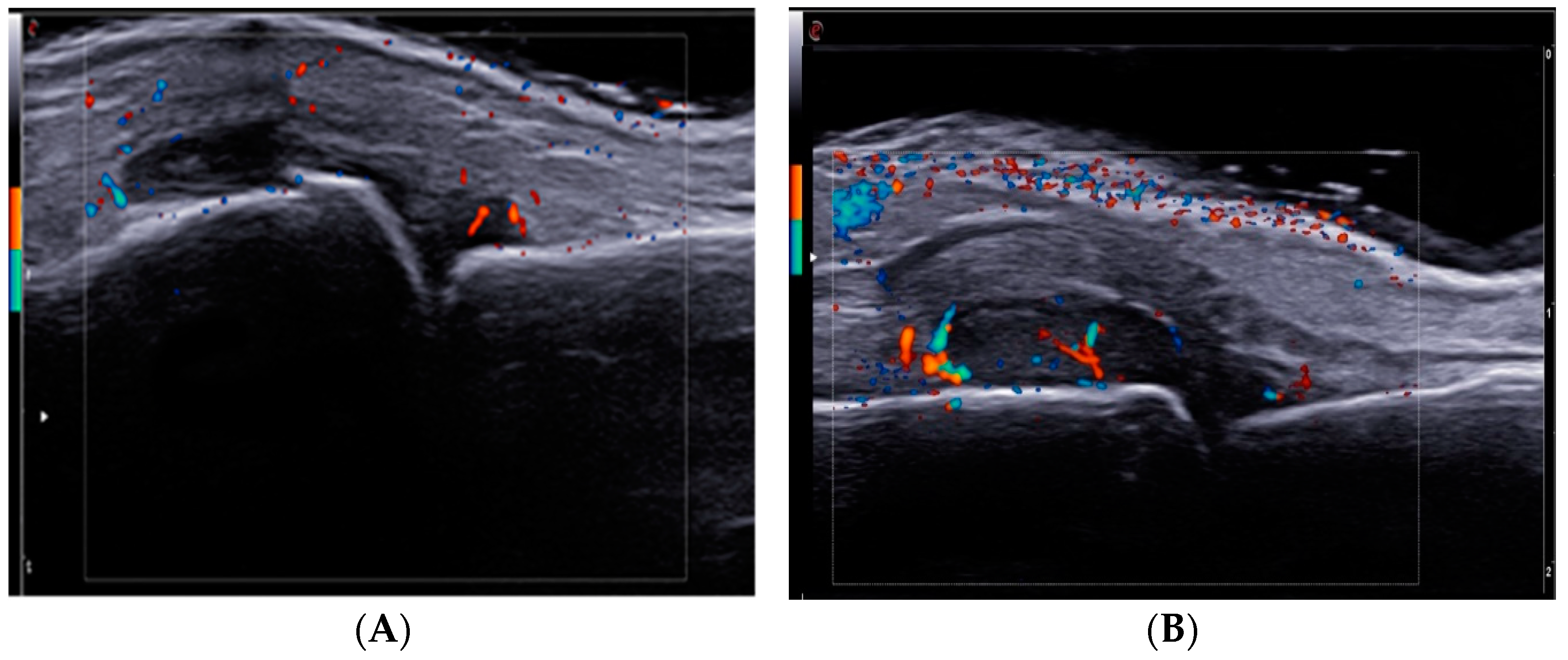
2.4. Ultrasound Examination
2.5. Ethical Issue
2.6. Statistical Analysis
3. Results
3.1. Demographics and Clinical Characteristics of the Study Subjects
3.2. Concentrations of Serum MMP-13, VEGF, TNF and IL-6 Levels and Correlations with Disease Activity Scores
3.3. Correlations between Serum Concentrations of MMP-13, VEGF, TNF-α, IL-6 and Ultrasonographic Parameters
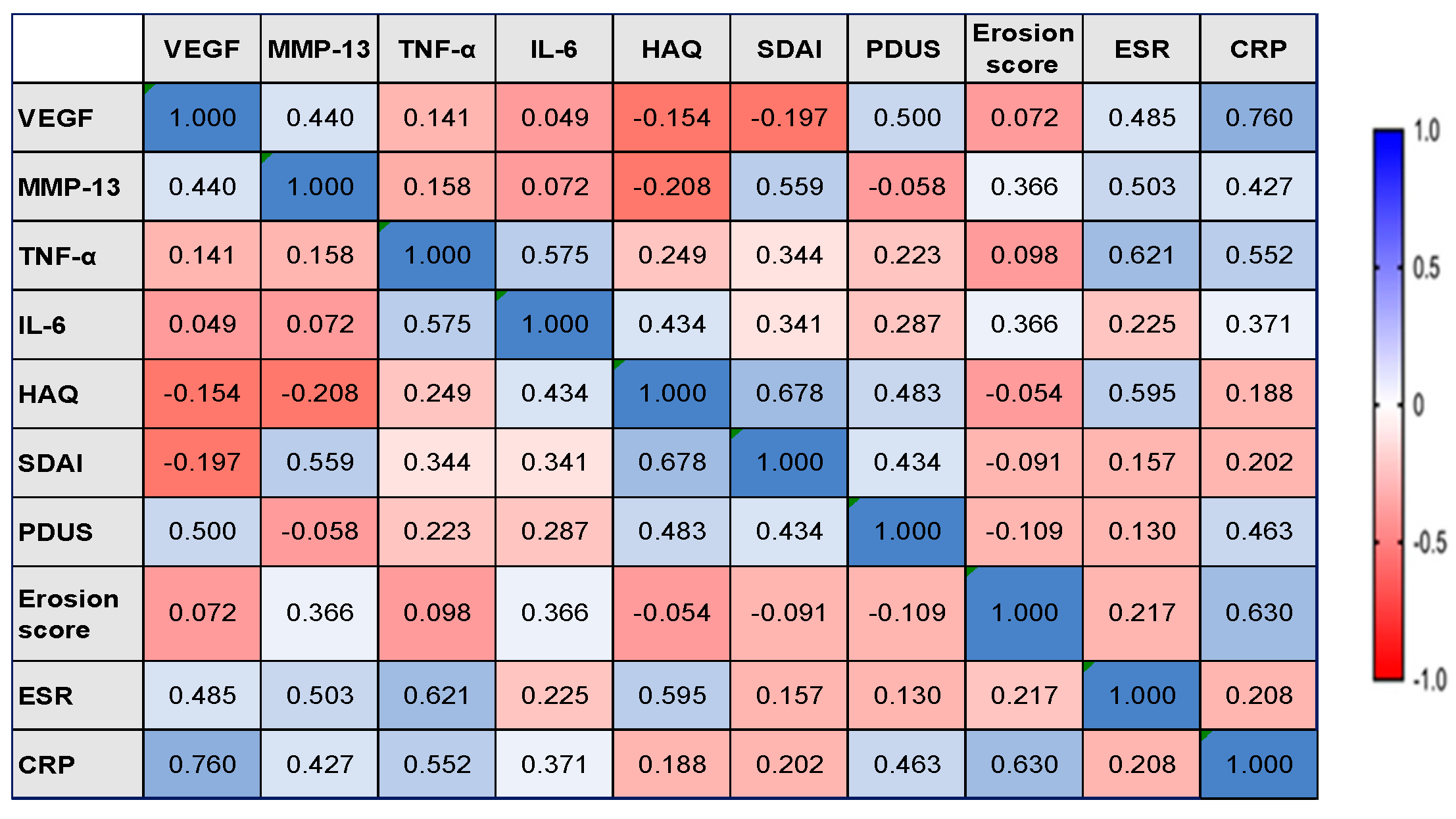
3.4. Correlations between the Serum Concentrations of MMP-13, VEGF, TNF-α, IL-6, and Inflammatory Markers
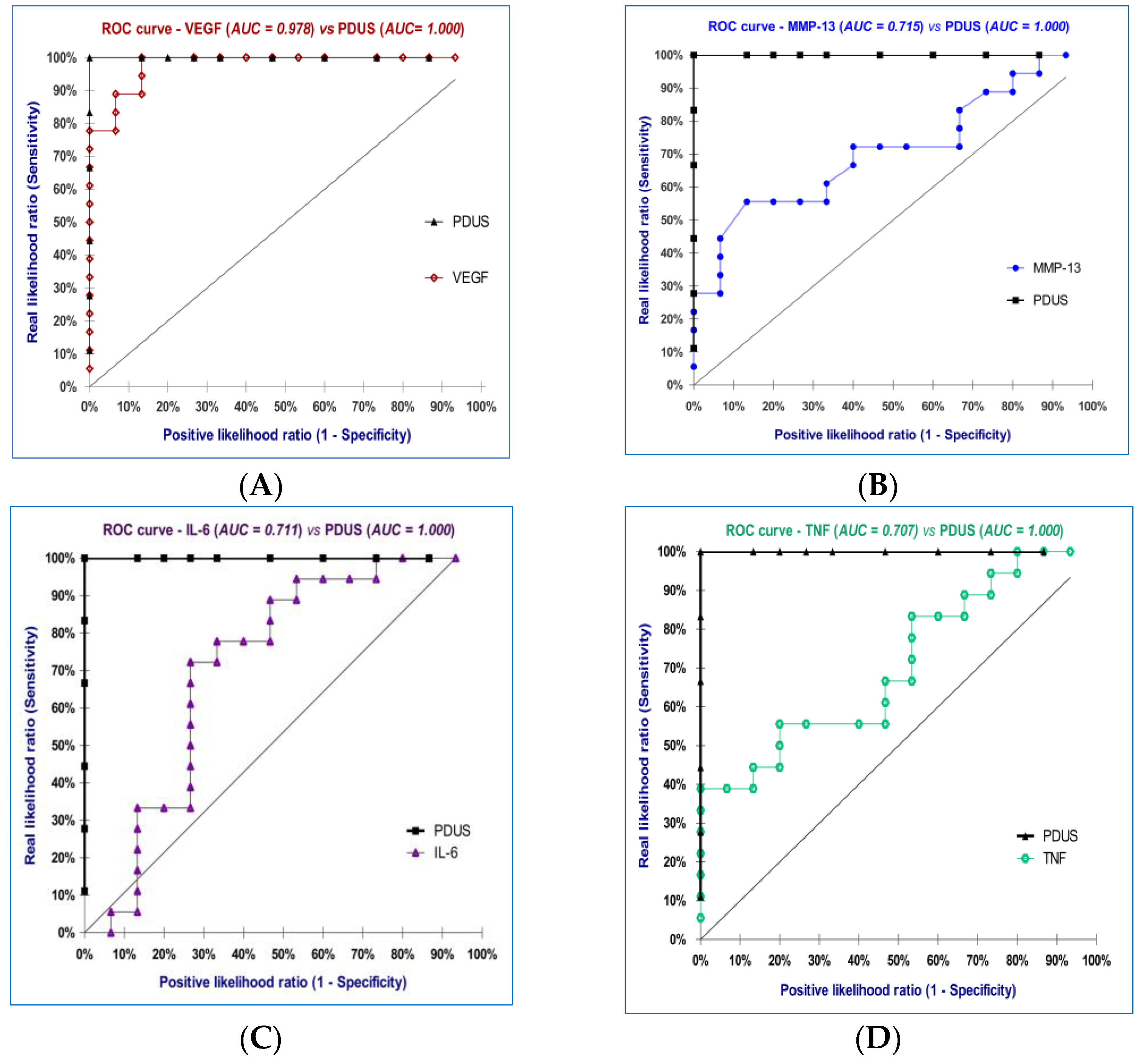
3.5. Diagnostic Accuracy of the Biomarkers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pucino, V.; Certo, M.; Varricchi, G.; Marone, G.; Ursini, F.; Rossi, F.W.; De Paulis, A.; Mauro, C.; Raza, K.; Buckley, C.D. Metabolic Checkpoints in Rheumatoid Arthritis. Front. Physiol. 2020, 11, 347. [Google Scholar] [CrossRef] [PubMed]
- Humby, F.; Lewis, M.; Ramamoorthi, N.; Hackney, J.A.; Barnes, M.R.; Bombardieri, M.; Setiadi, A.F.; Kelly, S.; Bene, F.; DiCicco, M.; et al. Synovial cellular and molecu-lar signatures stratify clinical response to csDMARD therapy and predict radiographic progression in early rheumatoid ar-thritis patients. Ann. Rheum. Dis. 2019, 78, 761–772. [Google Scholar] [CrossRef] [PubMed]
- Yap, H.Y.; Tee, S.Z.; Wong, M.M.; Chow, S.K.; Peh, S.C.; Teow, S.Y. Pathogenic Role of Immune Cells in Rheumatoid Ar-thritis: Implications in Clinical Treatment and Biomarker Development. Cells 2018, 7, 161. [Google Scholar] [CrossRef] [PubMed]
- Iain, B.; McInnes, F.R.C.P.; Schett, G. The Pathogenesis of Rheumatoid Arthritis. N. Engl. J. Med. 2011, 365, 2205–2219. [Google Scholar]
- Lee, S.Y.; Yoon, B.Y.; Kim, J.I.; Heo, Y.M.; Woo, Y.J.; Park, S.H.; Kim, H.Y.; Kim, S.I.; Cho, M.L. Interleukin-17 increases the expression of Toll-like receptor 3 via the STAT3 pathway in rheumatoid arthritis fibroblast-like synoviocytes. Immunology 2014, 141, 353–361. [Google Scholar] [CrossRef]
- Bartok, B.; Firestein, G.S. Fibroblast-like synoviocytes: Key effector cells in rheumatoid arthritis. Immunol. Rev. 2010, 233, 233–255. [Google Scholar] [CrossRef]
- Griffioen, A.W.; Molema, G. Angiogenesis: Potentials for pharmacologic intervention in the treatment of cancer, cardiovascular diseases, and chronic inflammation. Pharmacol. Rev. 2000, 52, 237–268. [Google Scholar] [PubMed]
- Bikfalvi, A. History and conceptual developments in vascular biology and angiogenesis research: A personal view. Angiogenesis 2017, 20, 463–478. [Google Scholar] [CrossRef]
- Nowak-Sliwinska, P.; Alitalo, K.; Allen, E.; Anisimov, A.; Aplin, A.C.; Auerbach, R.; Augustin, H.G.; Bates, D.O.; van Beijnum, J.R.; Bender, R.; et al. Consensus guidelines for the use and interpretation of angiogenesis assays. Angiogenesis 2018, 21, 425–532. [Google Scholar] [CrossRef]
- Elshabrawy, H.A.; Chen, Z.; Volin, M.V.; Ravella, S.; Virupannavar, S.; Shahrara, S. The pathogenic role of angiogenesis in rheumatoid arthritis. Angiogenesis 2015, 18, 433–448. [Google Scholar] [CrossRef]
- Fava, R.A.; Olsen, N.J.; Spencer-Green, G.; Yeo, K.T.; Yeo, T.K.; Berse, B.; Jackman, R.W.; Senger, D.R.; Dvorak, H.F.; Brown, L.F. Vascular permeability factor/endothelial growth factor (VPF/VEGF): Accumulation and expression in human synovial fluids and rheumatoid synovial tissue. J. Exp. Med. 1994, 180, 341–346. [Google Scholar] [CrossRef] [PubMed]
- Koch, A.E.; Harlow, L.A.; Haines, G.K.; Amento, E.P.; Unemori, E.N.; Wong, W.L.; Pope, R.M.; Ferrara, N. Vascular endothelial growth factor. A cytokine modulating endothelial function in rheumatoid arthritis. J. Immunol. 1994, 152, 4149–4156. [Google Scholar] [CrossRef] [PubMed]
- Yoo, S.-A.; Bae, D.-G.; Ryoo, J.-W.; Kim, H.-R.; Park, G.-S.; Cho, C.-S.; Chae, C.-B.; Kim, W.-U. Arginine-Rich Anti-Vascular Endothelial Growth Factor (Anti-VEGF) Hexapeptide Inhibits Collagen-Induced Arthritis and VEGF-Stimulated Productions of TNF- α and IL-6 by Human Monocytes. J. Immunol. 2005, 174, 5846–5855. [Google Scholar] [CrossRef] [PubMed]
- Mould, A.W.; Tonks, I.D.; Cahill, M.M.; Pettit, A.R.; Thomas, R.; Hayward, N.K.; Kay, G.F. Vegfb gene knockout mice display reduced pathology and synovial angiogenesis in both antigen-induced and collagen-induced models of arthritis. Arthritis Rheum. 2003, 48, 2660–2669. [Google Scholar] [CrossRef]
- Paleolog, E.M. Angiogenesis: A critical process in the pathogenesis of RA—A role for VEGF? Br. J. Rheumatol. 1996, 35, 917–919. [Google Scholar] [CrossRef]
- Kim, H.-R.; Kim, K.-W.; Kim, B.-M.; Cho, M.-L.; Lee, S.-H. The Effect of Vascular Endo-thelial Growth Factor on Osteoclasto-genesis in Rheumatoid Arthritis. PLoS ONE 2015, 10, e0124909. [Google Scholar]
- Wojdasiewicz, P.; Wajda, A.; Haładyj, E.; Romanowska-Próchnicka, K.; Felis-Giemza, A.; Nałęcz-Janik, J.; Walczyk, M.; Olesińska, M.; Tarnacka, B.; Paradowska-Gorycka, A. IL-35, TNF-α, BAFF, and VEGF serum levels in patients with different rheumatic diseases. Reumatologia 2019, 57, 145–150. [Google Scholar] [CrossRef]
- Paleolog, E.M. Angiogenesis in rheumatoid arthritis. Arthritis Res. Ther. 2002, 4, S81. [Google Scholar] [CrossRef]
- Lee, Y.H.; Bae, S.C. Correlation between circulating VEGF levels and disease activity in rheumatoid arthritis: A meta-analysis. Z. Rheumatol. 2018, 77, 240–248. [Google Scholar] [CrossRef]
- Kanbe, K.; Inoue, K.; Inoue, Y.; Suzuki, Y. Histological analysis of synovium in cases of effect attenuation associated with infliximab therapy in rheumatoid arthritis. Clin. Rheumatol. 2008, 27, 777–781. [Google Scholar] [CrossRef]
- Kim, J.W.; Kong, J.S.; Lee, S.; Yoo, S.A.; Koh, J.H.; Jin, J.; Kim, W.U. Angiogenic cytokines can reflect the synovitis severity and treatment response to biologics in rheumatoid arthritis. Exp. Mol. Med. 2020, 52, 843–853. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Maged, A.E.-S.; Gad, A.M.; Abdel-Aziz, A.K.; Aboulwafa, M.M.; Azab, S.S. Comparative study of anti-VEGF Ranibizumab and Interleukin-6 receptor antago-nist Tocilizumab in Adjuvant-induced Arthritis. Toxicol. Appl. Pharmacol. 2018, 356, 65–75. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Maged, A.E.; Gad, A.M.; Wahdan, S.A.; Azab, S.S. Efficacy and safety of Ramucirumab and methotrexate cotherapy in rheumatoid arthritis experimental model: Involvement of angiogenic and immunomodulatory signaling. Toxicol. Appl. Pharmacol. 2019, 380, 114702. [Google Scholar] [CrossRef] [PubMed]
- van Nieuwenhuijze, A.E.; van de Loo, F.A.; Walgreen, B.; Bennink, M.; Helsen, M.; van den Bersselaar, L.; Wicks, I.P.; van den Berg, W.B.; Koenders, M.I. Complementary action of granulocyte macrophage colony-stimulating factor and interleukin-17A induces inter-leukin-23, receptor activator of nuclear factor-kappa B ligand, and matrix metalloproteinases and drives bone and cartilage pathology in experimental arthritis: Rationale for combination therapy in rheumatoid arthritis. Arthritis Res. Ther. 2015, 17, 163. [Google Scholar] [PubMed]
- Stahle-Backdahl, M.; Sandstedt, B.; Bruce, K.; Lindahl, A.; Jimenez, M.G.; Vega, J.A.; Lopez-Otin, C. Collagenase-3 (MMP-13) is ex-pressed during human fetal ossification and re-expressed in postnatal bone remodeling and in rheumatoid arthritis. Lab. Investig. 1997, 76, 717–728. [Google Scholar] [PubMed]
- Konttinen, Y.T.; Ainola, M.; Valleala, H.; Ma, J.; Ida, H.; Mandelin, J.; Kinne, R.W.; Santavirta, S.; Sorsa, T.; López-Otín, C.; et al. Analysis of 16 different matrix metalloproteinases (MMP-1 to MMP-20) in the synovial membrane: Different profiles in trauma and rheumatoid arthritis. Ann. Rheum. Dis. 1999, 58, 691–697. [Google Scholar] [CrossRef] [PubMed]
- Jüngel, A.; Ospelt, C.; Lesch, M.; Thiel, M.; Sunyer, T.; Schorr, O.; Michel, B.A.; Gay, R.E.; Kolling, C.; Flory, C.; et al. Effect of the oral application of a highly selective MMP-13 inhibitor in three different animal models of rheumatoid arthritis. Ann. Rheum. Dis. 2010, 69, 898–902. [Google Scholar] [CrossRef]
- Kim, S.J.; Shin, H.H.; Park, S.Y.; Lee, D.S.; Lee, E.A.; Cho, S.D.; Cho, H.R.; Miyazawa, K.; Choi, H.S. Induction of MMP-13 expression by soluble human glucocorticoid-induced tumor necrosis factor receptor in fibroblast-like synovial cells. Osteoarthr. Cartil. 2006, 14, 146–153. [Google Scholar] [CrossRef]
- Goldring, M.B.; Otero, M.; Plumb, D.A.; Dragomir, C.; Favero, M.; El Hachem, K.; Hashimoto, K.; Roach, H.I.; Olivotto, E.; Borzi, R.M.; et al. Roles of inflammatory and anabolic cytokines in cartilage metabolism: Signals and multiple effectors con-verge upon MMP-13 regulation in osteoarthritis. Eur. Cells Mater. 2011, 21, 202–220. [Google Scholar] [CrossRef]
- Nakamura, H.; Shibakawa, A.; Tanaka, M.; Kato, T.; Nishioka, K. Effects of glucosamine hydrochloride on the production of prostaglandin E2, nitric oxide and metalloproteases by chondrocytes and synoviocytes in osteoarthritis. Clin. Exp. Rheumatol. 2004, 22, 293–299. [Google Scholar]
- Little, C.B.; Barai, A.; Burkhardt, D.; Smith, S.M.; Fosang, A.J.; Werb, Z.; Shah, M.; Thompson, E.W. Matrix metalloproteinase 13-deficient mice are resistant to osteoarthritic cartilage erosion but not chondrocyte hypertrophy or osteophyte develop-ment. Arthritis Rheum. 2009, 60, 3723–3733. [Google Scholar] [CrossRef] [PubMed]
- Liacini, A.; Sylvester, J.; Li, W.Q.; Huang, W.; Dehnade, F.; Ahmad, M.; Zafarullah, M. Induction of matrix metalloprotein-ase-13 gene expression by TNF-alpha is mediated by MAP kinases, AP-1, and NF-kappaB transcription factors in articular chondrocytes. Exp. Cell Res. 2003, 288, 208–217. [Google Scholar] [CrossRef] [PubMed]
- Mengshol, J.A.; Vincenti, M.P.; Coon, C.I.; Barchowsky, A.; Brinckerhoff, C.E. Interleukin-1 induction of collagenase 3 (ma-trix metalloproteinase 13) gene expression in chondrocytes requires p38, c-Jun N-terminal kinase, and nuclear factor kappaB: Differential regulation of collagenase 1 and collagenase 3. Arthritis Rheum. 2000, 43, 801–811. [Google Scholar] [CrossRef] [PubMed]
- Shen, P.; Jiao, Z.; Zheng, J.S.; Xu, W.F.; Zhang, S.Y.; Qin, A.; Yang, C. Injecting vascular endothelial growth factor into the temporomandibular joint induces osteoarthritis in mice. Sci. Rep. 2015, 5, 16244. [Google Scholar] [CrossRef]
- Selvaraj, D.; Gangadharan, V.; Michalski, C.W.; Kurejova, M.; Stösser, S.; Srivastava, K.; Schweizerhof, M.; Waltenberger, J.; Ferrara, N.; Heppenstall, P.; et al. A Functional Role for VEGFR1 Expressed in Peripheral Sensory Neurons in Cancer Pain. Cancer Cell 2015, 27, 780–796. [Google Scholar] [CrossRef] [PubMed]
- Barbulescu, A.L.; Ciurea, P.L.; Mitran, C.; Chisalau, B.A.; Parvanescu, C.D.; Firulescu, S.C.; Balasoiu, M.; Boldeanu, M.V.; Popoviciu, H.; Vreju, F.A. High-frequency ultrasonography of the hand versus anti-RA33 evaluation in early rheumatoid ar-thritis—A pilot study. Med. Ultrason. 2017, 19, 166–171. [Google Scholar] [CrossRef]
- Vreju, F.A.; Ciurea, M.E.; Popa, D.; Popa, F.; Parvanescu, C.D.; Chisalau, B.A.; Barbulescu, A.L.; Parvanescu, V.; Rosu, A.; Ciurea, P.L. Ultrasonography in the diagnosis and management of non inflammatory conditions of the hand and wrist. Med. Ultrason. 2016, 18, 90–95. [Google Scholar] [CrossRef]
- Ben Abdelghani, K.; Miladi, S.; Makhlouf, Y.; Fazaa, A.; Sallemi, M.; Souebni, L.; Ouenniche, K.; Kassab, S.; Chekili, S.; Ben Salem, K.; et al. Validity of Remission Criteria in Rheumatoid Arthritis Compared to Ultrasound-Defined Remission. Sultan Qaboos Univ. Med. J. 2022, 22, 554–560. [Google Scholar] [CrossRef]
- Wang, X.; Qian, G.; Duan, H. Diagnostic Value of Musculoskeletal Ultrasound in Rheumatoid Finger Arthritis. J. Coll. Physicians Surg. Pak. 2020, 30, 617–621. [Google Scholar] [CrossRef]
- Combe, B.; Landewe, R.; Daien, C.I.; Hua, C.; Aletaha, D.; Álvaro-Gracia, J.M.; Bakkers, M.; Brodin, N.; Burmester, G.R.; Codreanu, C.; et al. 2016 update of the EULAR recommendations for the management of early arthritis. Ann. Rheum. Dis. 2017, 76, 948–959. [Google Scholar] [CrossRef]
- Quinn, M.A.; Green, M.J.; Marzo-Ortega, H.; Proudman, S.; Karim, Z.; Wakefield, R.J.; Conaghan, P.G.; Emery, P. Prognostic factors in a large cohort of patients with early undifferentiated inflammatory arthritis after application of a structured management protocol. Arthritis Rheum. 2003, 48, 3039–3045. [Google Scholar] [CrossRef] [PubMed]
- van Aken, J.; van Bilsen, J.H.; Allaart, C.F.; Huizinga, T.W.; Breedveld, F.C. The Leiden early arthritis clinic. Clin. Exp. Rheumatol. 2003, 21, S100–S105. [Google Scholar] [PubMed]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O., III; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 Rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010, 62, 2569–2581. [Google Scholar] [CrossRef] [PubMed]
- Low, A.S.; Symmons, D.P.; Lunt, M.; Mercer, L.K.; Gale, C.P.; Watson, K.D.; Dixon, W.G.; Hyrich, K.L.; British Society for Rheumatology Biologics Register for Rheumatoid Arthritis (BSRBR-RA) and the BSRBR Control Centre Consortium. Relationship between exposure to tumor necrosis factor inhibitor therapy and incidence and severity of myocardial infarction in patients with rheumatoid arthritis. Ann. Rheum. Dis. 2017, 76, 654–660. [Google Scholar] [CrossRef]
- Wells, G.; Becker, J.C.; Teng, J.; Dougados, M.; Schiff, M.; Smolen, J.; Aletaha, D.; van Riel, P.L. Validation of the 28-joint Disease Activity Score (DAS28) and European League Against Rheumatism response criteria based on C-reactive protein against disease progression in patients with rheumatoid arthritis, and comparison with the DAS28 based on erythrocyte sedimentation rate. Ann. Rheum. Dis. 2009, 68, 954–960. [Google Scholar] [CrossRef]
- Bruce, B.; Fries, J.F. The Health Assessment Questionnaire (HAQ). Clin. Exp. Rheumatol. 2005, 23, S14–S18. [Google Scholar] [PubMed]
- Smolen, J.S.; Breedveld, F.C.; Schiff, M.H.; Kalden, J.R.; Emery, P.; Eberl, G.; van Riel, P.L.; Tugwell, P. A simplified dis-ease activity index for rheumatoid arthritis for use in clinical practice. Rheumatology 2003, 42, 244–257. [Google Scholar] [CrossRef]
- D’Agostino, M.A.; Terslev, L.; Aegerter, P.; Backhaus, M.; Balint, P.; Bruyn, G.A.; Filippucci, E.; Grassi, W.; Iagnocco, A.; Jousse-Joulin, S.; et al. Scoring ultrasound synovitis in rheumatoid arthritis: A EULAR-OMERACT ultrasound taskforce—Part 1: Definition and development of a standardized, consensus-based scoring system. RMD Open 2017, 3, e000428. [Google Scholar] [CrossRef]
- Backhaus, M.; Ohrndorf, S.; Kellner, H.; Strunk, J.; Backhaus, T.M.; Hartung, W.; Sattler, H.; Albrecht, K.; Kaufmann, J.; Becker, K.; et al. Evaluation of a novel 7-joint ultrasound score in daily rheumatologic practice: A pilot project. Arthritis Rheum. 2009, 61, 1194–1201. [Google Scholar] [CrossRef]
- Szkudlarek, M.; Court-Payen, M.; Jacobsen, S.; Klarlund, M.; Thomsen, H.S.; Østergaard, M. Interobserver agreement in ultrasonography of the finger and toe joints in rheumatoid arthritis. Arthritis Rheum. 2003, 48, 955–962. [Google Scholar] [CrossRef]
- Siloşi, I.; Boldeanu, M.V.; Cojocaru, M.; Biciuşcă, V.; Pădureanu, V.; Bogdan, M.; Badea, R.G.; Avramescu, C.; Petrescu, I.O.; Petrescu, F.; et al. The Relationship of Cytokines IL-13 and IL-17 with Autoantibodies Profile in Early Rheumatoid Arthritis. J. Immunol. Res. 2016, 2016, 3109135. [Google Scholar] [CrossRef] [PubMed]
- Siloşi, I.; Boldeanu, L.; Biciuşcă, V.; Bogdan, M.; Avramescu, C.; Taisescu, C.; Padureanu, V.; Boldeanu, M.V.; Dricu, A.; Siloşi, C.A. Serum Biomarkers for Discrimination between Hepatitis C-Related Arthropathy and Early Rheumatoid Arthritis. Int. J. Mol. Sci. 2017, 18, 1304. [Google Scholar] [CrossRef] [PubMed]
- Silosi, I.; Cojocaru, M.; Foia, L.; Boldeanu, M.V.; Petrescu, F.; Surlin, P.; Biciusca, V. Significance of Circulating and Crevicular Matrix Metalloproteinase-9 in Rheumatoid Arthritis-Chronic Periodontitis Association. J. Immunol. Res. 2015, 2015, 218060. [Google Scholar] [CrossRef] [PubMed]
- Macías, I.; García-Pérez, S.; Ruiz-Tudela, M.; Medina, F.; Chozas, N.; Girón-González, J.A. Modification of pro- and anti-inflammatory cytokines and vascular-related molecules by tumor necrosis factor-a blockade in patients with rheumatoid arthritis. J. Rheumatol. 2005, 32, 2102–2108. [Google Scholar]
- Tylor, P.C. Serum vascular markers and vascular imaging in assessment of rheumatoid arthritis disease activity and response to therapy. Rheumatology 2005, 44, 721–728. [Google Scholar] [CrossRef]
- Meyer, P.W.; Hodkinson, B.; Ally, M.; Musenge, E.; Wadee, A.A.; Fickl, H.; Tikly, M.; Anderson, R. Circulating cytokine profiles and their relationships with autoantibodies, acute phase reactants, and disease activity in patients with rheumatoid arthritis. Mediat. Inflamm. 2010, 2010, 158514. [Google Scholar] [CrossRef]
- Strunk, J.; Rumbaur, C.; Albrecht, K.; Neumann, E.; Müller-Ladner, U. Linking systemic angiogenic factors (VEGF, angiogenin, TIMP-2) and Doppler ultrasound to anti-inflammatory treatment in rheumatoid arthritis. Jt. Bone Spine 2013, 80, 270–273. [Google Scholar] [CrossRef]
- Clavel, G.; Bessis, N.; Lemeiter, D.; Fardellone, P.; Mejjad, O.; Ménard, J.F.; Pouplin, S.; Boumier, P.; Vittecoq, O.; Le Loët, X.; et al. Angiogenesis markers (VEGF, soluble receptor of VEGF and angiopoietin-1) in very early arthritis and their association with inflammation and joint destruction. Clin. Immunol. 2007, 124, 158–164. [Google Scholar] [CrossRef]
- Kitchen, J.; Kane, D. Greyscale and power Doppler ultrasonographic evaluation of normal synovial joints: Correlation with pro- and anti-inflammatory cytokines and angiogenic factors. Rheumatology 2015, 54, 458–462. [Google Scholar] [CrossRef]
- Algergawy, S.; Ismail, Y.M. Power Doppler Ultrasonography is an Important Technique in Rheumatoid Arthritis, Ankylosing Spondylitis and Osteoarthritis Arthritis among Egyptians. Aktuelle Rheumatol. 2015, 42, 442–447. [Google Scholar] [CrossRef]
- Misra, S.; Mondal, S.; Chatterjee, S.; Guin, A.; Sinhamahapatra, P.; Ghosh, A. Association of Angiogenic and Inflammatory Markers with Power Doppler Ultrasound Vascularity Grade and DAS28-CRP in Early Rheumatoid Arthritis: A Comparative Analysis. Biomed. Res. Int. 2018, 2018, 6906374. [Google Scholar] [CrossRef] [PubMed]
- Andersen, M.; Ellegaard, K.; Hebsgaard, J.B.; Christensen, R.; Torp-Pedersen, S.; Kvist, P.H.; Søe, N.; Rømer, J.N.; Bartels, E.M.; Danneskiold-Samsøe, B.; et al. Ultrasound colour Doppler is associated with synovial pathology in biopsies from hand joints in rheumatoid arthritis patients: A cross-sectional study. Ann. Rheum. Dis. 2014, 73, 678–683. [Google Scholar] [CrossRef] [PubMed]
- Naredo, E.; Collado, P.; Cruz, A.; Palop, M.J.; Cabero, F.; Richi, P.; Carmona, L.; Crespo, M. Longitudinal power Doppler ultrasonographic assessment of joint inflammatory activity in early rheumatoid arthritis: Predictive value in disease activity and radiologic progression. Arthritis Rheum. 2007, 57, 116–124. [Google Scholar] [CrossRef] [PubMed]
- Foltz, V.; Gandjbakhch, F.; Etchepare, F.; Rosenberg, C.; Tanguy, M.L.; Rozenberg, S.; Bourgeois, P.; Fautrel, B. Power Doppler ultrasound, but not low-field magnetic resonance imaging, predicts relapse and radiographic disease progression in rheumatoid arthritis patients with low levels of disease activity. Arthritis Rheum. 2012, 64, 67–76. [Google Scholar] [CrossRef]
- Bhasin, S.; Cheung, P.P. The role of power doppler ultrasonography as disease activity marker in rheumatoid arthritis. Dis. Markers 2015, 2015, 325909. [Google Scholar] [CrossRef] [PubMed]
- Mandl, P.; Kurucz, R.; Niedermayer, D.; Balint, P.V.; Smolen, J.S. Contributions of ultrasound beyond clinical data in assessing inflammatory disease activity in rheumatoid arthritis: Current insights and future prospects. Rheumatology 2014, 53, 2136–2142. [Google Scholar] [CrossRef] [PubMed]
- Kawashiri, S.Y.; Kawakami, A.; Iwamoto, N.; Fujikawa, K.; Satoh, K.; Tamai, M.; Nakamura, H.; Okada, A.; Koga, T.; Yamasaki, S.; et al. The power Doppler ultrasonography score from 24 synovial sites or 6 simplified synovial sites, including the metacarpophalangeal joints, reflects the clinical disease activity and level of serum biomarkers in patients with rheumatoid arthritis. Rheumatology 2011, 50, 962–965. [Google Scholar] [CrossRef] [PubMed]
- Dahlberg, L.; Billinghurst, R.C.; Manner, P.; Nelson, F.; Webb, G.; Ionescu, M.; Reiner, A.; Tanzer, M.; Zukor, D.; Chen, J.; et al. Selective enhancement of collagenase-mediated cleavage of resident type II collagen in cultured osteoarthritic cartilage and arrest with a synthetic inhibitor that spares collagenase 1 (matrix metalloproteinase 1). Arthritis Rheum. 2000, 43, 673–682. [Google Scholar] [CrossRef]
- Aigner, T.; Zien, A.; Gehrsitz, A.; Gebhard, P.M.; McKenna, L. Anabolic and catabolic gene expression pattern analysis in normal versus osteoarthritic cartilage using complementary DNA-array technology. Arthritis Rheum. 2001, 44, 2777–2789. [Google Scholar] [CrossRef]
- Bau, B.; Gebhard, P.M.; Haag, J.; Knorr, T.; Bartnik, E.; Aigner, T. Relative messenger RNA expression profiling of collagenases and aggrecanases in human articular chondrocytes in vivo and in vitro. Arthritis Rheum. 2002, 46, 2648–2657. [Google Scholar] [CrossRef]
- Davidson, R.K.; Waters, J.G.; Kevorkian, L.; Darrah, C.; Cooper, A.; Donell, S.T.; Clark, I.M. Expression profiling of metalloproteinases and their inhibitors in synovium and cartilage. Arthritis Res. Ther. 2006, 8, R124. [Google Scholar] [CrossRef] [PubMed]
- Kevorkian, L.; Young, D.A.; Darrah, C.; Donell, S.T.; Shepstone, L.; Porter, S.; Brockbank, S.M.; Edwards, D.R.; Parker, A.E.; Clark, I.M. Expression profiling of metalloproteinases and their inhibitors in cartilage. Arthritis Rheum. 2004, 50, 131–141. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Li, M.; Zeng, J.; Feng, Z.; Yang, J.; Shen, B.; Zeng, Y. Differential Expression of Renin-Angiotensin System-related Components in Patients with Rheumatoid Arthritis and Osteoarthritis. Am. J. Med. Sci. 2020, 359, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Hirata, S.; Dirven, L.; Shen, Y.; Centola, M.; Cavet, G.; Lems, W.F.; Tanaka, Y.; Huizinga, T.W.; Allaart, C.F. A multi-biomarker score measures rheumatoid arthritis disease activity in the BeSt study. Rheumatology 2013, 52, 1202–1207. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter (Mean ± SD) | C (n = 12) | L (n = 15) | M (n = 19) | p-Value |
|---|---|---|---|---|
| Age [years] | 50.36 ± 13.38 | 52.14 ± 10.20 | 54.70 ± 10.30 | 0.356 |
| Urban (%) | 6 (50.00%) | 7 (46.67%) | 7 (36.84%) | - |
| Rural (%) | 6 (50.00%) | 8 (53.33%) | 12 (63.16%) | - |
| ESR (mm/h) | 10.41 ± 4.36 | 53.90 ± 15.70 | 65.00 ± 20.10 | 0.054 |
| RF (U/L) | 2.54 ± 1.98 | 64.60 ± 39.70 | 103.00 ± 99.20 | 0.307 |
| CRP (mg/L) | 4.31 ± 1.67 | 31.50 ± 15.10 | 36.30 ± 14.80 | 0.322 |
| HAQ | - | 1.60 (1.10–2.10) | 1.77 (1.18–2.10) | 0.357 |
| SDAI | - | 28.50 ± 5.61 | 32.10 ± 5.85 | 0.175 |
| PDUS score | - | 9.60 ± 2.72 | 17.33 ± 1.64 | <0.0001 * |
| Erosion score | - | 2.00 ± 0.85 | 4.67 ± 1.64 | <0.0001 * |
| Parameter | Moderate RA (n = 19) | Low RA (n = 15) | ||||
|---|---|---|---|---|---|---|
| Moderate | Control | p | Low | Control | p | |
| VEGF (pg/mL) (Mean ± SD) | 1112.00 ± 269.00 | 386.00 ± 62.20 | <0.0001 | 590.00 ± 136.00 | 386.00 ± 62.20 | 0.0002 |
| MMP-13 (pg/mL) Median (Interquartile range) | 882.00 (388.00 – 1040.00) | 402.00 (369.00 – 437.00) | 0.023 | 413.00 (360.00 – 497.00) | 402.00 (369.00 – 437.00) | 0.625 |
| TNF-α (pg/mL) (Mean ± SD) | 24.20 ± 5.25 | 14.20 ± 3.20 | <0.0001 | 20.30 ± 3.26 | 14.20 ± 3.20 | 0.0005 |
| IL-6 (pg/mL) (Mean ± SD) | 27.40 ± 5.38 | 15.90 ± 3.86 | <0.0001 | 22.70 ± 8.49 | 15.90 ± 3.86 | 0.026 |
| Parameter | VEGF | MMP-13 | TNF | IL-6 |
|---|---|---|---|---|
| L group (Low RA DAS28(4v) CRP) | rho = 0.001 p = 0.998 | rho = 0.580 p = 0.023 * | rho = −0.071 p = 0.801 | rho = 0.477 p = 0.072 |
| M group (Moderate RA DAS28(4v) CRP) | rho = 0.240 p = 0.338 | rho = 0.530 p = 0.024 * | rho = −0.128 p = 0.613 | rho = 0.148 p = 0.558 |
| Parameter | AUC | Threshold Values | Sensitivity % | Specificity % | Youden Index | p-Value |
|---|---|---|---|---|---|---|
| VEGF | 0.978 | 926.10 | 77.78 | 100.00 | 0.778 | <0.0001 |
| MMP-13 | 0.715 | 703.10 | 55.56 | 86.67 | 0.412 | 0.039 |
| IL-6 | 0.711 | 24.17 | 72.22 | 73.33 | 0.456 | 0.036 |
| TNF-α | 0.707 | 23.36 | 55.56 | 80.00 | 0.356 | 0.043 |
| CRP | 0.691 | 29.46 | 55.56 | 66.67 | 0.222 | 0.032 |
| PDUS | 1.000 | 14.50 | 100.00 | 100.00 | 1.000 | <0.0001 |
| DAS28(4v) CRP | 1.000 | 3.70 | 100.00 | 100.00 | 1.000 | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boldeanu, M.V.; Boldeanu, L.; Cristea, O.M.; Ciobanu, D.A.; Poenariu, S.I.; Dijmărescu, A.L.; Bărbulescu, A.L.; Pădureanu, V.; Sas, T.N.; Dinescu, Ș.C.; et al. MMP-13, VEGF, and Disease Activity in a Cohort of Rheumatoid Arthritis Patients. Diagnostics 2023, 13, 1653. https://doi.org/10.3390/diagnostics13091653
Boldeanu MV, Boldeanu L, Cristea OM, Ciobanu DA, Poenariu SI, Dijmărescu AL, Bărbulescu AL, Pădureanu V, Sas TN, Dinescu ȘC, et al. MMP-13, VEGF, and Disease Activity in a Cohort of Rheumatoid Arthritis Patients. Diagnostics. 2023; 13(9):1653. https://doi.org/10.3390/diagnostics13091653
Chicago/Turabian StyleBoldeanu, Mihail Virgil, Lidia Boldeanu, Oana Mariana Cristea, Dana Alexandra Ciobanu, Sabin Ioan Poenariu, Anda Lorena Dijmărescu, Andreea Lili Bărbulescu, Vlad Pădureanu, Teodor Nicuşor Sas, Ștefan Cristian Dinescu, and et al. 2023. "MMP-13, VEGF, and Disease Activity in a Cohort of Rheumatoid Arthritis Patients" Diagnostics 13, no. 9: 1653. https://doi.org/10.3390/diagnostics13091653