
Dark-Blood Late Gadolinium Enhancement MRI Is Noninferior to Bright-Blood LGE in Non-Ischemic Cardiomyopathies
 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
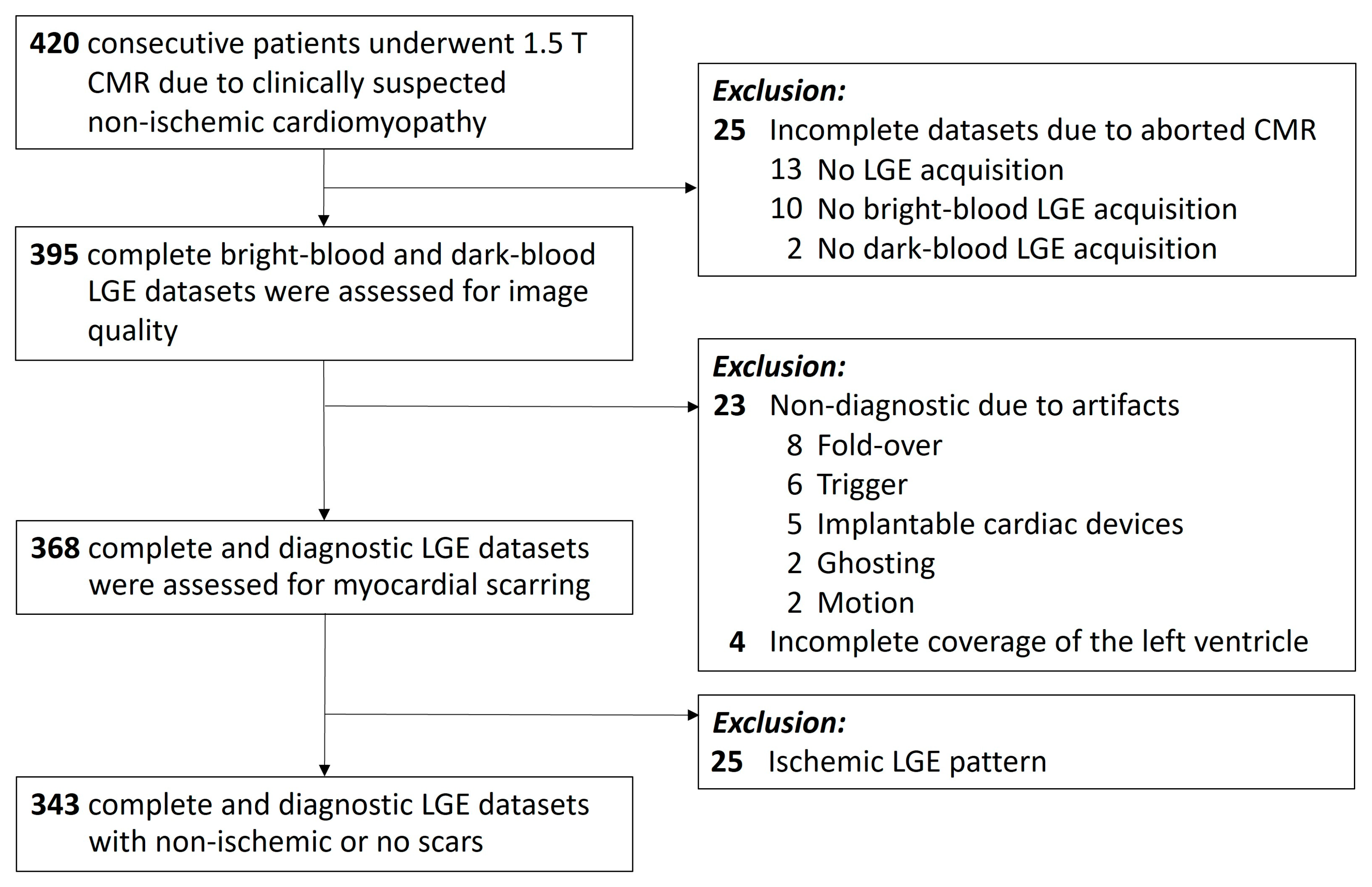
2.1. Study Population
2.2. Cardiac MRI Image Acquisition
2.3. Cardiac MRI Image Analysis
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Evaluation of Left Ventricular LGE Frequency, Pattern, and Localisation
3.3. Comparison of Total Scar Size
3.4. Reader Agreement and Diagnostic Confidence
3.5. Diagnostic Performance of Dark-Blood LGE
4. Discussion
- A prospective single-centre study enrolled patients referred for cardiac MRI for clinical suspicion of non-ischemic cardiomyopathy between January 2020 and March 2023.
- Dark-blood late gadolinium enhancement showed excellent sensitivity (99%, CI 98–100) and accuracy (99%, CI 99–100) for detecting non-ischemic scarring compared with bright-blood late gadolinium enhancement as the reference standard.
- Measurements of total scar size did not differ between dark-blood late gadolinium enhancement and bright-blood late gadolinium enhancement.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Pop, M.; Ghugre, N.R.; Ramanan, V.; Morikawa, L.; Stanisz, G.; Dick, A.J.; Wright, G. A Quantification of fibrosis in infarcted swine hearts by ex vivo late gadolinium-enhancement and diffusion-weighted MRI methods. Phys. Med. Biol. 2013, 58, 5009–5028. [Google Scholar] [CrossRef] [PubMed]
- Greulich, S.; Arai, A.E.; Sechtem, U.; Mahrholdt, H. Recent advances in cardiac magnetic resonance. F1000Research 2016, 5, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Bohl, S.; Wassmuth, R.; Abdel-Aty, H.; Rudolph, A.; Messroghli, D.; Dietz, R.; Schulz-Menger, J. Delayed enhancement cardiac magnetic resonance imaging reveals typical patterns of myocardial injury in patients with various forms of non-ischemic heart disease. Int. J. Cardiovasc. Imaging 2008, 24, 597–607. [Google Scholar] [CrossRef]
- Greulich, S.; Mayr, A.; Kitterer, D.; Latus, J.; Henes, J.; Vecchio, F.; Kaesemann, P.; Patrascu, A.; Greiser, A.; Groeninger, S.; et al. Advanced myocardial tissue characterisation by a multi-component CMR protocol in patients with rheumatoid arthritis. Eur. Radiol. 2017, 27, 4639–4649. [Google Scholar] [CrossRef] [PubMed]
- Gräni, C.; Eichhorn, C.; Bière, L.; Murthy, V.L.; Agarwal, V.; Kaneko, K.; Cuddy, S.; Aghayev, A.; Steigner, M.; Blankstein, R.; et al. Prognostic Value of Cardiac Magnetic Resonance Tissue Characterization in Risk Stratifying Patients With Suspected Myocarditis. J. Am. Coll. Cardiol. 2017, 70, 1964–1976. [Google Scholar] [CrossRef]
- Gräni, C.; Eichhorn, C.; Bière, L.; Kaneko, K.; Murthy, V.L.; Agarwal, V.; Aghayev, A.; Steigner, M.; Blankstein, R.; Jerosch-Herold, M.; et al. Comparison of myocardial fibrosis quantification methods by cardiovascular magnetic resonance imaging for risk stratification of patients with suspected myocarditis. J. Cardiovasc. Magn. Reson. 2019, 21, 1–11. [Google Scholar] [CrossRef]
- Mahrholdt, H.; Wagner, A.; Deluigi, C.C.; Kispert, E.; Hager, S.; Meinhardt, G.; Vogelsberg, H.; Fritz, P.; Dippon, J.; Bock, C.T.; et al. Presentation, patterns of myocardial damage, and clinical course of viral myocarditis. Circulation 2006, 114, 1581–1590. [Google Scholar] [CrossRef]
- Greulich, S.; Seitz, A.; Müller, K.A.L.; Grün, S.; Ong, P.; Ebadi, N.; Kreisselmeier, K.P.; Seizer, P.; Bekeredjian, R.; Zwadlo, C.; et al. Predictors of mortality in patients with biopsy-proven viral myocarditis: 10-year outcome data. J. Am. Heart Assoc. 2020, 9, e015351. [Google Scholar] [CrossRef]
- Halliday, B.P.; Baksi, A.J.; Gulati, A.; Ali, A.; Newsome, S.; Izgi, C.; Arzanauskaite, M.; Lota, A.; Tayal, U.; Vassiliou, V.S.; et al. Outcome in Dilated Cardiomyopathy Related to the Extent, Location, and Pattern of Late Gadolinium Enhancement. J. Am. Coll. Cardiol. 2019, 12, 1645–1655. [Google Scholar] [CrossRef]
- Iles, L.; Pfluger, H.; Lefkovits, L.; Butler, M.J.; Kistler, P.M.; Kaye, D.M.; Taylor, A.J. Myocardial fibrosis predicts appropriate device therapy in patients with implantable cardioverter-defibrillators for primary prevention of sudden cardiac death. J. Am. Coll. Cardiol. 2011, 57, 821–828. [Google Scholar] [CrossRef]
- Holtackers, R.J.; Van De Heyning, C.M.; Chiribiri, A.; Wildberger, J.E.; Botnar, R.M.; Kooi, M.E. Dark-blood late gadolinium enhancement cardiovascular magnetic resonance for improved detection of subendocardial scar: A review of current techniques. J. Cardiovasc. Magn. Reson. 2021, 23, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Holtackers, R.J.; Van De Heyning, C.M.; Nazir, M.S.; Rashid, I.; Ntalas, I.; Rahman, H.; Botnar, R.M.; Chiribiri, A. Clinical value of dark-blood late gadolinium enhancement cardiovascular magnetic resonance without additional magnetization preparation. J. Cardiovasc. Magn. Reson. 2019, 21, 44. [Google Scholar] [CrossRef] [PubMed]
- Holtackers, R.J.; Gommers, S.; Heckman, L.I.B.; Van De Heyning, C.M.; Chiribiri, A.; Prinzen, F.W. Histopathological Validation of Dark-Blood Late Gadolinium Enhancement MRI Without Additional Magnetization Preparation. J. Magn. Reson. Imaging 2022, 55, 190–197. [Google Scholar] [CrossRef]
- Francis, R.; Kellman, P.; Kotecha, T.; Baggiano, A.; Norrington, K.; Martinez-Naharro, A.; Nordin, S.; Knight, D.S.; Rakhit, R.D.; Lockie, T.; et al. Prospective comparison of novel dark blood late gadolinium enhancement with conventional bright blood imaging for the detection of scar. J. Cardiovasc. Magn. Reson. 2017, 19, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Monti, C.B.; Codari, M.; Cozzi, A.; Alì, M.; Saggiante, L.; Sardanelli, F.; Secchi, F. Image quality of late gadolinium enhancement in cardiac magnetic resonance with different doses of contrast material in patients with chronic myocardial infarction. Eur. Radiol. Exp. 2020, 4, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kramer, C.M.; Barkhausen, J.; Bucciarelli-Ducci, C.; Flamm, S.D.; Kim, R.J.; Nagel, E. Standardized cardiovascular magnetic resonance imaging (CMR) protocols: 2020 update. J. Cardiovasc. Magn. Reson. 2020, 22, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Holtackers, R.J.; Chiribiri, A.; Schneider, T.; Higgins, D.M.; Botnar, R.M. Dark-blood late gadolinium enhancement without additional magnetization preparation. J. Cardiovasc. Magn. Reson. 2017, 19, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Schulz-Menger, J.; Bluemke, D.A.; Bremerich, J.; Flamm, S.D.; Fogel, M.A.; Friedrich, M.G.; Kim, R.J.; von Knobelsdorff-Brenkenhoff, F.; Kramer, C.M.; Pennell, D.J.; et al. Standardized image interpretation and post-processing in cardiovascular magnetic resonance—2020 update. J. Cardiovasc. Magn. Reson. 2020, 22, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Bunck, A.C.; Baeβler, B.; Ritter, C.; Kröger, J.R.; Persigehl, T.; Pinto Santos, D.; Steinmetz, M.; Niehaus, A.; Bamberg, F.; Beer, M.; et al. Structured Reporting in Cross-Sectional Imaging of the Heart: Reporting Templates for CMR Imaging of Cardiomyopathies (Myocarditis, Dilated Cardiomyopathy, Hypertrophic Cardiomyopathy, Arrhythmogenic Right Ventricular Cardiomyopathy and Siderosis). Fortschr. Röntgenstr. 2020, 192, 27–37. [Google Scholar] [CrossRef]
- Liu, B.; Dardeer, A.M.; Moody, W.E.; Hayer, M.K.; Baig, S.; Price, A.M.; Leyva, F.; Edwards, N.C.; Steeds, R.P. Reference ranges for three-dimensional feature tracking cardiac magnetic resonance: Comparison with two-dimensional methodology and relevance of age and gender. Int. J. Cardiovasc. Imaging 2018, 34, 761–775. [Google Scholar] [CrossRef]
- Messroghli, D.R.; Moon, J.C.; Ferreira, V.M.; Grosse-Wortmann, L.; He, T.; Kellman, P.; Mascherbauer, J.; Nezafat, R.; Salerno, M.; Schelbert, E.B.; et al. Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: A consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imagi. J. Cardiovasc. Magn. Reson. 2017, 19, 75. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Hundley, W.G.; Bluemke, D.A.; Bogaert, J.; Flamm, S.D.; Fontana, M.; Friedrich, M.G.; Grosse-Wortmann, L.; Karamitsos, T.D.; Kramer, C.M.; Kwong, R.Y.; et al. Society for Cardiovascular Magnetic Resonance (SCMR) guidelines for reporting cardiovascular magnetic resonance examinations. J. Cardiovasc. Magn. Reson. 2022, 24, 1–26. [Google Scholar] [CrossRef] [PubMed]
- Tango, T. Equivalence test and confidence interval for the difference in proportions for the paired-sample design. Stat. Med. 1998, 17, 891–908. [Google Scholar] [CrossRef]
- Kuruvilla, S.; Adenaw, N.; Katwal, A.B.; Lipinski, M.J.; Kramer, C.M.; Salerno, M. Late gadolinium enhancement on cardiac magnetic resonance predicts adverse cardiovascular outcomes in nonischemic cardiomyopathy: A systematic review and meta-analysis. Circ. Cardiovasc. Imaging 2014, 7, 250–257. [Google Scholar] [CrossRef]
- Grün, S.; Schumm, J.; Greulich, S.; Wagner, A.; Schneider, S.; Bruder, O.; Kispert, E.M.; Hill, S.; Ong, P.; Klingel, K.; et al. Long-term follow-up of biopsy-proven viral myocarditis: Predictors of mortality and incomplete recovery. J. Am. Coll. Cardiol. 2012, 59, 1604–1615. [Google Scholar] [CrossRef]
- Aquaro, G.D.; Perfetti, M.; Camastra, G.; Monti, L.; Dellegrottaglie, S.; Moro, C.; Pepe, A.; Todiere, G.; Lanzillo, C.; Scatteia, A.; et al. Cardiac MR With Late Gadolinium Enhancement in Acute Myocarditis with Preserved Systolic Function: ITAMY Study. J. Am. Coll. Cardiol. 2017, 70, 1977–1987. [Google Scholar] [CrossRef]
- Arzanauskaite, M.; Newsome, S.; Vassiliou, V.; Alpendurada, F.; Pennell, D.; Guha, K.; Cowie, M.; Gregson, J.; Lota, A.; Vazir, A.; et al. Association between midwall late gadolinium enhancement and sudden cardiac death in patients with dilated cardiomyopathy and mild and moderate left ventricular systolic dysfunction. Circulation 2017, 135, 2106–2115. [Google Scholar] [CrossRef]
- Eichhorn, C.; Greulich, S.; Bucciarelli-Ducci, C.; Sznitman, R.; Kwong, R.Y.; Gräni, C. Multiparametric Cardiovascular Magnetic Resonance Approach in Diagnosing, Monitoring, and Prognostication of Myocarditis. JACC Cardiovasc. Imaging 2022, 15, 1325–1338. [Google Scholar] [CrossRef]
- Holtackers, R.J.; Emrich, T.; Botnar, R.M.; Kooi, M.E.; Wildberger, J.E.; Kreitner, K.F. Late Gadolinium Enhancement Cardiac Magnetic Resonance Imaging: From Basic Concepts to Emerging Methods. RoFo Fortschr. Auf Dem Geb. Der Rontgenstrahlen Und Der Bildgeb. Verfahr. 2022, 194, 491–504. [Google Scholar] [CrossRef]
- Jenista, E.R.; Wendell, D.C.; Azevedo, C.F.; Klem, I.; Judd, R.M.; Kim, R.J.; Kim, H.W. Revisiting how we perform late gadolinium enhancement CMR: Insights gleaned over 25 years of clinical practice. J. Cardiovasc. Magn. Reson. 2023, 25, 18. [Google Scholar] [CrossRef] [PubMed]
- Holtackers, R.J.; Gommers, S.; Van De Heyning, C.M.; Mihl, C.; Smink, J.; Higgins, D.M.; Wildberger, J.E.; ter Bekke, R.M.A. Steadily Increasing Inversion Time Improves Blood Suppression for Free-Breathing 3D Late Gadolinium Enhancement MRI with Optimized Dark-Blood Contrast. Invest. Radiol. 2021, 56, 335–340. [Google Scholar] [CrossRef]
- Krumm, P.; Greulich, S.; Nikolaou, K. Editorial for “Histopathological Validation of Dark-Blood Late Gadolinium Enhancement Cardiovascular Magnetic Resonance Without Additional Magnetization Preparation. ” J. Magn. Reson. Imaging 2022, 55, 198–199. [Google Scholar] [CrossRef] [PubMed]
- Krumm, P.; Zitzelsberger, T.; Weinmann, M.; Mangold, S.; Rath, D.; Nikolaou, K.; Gawaz, M.; Kramer, U.; Klumpp, B.D. Cardiac MRI left ventricular global function index and quantitative late gadolinium enhancement in unrecognized myocardial infarction. Eur. J. Radiol. 2017, 92, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Krumm, P.; Mueller, K.A.L.; Klingel, K.; Kramer, U.; Horger, M.S.; Zitzelsberger, T.; Kandolf, R.; Gawaz, M.; Nikolaou, K.; Klumpp, B.D.; et al. Cardiovascular magnetic resonance patterns of biopsy proven cardiac involvement in systemic sclerosis. J. Cardiovasc. Magn. Reson. 2016, 18, 70. [Google Scholar] [CrossRef]
- Shanbhag, S.M.; Greve, A.M.; Aspelund, T.; Schelbert, E.B.; Cao, J.J.; Danielsen, R.; Porgeirsson, G.; Sigurðsson, S.; Eiríksdóttir, G.; Harris, T.B.; et al. Prevalence and prognosis of ischaemic and non-ischaemic myocardial fibrosis in older adults. Eur. Heart J. 2019, 40, 529–538. [Google Scholar] [CrossRef] [PubMed]
- Nies, H.M.J.M.; Gommers, S.; Bijvoet, G.P.; Heckman, L.I.B.; Prinzen, F.W.; Vogel, G.; Van De Heyning, C.M.; Chiribiri, A.; Wildberger, J.E.; Mihl, C.; et al. Histopathological validation of semi-automated myocardial scar quantification techniques for dark-blood late gadolinium enhancement magnetic resonance imaging. Eur. Hear. J. Cardiovasc. Imaging 2022, 31, 1–9. [Google Scholar] [CrossRef]
- van der Velde, N.; Hassing, H.C.; Bakker, B.J.; Wielopolski, P.A.; Lebel, R.M.; Janich, M.A.; Kardys, I.; Budde, R.P.J.; Hirsch, A. Improvement of late gadolinium enhancement image quality using a deep learning–based reconstruction algorithm and its influence on myocardial scar quantification. Eur. Radiol. 2021, 31, 3846–3855. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Study Population |
|---|---|
| Age (years) | 44 ± 17 |
| Age total range (years) | 18–82 |
| Female | 124/343 (36%) |
| Male | 219/343 (64%) |
| Final diagnosis by cardiac MRI | |
| Myocarditis | 125/343 (36%) |
| Non-ischemic cardiomyopathy | 109/343 (32%) |
| Normal | 109/343 (32%) |
| Bright-Blood LGE | ||||
|---|---|---|---|---|
| Positive | Negative | ∑ | ||
| Dark-blood LGE | Positive | 361 | 5 | 366 |
| Negative | 2 | 661 | 663 | |
| ∑ | 363 | 666 | 1029 | |
| Sensitivity | Specificity | Positive Likelihood Ratio | Negative Likelihood Ratio | Positive Predictive Value | Negative Predictive Value | Accuracy | |
|---|---|---|---|---|---|---|---|
| Dark-blood LGE | 99 % | 99 % | 132 | 0.01 | 99 % | 100 % | 99 % |
| (CI 98–100) | (CI 98–100) | (CI 55–317) | (CI 0.00–0.02) | (CI 97–99) | (CI 99–100) | (CI 99–100) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brendel, J.M.; Holtackers, R.J.; Geisel, J.N.; Kübler, J.; Hagen, F.; Gawaz, M.; Nikolaou, K.; Greulich, S.; Krumm, P. Dark-Blood Late Gadolinium Enhancement MRI Is Noninferior to Bright-Blood LGE in Non-Ischemic Cardiomyopathies. Diagnostics 2023, 13, 1634. https://doi.org/10.3390/diagnostics13091634
Brendel JM, Holtackers RJ, Geisel JN, Kübler J, Hagen F, Gawaz M, Nikolaou K, Greulich S, Krumm P. Dark-Blood Late Gadolinium Enhancement MRI Is Noninferior to Bright-Blood LGE in Non-Ischemic Cardiomyopathies. Diagnostics. 2023; 13(9):1634. https://doi.org/10.3390/diagnostics13091634
Chicago/Turabian StyleBrendel, Jan M., Robert J. Holtackers, Jan N. Geisel, Jens Kübler, Florian Hagen, Meinrad Gawaz, Konstantin Nikolaou, Simon Greulich, and Patrick Krumm. 2023. "Dark-Blood Late Gadolinium Enhancement MRI Is Noninferior to Bright-Blood LGE in Non-Ischemic Cardiomyopathies" Diagnostics 13, no. 9: 1634. https://doi.org/10.3390/diagnostics13091634