
The Influence of Different SARS-CoV-2 Strains on Changes in Maximal Oxygen Consumption, Ventilatory Efficiency and Oxygen Pulse of Elite Athletes
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Participants and Study Design
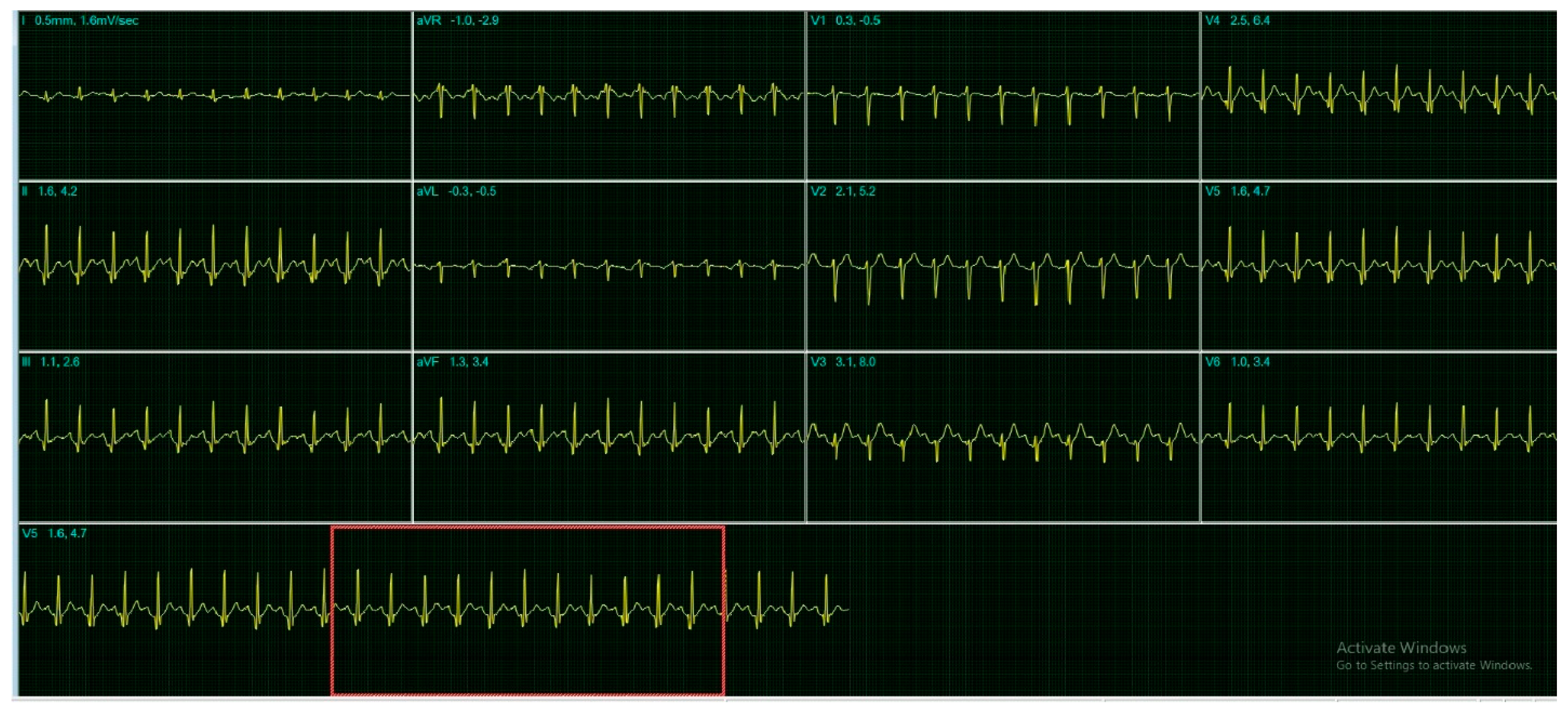
2.2. Electrocardiographic Monitoring and Respiratory Function
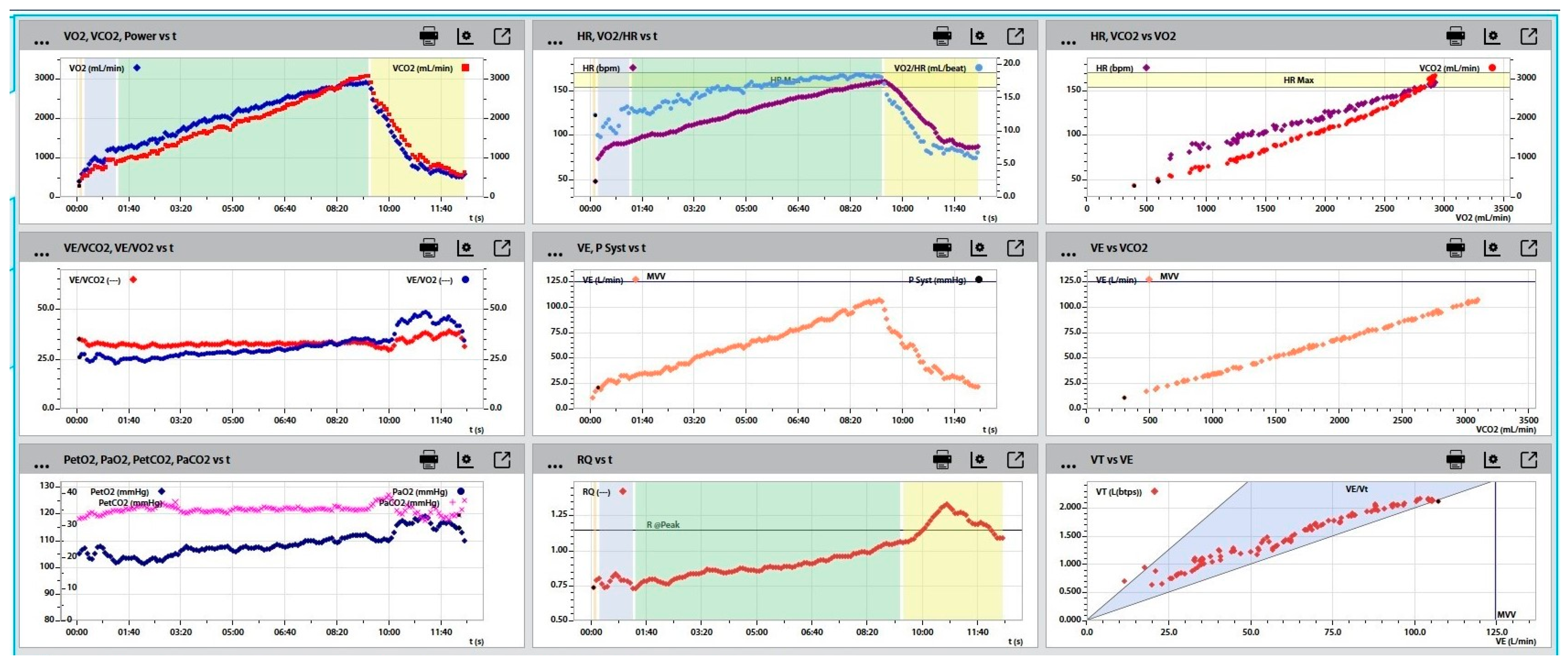
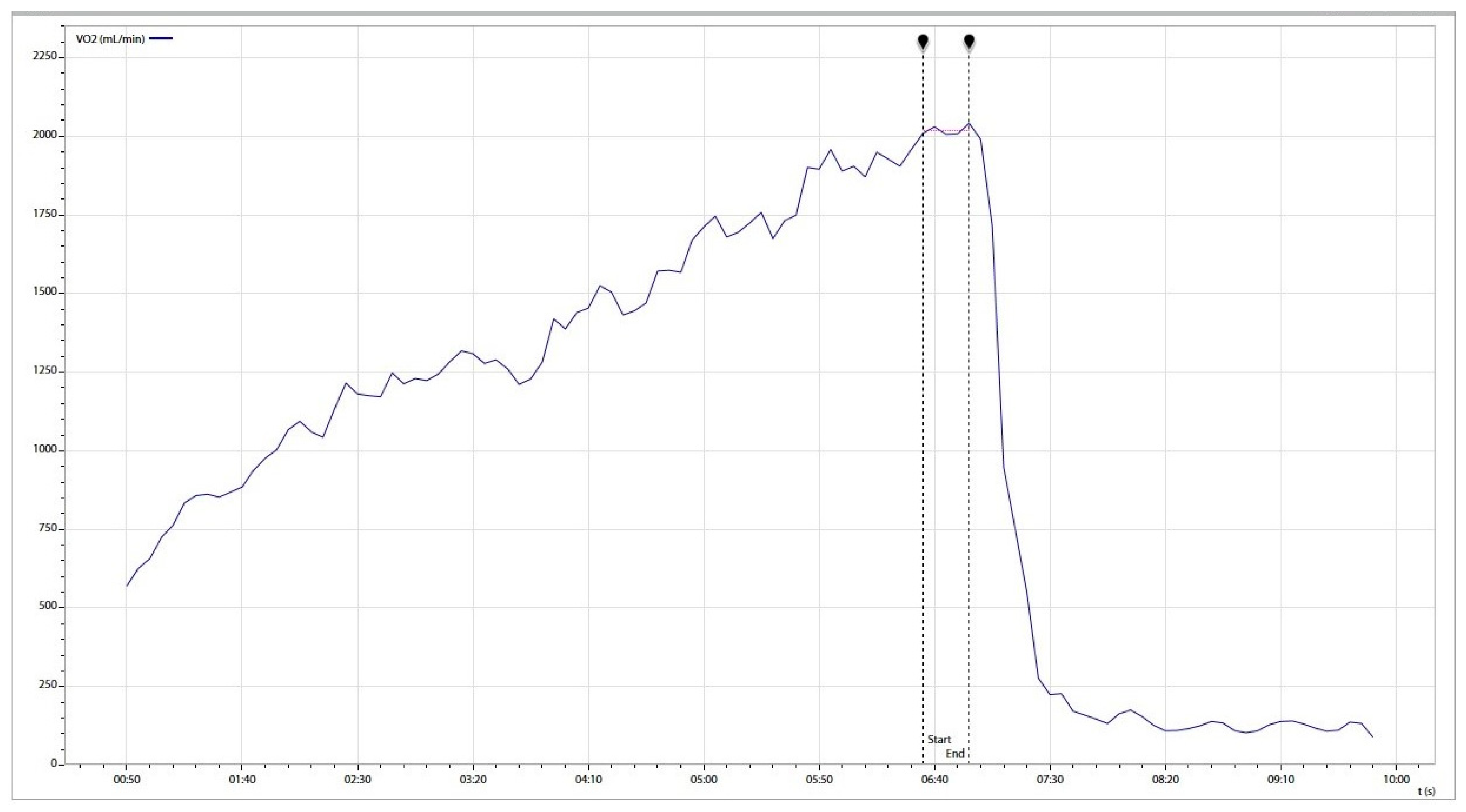
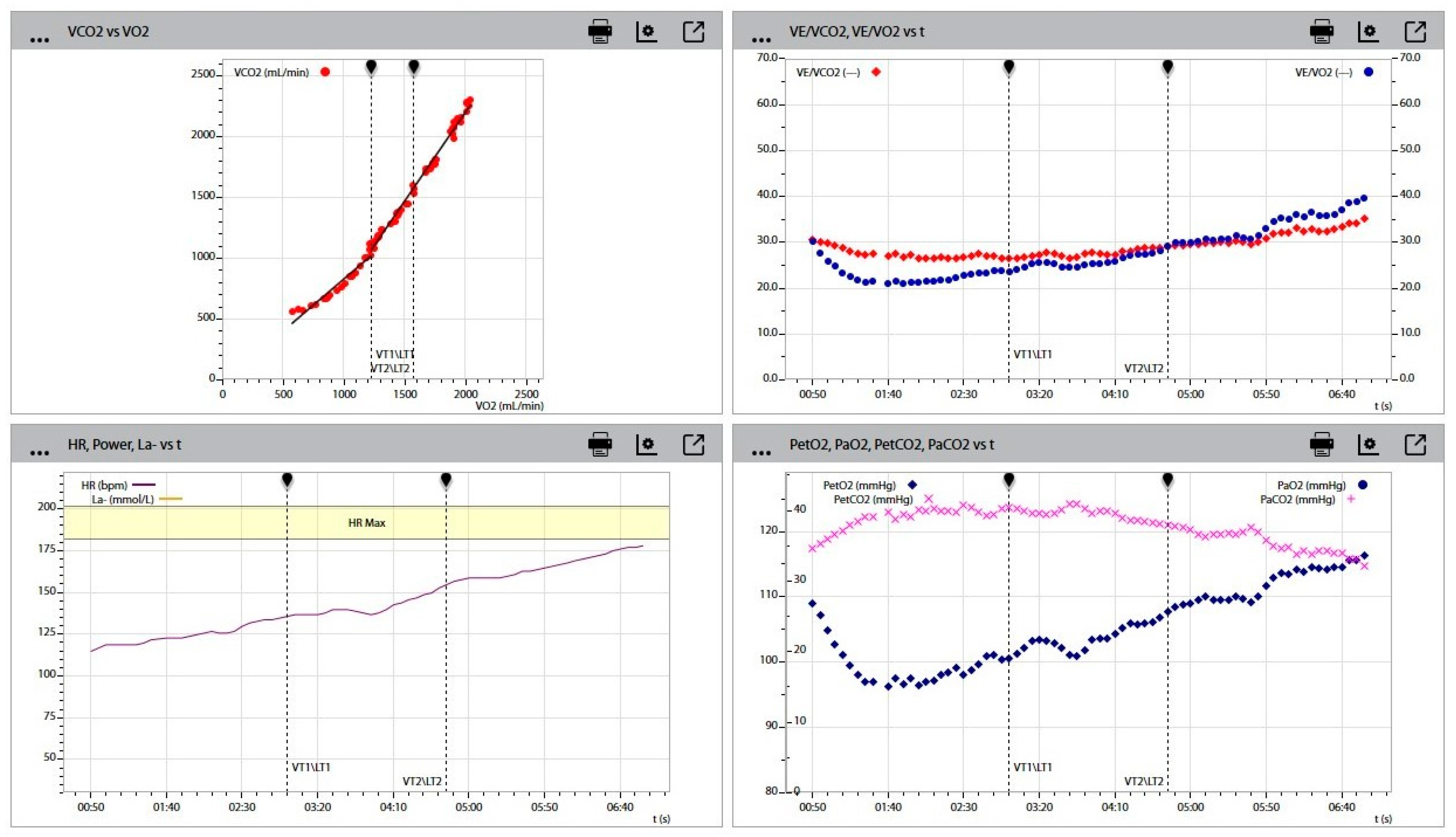
2.3. Aerobic Capacity and Metabolic Response to Effort
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 17 May 2020).
- Mohamadian, M.; Chiti, H.; Shoghli, A.; Biglari, S.; Parsamanesh, N.; Esmaeilzadeh, A. COVID-19: Virology, biology and novel laboratory diagnosis. J. Gene Med. 2021, 23, e3303. [Google Scholar] [CrossRef]
- Elrobaa, I.H.; New, K.J. COVID-19: Pulmonary and Extra Pulmonary Manifestations. Front. Public Health 2021, 9, 711616. [Google Scholar] [CrossRef] [PubMed]
- Grix, J.; Brannagan, P.M.; Grimes, H.; Neville, R. Impact of COVID-19 on sport. Int. J. Sport Policy 2020, 13, 1–2. [Google Scholar] [CrossRef]
- Grazioli, R.; Loturco, I.; Baroni, B.M.; Oliveira, G.S.; Saciura, V.; Vanoni, E.; Dias, R.; Veeck, F.; Pinto, R.S.; Cadore, E.L. Coronavirus Disease-19 Quarantine Is More Detrimental Than Traditional Off-Season on Physical Conditioning of Professional Soccer Players. J. Strength Cond. Res. 2020, 34, 3316–3320. [Google Scholar] [CrossRef] [PubMed]
- Pelliccia, A.; Sharma, S.; Gati, S.; Bäck, M.; Börjesson, M.; Caselli, S.; Collet, J.P.; Corrado, D.; Drezner, J.A.; Halle, M.; et al. 2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease. Eur. Heart J. 2021, 42, 17–96, Erratum in Eur. Heart J. 2021, 42, 548–549. [Google Scholar] [CrossRef] [PubMed]
- Wilson, M.G.; Hull, J.H.; Rogers, J.; Pollock, N.; Dodd, M.; Haines, J.; Harris, S.; Loosemore, M.; Malhotra, A.; Pieles, G.; et al. Cardiorespiratory considerations for return-to-play in elite athletes after COVID-19 infection: A practical guide for sport and exercise medicine physicians. Br. J. Sports Med. 2020, 54, 1157–1161. [Google Scholar] [CrossRef] [PubMed]
- Yeo, T.J. Sport and exercise during and beyond the COVID-19 pandemic. Eur. J. Prev. Cardiol. 2020, 27, 1239–1241. [Google Scholar] [CrossRef]
- Nedeljkovic, I.P.; Giga, V.; Ostojic, M.; Djordjevic-Dikic, A.; Stojmenovic, T.; Nikolic, I.; Dikic, N.; Nedeljkovic-Arsenovic, O.; Maksimovic, R.; Dobric, M.; et al. Focal Myocarditis after Mild COVID-19 Infection in Athletes. Diagnostics 2021, 11, 1519. [Google Scholar] [CrossRef] [PubMed]
- Mitrani, R.D.; Alfadhli, J.; Lowery, M.H.; Best, T.M.; Hare, J.M.; Fishman, J.; Dong, C.; Siegel, Y.; Scavo, V.; Basham, G.J.; et al. Utility of exercise testing to assess athletes for post COVID-19 myocarditis. Am. Heart J. Plus 2022, 14, 100125. [Google Scholar] [CrossRef]
- Chevalier, L.; Cochet, H.; Mahida, S.; Blanchard, S.; Benard, A.; Cariou, T.; Sridi-Cheniti, S.; Benhenda, S.; Doutreleau, S.; Cade, S.; et al. Resuming Training in High-Level Athletes After Mild COVID-19 Infection: A Multicenter Prospective Study (ASCCOVID-19). Sports Med. Open 2022, 8, 83. [Google Scholar] [CrossRef]
- Food and Drug Administration (.gov). Available online: https://www.fda.gov/medical-devices/coronavirus-covid-19-and-medical-devices/sars-cov-2-viral-mutations-impact-covid-19-tests (accessed on 16 March 2022).
- Institute for Public Health of Serbia BATUT. Available online: https://www.batut.org.rs/index.php?content=2523 (accessed on 11 October 2022).
- Papanikolaou, V.; Chrysovergis, A.; Ragos, V.; Tsiambas, E.; Katsinis, S.; Manoli, A.; Papouliakos, S.; Roukas, D.; Mastronikolis, S.; Peschos, D.; et al. From delta to Omicron: S1-RBD/S2 mutation/deletion equilibrium in SARS-CoV-2 defined variants. Gene 2022, 814, 146134. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Wu, J.; Nie, J.; Zhang, L.; Hao, H.; Liu, S.; Zhao, C.; Zhang, Q.; Liu, H.; Nie, L.; et al. The Impact of Mutations in SARS-CoV-2 Spike on Viral Infectivity and Antigenicity. Cell 2020, 182, 1284–1294.e9. [Google Scholar] [CrossRef]
- El-Shabasy, R.M.; Nayel, M.A.; Taher, M.M.; Abdelmonem, R.; Shoueir, K.R.; Kenawy, E.R. Three waves changes, new variant strains, and vaccination effect against COVID-19 pandemic. Int. J. Biol. Macromol. 2022, 204, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Sun, C.; Xie, C.; Bu, G.L.; Zhong, L.Y.; Zeng, M.S. Molecular characteristics, immune evasion, and impact of SARS-CoV-2 variants. Signal Transduct. Target. Ther. 2022, 7, 202. [Google Scholar] [PubMed]
- Milovancev, A.; Avakumovic, J.; Lakicevic, N.; Stajer, V.; Korovljev, D.; Todorovic, N.; Bianco, A.; Maksimovic, N.; Ostojic, S.; Drid, P. Cardiorespiratory Fitness in Volleyball Athletes Following a COVID-19 Infection: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 4059. [Google Scholar] [CrossRef] [PubMed]
- Babity, M.; Zamodics, M.; Konig, A.; Kiss, A.R.; Horvath, M.; Gregor, Z.; Rakoczi, R.; Kovacs, E.; Fabian, A.; Tokodi, M.; et al. Cardiopulmonary examinations of athletes returning to high-intensity sport activity following SARS-CoV-2 infection. Sci. Rep. 2022, 12, 21686. [Google Scholar] [CrossRef]
- Stavrou, T.V.; Kyriaki, A.; Vavougios, D.G.; Fatouros, G.I.; Metsios, S.G.; Kalabakas, K.; Karagiannis, D.; Daniil, Z.; Gourgoulianis, I.K.; Βasdekis, G. Athletes with mild post-COVID-19 symptoms experience increased respiratory and metabolic demands: A cross-sectional study. Sports Med. Health Sci. 2022; 1–6, In press. [Google Scholar] [CrossRef]
- Martinez, M.W.; Tucker, A.M.; Bloom, O.J.; Green, G.; DiFiori, J.P.; Solomon, G.; Phelan, D.; Kim, J.H.; Meeuwisse, W.; Sills, A.K.; et al. Prevalence of Inflammatory Heart Disease Among Professional Athletes with Prior COVID-19 Infection Who Received Systematic Return-to-Play Cardiac Screening. JAMA Cardiol. 2021, 6, 745–752. [Google Scholar] [CrossRef]
- Komici, K.; Bianco, A.; Perrotta, F.; Iacono, A.D.; Bencivenga, L.; D’Agnano, V.; Rocca, A.; Bianco, A.; Rengo, G.; Guerra, G. Clinical Characteristics, Exercise Capacity and Pulmonary Function in Post-COVID-19 Competitive Athletes. J. Clin. Med. 2021, 10, 3053. [Google Scholar] [CrossRef]
- Parpa, K.; Michaelides, M. Aerobic capacity of professional soccer players before and after COVID-19 infection. Sci. Rep. 2022, 12, 11850. [Google Scholar] [CrossRef]
- Gadzic, A.; Zivkovic, A.; Stojmenovic, T. Influence of Covid 19 on morphological and cardiovascular status of professional handball players. SportLogia 2021, 17, 83–92. [Google Scholar] [CrossRef]
- Reilly, T.; Bangsbo, J.; Franks, A. Anthropometric and physiological predispositions for elite soccer. J. Sports Sci. 2000, 18, 669–683. [Google Scholar] [CrossRef] [PubMed]
- Stojmenovic, D.; Trunic, N.; Stojmenovic, T. A comparative study of aerobic capacity among elite basketball players according to five different positions in the team. J. Phys. Educ. Sport 2022, 22, 2522–2529. [Google Scholar] [CrossRef]
- Phillips, D.B.; Collins, S.É.; Stickland, M.K. Measurement and Interpretation of Exercise Ventilatory Efficiency. Front. Physiol. 2020, 11, 659. [Google Scholar] [CrossRef] [PubMed]
- Mazaheri, R.; Schmied, C.; Niederseer, D.; Guazzi, M. Cardiopulmonary Exercise Test Parameters in Athletic Population: A Review. J. Clin. Med. 2021, 10, 5073. [Google Scholar] [CrossRef] [PubMed]
- Donina, Z.A. Causes of Hypoxemia in COVID-19. J. Evol. Biochem. Physiol. 2022, 58, 73–80. [Google Scholar] [CrossRef]
- Guarnieri, J.W.; Dybas, J.M.; Fazelinia, H.; Kim, M.S.; Frere, J.; Zhang, Y.; Albrecht, Y.S.; Murdock, D.G.; Angelin, A.; Singh, L.N.; et al. Targeted Down Regulation of Core Mitochondrial Genes During SARS-CoV-2 Infection. bioRxiv 2022. [Google Scholar] [CrossRef]
- Alfarouk, K.O.; Alhoufie, S.T.S.; Hifny, A.; Schwartz, L.; Alqahtani, A.S.; Ahmed, S.B.M.; Alqahtani, A.M.; Alqahtani, S.S.; Muddathir, A.K.; Ali, H.; et al. Of mitochondrion and COVID-19. J. Enzym. Inhib. Med. Chem. 2021, 36, 1258–1267. [Google Scholar] [CrossRef] [PubMed]
- Saito, S.; Shahbaz, S.; Sligl, W.; Osman, M.; Tyrrell, D.L.; Elahi, S. Differential Impact of SARS-CoV-2 Isolates, Namely, the Wuhan Strain, Delta, and Omicron Variants on Erythropoiesis. Microbiol. Spectr. 2022, 10, e0173022. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SARS-CoV-2 Strain | Wuhan | Delta | Omicron |
|---|---|---|---|
| Period of infection | September 2020–July 2021 | August 2021–January 2022 | February 2022–September 2022 |
| N° of participants | 88 | 66 | 66 |
| Wuhan | Delta | Omicron | |
|---|---|---|---|
| HR (bpm) | 59.4 ± 11.60 | 57.72 ± 10.68 | 55.82 ± 10.65 |
| SBP (mmHg) | 117.8 ± 7.80 | 119.4 ± 8.26 | 116.5 ± 7.60 |
| DBP (mmHg) | 73.5 ± 8.10 | 74.4 ± 7.43 | 73.8 ± 7.68 |
| RVd (mm) | 24.1 ± 3.58 | 23.8 ± 3.81 | 24.3 ± 3.60 |
| IVSd (mm) | 10.1 ± 2.0 | 9.6 ± 1.89 | 10.4 ± 1.79 |
| LVDd (mm) | 51.4 ± 5.78 | 51.7 ± 5.81 | 52.1 ± 5.16 |
| LVPWd (mm) | 9.7 ± 1.50 | 9.8 ± 1.46 | 10.0 ± 1.56 |
| LVSD (mm) | 34.8 ± 4.72 | 35.1 ± 4.23 | 35.8 ± 4.18 |
| EF (%) | 60.7 ± 7.51 | 60.2 ± 6.65 | 61.8 ± 6.46 |
| Wuhan | Delta | Omicron | Normal Range | |
|---|---|---|---|---|
| CRP (mg/L) | 2.68 ± 1.20 | 2.72 ± 0.63 | 3.08 ± 1.05 | 0.00–10.0 |
| D-Dimer (mg/L FEU) | 0.17 ± 0.80 | 0.22 ± 0.86 | 0.23 ± 0.60 | <0.50 |
| nt-pro BNP (pg/mL) | 16.54 ± 5.71 | 18.40 ± 4.43 | 17.21 ± 5.68 | 0–125 |
| hs-cTnT (µg/L) | 4.30 ± 3.01 | 4.59 ± 1.89 | 4.42 ± 1.40 | <10 |
| Variable | Wuhan Strain ( ± SD) | Delta Strain ( ± SD) | Omicron Strain ( ± SD) | p Value |
|---|---|---|---|---|
| N (number) | 88 | 66 | 66 | |
| Age | 23.52 ± 4.53 | 22.26 ± 4.67 | 23.21 ± 4.75 | |
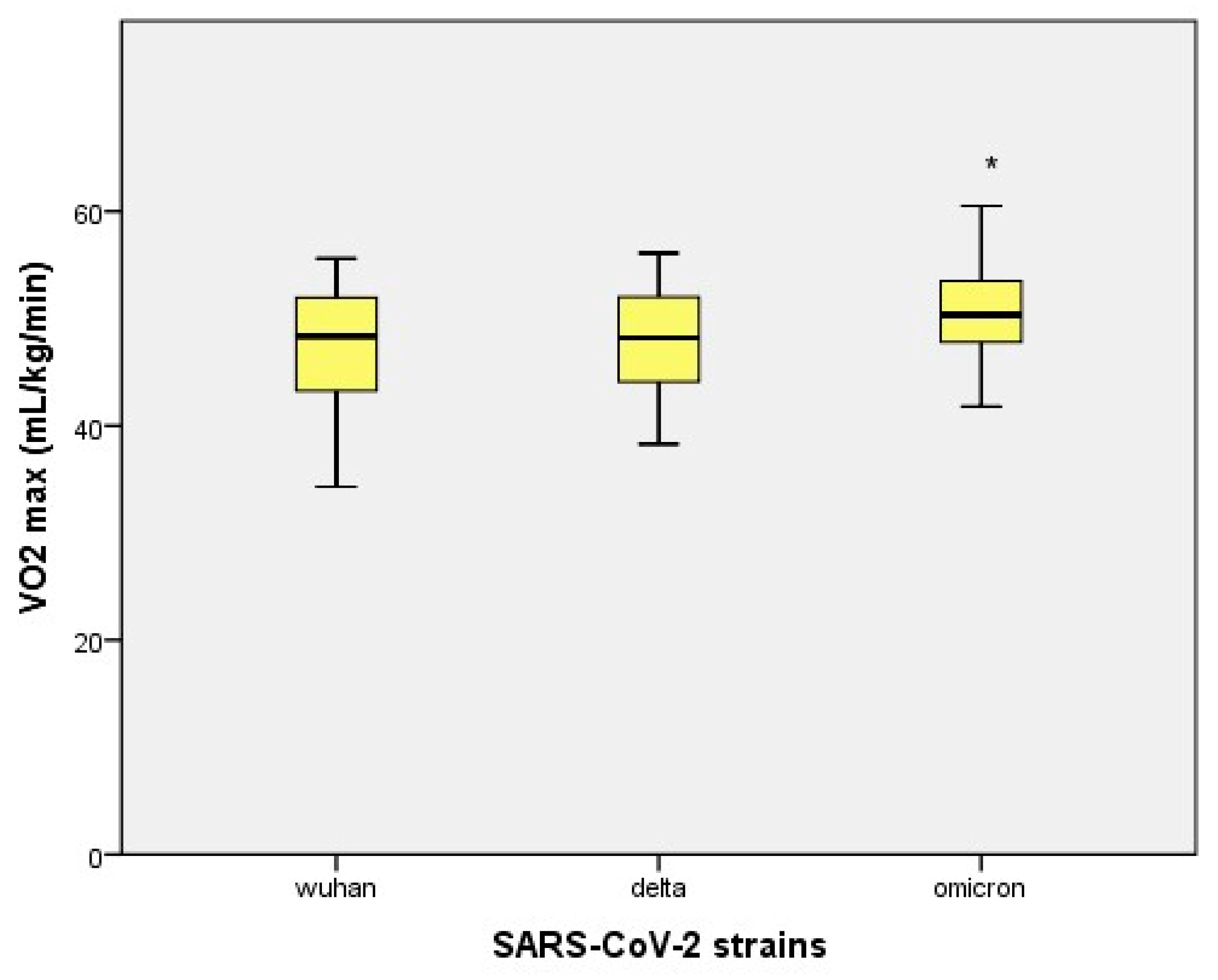
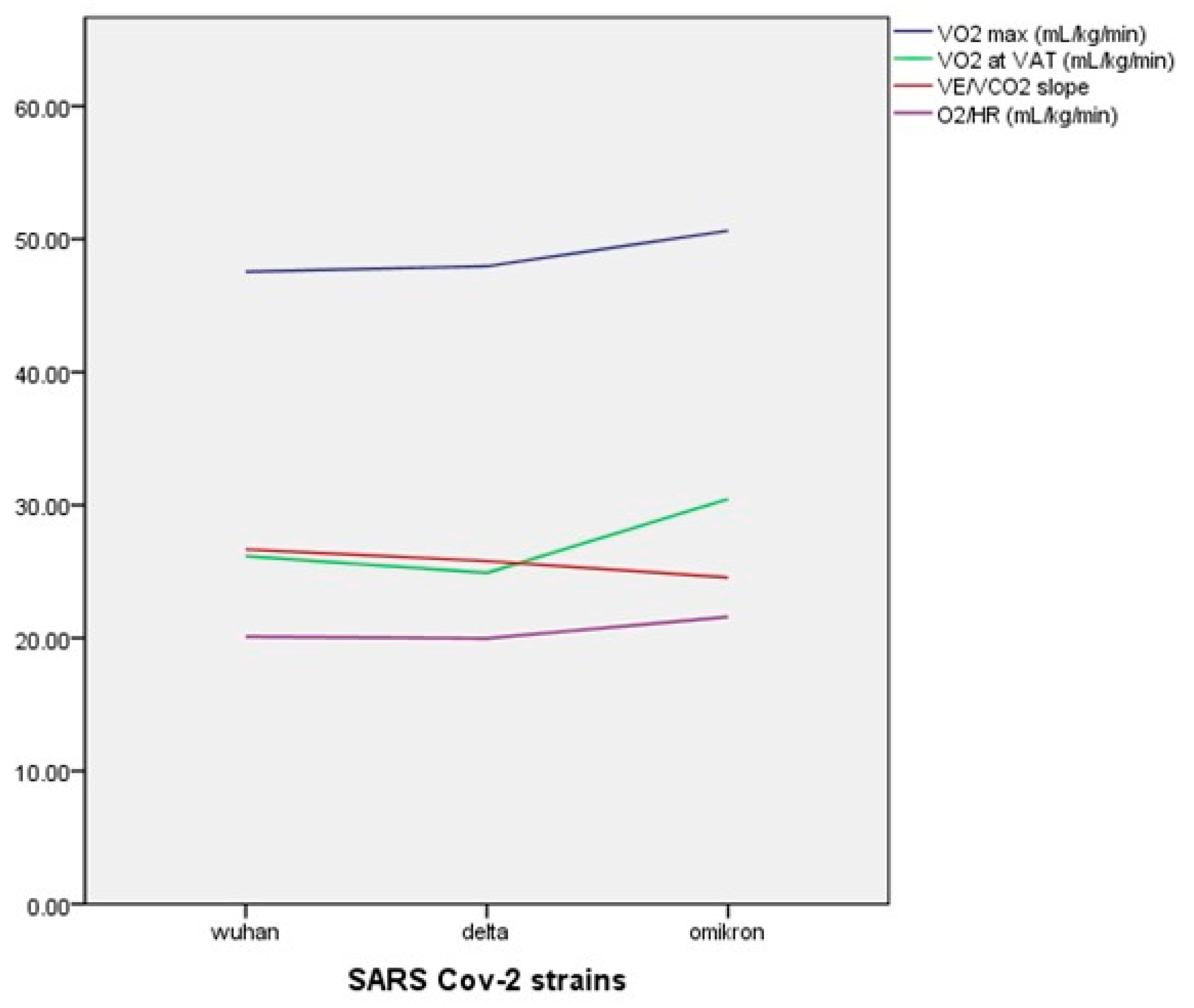
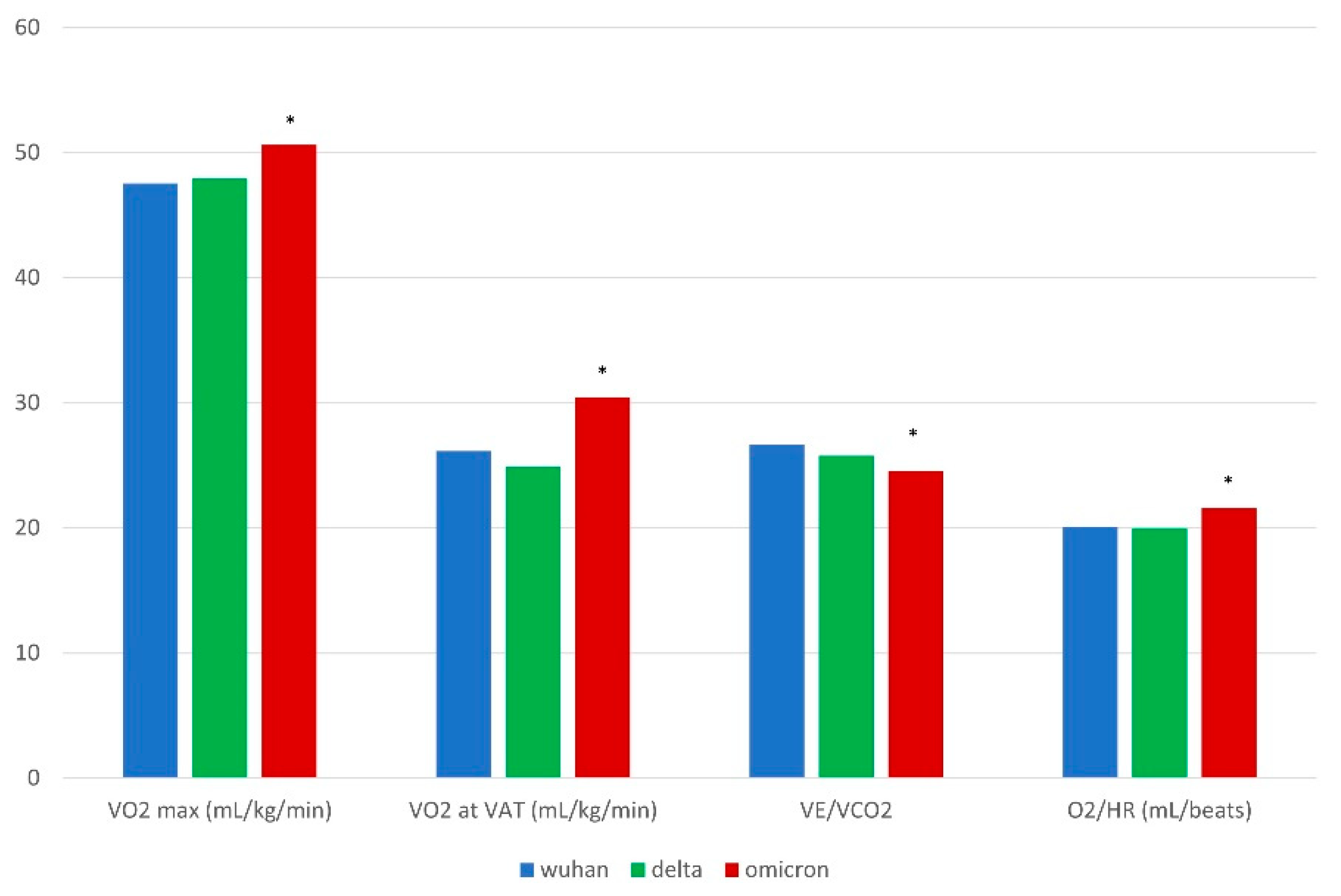
| VO2 max (mL/kg/min) | 47.55 ± 5.09 | 47.95 ± 4.64 | 50.63 ± 4.08 * | p < 0.001 |
| VO2 at VAT (ml/kg/min) | 26.15 ± 4.70 | 24.90 ± 3.77 | 30.45 ± 4.41 * | p < 0.001 |
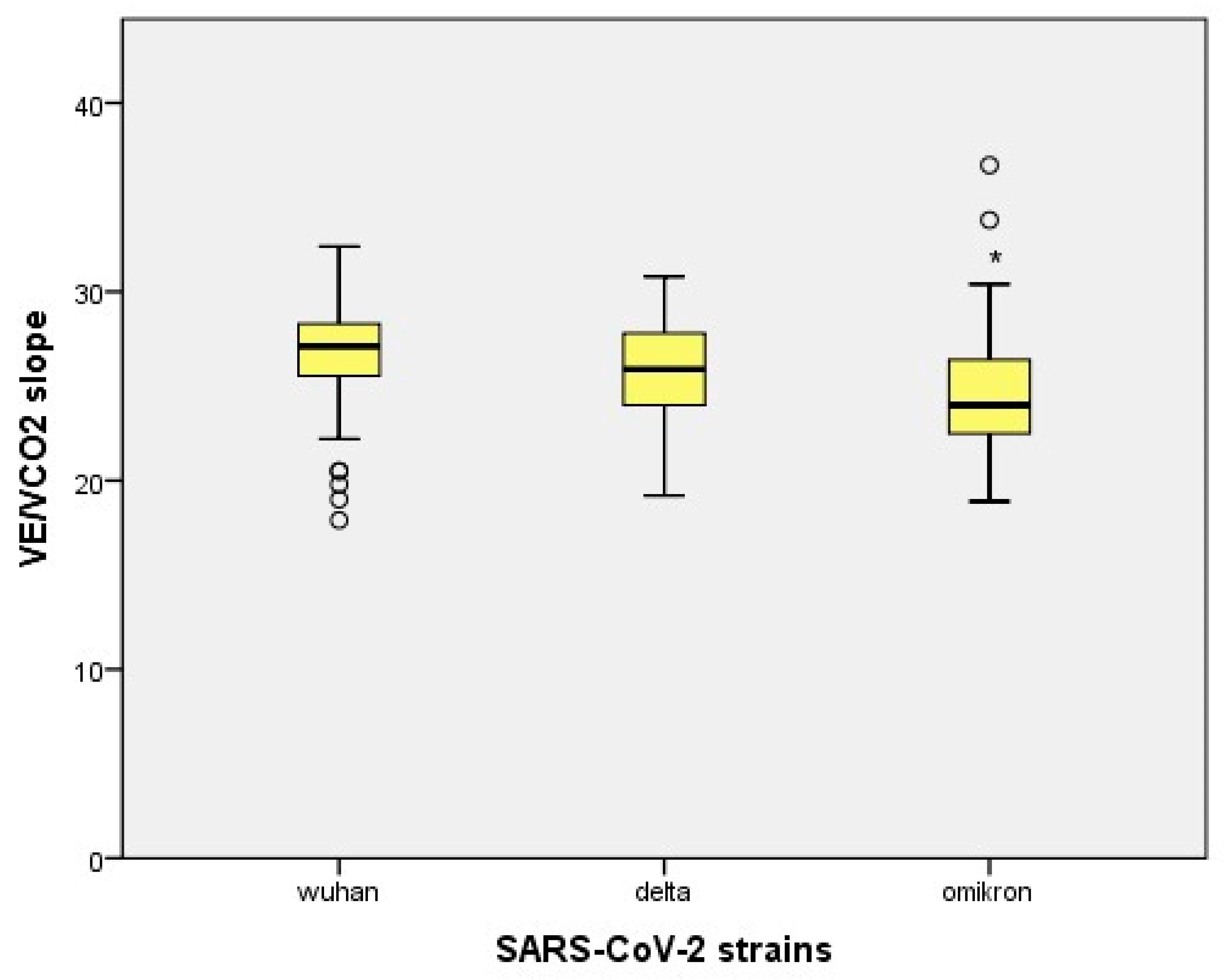
| VE/VCO2 slope | 26.66 ± 2.57 | 25.78 ± 2.69 | 24.55 ± 3.32 * | p < 0.001 |
| RER (CO2/O2) | 1.18 ± 0.065 | 1.19 ± 0.048 | 1.15 ± 0.032 * | p < 0.001 |
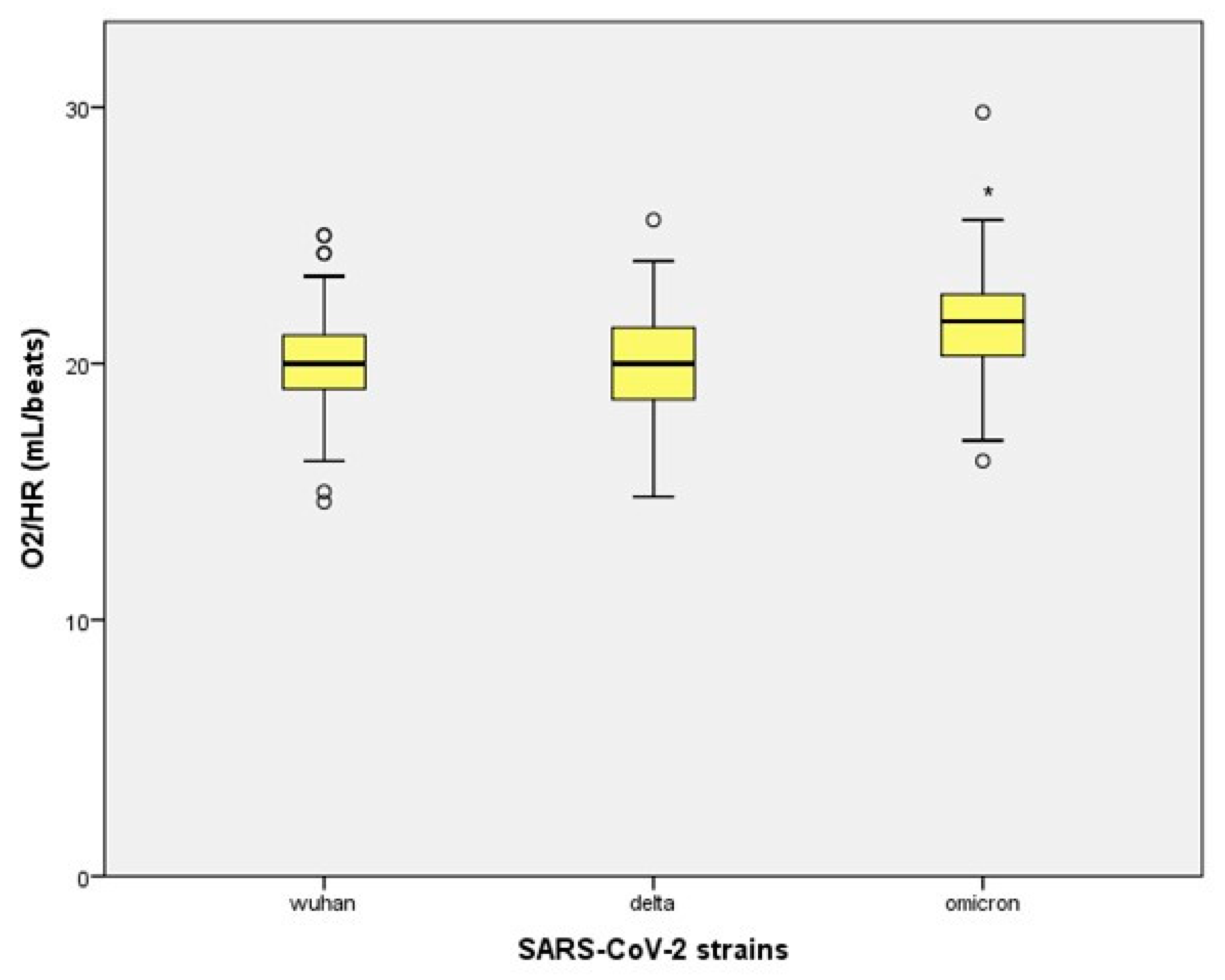
| O2/HR (mL/beat) | 20.10 ± 1.88 | 19.98 ± 2.1 | 21.59 ± 2.06 * | p < 0.001 |
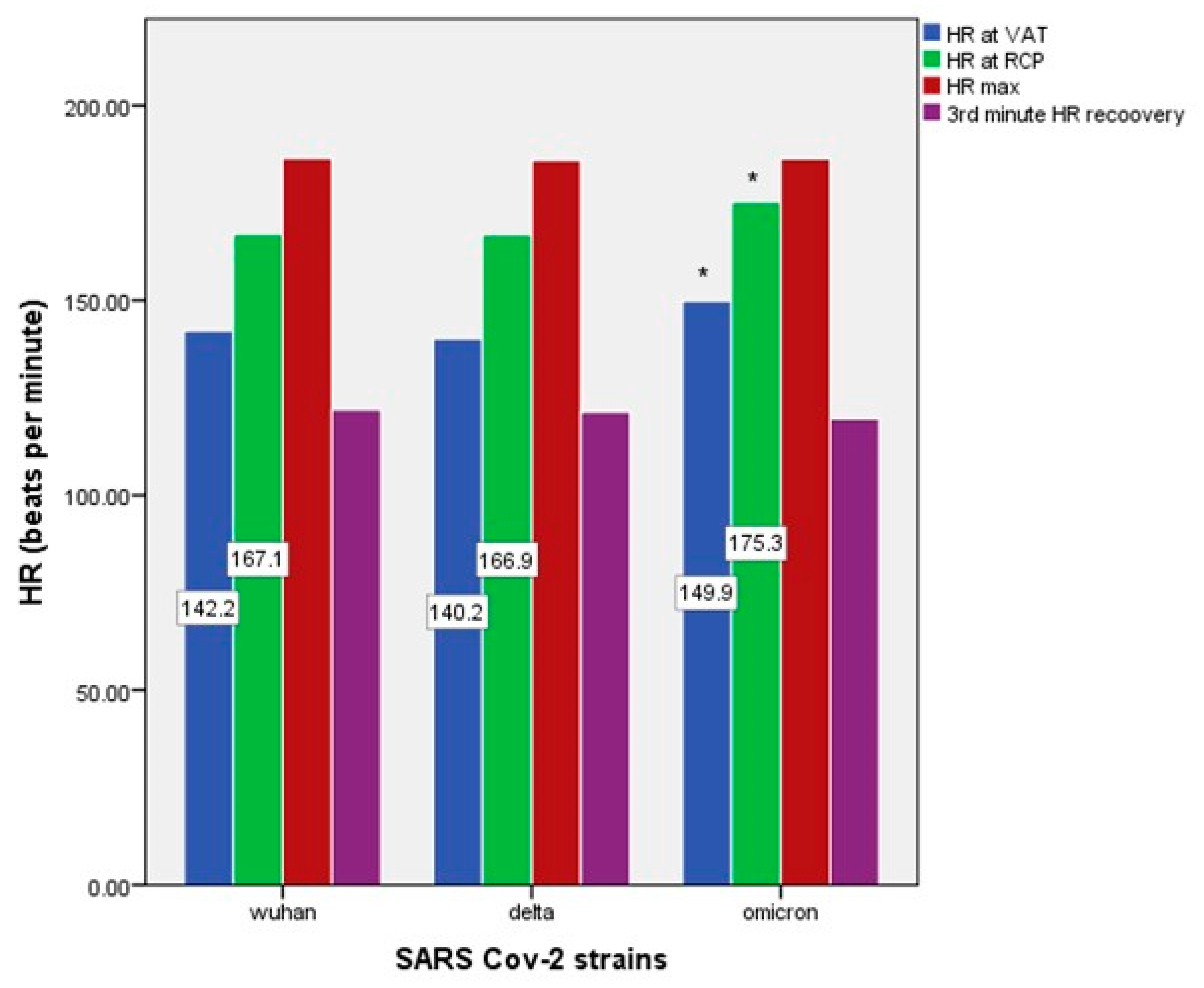
| HR at VAT (bpm) | 141.75 ± 11.42 | 140.17 ± 9.86 | 149.86 ± 8.11 * | p < 0.001 |
| HR at RCP (bpm) | 167.09 ± 10.94 | 166.92 ± 9.26 | 175.30 ± 7.95 * | p < 0.001 |
| HR max (bpm) | 186.49 ± 8.78 | 186.00 ± 8.31 | 186.39 ± 9.00 | p = 0.939 |
| HR recovery (1st minute) | 161.75 ± 11.97 | 159.27 ± 13.53 | 161.48 ± 13.25 | p = 0.738 |
| HR recovery (2nd minute) | 134.57 ± 15.39 | 131.87 ± 16.22 | 132.27 ± 15.71 | p = 0.836 |
| HR recovery (3rd minute) | 121.98 ± 14.35 | 121.37 ± 14.75 | 119.63 ± 14.77 | p = 0.603 |
| Wuhan | Delta | Omicron | p Value | |
|---|---|---|---|---|
| RER (CO2/O2) | 1.18 ± 0.065 | 1.19 ± 0.048 | 1.15 ± 0.032 * | p < 0.001 |
| HR at VAT (bpm) | 141.75 ± 11.42 | 140.17 ± 9.86 | 149.86 ± 8.11 * | p < 0.001 |
| HR at RCP (bpm) | 167.09 ± 10.94 | 166.92 ± 9.26 | 175.30 ± 7.95 * | p < 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stojmenovic, D.; Stojmenovic, T.; Andjelkovic, M.; Trunic, N.; Dikic, N.; Kilibarda, N.; Nikolic, I.; Nedeljkovic, I.; Ostojic, M.; Purkovic, M.; et al. The Influence of Different SARS-CoV-2 Strains on Changes in Maximal Oxygen Consumption, Ventilatory Efficiency and Oxygen Pulse of Elite Athletes. Diagnostics 2023, 13, 1574. https://doi.org/10.3390/diagnostics13091574
Stojmenovic D, Stojmenovic T, Andjelkovic M, Trunic N, Dikic N, Kilibarda N, Nikolic I, Nedeljkovic I, Ostojic M, Purkovic M, et al. The Influence of Different SARS-CoV-2 Strains on Changes in Maximal Oxygen Consumption, Ventilatory Efficiency and Oxygen Pulse of Elite Athletes. Diagnostics. 2023; 13(9):1574. https://doi.org/10.3390/diagnostics13091574
Chicago/Turabian StyleStojmenovic, Dragutin, Tamara Stojmenovic, Marija Andjelkovic, Nenad Trunic, Nenad Dikic, Natasa Kilibarda, Ivan Nikolic, Ivana Nedeljkovic, Marina Ostojic, Milos Purkovic, and et al. 2023. "The Influence of Different SARS-CoV-2 Strains on Changes in Maximal Oxygen Consumption, Ventilatory Efficiency and Oxygen Pulse of Elite Athletes" Diagnostics 13, no. 9: 1574. https://doi.org/10.3390/diagnostics13091574