
Technical Acoustic Measurements Combined with Clinical Parameters for the Differential Diagnosis of Nonalcoholic Steatohepatitis
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. ATI, NLV and Ratio Examination
2.3. SWS and SWD Examination
2.4. Biochemical Examination and Clinical Data Collection
2.5. Histopathological Examination
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Correlation between Pathological Parameters versus Technical Acoustic Measurements and Clinical Parameters
3.3. Influencing Factors of AC, NLV, NLV-SD, Ratio, SWE and SWS
3.4. The Diagnostic Performance of SWS, AC and NLV Values in Differentiating NASH from Non-NASH
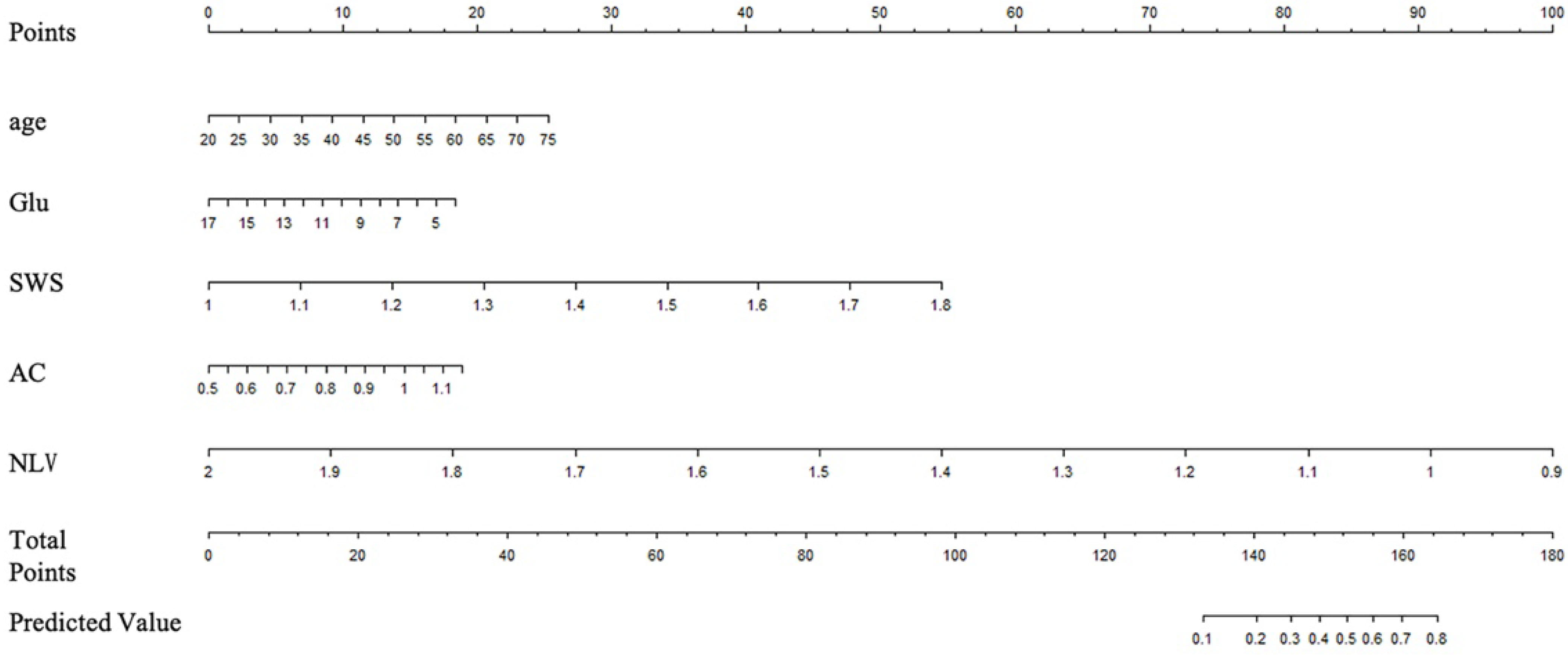
3.5. Establishment of a Nomogram Prediction Model Combining Technical Acoustic Measurements and Clinical Parameters for the Combined Diagnosis of NASH
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cotter, T.G.; Rinella, M. Nonalcoholic Fatty Liver Disease 2020: The State of the Disease. Gastroenterology 2020, 158, 1851–1864. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.; Tacke, F.; Arrese, M.; Sharma, B.C.; Mostafa, I.; Bugianesi, E.; Wong, V.W.-S.; Yilmaz, Y.; George, J.; Fan, J.; et al. Global Perspectives on Nonalcoholic Fatty Liver Disease and Nonalcoholic Steatohepatitis. Hepatology 2019, 69, 2672–2682. [Google Scholar] [CrossRef] [PubMed]
- Chalasani, N.; Younossi, Z.; LaVine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef] [PubMed]
- Ong, J.P.; Pitts, A.; Younossi, Z.M. Increased overall mortality and liver-related mortality in non-alcoholic fatty liver disease. J. Hepatol. 2008, 49, 608–612. [Google Scholar] [CrossRef] [PubMed]
- EEkstedt, M.; Hagström, H.; Nasr, P.; Fredrikson, M.; Stål, P.; Kechagias, S.; Hultcrantz, R. Fibrosis stage is the strongest predictor for disease-specific mortality in NAFLD after up to 33 years of follow-up. Hepatology 2015, 61, 1547–1554. [Google Scholar] [CrossRef]
- Angulo, P.; Kleiner, D.E.; Dam-Larsen, S.; Adams, L.A.; Björnsson, E.S.; Charatcharoenwitthaya, P.; Mills, P.R.; Keach, J.C.; Lafferty, H.D.; Stahler, A.; et al. Liver Fibrosis, but No Other Histologic Features, Is Associated with Long-term Outcomes of Patients With Nonalcoholic Fatty Liver Disease. Gastroenterology 2015, 149, 389–397.e310. [Google Scholar] [CrossRef]
- Dyson, J.K.; Anstee, Q.M.; McPherson, S. Non-alcoholic fatty liver disease: A practical approach to diagnosis and staging. Frontline Gastroenterol. 2014, 5, 211–218. [Google Scholar] [CrossRef]
- Xiao, G.; Zhu, S.; Xiao, X.; Yan, L.; Yang, J.; Wu, G. Comparison of laboratory tests, ultrasound, or magnetic resonance elastography to detect fibrosis in patients with nonalcoholic fatty liver disease: A meta-analysis. Hepatology 2017, 66, 1486–1501. [Google Scholar] [CrossRef]
- Cassinotto, C.; Boursier, J.; de Lédinghen, V.; Lebigot, J.; Lapuyade, B.; Cales, P.; Hiriart, J.B.; Michalak, S.; Bail, B.L.; Cartier, V.; et al. Liver stiffness in nonalcoholic fatty liver disease: A comparison of supersonic shear imaging, FibroScan, and ARFI with liver biopsy. Hepatology 2016, 63, 1817–1827. [Google Scholar] [CrossRef]
- Lee, D.H.; Cho, E.J.; Bae, J.S.; Lee, J.Y.; Yu, S.J.; Kim, H.; Lee, K.B.; Han, J.K.; Choi, B.I. Accuracy of 2-dimensional Shear Wave Elastography and Attenuation Imaging for Evaluation of Patients with Nonalcoholic Steatohepatitis. Clin. Gastroenterol. Hepatol. 2020, 19, 797–805.e7. [Google Scholar] [CrossRef]
- Lee, D.H.; Lee, J.Y.; Bae, J.S.; Yi, N.-J.; Lee, K.-W.; Suh, K.-S.; Kim, H.; Lee, K.B.; Han, J.K. Shear-Wave Dispersion Slope from US Shear-Wave Elastography: Detection of Allograft Damage after Liver Transplantation. Radiology 2019, 293, 327–333. [Google Scholar] [CrossRef]
- Dioguardi Burgio, M.A.-O.; Ronot, M.; Reizine, E.; Rautou, P.-E.; Castera, L.; Paradis, V.; Garteiser, P.; Van Beers, B.; Vilgrain, V. Quantification of hepatic steatosis with ultrasound: Promising role of attenuation imaging coefficient in a biopsy-proven cohort. Eur. Radiol. 2020, 30, 2293–2301. [Google Scholar] [CrossRef]
- Bae, J.S.; Lee, D.H.; Lee, J.Y.; Kim, H.; Yu, S.J.; Lee, J.-H.; Cho, E.J.; Lee, Y.B.; Han, J.K.; Choi, B.I. Assessment of hepatic steatosis by using attenuation imaging: A quantitative, easy-to-perform ultrasound technique. Eur. Radiol. 2019, 29, 6499–6507. [Google Scholar] [CrossRef]
- Tada, T.; Iijima, H.; Kobayashi, N.; Yoshida, M.; Nishimura, T.; Kumada, T.; Kondo, R.; Yano, H.; Kage, M.; Nakano, C.; et al. Usefulness of Attenuation Imaging with an Ultrasound Scanner for the Evaluation of Hepatic Steatosis. Ultrasound Med. Biol. 2019, 45, 2679–2687. [Google Scholar] [CrossRef]
- Bae, J.S.; Lee, J.Y.; Lee, D.H.; Kim, H.; Lee, Y.; Han, J.K. Quantitative Evaluation of Hepatic Steatosis Using Normalized Local Variance in a Rat Model: Comparison with Histopathology as the Reference Standard. Korean J. Radiol. 2019, 20, 1399–1407. [Google Scholar] [CrossRef]
- Zhao, Y.; Zhang, C.; Xu, S.; Zhang, H.; Wei, S.; Huang, P.; Zhang, L.; Wong, Y.N.; Xu, W.; Huang, P. Quantitative evaluation of hepatic steatosis using novel ultrasound technology normalized local variance (NLV) and its standard deviation with different ROIs in patients with metabolic-associated fatty liver disease: A pilot study. Abdom. Imaging 2021, 47, 693–703. [Google Scholar] [CrossRef]
- Chauhan, A.; Sultan, L.R.; Furth, E.E.; Jones, L.P.; Khungar, V.; Sehgal, C.M. Diagnostic accuracy of hepatorenal index in the detection and grading of hepatic steatosis. J. Clin. Ultrasound 2016, 44, 580–586. [Google Scholar] [CrossRef]
- Petzold, G.; Lasser, J.; Rühl, J.; Bremer, S.C.B.; Knoop, R.F.; Ellenrieder, V.; Kunsch, S.; Neesse, A. Diagnostic accuracy of B-Mode ultrasound and Hepatorenal Index for graduation of hepatic steatosis in patients with chronic liver disease. PLoS ONE 2020, 15, e0231044. [Google Scholar] [CrossRef]
- Ferraioli, G.; Wong, V.W.-S.; Castera, L.; Berzigotti, A.; Sporea, I.; Dietrich, C.F.; Choi, B.I.; Wilson, S.R.; Kudo, M.; Barr, R.G. Liver Ultrasound Elastography: An Update to the World Federation for Ultrasound in Medicine and Biology Guidelines and Recommendations. Ultrasound Med. Biol. 2018, 44, 2419–2440. [Google Scholar] [CrossRef]
- Kleiner, D.E.; Brunt, E.M.; Van Natta, M.; Behling, C.; Contos, M.J.; Cummings, O.W.; Ferrell, L.D.; Liu, Y.-C.; Torbenson, M.S.; Unalp-Arida, A.; et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology 2005, 41, 1313–1321. [Google Scholar] [CrossRef]
- Matteoni, C.A.; Younossi, Z.M.; Gramlich, T.; Boparai, N.; Liu, Y.C.; McCullough, A.J. Nonalcoholic fatty liver disease: A spectrum of clinical and pathological severity. Gastroenterology 1999, 116, 1413–1419. [Google Scholar] [CrossRef] [PubMed]
- Brunt, E.M.; Janney, C.G.; Di Bisceglie, A.M.; Neuschwander-Tetri, B.A.; Bacon, B.R. Nonalcoholic steatohepatitis: A proposal for grading and staging the histological lesions. Am. J. Gastroenterol. 1999, 94, 2467–2474. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.; Stepanova, M.; Ong, J.P.; Jacobson, I.M.; Bugianesi, E.; Duseja, A.; Eguchi, Y.; Wong, V.W.; Negro, F.; Yilmaz, Y.; et al. Nonalcoholic Steatohepatitis Is the Fastest Growing Cause of Hepatocellular Carcinoma in Liver Transplant Candidates. Clin. Gastroenterol. Hepatol. 2019, 17, 748–755.e743. [Google Scholar] [CrossRef] [PubMed]
- Ballestri, S.; Romagnoli, D.; Nascimbeni, F.; Francica, G.; Lonardo, A. Role of ultrasound in the diagnosis and treatment of nonalcoholic fatty liver disease and its complications. Expert Rev. Gastroenterol. Hepatol. 2015, 9, 603–627. [Google Scholar] [CrossRef]
- Ajmera, V.; Loomba, R. Can Elastography Differentiate Isolated Fatty Liver from Nonalcoholic Steatohepatitis? Semin. Liver Dis. 2018, 38, 14–20. [Google Scholar] [CrossRef]
- Siddiqui, M.S.; Vuppalanchi, R.; Van Natta, M.L.; Hallinan, E.; Kowdley, K.V.; Abdelmalek, M.; Neuschwander-Tetri, B.A.; Loomba, R.; Dasarathy, S.; Brandman, D.; et al. Vibration-Controlled Transient Elastography to Assess Fibrosis and Steatosis in Patients with Nonalcoholic Fatty Liver Disease. Clin. Gastroenterol. Hepatol. 2019, 17, 156–163.e152. [Google Scholar] [CrossRef]
- Deffieux, T.; Gennisson, J.-L.; Bousquet, L.; Corouge, M.; Cosconea, S.; Amroun, D.; Tripon, S.; Terris, B.; Mallet, V.; Sogni, P.; et al. Investigating liver stiffness and viscosity for fibrosis, steatosis and activity staging using shear wave elastography. J. Hepatol. 2015, 62, 317–324. [Google Scholar] [CrossRef]
- Sugimoto, K.; Moriyasu, F.; Oshiro, H.; Takeuchi, H.; Yoshimasu, Y.; Kasai, Y.; Itoi, T. Clinical utilization of shear wave dispersion imaging in diffuse liver disease. Ultrasonography 2020, 39, 3–10. [Google Scholar] [CrossRef]
- Morin, J.; Swanson, T.A.; Rinaldi, A.; Boucher, M.; Ross, T.; Hirenallur-Shanthappa, D. Application of Ultrasound and Shear Wave Elastography Imaging in a Rat Model of NAFLD/NASH. J. Vis. Exp. 2021, e62403. [Google Scholar] [CrossRef]
- Dietrich, C.F.; Bamber, J.; Berzigotti, A.; Bota, S.; Cantisani, V.; Castera, L.; Cosgrove, D.; Ferraioli, G.; Friedrich-Rust, M.; Gilja, O.H.; et al. EFSUMB Guidelines and Recommendations on the Clinical Use of Liver Ultrasound Elastography, Update 2017 (Short Version). Ultraschall Med. 2017, 38, 377–394. [Google Scholar] [CrossRef]
- Barr, R.G.; Ferraioli, G.; Palmeri, M.L.; Goodman, Z.D.; Garcia-Tsao, G.; Rubin, J.; Garra, B.; Myers, R.P.; Wilson, S.R.; Rubens, D.; et al. Elastography Assessment of Liver Fibrosis: Society of Radiologists in Ultrasound Consensus Conference Statement. Radiology 2015, 276, 845–861. [Google Scholar] [CrossRef]
- Sheka, A.C.; Adeyi, O.; Thompson, J.; Hameed, B.; Crawford, P.A.; Ikramuddin, S. Nonalcoholic Steatohepatitis: A Review. JAMA 2020, 323, 1175–1183. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Patients (n = 75) |
|---|---|
| Age (years, median, IQR) | 54.0 (40.0–60.0) |
| Sex (n, male:female) | 35:40 |
| Diabetes (n, yes:no) | 11:64 |
| Hypertension (n, yes:no) | 36:39 |
| BMI (kg/m2, median, IQR) | 25.8 (23.7–28.6) |
| Waist circumference (cm, mean ± SD) | 94.5 ± 10.0 |
| Liver biochemistry | |
| AST (IU/L, median, IQR) | 24.0 (19.0–29.0) |
| ALT (IU/L, median, IQR) | 24.0 (19.0–40.0) |
| GGT (IU/L, median, IQR) | 31.0 (19.8–49.8) |
| ALP (IU/L, mean ± SD) | 84.4 ± 24.1 |
| TBIL (μmol/L, median, IQR) | 12.9 (9.1–15.2) |
| Lipid profile | |
| TC (mg/dl, mean ± SD) | 5.3 ± 1.1 |
| HDL-C (mg/dl, median, IQR) | 1.2 (1.0–1.3) |
| LDL-C (mg/dl, mean ± SD) | 3.0 ± 0.7 |
| TG (mg/dl, median, IQR) | 1.8 (1.3–2.3) |
| ALB (g/dL, mean ± SD) | 43.4 ± 2.9 |
| PLT (×109/L, median, IQR) | 213.0 (180.8–257.8) |
| Glu (mg/dl, median, IQR) | 5.4 (5.0–6.0) |
| BUN (mmol/L, mean ± SD) | 4.9 ± 1.3 |
| UA (μmol/L, median, IQR) | 344.0 (300.0–442.5) |
| Depth (cm) | 1.8 (1.6–2.1) |
| Degree of steatosis (%) | |
| S0 (none, <5%) | 15 (20.0) |
| S1 (mild, 5–33%) | 41 (54.7) |
| S2 (moderate, >33–66%) | 13 (17.3) |
| S3 (severe, >66%) | 6 (8.0) |
| Intralobular Inflammation | |
| I0 (None) | 30 (40.0) |
| I1 (Mild) | 36 (48.0) |
| I2 (Moderate) | 7 (9.3) |
| I3 (Severe) | 2 (2.7) |
| Ballooning Degeneration | |
| B0 (None) | 59 (78.7) |
| B1 (Few balloon cells) | 13 (17.3) |
| B2 (Many cells/ prominent ballooning) | 3 (4.0) |
| Grade of fibrosis (%) | |
| F0 | 48 (64.0) |
| F1 | 20 (26.7) |
| F2 | 6 (8.0) |
| F3 | 1 (1.3) |
| F4 | 0 (0) |
| Pathological diagnosis | |
| Normal liver | 15 (20) |
| NAFL | 44 (58.7) |
| NASH | 16 (21.3) |
| Parameters | Cutoff Value | AUC (95% CI) | Sensitivity (%) (95% CI) | Specificity (%) (95% CI) | PLR (95% CI) | NLR (95% CI) |
|---|---|---|---|---|---|---|
| SWS | >1.3 | 0.719 (0.604, 0.817) | 62.5 (35.4, 84.8) | 81.4 (69.1, 90.3) | 3.35 (1.7, 6.4) | 0.46 (0.2, 0.9) |
| AC | >0.67 | 0.702 (0.582, 0.805) | 93.3 (68.1, 99.8) | 44.6 (31.3, 58.5) | 1.69 (1.3, 2.2) | 0.15 (0.02, 1.0) |
| NLV | ≤1.105 | 0.676 (0.554, 0.782) | 87.5 (61.7, 98.4) | 54.6 (40.6, 68.0) | 1.92 (1.4, 2.7) | 0.23 (0.06, 0.9) |
| Parameters | Training Set (n = 52) | Validation Set (n = 13) | p Value |
|---|---|---|---|
| age | 51.8 ± 11 | 50.0 ± 15 | 0.63 |
| Glu | 6.21 ± 2.36 | 5.45 ± 0.77 | 0.06 |
| SWS | 1.26 ± 0.14 | 1.27 ± 0.09 | 0.62 |
| AC | 0.75 ± 0.12 | 0.76 ± 0.14 | 0.76 |
| NLV | 1.13 ± 0.14 | 1.17 ± 0.12 | 0.35 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, Y.; Qiu, C.; Dong, Y.; Wang, X.; Chen, J.; Yao, J.; Jiang, Y.; Zhang, C.; Weng, H.; Liu, Y.; et al. Technical Acoustic Measurements Combined with Clinical Parameters for the Differential Diagnosis of Nonalcoholic Steatohepatitis. Diagnostics 2023, 13, 1547. https://doi.org/10.3390/diagnostics13091547
Zhao Y, Qiu C, Dong Y, Wang X, Chen J, Yao J, Jiang Y, Zhang C, Weng H, Liu Y, et al. Technical Acoustic Measurements Combined with Clinical Parameters for the Differential Diagnosis of Nonalcoholic Steatohepatitis. Diagnostics. 2023; 13(9):1547. https://doi.org/10.3390/diagnostics13091547
Chicago/Turabian StyleZhao, Yanan, Chen Qiu, Yiping Dong, Xuchu Wang, Jifan Chen, Jianting Yao, Yifan Jiang, Chao Zhang, Huifang Weng, Yajing Liu, and et al. 2023. "Technical Acoustic Measurements Combined with Clinical Parameters for the Differential Diagnosis of Nonalcoholic Steatohepatitis" Diagnostics 13, no. 9: 1547. https://doi.org/10.3390/diagnostics13091547