
Lactate versus Phosphate as Biomarkers to Aid Mechanical Circulatory Support Decisions in Patients with Out-of-Hospital Cardiac Arrest and Return of Spontaneous Circulation
 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
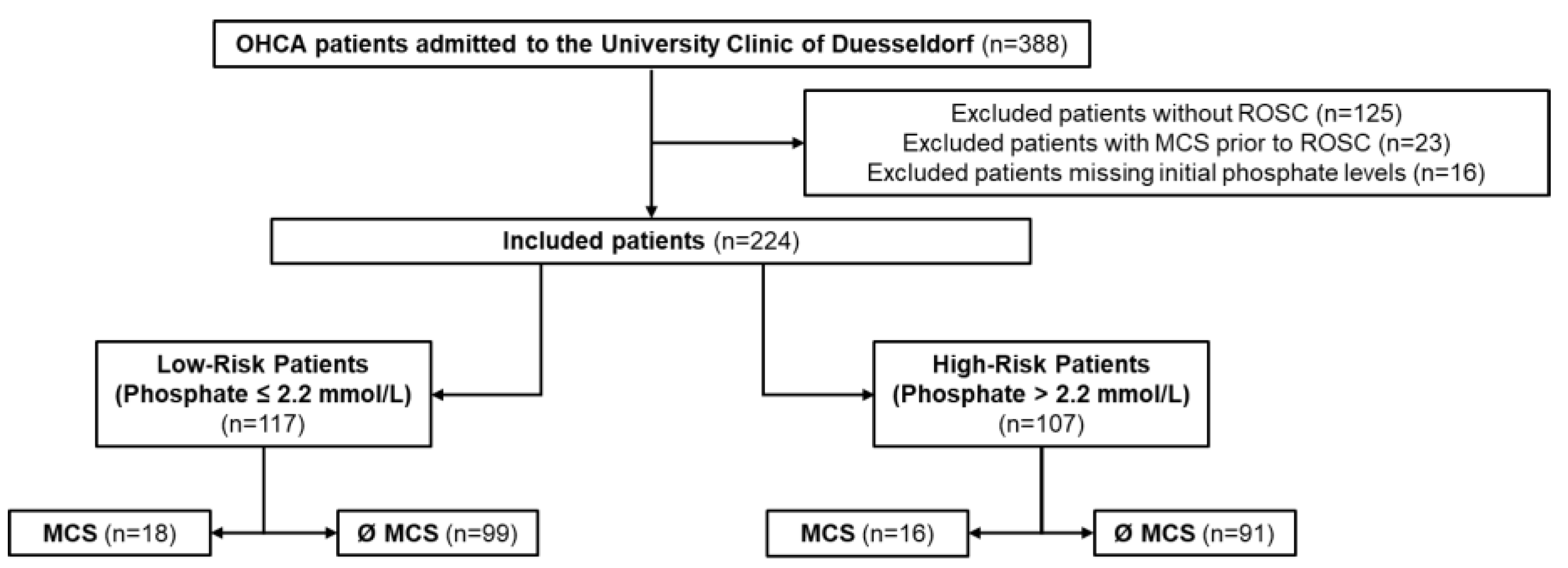
2.1. Study Design and Population
2.2. CPR and Mechanical Circulatory Support
2.3. Statistical Analysis
3. Results
3.1. Study Population
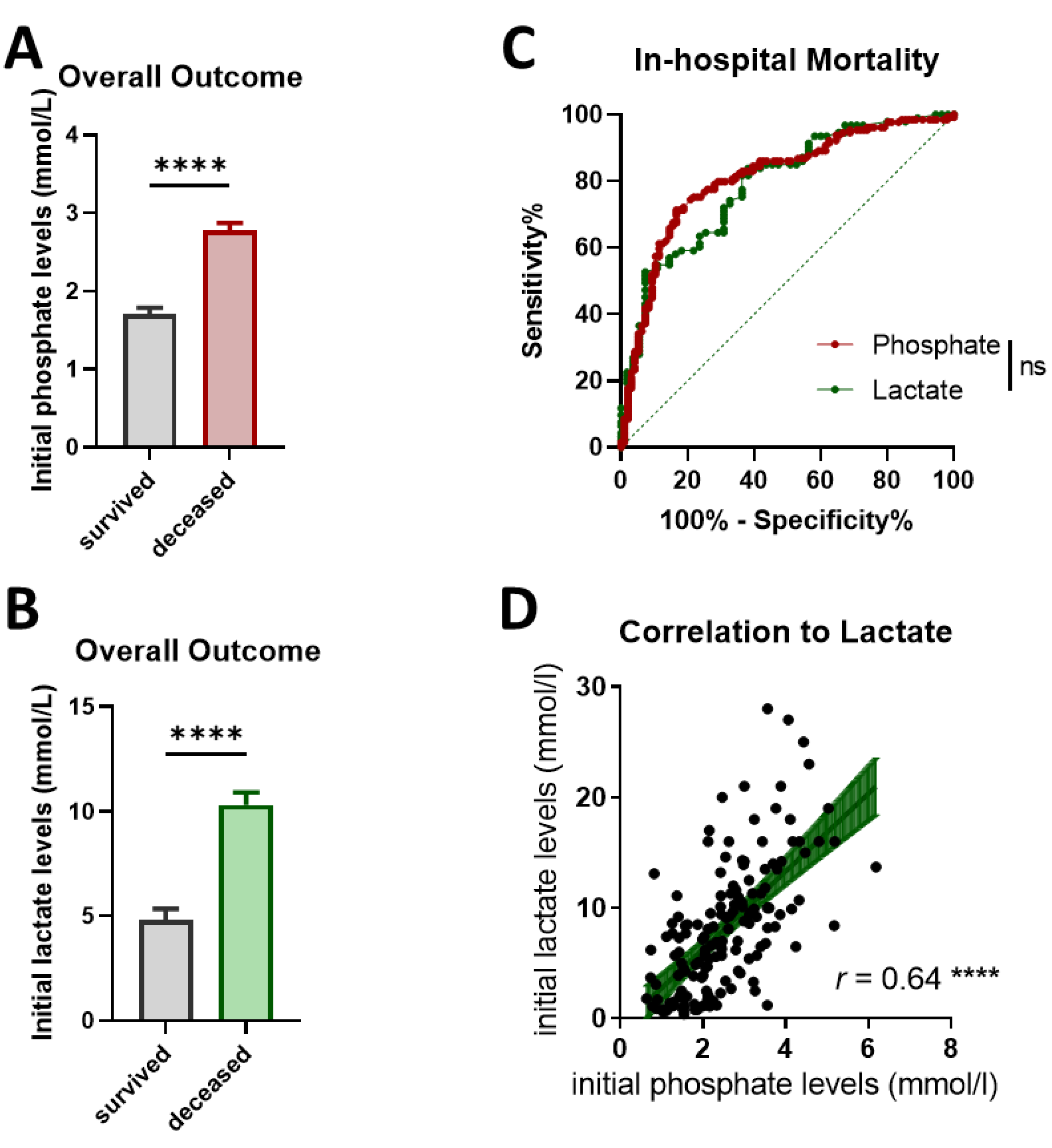
3.2. Initial Phosphate and Lactate Level Elevations in Deceased OHCA Patients
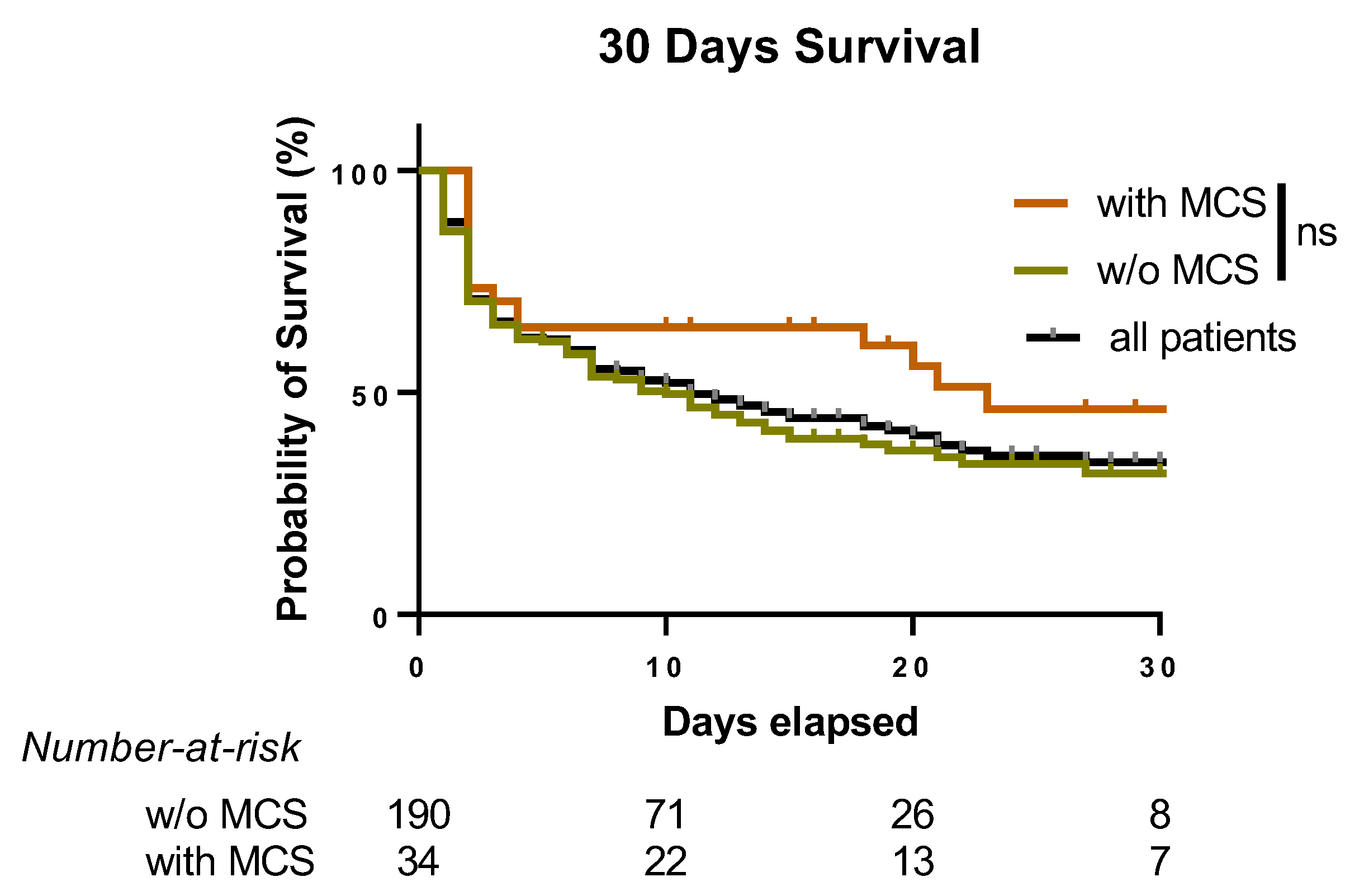
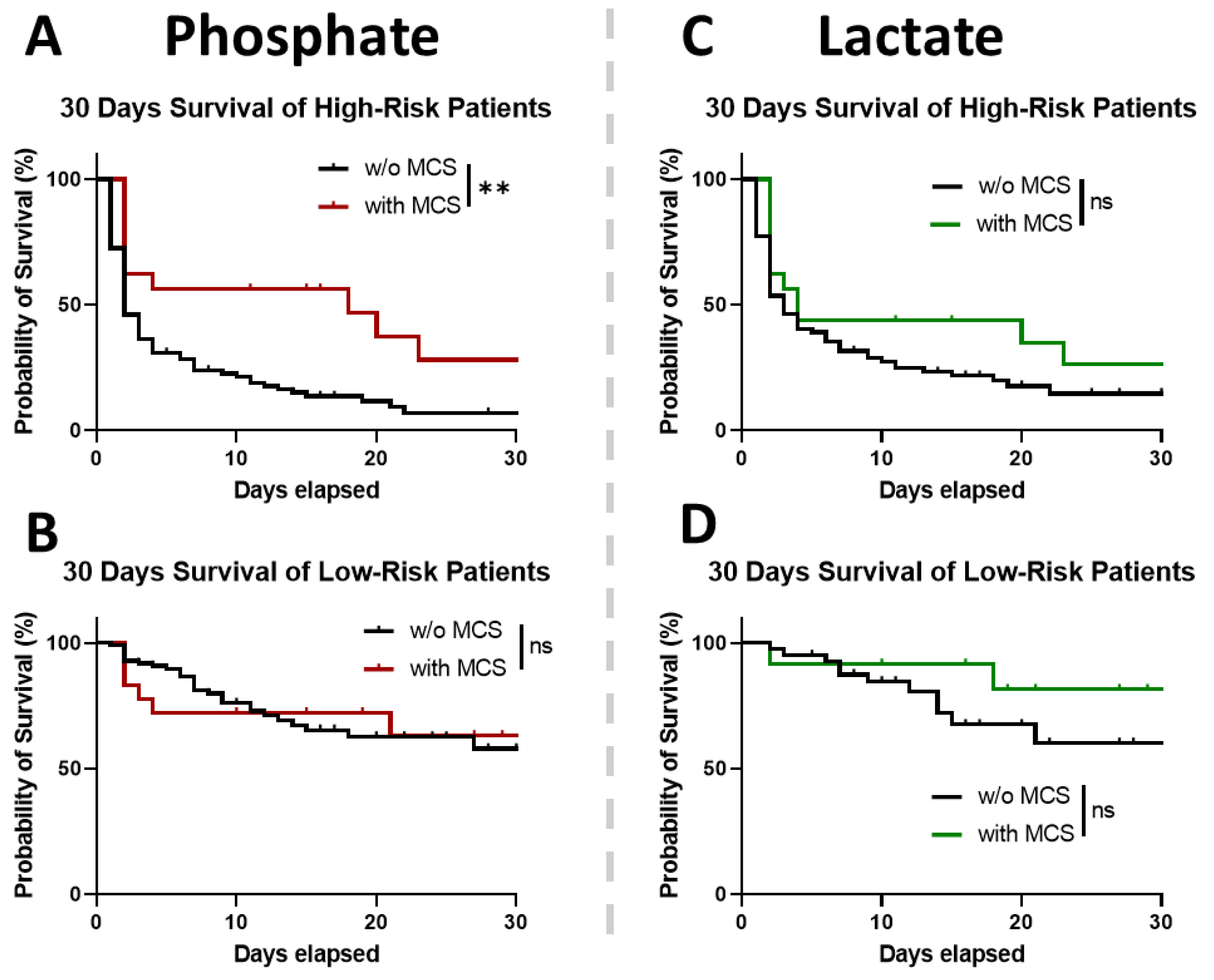
3.3. MCS Implementation in Low and High-Risk Patients Divided by Phosphate and Lactate
4. Discussion
Main Findings
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AHA | American Heart Association |
| AMI | acute myocardial infarction |
| AUC | area under the curve |
| CKD | chronic kidney disease |
| CS | cardiogenic shock |
| (e)CPR | (extracorporeal) cardiopulmonary resuscitation |
| HR | hazard ratios |
| LDH | Lactate Dehydrogenase |
| LV-EF | left-ventricular ejection fraction |
| MCS | mechanical circulatory support |
| OHCA | out-of-hospital cardiac arrest |
| RCT | randomized controlled trial |
| ROC | receiver-operating curve |
| ROSC | return of spontaneous circulation |
| SCAI | Society for Cardiovascular Angiography and Interventions |
| SEM | standard error of the mean |
| YI | Youden Index |
References
- Smith, T.W.; Cain, M.E. Sudden cardiac death: Epidemiologic and financial worldwide perspective. J. Interv. Card. Electrophysiol. 2006, 17, 199–203. [Google Scholar] [CrossRef] [PubMed]
- Czapla, M.; Zielińska, M.; Kubica-Cielińska, A.; Diakowska, D.; Quinn, T.; Karniej, P. Factors associated with return of spontaneous circulation after out-of-hospital cardiac arrest in Poland: A one-year retrospective study. BMC Cardiovasc. Disord. 2020, 20, 288. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.-C.; Hsu, C.W.; Hsu, S.C.; Chang, J.L.; Hsu, Y.P.; Lin, S.M.; Liu, Y.K. The factor influencing the rate of ROSC for nontraumatic OHCA in New Taipei city. Medicine 2021, 100, e28346. [Google Scholar] [CrossRef] [PubMed]
- Düring, J.; Annborn, M.; Dankiewicz, J.; Dupont, A.; Forsberg, S.; Friberg, H.; Kern, K.B.; May, T.L.; McPherson, J.; Patel, N.; et al. Influence of circulatory shock at hospital admission on outcome after out-of-hospital cardiac arrest. Sci. Rep. 2022, 12, 8293. [Google Scholar] [CrossRef] [PubMed]
- Jozwiak, M.; Bougouin, W.; Geri, G.; Grimaldi, D.; Cariou, A. Post-resuscitation shock: Recent advances in pathophysiology and treatment. Ann. Intensive Care 2020, 10, 170. [Google Scholar] [CrossRef]
- Martinell, L.; Nielsen, N.; Herlitz, J.; Karlsson, T.; Horn, J.; Wise, M.P.; Unden, J.; Rylander, C. Early predictors of poor outcome after out-of-hospital cardiac arrest. Crit. Care 2017, 21, 96. [Google Scholar] [CrossRef]
- Hallstrom, A.; Herlitz, J.; Kajino, K.; Olasveengen, T.M. Treatment of asystole and PEA. Resuscitation 2009, 80, 975–976. [Google Scholar] [CrossRef]
- Naidu, S.S.; Baran, D.A.; Jentzer, J.C.; Hollenberg, S.M.; van Diepen, S.; Basir, M.B.; Grines, C.L.; Diercks, D.B.; Hall, S.; Kapur, N.K.; et al. SCAI SHOCK Stage Classification Expert Consensus Update: A Review and Incorporation of Validation Studies: This statement was endorsed by the American College of Cardiology (ACC), American College of Emergency Physicians (ACEP), American Heart Association (AHA), European Society of Cardiology (ESC) Association for Acute Cardiovascular Care (ACVC), International Society for Heart and Lung Transplantation (ISHLT), Society of Critical Care Medicine (SCCM), and Society of Thoracic Surgeons (STS) in December 2021. J. Am. Coll. Cardiol. 2022, 79, 933–946. [Google Scholar] [CrossRef]
- Soar, J.; Berg, K.M.; Andersen, L.W.; Bottiger, B.W.; Cacciola, S.; Callaway, C.W.; Couper, K.; Cronberg, T.; D’Arrigo, S.; Deakin, C.D.; et al. Adult Advanced Life Support: 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Resuscitation 2020, 156, A80–A119. [Google Scholar] [CrossRef]
- Bartos, J.A.; Grunau, B.; Carlson, C.; Duval, S.; Ripeckyj, A.; Kalra, R.; Raveendran, G.; John, R.; Conterato, M.; Frascone, R.J.; et al. Improved Survival With Extracorporeal Cardiopulmonary Resuscitation Despite Progressive Metabolic Derangement Associated With Prolonged Resuscitation. Circulation 2020, 141, 877–886. [Google Scholar] [CrossRef]
- Ellouze, O.; Vuillet, M.; Perrot, J.; Grosjean, S.; Missaoui, A.; Aho, S.; Malapert, G.; Bouhemad, B.; Bouchot, O.; Girard, C. Comparable Outcome of Out-of-Hospital Cardiac Arrest and In-Hospital Cardiac Arrest Treated With Extracorporeal Life Support. Artif Organs 2018, 42, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Chatzis, G.; Markus, B.; Syntila, S.; Waechter, C.; Luesebrink, U.; Ahrens, H.; Divchev, D.; Schieffer, B.; Karatolios, K. Comparison of Mortality Risk Models in Patients with Postcardiac Arrest Cardiogenic Shock and Percutaneous Mechanical Circulatory Support. J. Interv. Cardiol. 2021, 2021, 8843935. [Google Scholar] [CrossRef] [PubMed]
- Geller, B.J.; Sinha, S.S.; Kapur, N.K.; Bakitas, M.; Balsam, L.B.; Chikwe, J.; Klein, D.G.; Kochar, A.; Masri, S.C.; Sims, D.B.; et al. Escalating and De-escalating Temporary Mechanical Circulatory Support in Cardiogenic Shock: A Scientific Statement From the American Heart Association. Circulation 2022, 146, e50–e68. [Google Scholar] [CrossRef] [PubMed]
- Thiele, H.; Ohman, E.M.; de Waha-Thiele, S.; Zeymer, U.; Desch, S. Management of cardiogenic shock complicating myocardial infarction: An update 2019. Eur. Heart J. 2019, 40, 2671–2683. [Google Scholar] [CrossRef] [PubMed]
- Thiele, H.; Zeymer, U.; Neumann, F.J.; Ferenc, M.; Olbrich, H.G.; Hausleiter, J.; Richardt, G.; Hennersdorf, M.; Empen, K.; Fuernau, G.; et al. Intraaortic balloon support for myocardial infarction with cardiogenic shock. N. Engl. J. Med. 2012, 367, 1287–1296. [Google Scholar] [CrossRef]
- Ostadal, P.; Rokyta, R.; Karasek, J.; Kruger, A.; Vondrakova, D.; Janotka, M.; Naar, J.; Smalcova, J.; Hubatova, M.; Hromadka, M.; et al. Extracorporeal Membrane Oxygenation in the Therapy of Cardiogenic Shock: Results of the ECMO-CS Randomized Clinical Trial. Circulation 2023, 147, 454–464. [Google Scholar] [CrossRef]
- Kraut, J.A.; Madias, N.E. Lactic Acidosis. N. Engl. J. Med. 2014, 371, 2309–2319. [Google Scholar] [CrossRef]
- Nishioka, N.; Kobayashi, D.; Izawa, J.; Irisawa, T.; Yamada, T.; Yoshiya, K.; Park, C.; Nishimura, T.; Ishibe, T.; Yagi, Y.; et al. Association between serum lactate level during cardiopulmonary resuscitation and survival in adult out-of-hospital cardiac arrest: A multicenter cohort study. Sci. Rep. 2021, 11, 1639. [Google Scholar] [CrossRef]
- Scolari, F.L.; Schneider, D.; Fogazzi, D.V.; Gus, M.; Rover, M.M.; Bonatto, M.G.; de Araújo, G.N.; Zimerman, A.; Sganzerla, D.; Goldraich, L.A.; et al. Association between serum lactate levels and mortality in patients with cardiogenic shock receiving mechanical circulatory support: A multicenter retrospective cohort study. BMC Cardiovasc. Disord. 2020, 20, 496. [Google Scholar] [CrossRef]
- Jensen, P.B.; Kann, S.H.; Veien, K.T.; Møller-Helgestad, O.K.; Dahl, J.S.; Rud, C.S.; Jensen, M.K.; Jensen, L.O.; Schmidt, H.; Møller, J.E. Single-centre experience with the Impella CP, 5.0 and RP in 109 consecutive patients with profound cardiogenic shock. Eur. Heart J. Acute Cardiovasc. Care 2018, 7, 53–61. [Google Scholar] [CrossRef]
- Duse, D.A.; Gröne, M.; Kramser, N.; Ortkemper, M.; Quast, C.; Voß, F.; Heramvand, N.; Kostev, K.; Kelm, M.; Horn, P.; et al. Elevated Initial Serum Phosphate Levels Predict Higher Mortality and Impaired Neurological Outcome in Cardiac Arrest Patients with Return of Spontaneous Circulation. Diagnostics 2023, 13, 479. [Google Scholar] [CrossRef] [PubMed]
- Jung, Y.H.; Lee, B.K.; Jeung, K.W.; Youn, C.S.; Lee, D.H.; Lee, S.M.; Heo, T.; Min, Y.I. Prognostic value of serum phosphate level in adult patients resuscitated from cardiac arrest. Resuscitation 2018, 128, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.Y.; Jung, Y.H.; Jeung, K.W.; Lee, B.K.; Youn, C.S.; Mamadjonov, N.; Kim, J.W.; Heo, T.; Min, Y.I. Ion shift index as a promising prognostic indicator in adult patients resuscitated from cardiac arrest. Resuscitation 2019, 137, 116–123. [Google Scholar] [CrossRef] [PubMed]
- Pesta, D.H.; Tsirigotis, D.N.; Befroy, D.E.; Caballero, D.; Jurczak, M.J.; Rahimi, Y.; Cline, G.W.; Dufour, S.; Birkenfeld, A.L.; Rothman, D.L.; et al. Hypophosphatemia promotes lower rates of muscle ATP synthesis. FASEB J. 2016, 30, 3378–3387. [Google Scholar] [CrossRef]
- Shibayama, J.; Taylor, T.G.; Venable, P.W.; Rhodes, N.L.; Gil, R.B.; Warren, M.; Wende, A.R.; Abel, E.D.; Cox, J.; Spitzer, K.W.; et al. Metabolic determinants of electrical failure in ex-vivo canine model of cardiac arrest: Evidence for the protective role of inorganic pyrophosphate. PLoS ONE 2013, 8, e57821. [Google Scholar] [CrossRef]
- Makino, J.; Uchino, S.; Morimatsu, H.; Bellomo, R. A quantitative analysis of the acidosis of cardiac arrest: A prospective observational study. Crit. Care 2005, 9, R357–R362. [Google Scholar] [CrossRef]
- Oster, J.R.; Alpert, H.C.; Vaamonde, C.A. Effect of acid-base status on plasma phosphorus response to lactate. Can. J. Physiol. Pharm. 1984, 62, 939–942. [Google Scholar] [CrossRef]
- Kliegel, A.; Losert, H.; Sterz, F.; Holzer, M.; Zeiner, A.; Havel, C.; Laggner, A.N. Serial lactate determinations for prediction of outcome after cardiac arrest. Medicine 2004, 83, 274–279. [Google Scholar] [CrossRef]
- Monsieurs, K.G.; Nolan, J.P.; Bossaert, L.L.; Greif, R.; Maconochie, I.K.; Nikolaou, N.I.; Perkins, G.D.; Soar, J.; Truhlar, A.; Wyllie, J.; et al. European Resuscitation Council Guidelines for Resuscitation 2015: Section 1. Executive summary. Resuscitation 2015, 95, 1–80. [Google Scholar] [CrossRef]
- Donnino, M.W.; Andersen, L.W.; Giberson, T.; Gaieski, D.F.; Abella, B.S.; Peberdy, M.A.; Rittenberger, J.C.; Callaway, C.W.; Ornato, J.; Clore, J.; et al. Initial lactate and lactate change in post-cardiac arrest: A multicenter validation study. Crit. Care Med. 2014, 42, 1804–1811. [Google Scholar] [CrossRef]
- Rugg, C.; Bachler, M.; Kammerlander, R.; Niederbrunner, D.; Bösch, J.; Schmid, S.; Kreutziger, J.; Ströhle, M. ICU-Admission Hyperphosphataemia Is Related to Shock and Tissue Damage, Indicating Injury Severity and Mortality in Polytrauma Patients. Diagnostics 2021, 11, 1548. [Google Scholar] [CrossRef] [PubMed]
- Linde, L.; Mørk, S.R.; Gregers, E.; Andreasen, J.B.; Lassen, J.F.; Ravn, H.B.; Schmidt, H.; Riber, L.P.; Thomassen, S.A.; Laugesen, H.; et al. Selection of patients for mechanical circulatory support for refractory out-of-hospital cardiac arrest. Heart 2023, 109, 216–222. [Google Scholar] [CrossRef]
- Neumar, R.W.; Nolan, J.P.; Adrie, C.; Aibiki, M.; Berg, R.A.; Bottiger, B.W.; Callaway, C.; Clark, R.S.; Geocadin, R.G.; Jauch, E.C.; et al. Post-cardiac arrest syndrome: Epidemiology, pathophysiology, treatment, and prognostication. A consensus statement from the International Liaison Committee on Resuscitation (American Heart Association, Australian and New Zealand Council on Resuscitation, European Resuscitation Council, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Council of Asia, and the Resuscitation Council of Southern Africa); the American Heart Association Emergency Cardiovascular Care Committee; the Council on Cardiovascular Surgery and Anesthesia; the Council on Cardiopulmonary, Perioperative, and Critical Care; the Council on Clinical Cardiology; and the Stroke Council. Circulation 2008, 118, 2452–2483. [Google Scholar] [CrossRef]
- Bartos, J.A. The rise of the machines: ECLS and other temporary mechanical support for patients with cardiac arrest. Resuscitation 2020, 151, 208–210. [Google Scholar] [CrossRef] [PubMed]
- Karatolios, K.; Chatzis, G.; Markus, B.; Luesebrink, U.; Ahrens, H.; Dersch, W.; Betz, S.; Ploeger, B.; Boesl, E.; O’Neill, W.; et al. Impella support compared to medical treatment for post-cardiac arrest shock after out of hospital cardiac arrest. Resuscitation 2018, 126, 104–110. [Google Scholar] [CrossRef]
- Bertaina, M.; Galluzzo, A.; Morici, N.; Sacco, A.; Oliva, F.; Valente, S.; D’Ascenzo, F.; Frea, S.; Sbarra, P.; Petitti, E.; et al. Pulmonary Artery Catheter Monitoring in Patients with Cardiogenic Shock: Time for a Reappraisal? Card. Fail. Rev. 2022, 8, e15. [Google Scholar] [CrossRef]
- Smolenski, R.T.; Swierczynski, J.; Narkiewicz, M.; Zydowo, M.M. Purines, lactate and phosphate release from child and adult heart during cardioplegic arrest. Clin. Chim. Acta 1990, 192, 155–163. [Google Scholar] [CrossRef]
- Dundar, Z.D.; Cander, B.; Gul, M.; Karabulut, K.U.; Kocak, S.; Girisgin, S.; Mehmetoglu, I.; Toy, H. Serum intestinal fatty acid binding protein and phosphate levels in the diagnosis of acute intestinal ischemia: An experimental study in rabbits. J. Emerg. Med. 2012, 42, 741–747. [Google Scholar] [CrossRef]
- Malberti, F. Hyperphosphataemia: Treatment options. Drugs 2013, 73, 673–688. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean ± SEM, N = 224 | Total |
|---|---|
| Study Population | |
| age [years] | 65.4 ± 0.99 |
| gender [% male] | 65.6 |
| survival [%] | 42.4 |
| Initial Laboratory Values | |
| phosphate [mmol/L] | 2.34 ± 0.07 |
| creatinine [mg/dL] | 1.5 ± 0.07 |
| lactate [mmol/L] (n =154) | 8.15 ± 0.47 |
| potassium [mmol/L] | 4.5 ± 0.07 |
| LDH [U/L] | 646.5 ± 57.8 |
| NSE [µg/L] (n = 193) | 103.6 ± 7.87 |
| CPR Data | |
| MCS [%] | 15.2 |
| AMI [%] | 37.1 |
| bystander CPR [%] | 44.8 |
| initial rhythm (VT/VFib) [%] | 49.6 |
| time to ROSC [min] | 25.2 ± 1.7 |
| witnessed arrest [%] | 71.9 |
| compression-only CPR [%] | 41 |
| Mean ± SEM, n = 107 | MCS | w/o MCS | p-Value |
|---|---|---|---|
| Study subpopulation | |||
| n | 16 | 91 | --- |
| age [years] | 55.5 ± 3.5 | 64.9 ± 1.65 | 0.0179 |
| gender [% male] | 68.75 | 71.43 | 0.7749 |
| survival [%] | 37.5 | 12.09 | 0.02 |
| Initial Laboratory Values | |||
| phosphate [mmol/L] | 3.3 ± 0.17 | 3.2 ± 0.09 | 0.6510 |
| creatinine [mg/dL] | 1.3 ± 0.10 | 1.8 ± 0.14 | 0.3540 |
| lactate [mmol/L] (n = 85) | 9.8 ± 0.79 | 11.4 ± 0.72 | 0.3304 |
| potassium [mmol/L] | 4.2 ± 0.21 | 4.7 ± 0.13 | 0.1835 |
| LDH [U/L] | 582 ± 60 | 905 ± 134 | 0.5633 |
| CPR Data | |||
| AMI [%] | 50 | 23.08 | 0.0347 |
| bystander CPR [%] | 43.75 | 46.15 | >0.9999 |
| initial rhythm (VT/VFib) [%] | 81.25 | 35.16 | 0.0008 |
| time to ROSC [min] | 31.9 ± 5.6 | 36.1 ± 3.2 | 0.9983 |
| witnessed arrest [%] | 81.25 | 67.03 | 0.3806 |
| compression-only CPR [%] | 31.25 | 53.85 | 0.1110 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duse, D.A.; Voß, F.; Heyng, L.; Wolff, G.; Quast, C.; Scheiber, D.; Horn, P.; Kelm, M.; Westenfeld, R.; Jung, C.; et al. Lactate versus Phosphate as Biomarkers to Aid Mechanical Circulatory Support Decisions in Patients with Out-of-Hospital Cardiac Arrest and Return of Spontaneous Circulation. Diagnostics 2023, 13, 1523. https://doi.org/10.3390/diagnostics13091523
Duse DA, Voß F, Heyng L, Wolff G, Quast C, Scheiber D, Horn P, Kelm M, Westenfeld R, Jung C, et al. Lactate versus Phosphate as Biomarkers to Aid Mechanical Circulatory Support Decisions in Patients with Out-of-Hospital Cardiac Arrest and Return of Spontaneous Circulation. Diagnostics. 2023; 13(9):1523. https://doi.org/10.3390/diagnostics13091523
Chicago/Turabian StyleDuse, Dragos Andrei, Fabian Voß, Laura Heyng, Georg Wolff, Christine Quast, Daniel Scheiber, Patrick Horn, Malte Kelm, Ralf Westenfeld, Christian Jung, and et al. 2023. "Lactate versus Phosphate as Biomarkers to Aid Mechanical Circulatory Support Decisions in Patients with Out-of-Hospital Cardiac Arrest and Return of Spontaneous Circulation" Diagnostics 13, no. 9: 1523. https://doi.org/10.3390/diagnostics13091523