
Multiparametric Skin Assessment in a Monocentric Cohort of Systemic Sclerosis Patients: Is There a Role for Ultra-High Frequency Ultrasound?

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
- -
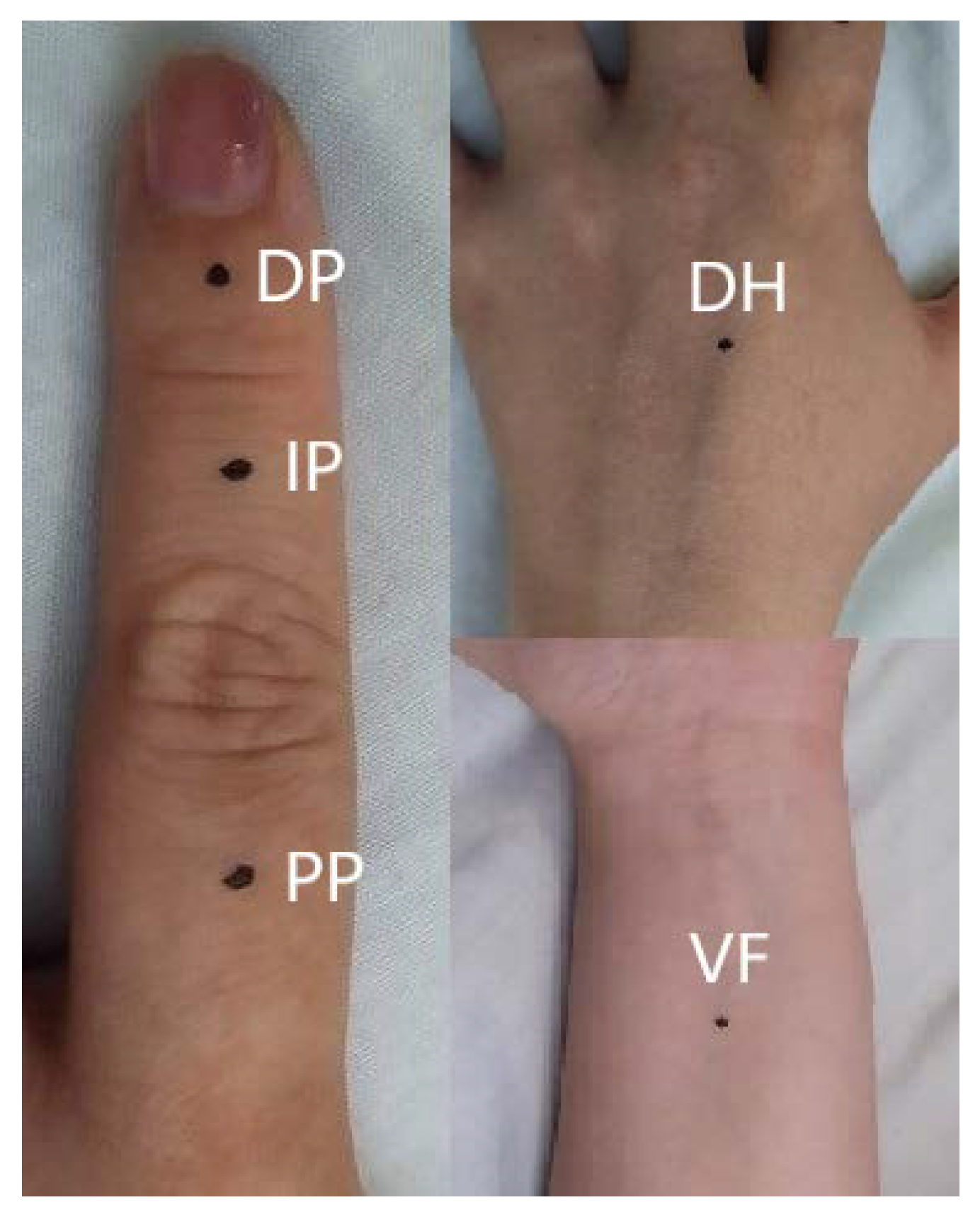
- on the central dorsal side of the intermediate phalanx (IP) of the second finger.
- -
- on the central dorsal side of the proximal phalanx (PP) of the second finger.
- -
- on the dorsum of the hand (DH) (3 cm distally to the wrist joint).
- -
- on the volar side of the forearm (VF) (5 cm proximally to the wrist joint).
2.2. Instrumental Assessment
2.3. Statistical Analysis
3. Results
3.1. Patients and mRSS
3.2. Durometer
3.3. UHFUS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Di Battista, M.; Barsotti, S.; Orlandi, M.; Lepri, G.; Codullo, V.; Della Rossa, A.; Guiducci, S.; Del Galdo, F. One year in review 2021: Systemic sclerosis. Clin. Exp. Rheumatol. 2021, 39, 3–12. [Google Scholar] [CrossRef]
- D’Oria, M.; Gandin, I.; Riccardo, P.; Hughes, M.; Lepidi, S.; Salton, F.; Confalonieri, P.; Confalonieri, M.; Tavano, S.; Ruaro, B. Correlation between Microvascular Damage and Internal Organ Involvement in Scleroderma: Focus on Lung Damage and Endothelial Dysfunction. Diagnostics 2023, 13, 55. [Google Scholar] [CrossRef]
- Czirják, L.; Foeldvari, I.; Müller-Ladner, U. Skin involvement in systemic sclerosis. Rheumatology 2008, 47, v44–v45. [Google Scholar] [CrossRef]
- Tieu, A.; Chaigne, B.; Dunogué, B.; Dion, J.; Régent, A.; Casadevall, M.; Cohen, P.; Legendre, P.; Terrier, B.; Costedoat-Chalumeau, N.; et al. Autoantibodies versus Skin Fibrosis Extent in Systemic Sclerosis: A Case-Control Study of Inverted Phenotypes. Diagnostics 2022, 12, 1067. [Google Scholar] [CrossRef]
- Khanna, D.; Furst, D.E.; Clements, P.J.; Allanore, Y.; Baron, M.; Czirjak, L.; Distler, O.; Foeldvari, I.; Kuwana, M.; Matucci-Cerinic, M.; et al. Standardization of the modified Rodnan skin score for use in clinical trials of systemic sclerosis. J. Scleroderma Relat. Disord. 2017, 2, 11–18. [Google Scholar] [CrossRef]
- Merkel, P.A.; Silliman, N.P.; Denton, C.P.; Furst, D.E.; Khanna, D.; Emery, P.; Hsu, V.M.; Streisand, J.B.; Polisson, R.P.; Åkesson, A.; et al. Validity, reliability, and feasibility of durometer measurements of scleroderma skin disease in a multicenter treatment trial. Arthritis Rheumatol. 2008, 59, 699–705. [Google Scholar] [CrossRef]
- Santiago, T.; Santiago, M.; Ruaro, B.; Salvador, M.J.; Cutolo, M.; da Silva, J.A.P. Ultrasonography for the assessment of skin in systemic sclerosis: A systematic review. Arthritis Care Res. 2019, 71, 563–574. [Google Scholar] [CrossRef]
- Naredo, E.; Pascau, J.; Damjanov, N.; Lepri, G.; Gordaliza, P.M.; Janta, I.; Ovalles-Bonilla, J.G.; López-Longo, F.J.; Matucci-Cerinic, M. Performance of ultra-high-frequency ultrasound in the evaluation of skin involvement in systemic sclerosis: A preliminary report. Rheumatology 2020, 59, 1671–1678. [Google Scholar] [CrossRef]
- Van Den Hoogen, F.; Khanna, D.; Fransen, J.; Johnson, S.R.; Baron, M.; Tyndall, A.; Matucci-Cerinic, M.; Naden, R.P.; Medsger, T.A.; Carreira, P.E.; et al. 2013 classification criteria for systemic sclerosis: An American college of rheumatology/European league against rheumatism collaborative initiative. Ann. Rheum. Dis. 2013, 72, 1747–1755. [Google Scholar] [CrossRef]
- LeRoy, E.; Black, C.; Fleischmajer, R.; Jablonska, S.; Krieg, T.; Medsger, T.A.; Wollheim, F. Scleroderma (systemic sclerosis): Classification, subsets and pathogenesis. J. Rheumatol. 1988, 15, 202–205. [Google Scholar]
- Moon, K.W.; Song, R.; Kim, J.H.; Lee, E.Y.; Lee, E.B.; Song, Y.W. The correlation between durometer score and modified Rodnan skin score in systemic sclerosis. Rheumatol. Int. 2012, 32, 2465–2470. [Google Scholar] [CrossRef]
- Dinsdale, G.; Wilkinson, S.; Wilkinson, J.; Moore, T.L.; Manning, J.B.; Berks, M.; Marjanovic, E.; Dickinson, M.; Herrick, A.L.; Murray, A.K. State-of-the-art technologies provide new insights linking skin and blood vessel abnormalities in SSc-related disorders. Microvasc. Res. 2020, 130, 104006. [Google Scholar] [CrossRef]
- Hesselstrand, R.; Scheja, A.; Wildt, M.; Åkesson, A. High-frequency ultrasound of skin involvement in systemic sclerosis reflects oedema, extension and severity in early disease. Rheumatology 2008, 47, 84–87. [Google Scholar] [CrossRef]
- Kaloudi, O.; Bandinelli, F.; Filippucci, E.; Conforti, M.L.; Miniati, I.; Guiducci, S.; Porta, F.; Candelieri, A.; Conforti, D.; Grassiri, G.; et al. High frequency ultrasound measurement of digital dermal thickness in systemic sclerosis. Ann. Rheum. Dis. 2010, 69, 1140–1143. [Google Scholar] [CrossRef]
- Hesselstrand, R.; Carlestam, J.; Wildt, M.; Sandqvist, G.; Andréasson, K. High frequency ultrasound of skin involvement in systemic sclerosis—A follow-up study. Arthritis Res. Ther. 2015, 17, 329. [Google Scholar] [CrossRef]
- Sulli, A.; Ruaro, B.; Smith, V.; Paolino, S.; Pizzorni, C.; Pesce, G.; Cutolo, M. Subclinical dermal involvement is detectable by high frequency ultrasound even in patients with limited cutaneous systemic sclerosis. Arthritis Res. Ther. 2017, 19, 61. [Google Scholar] [CrossRef]
- Li, H.; Furst, D.E.; Jin, H.; Sun, C.; Wang, X.; Yang, L.; He, J.; Wang, Y.; Liu, A. High-frequency ultrasound of the skin in systemic sclerosis: An exploratory study to examine correlation with disease activity and to define the minimally detectable difference. Arthritis Res. Ther. 2018, 20, 181. [Google Scholar] [CrossRef]
- Kissin, E.Y.; Schiller, A.M.; Gelbard, R.B.; Anderson, J.J.; Falanga, V.; Simms, R.W.; Korn, J.H.; Merkel, P.A. Durometry for the assessment of skin disease in systemic sclerosis. Arthritis Rheumatol. 2006, 55, 603–609. [Google Scholar] [CrossRef]
- Santiago, T.; Santos, E.; Ruaro, B.; Lepri, G.; Green, L.; Wildt, M.; Watanabe, S.; Lescoat, A.; Hesselstrand, R.; Del Galdo, F.; et al. Ultrasound and elastography in the assessment of skin involvement in systemic sclerosis: A systematic literature review focusing on validation and standardization – WSF Skin Ultrasound Group. Semin. Arthritis Rheum. 2022, 52, 151954. [Google Scholar] [CrossRef]
- Dźwigała, M.; Sobolewski, P.; Maślińska, M.; Yurtsever, I.; Szymańska, E.; Walecka, I. High-resolution ultrasound imaging of skin involvement in systemic sclerosis: A systematic review. Rheumatol. Int. 2021, 41, 285–295. [Google Scholar] [CrossRef]
- Kumánovics, G.; Péntek, M.; Bae, S.; Opris, D.; Khanna, D.; Furst, D.E.; Czirják, L. Assessment of skin involvement in systemic sclerosis. Rheumatology 2017, 56, V53–V66. [Google Scholar] [CrossRef] [PubMed]
- Flower, V.A.; Barratt, S.L.; Hart, D.J.; Mackenzie, A.B.; Shipley, J.A.; Ward, S.G.; Pauling, J.D. High-frequency ultrasound assessment of systemic sclerosis skin involvement: Intraobserver repeatability and relationship with clinician assessment and dermal collagen content. J. Rheumatol. 2021, 48, 867–876. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Cheng, Y.; Zhu, X.; Cai, Y.; Xue, Y.; Kong, N.; Yu, Y.; Xuan, D.; Zheng, S.; Yang, X.; et al. Ultrasound assessment of skin thickness and stiffness: The correlation with histology and clinical score in systemic sclerosis. Arthritis Res. Ther. 2020, 22, 197. [Google Scholar] [CrossRef]
- Ruaro, B.; Soldano, S.; Smith, V.; Paolino, S.; Contini, P.; Montagna, P.; Pizzorni, C.; Casabella, A.; Tardito, S.; Sulli, A.; et al. Correlation between circulating fibrocytes and dermal thickness in limited cutaneous systemic sclerosis patients: A pilot study. Rheumatol. Int. 2019, 39, 1369–1376. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| SSc (n = 47) | HC (n = 15) | p | |
|---|---|---|---|
| Female | 41 (87.2%) | 11 (73.3%) | n.s. |
| Age (years) | 56.4 ± 13.5 | 54.7 ± 14.3 | n.s. |
| Disease duration (years) | 10.8 ± 10.3 | ||
| ACA | 27 (57.4%) | ||
| Scl70 | 16 (34%) | ||
| - ssSSc | 9 (19.1%) | ||
| - lcSSc | 27 (57.4%) | ||
| - dcSSc | 11 (23.4%) | ||
| DUs history | 22 (46.8%) | ||
| Hand contractures | 5 (10.6%) |
| SSc (n = 47) | HC (n = 15) | p | |
|---|---|---|---|
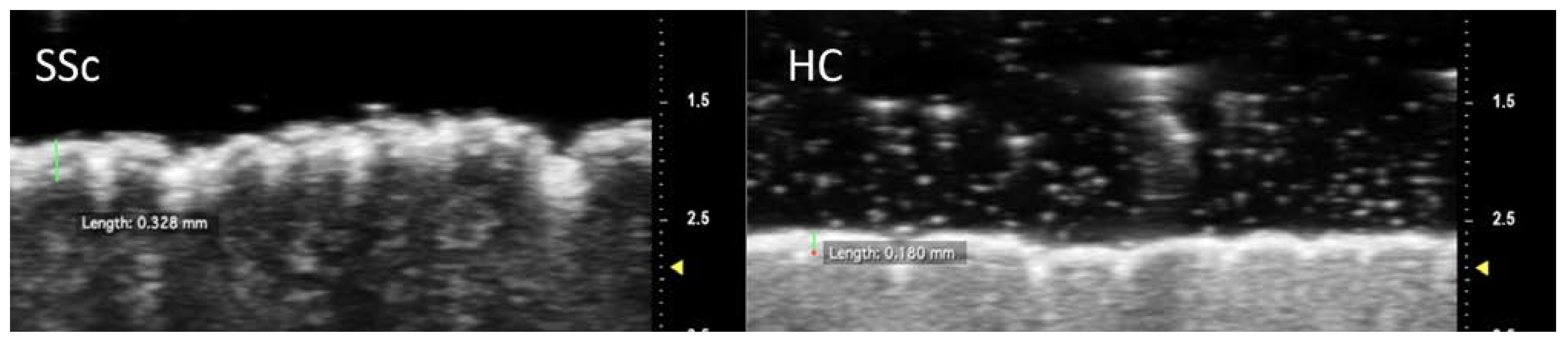
| Epidermal thickness (µm) | |||
| - DP | 258.6 ± 64.2 | 176.5 ± 21.1 | <0.001 |
| - IP | 238.4 ± 77.7 | 173.3 ± 20.3 | <0.001 |
| - PP | 206.9 ± 42.9 | 156.2 ± 18.1 | <0.001 |
| - DH | 182.1 ± 33.3 | 146.7 ± 12.7 | <0.001 |
| - VF | 180.1 ± 36.4 | 143.0 ± 18.0 | <0.001 |
| Epidermal MGV (0–255) | |||
| - DP | 168.6 ± 40.6 | 191.0 ± 23.7 | 0.01 |
| - IP | 168.2 ± 37.8 | 195.6 ± 20.9 | 0.01 |
| - PP | 174.2 ± 38.8 | 193.4 ± 18.8 | 0.01 |
| - DH | 184.5 ± 27.7 | 195.1 ± 19.2 | n.s. |
| - VF | 185.4 ± 24.6 | 190.1 ± 39.9 | n.s. |
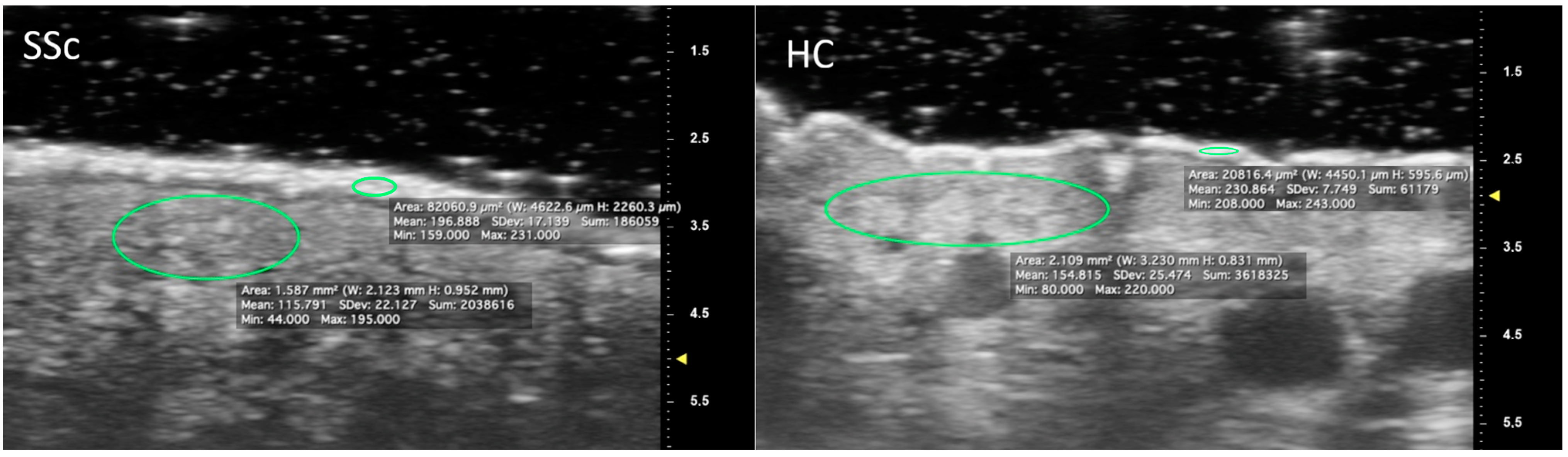
| Dermal MGV (0–255) | |||
| - DP | 62.9 ± 33.5 | 100.8 ± 27.2 | <0.001 |
| - IP | 70.0 ± 35.6 | 98.3 ± 25.8 | 0.006 |
| - PP | 87.0 ± 37.9 | 107.4 ± 13.8 | 0.04 |
| - DH | 109.4 ± 32.7 | 118.1 ± 22.0 | n.s. |
| - VF | 124.7 ± 33.8 | 130.6 ± 31.5 | n.s. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Battista, M.; Barsotti, S.; Vitali, S.; Palma, M.; Granieri, G.; Oranges, T.; Aringhieri, G.; Dini, V.; Della Rossa, A.; Neri, E.; et al. Multiparametric Skin Assessment in a Monocentric Cohort of Systemic Sclerosis Patients: Is There a Role for Ultra-High Frequency Ultrasound? Diagnostics 2023, 13, 1495. https://doi.org/10.3390/diagnostics13081495
Di Battista M, Barsotti S, Vitali S, Palma M, Granieri G, Oranges T, Aringhieri G, Dini V, Della Rossa A, Neri E, et al. Multiparametric Skin Assessment in a Monocentric Cohort of Systemic Sclerosis Patients: Is There a Role for Ultra-High Frequency Ultrasound? Diagnostics. 2023; 13(8):1495. https://doi.org/10.3390/diagnostics13081495
Chicago/Turabian StyleDi Battista, Marco, Simone Barsotti, Saverio Vitali, Marco Palma, Giammarco Granieri, Teresa Oranges, Giacomo Aringhieri, Valentina Dini, Alessandra Della Rossa, Emanuele Neri, and et al. 2023. "Multiparametric Skin Assessment in a Monocentric Cohort of Systemic Sclerosis Patients: Is There a Role for Ultra-High Frequency Ultrasound?" Diagnostics 13, no. 8: 1495. https://doi.org/10.3390/diagnostics13081495