
Update on the Applications of Radiomics in Diagnosis, Staging, and Recurrence of Intrahepatic Cholangiocarcinoma
 , , , , , and
, , , , , and 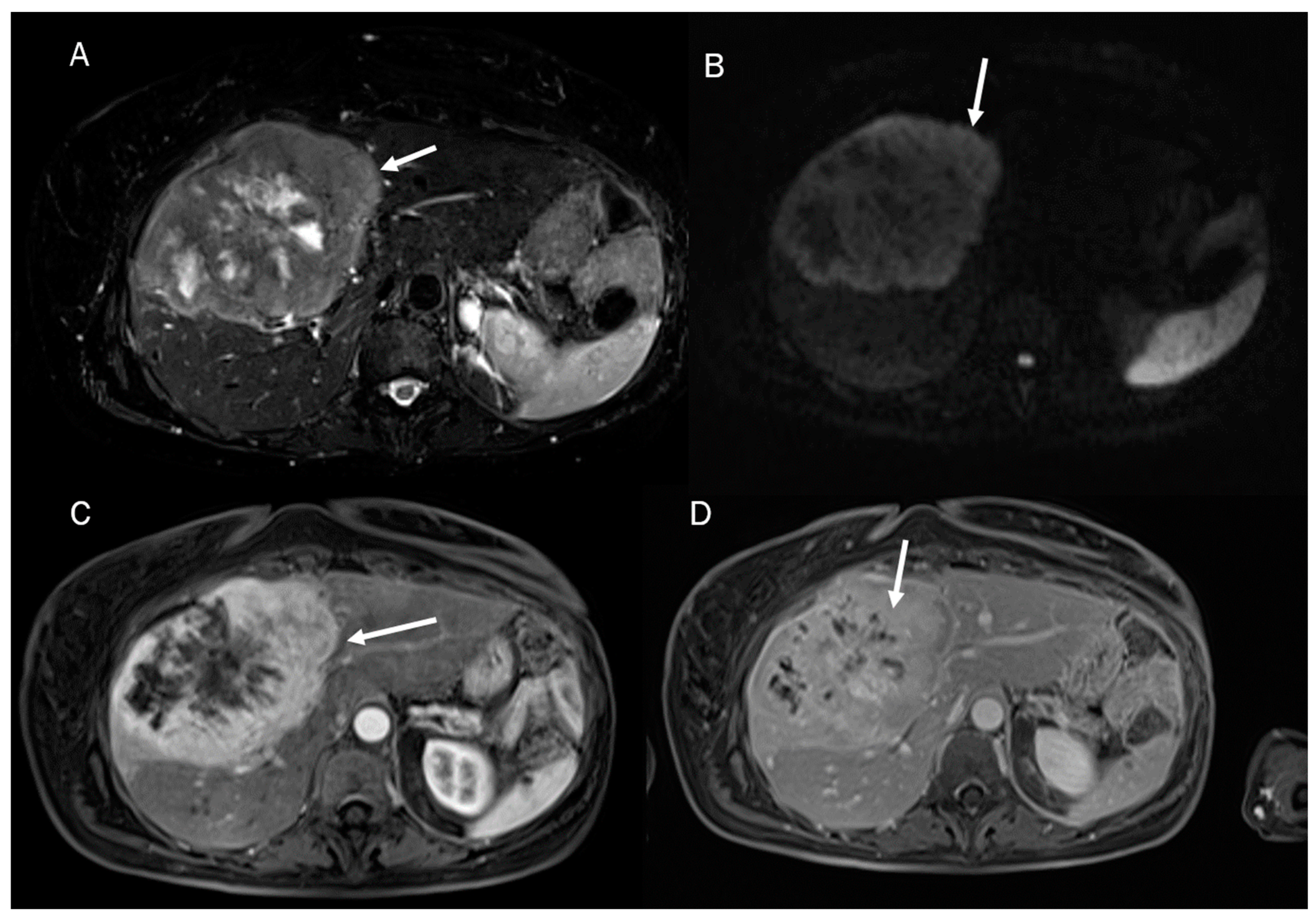{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
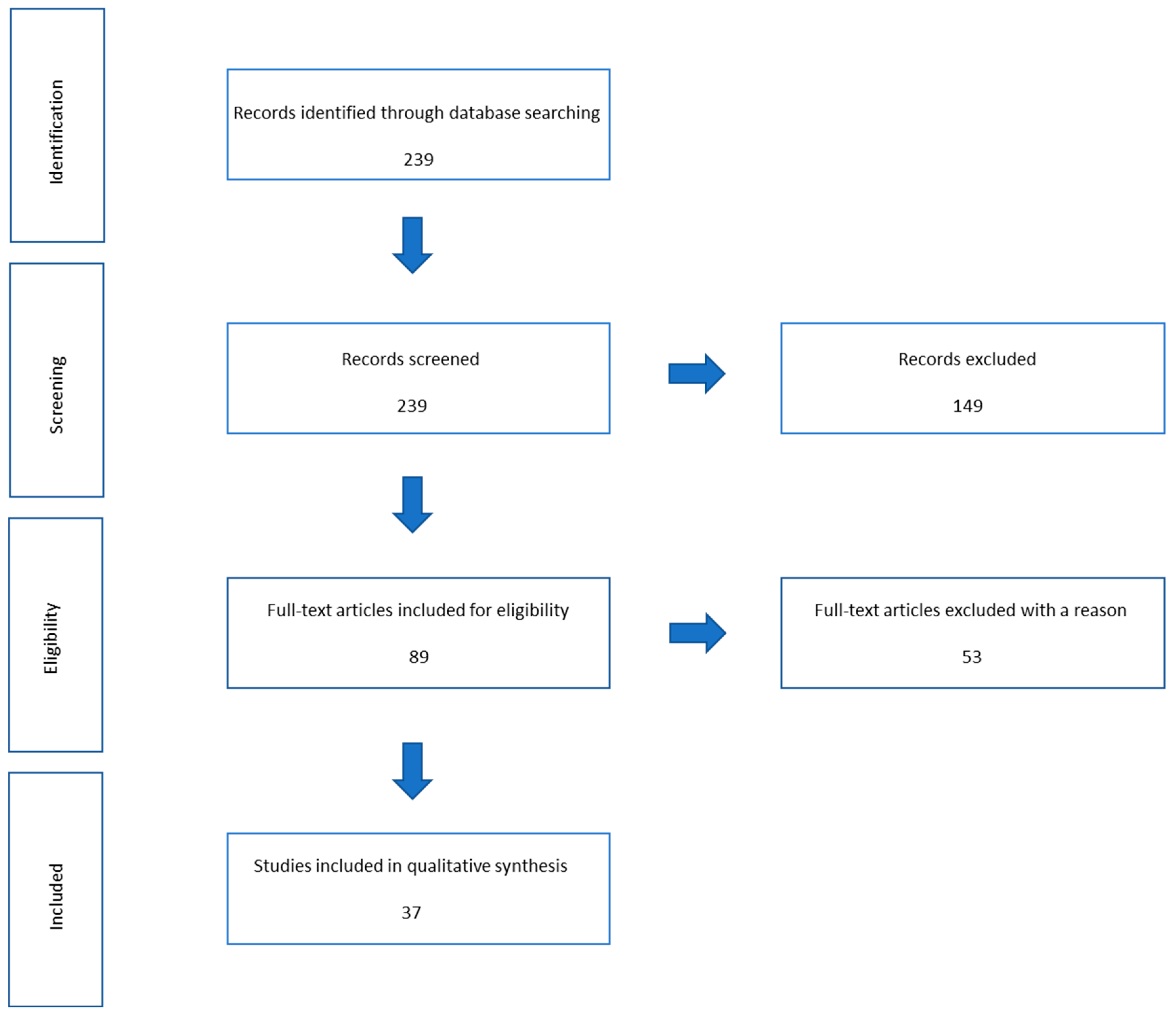
2. Methods
3. Results
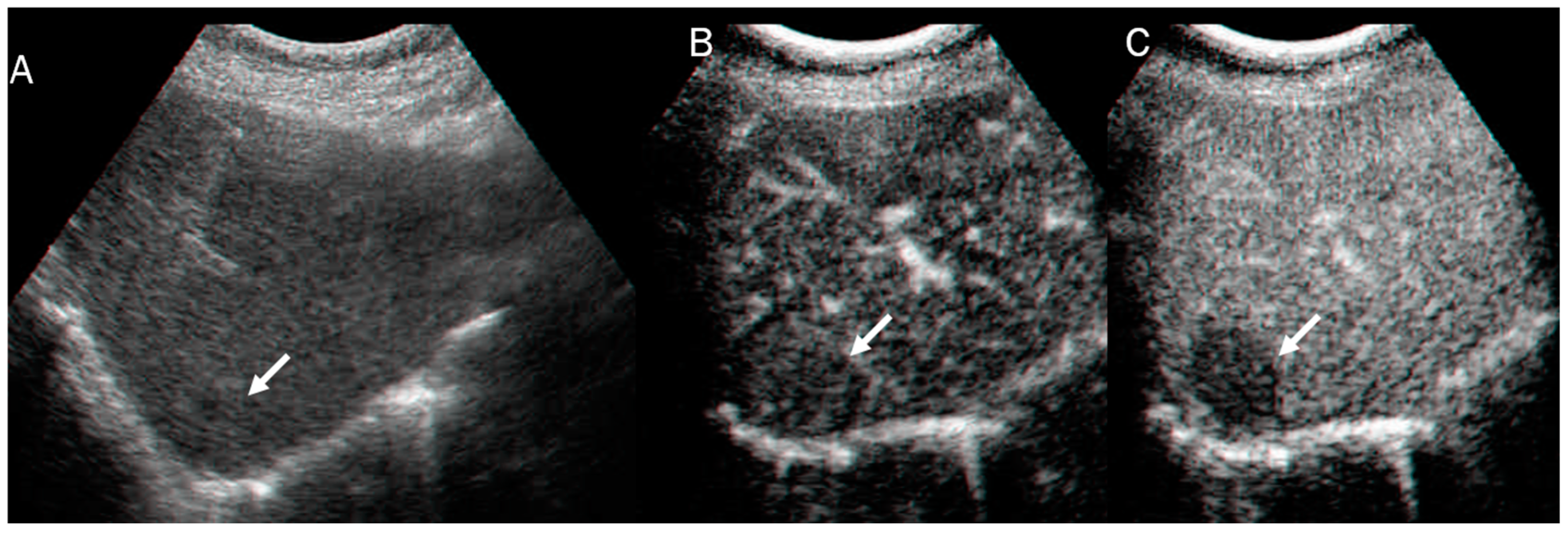
3.1. Ultrasound
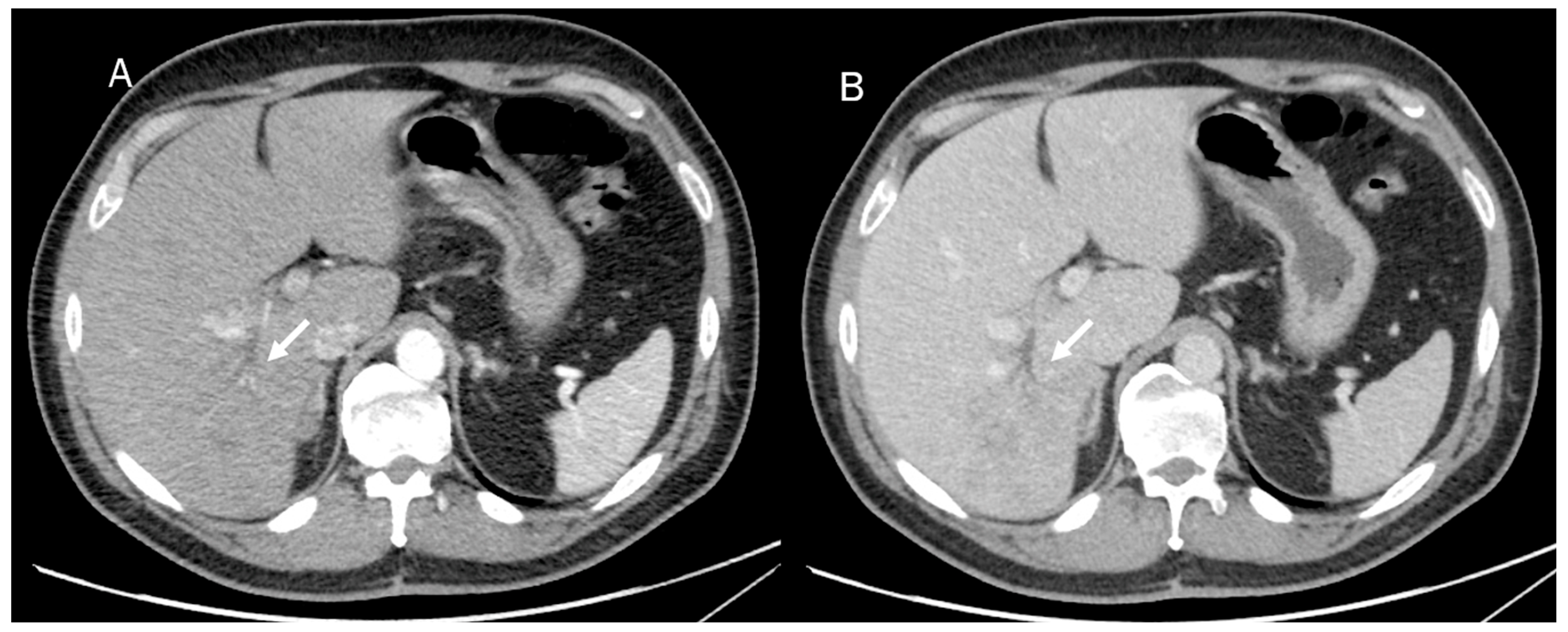
3.2. Computed Tomography
3.3. Magnetic Resonance Imaging
4. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Capuozzo, M.; Santorsola, M.; Landi, L.; Granata, V.; Perri, F.; Celotto, V.; Gualillo, O.; Nasti, G.; Ottaiano, A. Evolution of Treatment in Advanced Cholangiocarcinoma: Old and New towards Precision Oncology. Int. J. Mol. Sci. 2022, 23, 15124. [Google Scholar] [CrossRef] [PubMed]
- Di Benedetto, F.; Magistri, P.; Guerrini, G.P.; Di Sandro, S. Robotic liver partition and portal vein embolization for staged hepatectomy for perihilar cholangiocarcinoma. Updates Surg. 2022, 74, 773–777. [Google Scholar] [CrossRef] [PubMed]
- Saha, S.K.; Zhu, A.X.; Fuchs, C.S.; Brooks, G.A. Forty-Year Trends in Cholangiocarcinoma Incidence in the U.S.: Intrahepatic Disease on the Rise. Oncologist 2016, 21, 594–599. [Google Scholar] [CrossRef] [PubMed]
- Granata, V.; Fusco, R.; Belli, A.; Borzillo, V.; Palumbo, P.; Bruno, F.; Grassi, R.; Ottaiano, A.; Nasti, G.; Pilone, V.; et al. Correction: Conventional, functional and radiomics assessment for intrahepatic cholangiocarcinoma. Infect. Agent Cancer 2022, 17, 22, Erratum in Infect. Agent Cancer 2022, 17, 13. [Google Scholar] [CrossRef] [PubMed]
- Vijgen, S.; Terris, B.; Rubbia-Brandt, L. Pathology of intrahepatic cholangiocarcinoma. Hepatobiliary Surg. Nutr. 2017, 6, 22–34. [Google Scholar] [CrossRef] [PubMed]
- Granata, V.; Grassi, R.; Fusco, R.; Setola, S.V.; Belli, A.; Ottaiano, A.; Nasti, G.; La Porta, M.; Danti, G.; Cappabianca, S.; et al. Intrahepatic cholangiocarcinoma and its differential diagnosis at MRI: How radiologist should assess MR features. Radiol. Med. 2021, 126, 1584–1600. [Google Scholar] [CrossRef]
- Seok, J.Y.; Na, D.C.; Woo, H.G.; Roncalli, M.; Kwon, S.M.; Yoo, J.E.; Ahn, E.Y.; Kim, G.I.; Choi, J.S.; Kim, Y.B.; et al. A fibrous stromal component in hepatocellular carcinoma reveals a cholangiocarcinoma-like gene expression trait and epithelial-mesenchymal transition. Hepatology 2012, 55, 1776–1786. [Google Scholar] [CrossRef]
- Lewis, S.; Besa, C.; Wagner, M.; Jhaveri, K.; Kihira, S.; Zhu, H.; Sadoughi, N.; Fischer, S.; Srivastava, A.; Yee, E.; et al. Prediction of the histopathologic findings of intrahepatic cholangiocarcinoma: Qualitative and quantitative assessment of diffusion-weighted imaging. Eur. Radiol. 2018, 28, 2047–2057. [Google Scholar] [CrossRef]
- Machairas, N.; Kostakis, I.D.; Schizas, D.; Kykalos, S.; Nikiteas, N.; Sotiropoulos, G.C. Meta-analysis of laparoscopic versus open liver resection for intrahepatic cholangiocarcinoma. Updates Surg. 2021, 73, 59–68. [Google Scholar] [CrossRef]
- Marino, R.; Ratti, F.; Catena, M.; Aldrighetti, L. Portal vein arterialization: A possibility in cholangiocarcinomas infiltrating the right hepatic artery? Updates Surg. 2022, 74, 1781–1786. [Google Scholar] [CrossRef]
- Vicini, S.; Bortolotto, C.; Rengo, M.; Ballerini, D.; Bellini, D.; Carbone, I.; Preda, L.; Laghi, A.; Coppola, F.; Faggioni, L. A narrative review on current imaging applications of artificial intelligence and radiomics in oncology: Focus on the three most common cancers. Radiol. Med. 2022, 127, 819–836. [Google Scholar] [CrossRef] [PubMed]
- Mazzella, A.; Bertolaccini, L.; Sedda, G.; Prisciandaro, E.; Loi, M.; Iacono, G.L.; Spaggiari, L. Pneumonectomy and broncho-pleural fistula: Predicting factors and stratification of the risk. Updates Surg. 2022, 74, 1471–1478. [Google Scholar] [CrossRef]
- Xia, D.; Chen, G.; Wu, K.; Yu, M.; Zhang, Z.; Lu, Y.; Xu, L.; Wang, Y. Research progress and hotspot of the artificial intelligence application in the ultrasound during 2011–2021: A bibliometric analysis. Front. Public Health 2022, 10, 990708. [Google Scholar] [CrossRef] [PubMed]
- Scapicchio, C.; Gabelloni, M.; Barucci, A.; Cioni, D.; Saba, L.; Neri, E. A deep look into radiomics. Radiol. Med. 2021, 126, 1296–1311. [Google Scholar] [CrossRef]
- Rocca, A.; Brunese, M.C.; Santone, A.; Avella, P.; Bianco, P.; Scacchi, A.; Scaglione, M.; Bellifemine, F.; Danzi, R.; Varriano, G.; et al. Early Diagnosis of Liver Metastases from Colorectal Cancer through CT Radiomics and Formal Methods: A Pilot Study. J. Clin. Med. 2021, 11, 31. [Google Scholar] [CrossRef]
- Brunese, L.; Mercaldo, F.; Reginelli, A.; Santone, A. Formal methods for prostate cancer Gleason score and treatment prediction using radiomic biomarkers. Magn. Reson. Imaging 2020, 66, 165–175. [Google Scholar] [CrossRef] [PubMed]
- Brunese, L.; Brunese, M.C.; Carbone, M.; Ciccone, V.; Mercaldo, F.; Santone, A. Automatic PI-RADS assignment by means of formal methods. Radiol. Med. 2022, 127, 83–89. [Google Scholar] [CrossRef]
- Santone, A.; Brunese, M.C.; Donnarumma, F.; Guerriero, P.; Mercaldo, F.; Reginelli, A.; Miele, V.; Giovagnoni, A.; Brunese, L. Radiomic features for prostate cancer grade detection through formal verification. Radiol. Med. 2021, 126, 688–697. [Google Scholar] [CrossRef]
- Haghbin, H.; Aziz, M. Artificial intelligence and cholangiocarcinoma: Updates and prospects. World J. Clin. Oncol. 2022, 13, 125–134. [Google Scholar] [CrossRef]
- Yao, F.; Bian, S.; Zhu, D.; Yuan, Y.; Pan, K.; Pan, Z.; Feng, X.; Tang, K.; Yang, Y. Machine learning-based radiomics for multiple primary prostate cancer biological characteristics prediction with 18F-PSMA-1007 PET: Comparison among different volume segmentation thresholds. Radiol. Med. 2022, 127, 1170–1178. [Google Scholar] [CrossRef]
- Cacciamani, G.E.; Sanford, D.I.; Chu, T.N.; Kaneko, M.; De Castro Abreu, A.L.; Duddalwar, V.; Gill, I.S. Is Artificial Intelligence Replacing Our Radiology Stars? Not Yet! Eur. Urol. Open Sci. 2022, 48, 14–16. [Google Scholar] [CrossRef] [PubMed]
- Billet, N.; Grégory, J.; Ronot, M. MRI appearance of combined hepatocellular cholangiocarcinoma. Diagn. Interv. Imaging 2022, 103, 625–626. [Google Scholar] [CrossRef]
- Capretti, G.; Bonifacio, C.; De Palma, C.; Nebbia, M.; Giannitto, C.; Cancian, P.; Laino, M.E.; Balzarini, L.; Papanikolaou, N.; Savevski, V.; et al. A machine learning risk model based on preoperative computed tomography scan to predict postoperative outcomes after pancreatoduodenectomy. Updates Surg. 2022, 74, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Cellina, M.; Pirovano, M.; Ciocca, M.; Gibelli, D.; Floridi, C.; Oliva, G. Radiomic analysis of the optic nerve at the first episode of acute optic neuritis: An indicator of optic nerve pathology and a predictor of visual recovery? Radiol. Med. 2021, 126, 698–706. [Google Scholar] [CrossRef]
- Dong, Z.; Chen, X.; Cheng, Z.; Luo, Y.; He, M.; Chen, T.; Zhang, Z.; Qian, X.; Chen, W. Differential diagnosis of pancreatic cystic neoplasms through a radiomics-assisted system. Front. Oncol. 2022, 12, 941744. [Google Scholar] [CrossRef]
- Marte, G.; Scuderi, V.; Rocca, A.; Surfaro, G.; Migliaccio, C.; Ceriello, A. Laparoscopic splenectomy: A single center experience. Unusual cases and expanded inclusion criteria for laparoscopic approach. Updates Surg. 2013, 65, 115–119. [Google Scholar] [CrossRef]
- Gitto, S.; Bologna, M.; Corino, V.D.A.; Emili, I.; Albano, D.; Messina, C.; Armiraglio, E.; Parafioriti, A.; Luzzati, A.; Mainardi, L.; et al. Diffusion-weighted MRI radiomics of spine bone tumors: Feature stability and machine learning-based classification performance. Radiol. Med. 2022, 127, 518–525. [Google Scholar] [CrossRef] [PubMed]
- Satake, H.; Ishigaki, S.; Ito, R.; Naganawa, S. Radiomics in breast MRI: Current progress toward clinical application in the era of artificial intelligence. Radiol. Med. 2022, 127, 39–56. [Google Scholar] [CrossRef]
- Komici, K.; Bianco, A.; Perrotta, F.; Dello Iacono, A.; Bencivenga, L.; D’Agnano, V.; Rocca, A.; Bianco, A.; Rengo, G.; Guerra, G. Clinical Characteristics, Exercise Capacity and Pulmonary Function in Post-COVID-19 Competitive Athletes. J. Clin. Med. 2021, 10, 3053. [Google Scholar] [CrossRef]
- Amato, B.; Compagna, R.; Rocca, A.; Bianco, T.; Milone, M.; Sivero, L.; Vigliotti, G.; Amato, M.; Danzi, M.; Aprea, G.; et al. Fondaparinux vs warfarin for the treatment of unsuspected pulmonary embolism in cancer patients. Drug Des. Devel. Ther. 2016, 10, 2041–2046. [Google Scholar] [CrossRef]
- Kao, Y.S.; Lin, K.T. A meta-analysis of the diagnostic test accuracy of CT-based radiomics for the prediction of COVID-19 severity. Radiol. Med. 2022, 127, 754–762. [Google Scholar] [CrossRef] [PubMed]
- Giuliani, A.; Avella, P.; Segreto, A.L.; Izzo, M.L.; Buondonno, A.; Coluzzi, M.; Cappuccio, M.; Brunese, M.C.; Vaschetti, R.; Scacchi, A.; et al. Postoperative Outcomes Analysis After Pancreatic Duct Occlusion: A Safe Option to Treat the Pancreatic Stump After Pancreaticoduodenectomy in Low-Volume Centers. Front. Surg. 2021, 8, 804675. [Google Scholar] [CrossRef] [PubMed]
- Grassi, R.; Belfiore, M.P.; Montanelli, A.; Patelli, G.; Urraro, F.; Giacobbe, G.; Fusco, R.; Granata, V.; Petrillo, A.; Sacco, P.; et al. COVID-19 pneumonia: Computer-aided quantification of healthy lung parenchyma, emphysema, ground glass and consolidation on chest computed tomography (CT). Radiol. Med. 2021, 126, 553–560. [Google Scholar] [CrossRef]
- Buondonno, A.; Avella, P.; Cappuccio, M.; Scacchi, A.; Vaschetti, R.; Di Marzo, G.; Maida, P.; Luciani, C.; Amato, B.; Brunese, M.C.; et al. A Hub and Spoke Learning Program in Bariatric Surgery in a Small Region of Italy. Front. Surg. 2022, 9, 855527. [Google Scholar] [CrossRef]
- Brunese, L.; Mercaldo, F.; Reginelli, A.; Santone, A. Explainable Deep Learning for Pulmonary Disease and Coronavirus COVID-19 Detection from X-rays. Comput. Methods Programs Biomed. 2020, 196, 105608. [Google Scholar] [CrossRef] [PubMed]
- Cardobi, N.; Benetti, G.; Cardano, G.; Arena, C.; Micheletto, C.; Cavedon, C.; Montemezzi, S. CT radiomic models to distinguish COVID-19 pneumonia from other interstitial pneumonias. Radiol. Med. 2021, 126, 1037–1043. [Google Scholar] [CrossRef]
- Baeza, S.; Gil, D.; Garcia-Olivé, I.; Salcedo-Pujantell, M.; Deportós, J.; Sanchez, C.; Torres, G.; Moragas, G.; Rosell, A. A novel intelligent radiomic analysis of perfusion SPECT/CT images to optimize pulmonary embolism diagnosis in COVID-19 patients. EJNMMI Phys. 2022, 9, 84. [Google Scholar] [CrossRef]
- Rizzetto, F.; Berta, L.; Zorzi, G.; Cincotta, A.; Travaglini, F.; Artioli, D.; Nerini Molteni, S.; Vismara, C.; Scaglione, F.; Torresin, A.; et al. Diagnostic Performance in Differentiating COVID-19 from Other Viral Pneumonias on CT Imaging: Multi-Reader Analysis Compared with an Artificial Intelligence-Based Model. Tomography 2022, 8, 2815–2827. [Google Scholar] [CrossRef]
- Liu, J.; Wang, C.; Guo, W.; Zeng, P.; Liu, Y.; Lang, N.; Yuan, H. A preliminary study using spinal MRI-based radiomics to predict high-risk cytogenetic abnormalities in multiple myeloma. Radiol. Med. 2021, 126, 1226–1235. [Google Scholar] [CrossRef]
- Mercaldo, F.; Brunese, M.C.; Merolla, F.; Rocca, A.; Zappia, M.; Santone, A. Prostate Gleason Score Detection by Calibrated Machine Learning Classification through Radiomic Features. Appl. Sci. 2022, 12, 11900. [Google Scholar] [CrossRef]
- van der Lubbe, M.F.J.A.; Vaidyanathan, A.; de Wit, M.; van den Burg, E.L.; Postma, A.A.; Bruintjes, T.D.; Bilderbeek-Beckers, M.A.L.; Dammeijer, P.F.M.; Bossche, S.V.; Van Rompaey, V.; et al. A non-invasive, automated diagnosis of Menière’s disease using radiomics and machine learning on conventional magnetic resonance imaging: A multicentric, case-controlled feasibility study. Radiol. Med. 2022, 127, 72–82. [Google Scholar] [CrossRef]
- van der Lubbe, M.F.J.A.; Vaidyanathan, A.; de Wit, M.; van den Burg, E.L.; Postma, A.A.; Bruintjes, T.D.; Bilderbeek-Beckers, M.A.L.; Dammeijer, P.F.M.; Bossche, S.V.; Van Rompaey, V.; et al. Response to the letter to the editor on the article: A non-invasive, automated diagnosis of Menière’s disease using radiomics and machine learning on conventional magnetic resonance imaging-a multicentric, case-controlled feasibility study. Radiol. Med. 2022, 127, 1059–1061. [Google Scholar] [CrossRef]
- Mori, M.; Palumbo, D.; De Cobelli, F.; Fiorino, C. Does radiomics play a role in the diagnosis, staging and re-staging of gastroesophageal junction adenocarcinoma? Updates Surg. 2022, 75, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Javed, S.; Qureshi, T.A.; Gaddam, S.; Wang, L.; Azab, L.; Wachsman, A.M.; Chen, W.; Asadpour, V.; Jeon, C.Y.; Wu, B.; et al. Risk prediction of pancreatic cancer using AI analysis of pancreatic subregions in computed tomography images. Front. Oncol. 2022, 12, 1007990. [Google Scholar] [CrossRef] [PubMed]
- Bianconi, F.; Palumbo, I.; Fravolini, M.L.; Chiari, R.; Minestrini, M.; Brunese, L.; Palumbo, B. Texture Analysis on [18F]FDG PET/CT in Non-Small-Cell Lung Cancer: Correlations Between PET Features, CT Features, and Histological Types. Mol. Imaging Biol. 2019, 21, 1200–1209. [Google Scholar] [CrossRef] [PubMed]
- Chiti, G.; Grazzini, G.; Flammia, F.; Matteuzzi, B.; Tortoli, P.; Bettarini, S.; Pasqualini, E.; Granata, V.; Busoni, S.; Messserini, L.; et al. Gastroenteropancreatic neuroendocrine neoplasms (GEP-NENs): A radiomic model to predict tumor grade. Radiol. Med. 2022, 127, 928–938. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Zhou, B. A review of radiomics and genomics applications in cancers: The way towards precision medicine. Radiat. Oncol. 2022, 17, 217. [Google Scholar] [CrossRef]
- Caruso, D.; Polici, M.; Rinzivillo, M.; Zerunian, M.; Nacci, I.; Marasco, M.; Magi, L.; Tarallo, M.; Gargiulo, S.; Iannicelli, E.; et al. CT-based radiomics for prediction of therapeutic response to Everolimus in metastatic neuroendocrine tumors. Radiol. Med. 2022, 127, 691–701. [Google Scholar] [CrossRef]
- Giannini, V.; Rosati, S.; Defeudis, A.; Balestra, G.; Vassallo, L.; Cappello, G.; Mazzetti, S.; De Mattia, C.; Rizzetto, F.; Torresin, A.; et al. Radiomics predicts response of individual HER2-amplified colorectal cancer liver metastases in patients treated with HER2-targeted therapy. Int. J. Cancer 2020, 147, 3215–3223. [Google Scholar] [CrossRef]
- Gao, W.; Wang, W.; Song, D.; Yang, C.; Zhu, K.; Zeng, M.; Rao, S.X.; Wang, M. A predictive model integrating deep and radiomics features based on gadobenate dimeglumine-enhanced MRI for postoperative early recurrence of hepatocellular carcinoma. Radiol. Med. 2022, 127, 259–271. [Google Scholar] [CrossRef]
- Shi, Y.; Gao, F.; Qi, Y.; Lu, H.; Ai, F.; Hou, Y.; Liu, C.; Xu, Y.; Zhang, X.; Cai, X. Computed tomography-adjusted fistula risk score for predicting clinically relevant postoperative pancreatic fistula after pancreatoduodenectomy: Training and external validation of model upgrade. EBioMedicine 2020, 62, 103096. [Google Scholar] [CrossRef]
- Han, D.; Yu, N.; Yu, Y.; He, T.; Duan, X. Performance of CT radiomics in predicting the overall survival of patients with stage III clear cell renal carcinoma after radical nephrectomy. Radiol. Med. 2022, 127, 837–847. [Google Scholar] [CrossRef]
- Cui, Y.; Li, Z.; Xiang, M.; Han, D.; Yin, Y.; Ma, C. Machine learning models predict overall survival and progression free survival of non-surgical esophageal cancer patients with chemoradiotherapy based on CT image radiomics signatures. Radiat. Oncol. 2022, 17, 212. [Google Scholar] [CrossRef]
- Schlanger, D.; Graur, F.; Popa, C.; Moiș, E.; Al Hajjar, N. The role of artificial intelligence in pancreatic surgery: A systematic review. Updates Surg. 2022, 74, 417–429. [Google Scholar] [CrossRef]
- Wang, F.H.; Zheng, H.L.; Li, J.T.; Li, P.; Zheng, C.H.; Chen, Q.Y.; Huang, C.M.; Xie, J.W. Prediction of recurrence-free survival and adjuvant therapy benefit in patients with gastrointestinal stromal tumors based on radiomics features. Radiol. Med. 2022, 127, 1085–1097. [Google Scholar] [CrossRef] [PubMed]
- Ceccarelli, G.; Costa, G.; De Rosa, M.; Codacci Pisanelli, M.; Frezza, B.; De Prizio, M.; Bravi, I.; Scacchi, A.; Gallo, G.; Amato, B.; et al. Minimally Invasive Approach to Gastric GISTs: Analysis of a Multicenter Robotic and Laparoscopic Experience with Literature Review. Cancers 2021, 13, 4351. [Google Scholar] [CrossRef]
- Dalal, V.; Carmicheal, J.; Dhaliwal, A.; Jain, M.; Kaur, S.; Batra, S.K. Radiomics in stratification of pancreatic cystic lesions: Machine learning in action. Cancer Lett. 2020, 469, 228–237. [Google Scholar] [CrossRef]
- Autorino, R.; Gui, B.; Panza, G.; Boldrini, L.; Cusumano, D.; Russo, L.; Nardangeli, A.; Persiani, S.; Campitelli, M.; Ferrandina, G.; et al. Radiomics-based prediction of two-year clinical outcome in locally advanced cervical cancer patients undergoing neoadjuvant chemoradiotherapy. Radiol. Med. 2022, 127, 498–506. [Google Scholar] [CrossRef] [PubMed]
- Santambrogio, R.; Barabino, M.; D’Alessandro, V.; Iacob, G.; Opocher, E.; Gemma, M.; Zappa, M.A. Micronvasive behaviour of single small hepatocellular carcinoma: Which treatment? Updates Surg. 2021, 73, 1359–1369. [Google Scholar] [CrossRef] [PubMed]
- Cusumano, D.; Meijer, G.; Lenkowicz, J.; Chiloiro, G.; Boldrini, L.; Masciocchi, C.; Dinapoli, N.; Gatta, R.; Casà, C.; Damiani, A.; et al. A field strength independent MR radiomics model to predict pathological complete response in locally advanced rectal cancer. Radiol. Med. 2021, 126, 421–429. [Google Scholar] [CrossRef]
- Chen, S.; Ren, S.; Guo, K.; Daniels, M.J.; Wang, Z.; Chen, R. Preoperative differentiation of serous cystic neoplasms from mucin-producing pancreatic cystic neoplasms using a CT-based radiomics nomogram. Abdom. Radiol. 2021, 46, 2637–2646. [Google Scholar] [CrossRef] [PubMed]
- Wong, P.K.; Chan, I.N.; Yan, H.M.; Gao, S.; Wong, C.H.; Yan, T.; Yao, L.; Hu, Y.; Wang, Z.R.; Yu, H.H. Deep learning based radiomics for gastrointestinal cancer diagnosis and treatment: A minireview. World J. Gastroenterol. 2022, 28, 6363–6379. [Google Scholar] [CrossRef]
- Benedetti, G.; Mori, M.; Panzeri, M.M.; Barbera, M.; Palumbo, D.; Sini, C.; Muffatti, F.; Andreasi, V.; Steidler, S.; Doglioni, C.; et al. CT-derived radiomic features to discriminate histologic characteristics of pancreatic neuroendocrine tumors. Radiol. Med. 2021, 126, 745–760. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Shu, Z.; Zhu, R.H.; Xin, J.Y.; Wu, L.L.; Wang, H.Z.; Chen, J.; Zhang, Z.W.; Luo, H.C.; Li, K.Y. Deep learning-based radiomics based on contrast-enhanced ultrasound predicts early recurrence and survival outcome in hepatocellular carcinoma. World J. Gastrointest. Oncol. 2022, 14, 2380–2392. [Google Scholar] [CrossRef] [PubMed]
- Gregucci, F.; Fiorentino, A.; Mazzola, R.; Ricchetti, F.; Bonaparte, I.; Surgo, A.; Figlia, V.; Carbonara, R.; Caliandro, M.; Ciliberti, M.P.; et al. Radiomic analysis to predict local response in locally advanced pancreatic cancer treated with stereotactic body radiation therapy. Radiol. Med. 2022, 127, 100–107. [Google Scholar] [CrossRef]
- Sim, K.C.; Kim, M.J.; Cho, Y.; Kim, H.J.; Park, B.J.; Sung, D.J.; Han, N.Y.; Han, Y.E.; Kim, T.H.; Lee, Y.J. Radiomics Analysis of Magnetic Resonance Proton Density Fat Fraction for the Diagnosis of Hepatic Steatosis in Patients with Suspected Non-Alcoholic Fatty Liver Disease. J. Korean Med. Sci. 2022, 37, e339. [Google Scholar] [CrossRef]
- Kotowski, K.; Kucharski, D.; Machura, B.; Adamski, S.; Gutierrez Becker, B.; Krason, A.; Zarudzki, L.; Tessier, J.; Nalepa, J. Detecting liver cirrhosis in computed tomography scans using clinically-inspired and radiomic features. Comput. Biol. Med. 2022, 152, 106378. [Google Scholar] [CrossRef]
- Li, B.; Tai, D.I.; Yan, K.; Chen, Y.C.; Chen, C.J.; Huang, S.F.; Hsu, T.H.; Yu, W.T.; Xiao, J.; Le, L.; et al. Accurate and generalizable quantitative scoring of liver steatosis from ultrasound images via scalable deep learning. World J. Gastroenterol. 2022, 28, 2494–2508. [Google Scholar] [CrossRef]
- Romeo, V.; Verde, F.; Sarno, L.; Migliorini, S.; Petretta, M.; Mainenti, P.P.; D’Armiento, M.; Guida, M.; Brunetti, A.; Maurea, S. Prediction of placenta accreta spectrum in patients with placenta previa using clinical risk factors, ultrasound and magnetic resonance imaging findings. Radiol. Med. 2021, 126, 1216–1225. [Google Scholar] [CrossRef]
- Jeon, S.K.; Lee, J.M.; Joo, I.; Yoon, J.H. Assessment of the inter-platform reproducibility of ultrasound attenuation examination in nonalcoholic fatty liver disease. Ultrasonography 2022, 41, 355–364. [Google Scholar] [CrossRef]
- Mao, Y.; Mu, J.; Zhao, J.; Yang, F.; Zhao, L. The comparative study of color doppler flow imaging, superb microvascular imaging, contrast-enhanced ultrasound micro flow imaging in blood flow analysis of solid renal mass. Cancer Imaging 2022, 22, 21. [Google Scholar] [CrossRef]
- Ceccarelli, G.; Andolfi, E.; Fontani, A.; Calise, F.; Rocca, A.; Giuliani, A. Robot-assisted liver surgery in a general surgery unit with a “Referral Centre Hub&Spoke Learning Program”. Early outcomes after our first 70 consecutive patients. Minerva Chir. 2018, 73, 460–468. [Google Scholar] [CrossRef]
- Di Serafino, M.; Vallone, G. The role of point of care ultrasound in radiology department: Update and prospective. A statement of Italian college ultrasound. Radiol. Med. 2021, 126, 636–641. [Google Scholar] [CrossRef]
- Aprea, G.; Rocca, A.; Salzano, A.; Sivero, L.; Scarpaleggia, M.; Ocelli, P.; Amato, M.; Bianco, T.; Serra, R.; Amato, B. Laparoscopic single site (LESS) and classic video-laparoscopic cholecystectomy in the elderly: A single centre experience. Int. J. Surg. 2016, 33 (Suppl. 1), S1–S3. [Google Scholar] [CrossRef] [PubMed]
- Barton, A. Considering the uncompliant patient: A four-step approach. Br. J. Nurs. 2017, 26, S12. [Google Scholar] [CrossRef]
- Rocca, A.; Brunese, M.C.; Cappuccio, M.; Scacchi, A.; Martucci, G.; Buondonno, A.; Perrotta, F.M.; Quarto, G.; Avella, P.; Amato, B. Impact of Physical Activity on Disability Risk in Elderly Patients Hospitalized for Mild Acute Diverticulitis and Diverticular Bleeding Undergone Conservative Management. Medicina 2021, 57, 360. [Google Scholar] [CrossRef]
- Ruan, S.M.; Huang, H.; Cheng, M.Q.; Lin, M.X.; Hu, H.T.; Huang, Y.; Li, M.D.; Lu, M.D.; Wang, W. Shear-wave elastography combined with contrast-enhanced ultrasound algorithm for noninvasive characterization of focal liver lesions. Radiol. Med. 2022. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Yin, S.; Zhao, L.; Zhang, X.; Li, M.; Ding, J.; Yan, K.; Jing, X. CEUS and CT/MRI LI-RADS in Association with Serum Biomarkers for Differentiation of Combined Hepatocellular-Cholangiocarcinoma From Hepatocellular Carcinoma. Front. Oncol. 2022, 12, 897090. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.T.; Wang, W.; Chen, L.D.; Ruan, S.M.; Chen, S.L.; Li, X.; Lu, M.D.; Xie, X.Y.; Kuang, M. Artificial intelligence assists identifying malignant versus benign liver lesions using contrast-enhanced ultrasound. J. Gastroenterol. Hepatol. 2021, 36, 2875–2883. [Google Scholar] [CrossRef]
- Nakanuma, Y.; Sripa, B.; Vatanasapt, V.; Leong, A.S.Y.; Ponchon, T.; Ishak, K.G. Intrahepatic cholangiocarcinoma. In World Health Organization Classification of Tumours Pathology and Genetics of Tumours of the Digestive System; WHO: Geneva, Switzerland, 2000; pp. 173–180. [Google Scholar]
- Takakura, K.; Kajihara, M.; Iwasaki, T.; Ide, D.; Miyazaki, T.; Arai, Y.; Saruta, M.; Arihiro, S.; Matsuoka, M.; Koido, S.; et al. Unusual images of mass-forming intrahepatic cholangiocarcinoma. Case Rep. Gastroenterol. 2013, 7, 414–419. [Google Scholar] [CrossRef] [PubMed]
- Vidili, G.; Arru, M.; Solinas, G.; Calvisi, D.F.; Meloni, P.; Sauchella, A.; Turilli, D.; Fabio, C.; Cossu, A.; Madeddu, G.; et al. Contrast-enhanced ultrasound Liver Imaging Reporting and Data System: Lights and shadows in hepatocellular carcinoma and cholangiocellular carcinoma diagnosis. World J. Gastroenterol. 2022, 28, 3488–3502. [Google Scholar] [CrossRef]
- Zeng, D.; Xu, M.; Liang, J.Y.; Cheng, M.Q.; Huang, H.; Pan, J.M.; Huang, Y.; Tong, W.J.; Xie, X.Y.; Lu, M.D.; et al. Using new criteria to improve the differentiation between HCC and non-HCC malignancies: Clinical practice and discussion in CEUS LI-RADS 2017. Radiol. Med. 2022, 127, 1–10. [Google Scholar] [CrossRef]
- Karmazanovsky, G.; Gruzdev, I.; Tikhonova, V.; Kondratyev, E.; Revishvili, A. Computed tomography-based radiomics approach in pancreatic tumors characterization. Radiol. Med. 2021, 126, 1388–1395. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL clinical practice guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed]
- Argalia, G.; Ventura, C.; Tosi, N.; Campioni, D.; Tagliati, C.; Tufillaro, M.; Cucco, M.; Svegliati Baroni, G.; Giovagnoni, A. Comparison of point shear wave elastography and transient elastography in the evaluation of patients with NAFLD. Radiol. Med. 2022, 127, 571–576. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Zhu, Y.; Chen, K.; Wang, H.; Zhang, W.; Bao, J.; Wang, W. Differentiation between hepatocellular carcinoma and intrahepatic cholangiocarcinoma using contrast-enhanced ultrasound: A systematic review and meta-analysis. Clin. Hemorheol. Microcirc. 2021, 79, 293–309. [Google Scholar] [CrossRef]
- Gurgitano, M.; Angileri, S.A.; Rodà, G.M.; Liguori, A.; Pandolfi, M.; Ierardi, A.M.; Wood, B.J.; Carrafiello, G. Interventional Radiology ex-machina: Impact of Artificial Intelligence on practice. Radiol. Med. 2021, 126, 998–1006. [Google Scholar] [CrossRef] [PubMed]
- Peng, Y.; Lin, P.; Wu, L.; Wan, D.; Zhao, Y.; Liang, L.; Ma, X.; Qin, H.; Liu, Y.; Li, X.; et al. Ultrasound-Based Radiomics Analysis for Preoperatively Predicting Different Histopathological Subtypes of Primary Liver Cancer. Front. Oncol. 2020, 10, 1646. [Google Scholar] [CrossRef] [PubMed]
- Ren, S.; Li, Q.; Liu, S.; Qi, Q.; Duan, S.; Mao, B.; Li, X.; Wu, Y.; Zhang, L. Clinical Value of Machine Learning-Based Ultrasomics in Preoperative Differentiation Between Hepatocellular Carcinoma and Intrahepatic Cholangiocarcinoma: A Multicenter Study. Front. Oncol. 2021, 11, 749137. [Google Scholar] [CrossRef]
- Li, C.Q.; Zheng, X.; Guo, H.L.; Cheng, M.Q.; Huang, Y.; Xie, X.Y.; Lu, M.D.; Kuang, M.; Wang, W.; Chen, L.D. Differentiation between combined hepatocellular carcinoma and hepatocellular carcinoma: Comparison of diagnostic performance between ultrasomics-based model and CEUS LI-RADS v2017. BMC Med. Imaging 2022, 22, 36, Erratum in BMC Med. Imaging. 2022, 22, 57. [Google Scholar] [CrossRef]
- Barabino, M.; Gurgitano, M.; Fochesato, C.; Angileri, S.A.; Franceschelli, G.; Santambrogio, R.; Mariani, N.M.; Opocher, E.; Carrafiello, G. LI-RADS to categorize liver nodules in patients at risk of HCC: Tool or a gadget in daily practice? Radiol. Med. 2021, 126, 5–13. [Google Scholar] [CrossRef]
- Peng, Y.T.; Zhou, C.Y.; Lin, P.; Wen, D.Y.; Wang, X.D.; Zhong, X.Z.; Pan, D.H.; Que, Q.; Li, X.; Chen, L.; et al. Preoperative Ultrasound Radiomics Signatures for Noninvasive Evaluation of Biological Characteristics of Intrahepatic Cholangiocarcinoma. Acad. Radiol. 2020, 27, 785–797. [Google Scholar] [CrossRef]
- Argalia, G.; Tarantino, G.; Ventura, C.; Campioni, D.; Tagliati, C.; Guardati, P.; Kostandini, A.; Marzioni, M.; Giuseppetti, G.M.; Giovagnoni, A. Shear wave elastography and transient elastography in HCV patients after direct-acting antivirals. Radiol. Med. 2021, 126, 894–899. [Google Scholar] [CrossRef] [PubMed]
- Wen, Q.; Wang, Z.; Traverso, A.; Liu, Y.; Xu, R.; Feng, Y.; Qian, L. A radiomics nomogram for the ultrasound-based evaluation of central cervical lymph node metastasis in papillary thyroid carcinoma. Front. Endocrinol. 2022, 13, 1064434. [Google Scholar] [CrossRef]
- Yang, R.; Wu, J.; Sun, L.; Lai, S.; Xu, Y.; Liu, X.; Ma, Y.; Zhen, X. Radiomics of small renal masses on multiphasic CT: Accuracy of machine learning-based classification models for the differentiation of renal cell carcinoma and angiomyolipoma without visible fat. Eur Radiol. 2020, 30, 1254–1263. [Google Scholar] [CrossRef]
- Celletti, I.; Fresilli, D.; De Vito, C.; Bononi, M.; Cardaccio, S.; Cozzolino, A.; Durante, C.; Grani, G.; Grimaldi, G.; Isidori, A.M.; et al. TIRADS, SRE and SWE in INDETERMINATE thyroid nodule characterization: Which has better diagnostic performance? Radiol. Med. 2021, 126, 1189–1200. [Google Scholar] [CrossRef] [PubMed]
- Lu, W.; Zhang, D.; Zhang, Y.; Qian, X.; Qian, C.; Wei, Y.; Xia, Z.; Ding, W.; Ni, X. Ultrasound Radiomics Nomogram to Diagnose Sub-Centimeter Thyroid Nodules Based on ACR TI-RADS. Cancers 2022, 14, 4826. [Google Scholar] [CrossRef] [PubMed]
- Soyer Güldoğan, E.; Ergun, O.; Taşkın Türkmenoğlu, T.; Yılmaz, K.B.; Akdağ, T.; Özbal Güneş, S.; Durmaz, H.A.; Hekimoğlu, B. The impact of TI-RADS in detecting thyroid malignancies: A prospective study. Radiol. Med. 2021, 126, 1335–1344. [Google Scholar] [CrossRef]
- Qin, H.; Que, Q.; Lin, P.; Li, X.; Wang, X.R.; He, Y.; Chen, J.Q.; Yang, H. Magnetic resonance imaging (MRI) radiomics of papillary thyroid cancer (PTC): A comparison of predictive performance of multiple classifiers modeling to identify cervical lymph node metastases before surgery. Radiol. Med. 2021, 126, 1312–1327. [Google Scholar] [CrossRef]
- Zhang, L.; Sun, K.; Shi, L.; Qiu, J.; Wang, X.; Wang, S. Ultrasound Image-Based Deep Features and Radiomics for the Discrimination of Small Fat-Poor Angiomyolipoma and Small Renal Cell Carcinoma. Ultrasound Med. Biol. 2023, 49, 560–568. [Google Scholar] [CrossRef]
- Cui, H.; Zhang, D.; Peng, F.; Kong, H.; Guo, Q.; Wu, T.; Wen, X.; Zhang, L.; Tian, J. Identifying ultrasound features of positive expression of Ki67 and P53 in breast cancer using radiomics. Asia Pac. J. Clin. Oncol. 2021, 17, e176–e184. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.G.; Xu, F.J.; Agyekum, E.A.; Xiang, H.; Wang, Y.D.; Zhang, J.; Sun, H.; Zhang, G.L.; Bo, X.S.; Lv, W.Z.; et al. Radiomic Model for Determining the Value of Elasticity and Grayscale Ultrasound Diagnoses for Predicting BRAFV600E Mutations in Papillary Thyroid Carcinoma. Front. Endocrinol. 2022, 13, 872153. [Google Scholar] [CrossRef] [PubMed]
- Xu, M.L.; Zeng, S.E.; Li, F.; Cui, X.W.; Liu, G.F. Preoperative prediction of lymphovascular invasion in patients with T1 breast invasive ductal carcinoma based on radiomics nomogram using grayscale ultrasound. Front. Oncol. 2022, 12, 1071677. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Wu, J.; Wang, Y.; Jin, Y. Development and Validation of an Ultrasound-Based Radiomics Nomogram for Identifying HER2 Status in Patients with Breast Carcinoma. Diagnostics 2022, 12, 3130. [Google Scholar] [CrossRef]
- Jiang, M.; Zhang, D.; Tang, S.C.; Luo, X.M.; Chuan, Z.R.; Lv, W.Z.; Jiang, F.; Ni, X.J.; Cui, X.W.; Dietrich, C.F. Deep learning with convolutional neural network in the assessment of breast cancer molecular subtypes based on US images: A multicenter retrospective study. Eur. Radiol. 2021, 31, 3673–3682. [Google Scholar] [CrossRef]
- Gu, J.; Jiang, T. Ultrasound radiomics in personalized breast management: Current status and future prospects. Front. Oncol. 2022, 12, 963612. [Google Scholar] [CrossRef]
- Rimola, J.; Forner, A.; Reig, M.; Vilana, R.; de Lope, C.R.; Ayuso, C.; Bruix, J. Cholangiocarcinoma in cirrhosis: Absence of contrast washout in delayed phases by magnetic resonance imaging avoids misdiagnosis of hepatocel- lular carcinoma. Hepatology 2009, 50, 791–798. [Google Scholar] [CrossRef]
- Chen, Y.; Pan, Y.; Shen, K.R.; Zhu, X.L.; Lu, C.Y.; Li, Q.H.; Han, S.G.; Fu, Y.B.; Xu, X.F.; Yu, R.S. Contrast-enhanced multiple-phase imaging features of intrahepatic mass-forming cholangiocarcinoma and hepatocellular carcinoma with cirrhosis: A comparative study. Oncol. Lett. 2017, 14, 4213–4219. [Google Scholar] [CrossRef]
- Weber, S.M.; Ribero, D.; O’Reilly, E.M.; Kokudo, N.; Miyazaki, M.; Pawlik, T.M. Intrahepatic cholangiocarcinoma: Expert consensus statement. HPB 2015, 17, 669–680. [Google Scholar] [CrossRef]
- Fábrega-Foster, K.; Ghasabeh, M.A.; Pawlik, T.M.; Kamel, I.R. Multimodality imaging of intrahepatic cholangiocarcinoma. Hepatobiliary Surg. Nutr. 2017, 6, 67–78. [Google Scholar] [CrossRef]
- Marrero, J.A.; Kulik, L.M.; Sirlin, C.B.; Zhu, A.X.; Finn, R.S.; Abecassis, M.M.; Roberts, L.R.; Heimbach, J.K. Diagnosis, staging, and management of hepatocellular carcinoma: 2018 practice guid- ance by the American association for the study of liver diseases. Hepatology 2018, 68, 723–750. [Google Scholar] [CrossRef] [PubMed]
- Cicero, G.; Mazziotti, S.; Silipigni, S.; Blandino, A.; Cantisani, V.; Pergolizzi, S.; D’Angelo, T.; Stagno, A.; Maimone, S.; Squadrito, G.; et al. Dual-energy CT quantification of fractional extracellular space in cirrhotic patients: Comparison between early and delayed equilibrium phases and correlation with oesophageal varices. Radiol. Med. 2021, 126, 761–767. [Google Scholar] [CrossRef] [PubMed]
- Scialpi, M.; Palumbo, B.; Pierotti, L.; Gravante, S.; Piunno, A.; Rebonato, A.; D’Andrea, A.; Reginelli, A.; Piscioli, I.; Brunese, L.; et al. Detection and characterization of focal liver lesions by split-bolus multidetector-row CT: Diagnostic accuracy and radiation dose in oncologic patients. Anticancer Res. 2014, 34, 4335–4344. [Google Scholar] [PubMed]
- Mahmoudi, S.; Bernatz, S.; Althoff, F.C.; Koch, V.; Grünewald, L.D.; Scholtz, J.E.; Walter, D.; Zeuzem, S.; Wild, P.J.; Vogl, T.J.; et al. Dual-energy CT based material decomposition to differentiate intrahepatic cholangiocarcinoma from hepatocellular carcinoma. Eur. J. Radiol. 2022, 156, 110556. [Google Scholar] [CrossRef]
- Renzulli, M.; Brandi, N.; Argalia, G.; Brocchi, S.; Farolfi, A.; Fanti, S.; Golfieri, R. Morphological, dynamic and functional characteristics of liver pseudolesions and benign lesions. Radiol. Med. 2022, 127, 129–144. [Google Scholar] [CrossRef]
- Yoon, J.; Park, S.H.; Ahn, S.J.; Shim, Y.S. Atypical Manifestation of Primary Hepatocellular Carcinoma and Hepatic Malignancy Mimicking Lesions. J. Korean Soc. Radiol. 2022, 83, 808–829. [Google Scholar] [CrossRef]
- Nakamura, Y.; Higaki, T.; Honda, Y.; Tatsugami, F.; Tani, C.; Fukumoto, W.; Narita, K.; Kondo, S.; Akagi, M.; Awai, K. Advanced CT techniques for assessing hepatocellular carcinoma. Radiol. Med. 2021, 126, 925–935. [Google Scholar] [CrossRef]
- Viganò, L.; Lleo, A.; Muglia, R.; Gennaro, N.; Samà, L.; Colapietro, F.; Roncalli, M.; Aghemo, A.; Chiti, A.; Di Tommaso, L.; et al. Intrahepatic cholangiocellular carcinoma with radiological enhancement patterns mimicking hepatocellular carcinoma. Updates Surg. 2020, 72, 413–421. [Google Scholar] [CrossRef]
- Fusco, R.; Setola, S.V.; Raiano, N.; Granata, V.; Cerciello, V.; Pecori, B.; Petrillo, A. Analysis of a monocentric computed tomography dosimetric database using a radiation dose index monitoring software: Dose levels and alerts before and after the implementation of the adaptive statistical iterative reconstruction on CT images. Radiol. Med. 2022, 127, 733–742. [Google Scholar] [CrossRef] [PubMed]
- Scialpi, M.; Moschini, T.O.; De Filippis, G. PET/contrast-enhanced CT in oncology: “to do, or not to do, that is the question”. Radiol. Med. 2022, 127, 925–927. [Google Scholar] [CrossRef]
- Rocca, A.; Calise, F.; Marino, G.; Montagnani, S.; Cinelli, M.; Amato, B.; Guerra, G. Primary giant hepatic neuroendocrine carcinoma: A case report. Int. J. Surg. 2014, 12 (Suppl. 1), S218–S221. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Wang, Y.; Deng, L.; Yu, H.; Chen, K.; Bao, W.; Chen, K.; Chen, G. Development and validation of a nomogram for predicting the cancer-specific survival of fibrolamellar hepatocellular carcinoma patients. Updates Surg. 2022, 74, 1589–1599. [Google Scholar] [CrossRef] [PubMed]
- Danti, G.; Flammia, F.; Matteuzzi, B.; Cozzi, D.; Berti, V.; Grazzini, G.; Pradella, S.; Recchia, L.; Brunese, L.; Miele, V. Gastrointestinal neuroendocrine neoplasms (GI-NENs): Hot topics in morphological, functional, and prognostic imaging. Radiol. Med. 2021, 126, 1497–1507. [Google Scholar] [CrossRef] [PubMed]
- Nakai, H.; Fujimoto, K.; Yamashita, R.; Sato, T.; Someya, Y.; Taura, K.; Isoda, H.; Nakamoto, Y. Convolutional neural network for classifying primary liver cancer based on triple-phase CT and tumor marker information: A pilot study. Jpn. J. Radiol. 2021, 39, 690–702. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Huang, Z.; Cao, L.; Zhang, Z.; Wei, Y.; Zhang, X.; Song, B. Differentiation combined hepatocellular and cholangiocarcinoma from intrahepatic cholangiocarcinoma based on radiomics machine learning. Ann. Transl. Med. 2020, 8, 119. [Google Scholar] [CrossRef]
- Liu, X.; Khalvati, F.; Namdar, K.; Fischer, S.; Lewis, S.; Taouli, B.; Haider, M.A.; Jhaveri, K.S. Can machine learning radiomics provide pre-operative differentiation of combined hepatocellular cholangiocarcinoma from hepatocellular carcinoma and cholangiocarcinoma to inform optimal treatment planning? Eur. Radiol. 2021, 31, 244–255. [Google Scholar] [CrossRef]
- Wan, Y.; Yang, P.; Xu, L.; Yang, J.; Luo, C.; Wang, J.; Chen, F.; Wu, Y.; Lu, Y.; Ruan, D.; et al. Radiomics analysis combining unsupervised learning and handcrafted features: A multiple-disease study. Med. Phys. 2021, 48, 7003–7015. [Google Scholar] [CrossRef]
- Xu, X.; Mao, Y.; Tang, Y.; Liu, Y.; Xue, C.; Yue, Q.; Liu, Q.; Wang, J.; Yin, Y. Classification of Hepatocellular Carcinoma and Intrahepatic Cholangiocarcinoma Based on Radiomic Analysis. Comput. Math. Methods Med. 2022, 2022, 5334095. [Google Scholar] [CrossRef]
- Matake, K.; Yoshimitsu, K.; Kumazawa, S.; Higashida, Y.; Irie, H.; Asayama, Y.; Nakayama, T.; Kakihara, D.; Katsuragawa, S.; Doi, K.; et al. Usefulness of artificial neural network for differential diagnosis of hepatic masses on CT images. Acad. Radiol. 2006, 13, 951–962. [Google Scholar] [CrossRef]
- Zhou, J.; Wang, W.; Lei, B.; Ge, W.; Huang, Y.; Zhang, L.; Yan, Y.; Zhou, D.; Ding, Y.; Wu, J.; et al. Automatic Detection and Classification of Focal Liver Lesions Based on Deep Convolutional Neural Networks: A Preliminary Study. Front. Oncol. 2021, 10, 581210. [Google Scholar] [CrossRef]
- Yasaka, K.; Akai, H.; Abe, O.; Kiryu, S. Deep Learning with Convolutional Neural Network for Differentiation of Liver Masses at Dynamic Contrast-enhanced CT: A Preliminary Study. Radiology 2018, 286, 887–896. [Google Scholar] [CrossRef]
- Xu, H.; Zou, X.; Zhao, Y.; Zhang, T.; Tang, Y.; Zheng, A.; Zhou, X.; Ma, X. Differentiation of Intrahepatic Cholangiocarcinoma and Hepatic Lymphoma Based on Radiomics and Machine Learning in Contrast-Enhanced Computer Tomography. Technol. Cancer Res. Treat. 2021, 20, 15330338211039125. [Google Scholar] [CrossRef] [PubMed]
- Lorio, E.; Patel, P.; Rosenkranz, L.; Patel, S.; Sayana, H. Management of Hepatolithiasis: Review of the Literature. Curr. Gastroenterol. Rep. 2020, 22, 30. [Google Scholar] [CrossRef] [PubMed]
- Shen, X.; Zhao, H.; Jin, X.; Chen, J.; Yu, Z.; Ramen, K.; Zheng, X.; Wu, X.; Shan, Y.; Bai, J.; et al. Development and validation of a machine learning-based nomogram for prediction of intrahepatic cholangiocarcinoma in patients with intrahepatic lithiasis. Hepatobiliary Surg. Nutr. 2021, 10, 749–765. [Google Scholar] [CrossRef]
- Xue, B.; Wu, S.; Zheng, M.; Jiang, H.; Chen, J.; Jiang, Z.; Tian, T.; Tu, Y.; Zhao, H.; Shen, X.; et al. Development and Validation of a Radiomic-Based Model for Prediction of Intrahepatic Cholangiocarcinoma in Patients With Intrahepatic Lithiasis Complicated by Imagologically Diagnosed Mass. Front. Oncol. 2021, 10, 598253. [Google Scholar] [CrossRef]
- Lu, Q.; Yang, J.; Wang, P.; Liu, J.; Fan, Y.; Fang, C. Digital Surgical Diagnosis and Management of Hepatolithiasis. In Biliary Tract Surgery; Fang, C., Lau, W.Y., Eds.; Springer: Singapore, 2021. [Google Scholar] [CrossRef]
- Mansour, J.C.; Aloia, T.A.; Crane, C.H.; Heimbach, J.K.; Nagino, M.; Vauthey, J.N. Hilar cholangiocarcinoma: Expert consensus statement. HPB 2015, 17, 691–699. [Google Scholar] [CrossRef]
- Suzuki, Y.; Mori, T.; Momose, H.; Matsuki, R.; Kogure, M.; Abe, N.; Isayama, H.; Tazuma, S.; Tanaka, A.; Takikawa, H.; et al. Predictive factors for subsequent intrahepatic cholangiocarcinoma associated with hepatolithiasis: Japanese National Cohort Study for 18 years. J. Gastroenterol. 2022, 57, 387–395. [Google Scholar] [CrossRef] [PubMed]
- Ji, G.W.; Zhu, F.P.; Zhang, Y.D.; Liu, X.S.; Wu, F.Y.; Wang, K.; Xia, Y.X.; Zhang, Y.D.; Jiang, W.J.; Li, X.C.; et al. A radiomics approach to predict lymph node metastasis and clinical outcome of intrahepatic cholangiocarcinoma. Eur Radiol. 2019, 29, 3725–3735. [Google Scholar] [CrossRef]
- Xue, B.; Wu, S.; Zhang, M.; Hong, J.; Liu, B.; Xu, N.; Zeng, Q.; Tang, K.; Zheng, X. A radiomic-based model of different contrast-enhanced CT phase for differentiate intrahepatic cholangiocarcinoma from inflammatory mass with hepatolithiasis. Abdom. Radiol. 2021, 46, 3835–3844. [Google Scholar] [CrossRef]
- Uenishi, T.; Hamba, H.; Takemura, S.; Oba, K.; Ogawa, M.; Yamamoto, T.; Tanaka, S.; Kubo, S. Outcomes of hepatic resection for hepatolithiasis. Am. J. Surg. 2009, 198, 199–202. [Google Scholar] [CrossRef]
- Su, C.H.; Shyr, Y.M.; Lui, W.Y.; P’Eng, F.K. Hepatolithiasis associated with cholangiocarcinoma. Br. J. Surg. 1997, 84, 969–973. [Google Scholar] [CrossRef] [PubMed]
- Bozkurt, M.; Eldem, G.; Bozbulut, U.B.; Bozkurt, M.F.; Kılıçkap, S.; Peynircioğlu, B.; Çil, B.; Lay Ergün, E.; Volkan-Salanci, B. Factors affecting the response to Y-90 microsphere therapy in the cholangiocarcinoma patients. Radiol. Med. 2021, 126, 323–333. [Google Scholar] [CrossRef] [PubMed]
- Jolissaint, J.S.; Wang, T.; Soares, K.C.; Chou, J.F.; Gönen, M.; Pak, L.M.; Boerner, T.; Do, R.K.G.; Balachandran, V.P.; D’Angelica, M.I.; et al. Machine learning radiomics can predict early liver recurrence after resection of intrahepatic cholangiocarcinoma. HPB 2022, 24, 1341–1350. [Google Scholar] [CrossRef] [PubMed]
- De Robertis, R.; Geraci, L.; Tomaiuolo, L.; Bortoli, L.; Beleù, A.; Malleo, G.; D’Onofrio, M. Liver metastases in pancreatic ductal adenocarcinoma: A predictive model based on CT texture analysis. Radiol. Med. 2022, 127, 1079–1084. [Google Scholar] [CrossRef]
- Zhu, Y.; Mao, Y.; Chen, J.; Qiu, Y.; Guan, Y.; Wang, Z.; He, J. Radiomics-based model for predicting early recurrence of intrahepatic mass-forming cholangiocarcinoma after curative tumor resection. Sci. Rep. 2021, 11, 18347. [Google Scholar] [CrossRef]
- Wakiya, T.; Ishido, K.; Kimura, N.; Nagase, H.; Kanda, T.; Ichiyama, S.; Soma, K.; Matsuzaka, M.; Sasaki, Y.; Kubota, S.; et al. CT-based deep learning enables early postoperative recurrence prediction for intrahepatic cholangiocarcinoma. Sci. Rep. 2022, 12, 8428. [Google Scholar] [CrossRef]
- Hao, X.; Liu, B.; Hu, X.; Wei, J.; Han, Y.; Liu, X.; Chen, Z.; Li, J.; Bai, J.; Chen, Y.; et al. A Radiomics-based Approach for Predicting Early Recurrence in Intrahepatic Cholangiocarcinoma after Surgical Resection: A Multicenter Study. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2021, 2021, 3659–3662. [Google Scholar] [CrossRef] [PubMed]
- Chu, H.; Liu, Z.; Liang, W.; Zhou, Q.; Zhang, Y.; Lei, K.; Tang, M.; Cao, Y.; Chen, S.; Peng, S.; et al. Radiomics using CT images for preoperative prediction of futile resection in intrahepatic cholangiocarcinoma. Eur. Radiol. 2021, 31, 2368–2376. [Google Scholar] [CrossRef]
- Granata, V.; Fusco, R.; De Muzio, F.; Cutolo, C.; Setola, S.V.; Grassi, R.; Grassi, F.; Ottaiano, A.; Nasti, G.; Tatangelo, F.; et al. Radiomics textural features by MR imaging to assess clinical outcomes following liver resection in colorectal liver metastases. Radiol. Med. 2022, 127, 461–470. [Google Scholar] [CrossRef]
- Zhang, S.; Huang, S.; He, W.; Wei, J.; Huo, L.; Jia, N.; Lin, J.; Tang, Z.; Yuan, Y.; Tian, J.; et al. Radiomics-Based Preoperative Prediction of Lymph Node Metastasis in Intrahepatic Cholangiocarcinoma Using Contrast-Enhanced Computed Tomography. Ann. Surg. Oncol. 2022, 29, 6786–6799. [Google Scholar] [CrossRef]
- Xiang, F.; Wei, S.; Liu, X.; Liang, X.; Yang, L.; Yan, S. Radiomics Analysis of Contrast-Enhanced CT for the Preoperative Prediction of Microvascular Invasion in Mass-Forming Intrahepatic Cholangiocarcinoma. Front. Oncol. 2021, 11, 774117. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Chen, J.; Kong, W.; Mao, L.; Kong, W.; Zhou, Q.; Zhou, Z.; Zhu, B.; Wang, Z.; He, J.; et al. Predicting idh mutation status of intrahepatic cholangiocarcinomas based on contrast-enhanced CT features. Eur. Radiol. 2018, 28, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Mao, Y.; Chen, J.; Qiu, Y.; Guan, Y.; Wang, Z.; He, J. Value of contrast-enhanced CT texture analysis in predicting IDH mutation status of intrahepatic cholangiocarcinoma. Sci. Rep. 2021, 11, 6933. [Google Scholar] [CrossRef]
- Zhang, Y.; Esmail, A.; Mazzaferro, V.; Abdelrahim, M. Newest Therapies for Cholangiocarcinoma: An Updated Overview of Approved Treatments with Transplant Oncology Vision. Cancers 2022, 14, 5074. [Google Scholar] [CrossRef]
- Gruttadauria, S.; Barbara, M.; Liotta, R. Liver transplantation for unresectable intrahepatic cholangiocarcinoma: An Italian experience. Updates Surg. 2021, 73, 1587–1588. [Google Scholar] [CrossRef] [PubMed]
- Halder, R.; Amaraneni, A.; Shroff, R.T. Cholangiocarcinoma: A review of the literature and future directions in therapy. Hepatobiliary Surg. Nutr. 2022, 11, 555–566. [Google Scholar] [CrossRef]
- Tsilimigras, D.I.; Sahara, K.; Wu, L.; Moris, D.; Bagante, F.; Guglielmi, A.; Aldrighetti, L.; Weiss, M.; Bauer, T.W.; Alexandrescu, S.; et al. Very Early Recurrence After Liver Resection for Intrahepatic Cholangiocarcinoma: Considering Alternative Treatment Approaches. JAMA Surg. 2020, 155, 823–831. [Google Scholar] [CrossRef]
- Loffredo, D.; Marvaso, A.; Ceraso, S.; Cinelli, N.; Rocca, A.; Vitale, M.; Rossi, M.; Genovese, E.; Amato, B.; Cinelli, M. Minimal invasive surgery in treatment of liver metastases from colorectal carcinomas: Case studies and survival rates. BMC Surg. 2013, 13 (Suppl. S2), S45. [Google Scholar] [CrossRef]
- Bartolini, I.; Risaliti, M.; Fortuna, L.; Agostini, C.; Ringressi, M.N.; Taddei, A.; Muiesan, P. Current management of intrahepatic cholangiocarcinoma: From resection to palliative treatments. Radiol. Oncol. 2020, 54, 263–271. [Google Scholar] [CrossRef]
- Masci, G.M.; Ciccarelli, F.; Mattei, F.I.; Grasso, D.; Accarpio, F.; Catalano, C.; Laghi, A.; Sammartino, P.; Iafrate, F. Role of CT texture analysis for predicting peritoneal metastases in patients with gastric cancer. Radiol. Med. 2022, 127, 251–258. [Google Scholar] [CrossRef]
- Rocca, A.; Scacchi, A.; Cappuccio, M.; Avella, P.; Bugiantella, W.; De Rosa, M.; Costa, G.; Polistena, A.; Codacci-Pisanelli, M.; Amato, B.; et al. Robotic surgery for colorectal liver metastases resection: A systematic review. Int. J. Med. Robot. 2021, 17, e2330. [Google Scholar] [CrossRef] [PubMed]
- Sijberden, J.P.; Cipriani, F.; Lanari, J.; Russolillo, N.; Benedetti Cacciaguerra, A.; Osei-Bordom, D.; Conci, S.; Görgec, B.; Primrose, J.N.; Edwin, B.; et al. Minimally invasive ver-sus open liver resection for hepatocellular carcinoma in the elderly: International multicentre propensity score-matched study. Br. J. Surg. 2022, 13, znac423. [Google Scholar] [CrossRef] [PubMed]
- Rocca, A.; Cipriani, F.; Belli, G.; Berti, S.; Boggi, U.; Bottino, V.; Cillo, U.; Cescon, M.; Cimino, M.; Corcione, F.; et al. The Italian Consensus on minimally invasive simultaneous resections for synchronous liver metastasis and primary colorectal cancer: A Delphi methodology. Updates Surg. 2021, 73, 1247–1265. [Google Scholar] [CrossRef]
- Arizza, G.; Russolillo, N.; Ferrero, A.; Syn, N.L.; Cipriani, F.; Aghayan, D.; Marino, M.V.; Memeo, R.; Mazzaferro, V.; Chiow, A.K.H.; et al. Impact of tumor size on the difficulty of laparoscopic left lateral sectionectomies. J. Hepatobiliary Pancreat. Sci. 2022; early view. [Google Scholar] [CrossRef]
- Ceccarelli, G.; Rocca, A.; De Rosa, M.; Fontani, A.; Ermili, F.; Andolfi, E.; Bugiantella, W.; Levi Sandri, G.B. Minimally invasive robotic-assisted combined colorectal and liver excision surgery: Feasibility, safety and surgical technique in a pilot series. Updates Surg. 2021, 73, 1015–1022, Erratum in Updates Surg 2021, 73, 1023–1027. [Google Scholar] [CrossRef]
- Magistri, P.; Assirati, G.; Ballarin, R.; Di Sandro, S.; Di Benedetto, F. Major robotic hepatectomies: Technical considerations. Updates Surg. 2021, 73, 989–997. [Google Scholar] [CrossRef]
- Zhao, Z.; Yin, Z.; Pan, L.; Li, C.; Hu, M.; Lau, W.Y.; Liu, R. Robotic hepatic resection in postero-superior region of liver. Updates Surg. 2021, 73, 1007–1014. [Google Scholar] [CrossRef]
- Calise, F.; Giuliani, A.; Sodano, L.; Crolla, E.; Bianco, P.; Rocca, A.; Ceriello, A. Segmentectomy: Is minimally invasive surgery going to change a liver dogma? Updates Surg. 2015, 67, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Lendoire, J.C.; Gil, L.; Imventarza, O. Intrahepatic cholangiocarcinoma surgery: The impact of lymphadenectomy. Chin. Clin. Oncol. 2018, 7, 53. [Google Scholar] [CrossRef]
- Kanno, H.; Hisaka, T.; Fujiyoshi, K.; Akiba, J.; Hashimoto, K.; Fujita, F.; Akagi, Y. Prognostic Significance of the Histopathological Growth Pattern and Tumor-Infiltrating Lymphocytes in Stratifying Survival After Hepatectomy for Colorectal Liver Metastases. Ann. Surg. Oncol. 2022, 30, 3139–3147. [Google Scholar] [CrossRef] [PubMed]
- Sutton, T.L.; Wong, L.H.; Walker, B.S.; Dewey, E.N.; Eil, R.; Lopez, C.D.; Kardosh, A.; Chen, E.Y.; Rocha, F.G.; Billingsley, K.G.; et al. Hepatectomy is associated with improved oncologic outcomes in recurrent colorectal liver metastases: A propensity-matched analysis. Surgery, 2022; in press. [Google Scholar] [CrossRef] [PubMed]
- Shen, W.F.; Zhong, W.; Xu, F.; Kan, T.; Geng, L.; Xie, F.; Sui, C.J.; Yang, J.M. Clinicopathological and prognostic analysis of 429 patients with intrahepatic cholangiocarcinoma. World J. Gastroenterol. 2009, 15, 5976–5982. [Google Scholar] [CrossRef]
- Zhang, D.; Zeng, H.; Pan, Y.; Zhao, Y.; Wang, X.; Chen, J.; Wang, J.; Zhang, Y.; Zhou, Z.; Xu, L.; et al. Liver Tumor Markers, HALP Score, and NLR: Simple, Cost-Effective, Easily Accessible Indexes for Predicting Prognosis in ICC Patients after Surgery. J. Pers. Med. 2022, 12, 2041. [Google Scholar] [CrossRef] [PubMed]
- Viganò, L.; Galvanin, J.; Cimino, M.; Torzilli, G. Laparoscopic application of the hooking technique for ultrasound-guided minimally invasive liver surgery. Updates Surg. 2022, 74, 373–377. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Cao, B.; Bi, X.; Chen, W.; Wang, L.; Du, Z.; Zhang, X.; Yu, X. Evaluation of liver function in patients with chronic hepatitis B using Gd-EOB-DTPA-enhanced T1 mapping at different acquisition time points: A feasibility study. Radiol. Med. 2021, 126, 1149–1158. [Google Scholar] [CrossRef]
- Hyodo, R.; Takehara, Y.; Naganawa, S. 4D Flow MRI in the portal venous system: Imaging and analysis methods, and clinical applications. Radiol. Med. 2022, 127, 1181–1198. [Google Scholar] [CrossRef]
- Gentile, D.; Donadon, M.; Civilini, E.; Torzilli, G. Total upper transversal hepatectomy with outflow reconstruction for advanced mass-forming cholangiocarcinoma. Updates Surg. 2021, 73, 769–773. [Google Scholar] [CrossRef] [PubMed]
- Ruzzenente, A.; Alaimo, L.; Conci, S.; De Bellis, M.; Marchese, A.; Ciangherotti, A.; Campagnaro, T.; Guglielmi, A. Hyper accuracy three-dimensional (HA3D™) technology for planning complex liver resections: A preliminary single center experience. Updates Surg. 2022, 75, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Zerunian, M.; Pucciarelli, F.; Caruso, D.; Polici, M.; Masci, B.; Guido, G.; De Santis, D.; Polverari, D.; Principessa, D.; Benvenga, A.; et al. Artificial intelligence based image quality enhancement in liver MRI: A quantitative and qualitative evaluation. Radiol. Med. 2022, 127, 1098–1105. [Google Scholar] [CrossRef]
- Sammon, J.; Fischer, S.; Menezes, R.; Hosseini-Nik, H.; Lewis, S.; Taouli, B.; Jhaveri, K. MRI features of combined hepatocellular- cholangiocarcinoma versus mass forming intrahepatic cholangiocarcinoma. Cancer Imaging 2018, 18, 8. [Google Scholar] [CrossRef]
- Bilreiro, C.; Soler, J.C.; Ayuso, J.R.; Caseiro-Alves, F.; Ayuso, C. Diagnostic value of morphological enhancement patterns in the hepatobiliary phase of gadoxetic acid-enhanced MRI to distinguish focal nodular hyperplasia from hepatocellular adenoma. Radiol. Med. 2021, 126, 1379–1387. [Google Scholar] [CrossRef]
- Jhaveri, K.S.; Hosseini-Nik, H. MRI of cholangiocarcinoma. J. Magn. Reson. Imaging 2015, 42, 1165–1179. [Google Scholar] [CrossRef] [PubMed]
- Kwon, S.; Kim, Y.K.; Park, H.J.; Jeong, W.K.; Lee, W.J.; Choi, D. Is gadoxetic acid-enhanced MRI limited in tumor characterization for patients with chronic liver disease? Magn. Reson. Imaging 2014, 32, 1214–1222. [Google Scholar] [CrossRef] [PubMed]
- Hamm, C.A.; Wang, C.J.; Savic, L.J.; Ferrante, M.; Schobert, I.; Schlachter, T.; Lin, M.; Duncan, J.S.; Weinreb, J.C.; Chapiro, J.; et al. Deep learning for liver tumor diagnosis part I: Development of a convolutional neural network classifier for multi-phasic MRI. Eur. Radiol. 2019, 29, 3338–3347. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.J.; Hamm, C.A.; Savic, L.J.; Ferrante, M.; Schobert, I.; Schlachter, T.; Lin, M.; Weinreb, J.C.; Duncan, J.S.; Chapiro, J.; et al. Deep learning for liver tumor diagnosis part II: Convolutional neural network interpretation using radiologic imaging features. Eur. Radiol. 2019, 29, 3348–3357. [Google Scholar] [CrossRef]
- Zhou, Y.; Zhou, G.; Zhang, J.; Xu, C.; Wang, X.; Xu, P. Radiomics signature on dynamic contrast-enhanced MR images: A potential imaging biomarker for prediction of microvascular invasion in mass-forming intrahepatic cholangiocarcinoma. Eur. Radiol. 2021, 31, 6846–6855. [Google Scholar] [CrossRef]
- Huang, F.; Liu, X.; Liu, P.; Xu, D.; Li, Z.; Lin, H.; Xie, A. The Application Value of MRI T2∗WI Radiomics Nomogram in Discriminating Hepatocellular Carcinoma from Intrahepatic Cholangiocarcinoma. Comput. Math. Methods Med. 2022, 2022, 7099476. [Google Scholar] [CrossRef] [PubMed]
- Hu, R.; Li, H.; Horng, H.; Thomasian, N.M.; Jiao, Z.; Zhu, C.; Zou, B.; Bai, H.X. Automated machine learning for differentiation of hepatocellular carcinoma from intrahepatic cholangiocarcinoma on multiphasic MRI. Sci. Rep. 2022, 12, 7924. [Google Scholar] [CrossRef]
- Song, W.; Chen, Q.; Guo, D.; Jiang, C. Preoperative estimation of the survival of patients with unresectable hepatocellular carcinoma achieving complete response after conventional transcatheter arterial chemoembolization: Assessments of clinical and LI-RADS MR features. Radiol. Med. 2022, 127, 939–949. [Google Scholar] [CrossRef]
- Xu, L.; Wan, Y.; Luo, C.; Yang, J.; Yang, P.; Chen, F.; Wang, J.; Niu, T. Integrating intratumoral and peritumoral features to predict tumor recurrence in intrahepatic cholangiocarcinoma. Phys. Med. Biol. 2021, 66, 125001. [Google Scholar] [CrossRef]
- Zhao, L.; Ma, X.; Liang, M.; Li, D.; Ma, P.; Wang, S.; Wu, Z.; Zhao, X. Prediction for early recurrence of intrahepatic mass-forming cholangiocarcinoma: Quantitative magnetic resonance imaging combined with prognostic immunohistochemical markers. Cancer Imaging 2019, 19, 49. [Google Scholar] [CrossRef]
- Xu, L.; Yang, P.; Liang, W.; Liu, W.; Wang, W.; Luo, C.; Wang, J.; Peng, Z.; Xing, L.; Huang, M.; et al. A radiomics approach based on support vector machine using MR images for preoperative lymph node status evaluation in intrahepatic cholangiocarcinoma. Theranostics 2019, 9, 5374–5385. [Google Scholar] [CrossRef]
- Nishioka, E.; Tsurusaki, M.; Kozuki, R.; Im, S.W.; Kono, A.; Kitajima, K.; Murakami, T.; Ishii, K. Comparison of Conventional Imaging and 18F-Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography in the Diagnostic Accuracy of Staging in Patients with Intrahepatic Cholangiocarcinoma. Diagnostics 2022, 12, 2889. [Google Scholar] [CrossRef]
- Cellina, M.; Gibelli, D.; Martinenghi, C.; Giardini, D.; Soresina, M.; Menozzi, A.; Oliva, G.; Carrafiello, G. Non-contrast magnetic resonance lymphography (NCMRL) in cancer-related secondary lymphedema: Acquisition technique and imaging findings. Radiol. Med. 2021, 126, 1477–1486. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Wu, Z.; Zhang, X.; Liu, S.; Zhao, J.; Yuan, F.; Shi, Y.; Song, B. Machine learning: An approach to preoperatively predict PD-1/PD-L1 expression and outcome in intrahepatic cholangiocarcinoma using MRI biomarkers. ESMO Open 2020, 5, e000910. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Zhou, G.; Zhang, J.; Xu, C.; Zhu, F.; Xu, P. DCE-MRI based radiomics nomogram for preoperatively differentiating combined hepatocellular-cholangiocarcinoma from mass-forming intrahepatic cholangiocarcinoma. Eur. Radiol. 2022, 32, 5004–5015. [Google Scholar] [CrossRef] [PubMed]
- Qian, X.; Lu, X.; Ma, X.; Zhang, Y.; Zhou, C.; Wang, F.; Shi, Y.; Zeng, M. A Multi-Parametric Radiomics Nomogram for Preoperative Prediction of Microvascular Invasion Status in Intrahepatic Cholangiocarcinoma. Front. Oncol. 2022, 12, 838701. [Google Scholar] [CrossRef] [PubMed]
- Soyer, P.; Fishman, E.K.; Rowe, S.P.; Patlas, M.N.; Chassagnon, G. Does artificial intelligence surpass the radiologist? Diagn. Interv. Imaging 2022, 103, 445–447. [Google Scholar] [CrossRef]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brunese, M.C.; Fantozzi, M.R.; Fusco, R.; De Muzio, F.; Gabelloni, M.; Danti, G.; Borgheresi, A.; Palumbo, P.; Bruno, F.; Gandolfo, N.; et al. Update on the Applications of Radiomics in Diagnosis, Staging, and Recurrence of Intrahepatic Cholangiocarcinoma. Diagnostics 2023, 13, 1488. https://doi.org/10.3390/diagnostics13081488
Brunese MC, Fantozzi MR, Fusco R, De Muzio F, Gabelloni M, Danti G, Borgheresi A, Palumbo P, Bruno F, Gandolfo N, et al. Update on the Applications of Radiomics in Diagnosis, Staging, and Recurrence of Intrahepatic Cholangiocarcinoma. Diagnostics. 2023; 13(8):1488. https://doi.org/10.3390/diagnostics13081488
Chicago/Turabian StyleBrunese, Maria Chiara, Maria Rita Fantozzi, Roberta Fusco, Federica De Muzio, Michela Gabelloni, Ginevra Danti, Alessandra Borgheresi, Pierpaolo Palumbo, Federico Bruno, Nicoletta Gandolfo, and et al. 2023. "Update on the Applications of Radiomics in Diagnosis, Staging, and Recurrence of Intrahepatic Cholangiocarcinoma" Diagnostics 13, no. 8: 1488. https://doi.org/10.3390/diagnostics13081488