
Automated Detection of Endometrial Polyps from Hysteroscopic Videos Using Deep Learning

Abstract
:1. Introduction
- We proposed group normalization in the deep learning model YOLOX to improve the performance of real-time detection of endometrial polyps from hysteroscopic images.
- A video adjacent-frame association algorithm was applied in the post-processing stage. The algorithm effectively solved the problem of the original YOLOX, i.e., unstable polyp detection.
- We present the first application based on deep learning to detect endometrial polyps from hysteroscopic images.
2. Methods
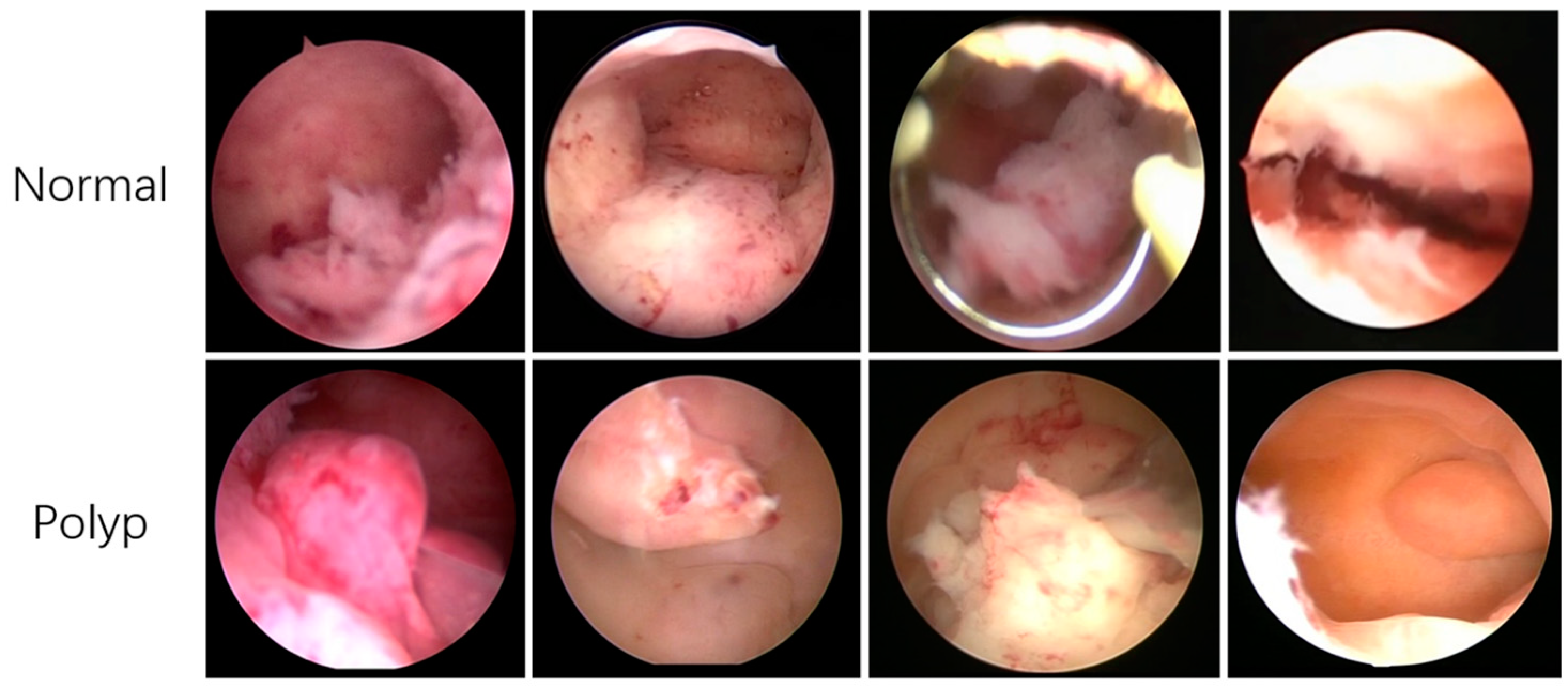
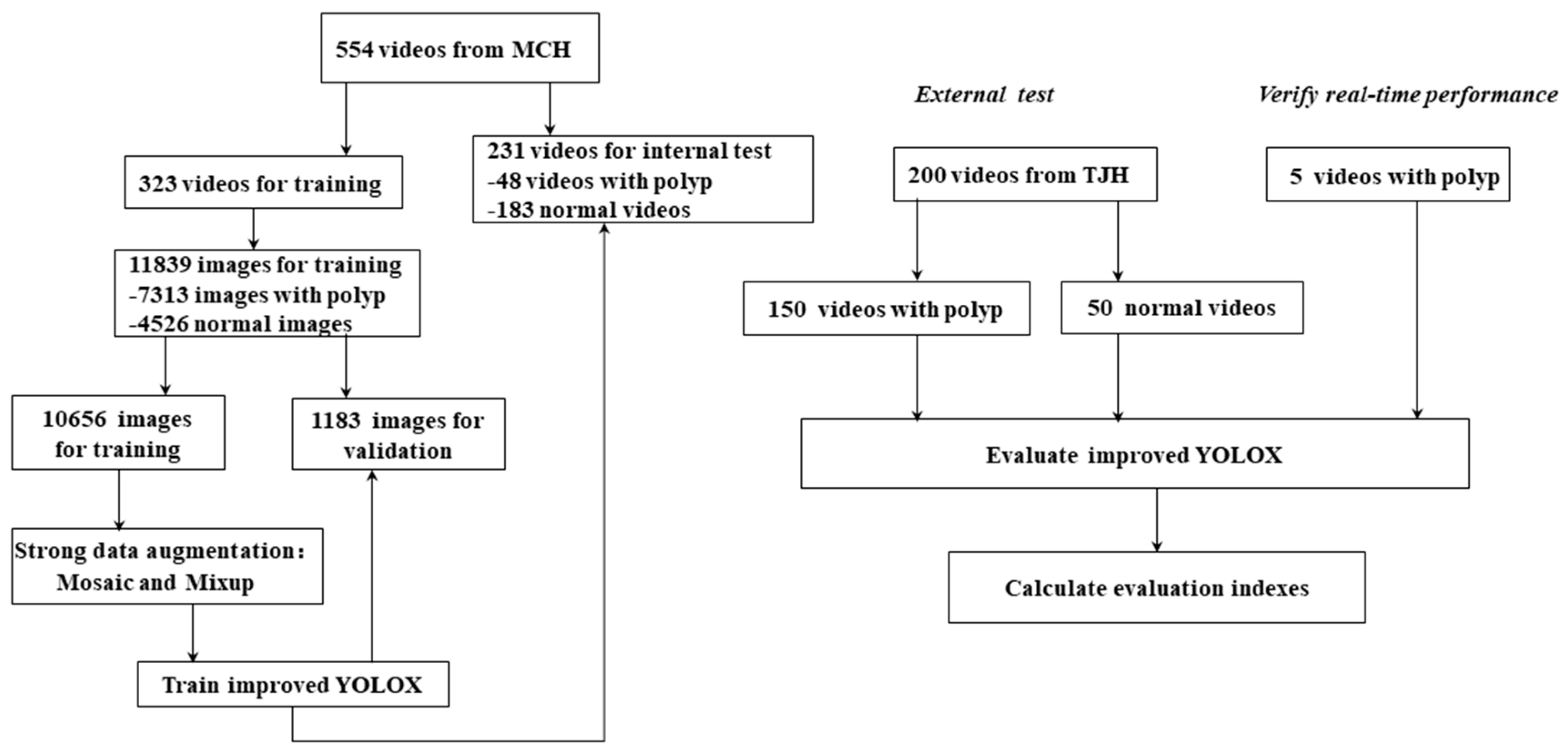
2.1. Datasets
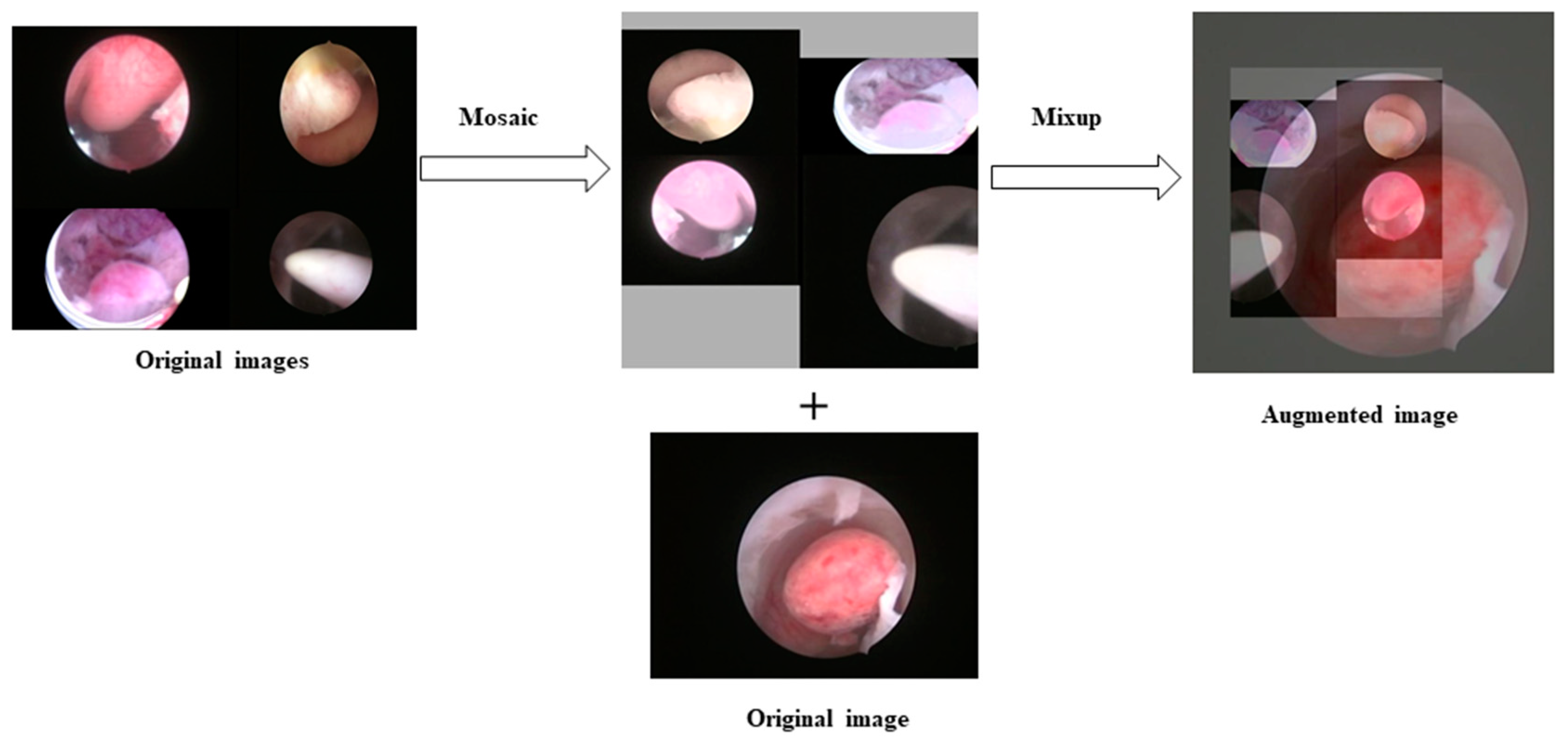
2.2. Data Preprocessing
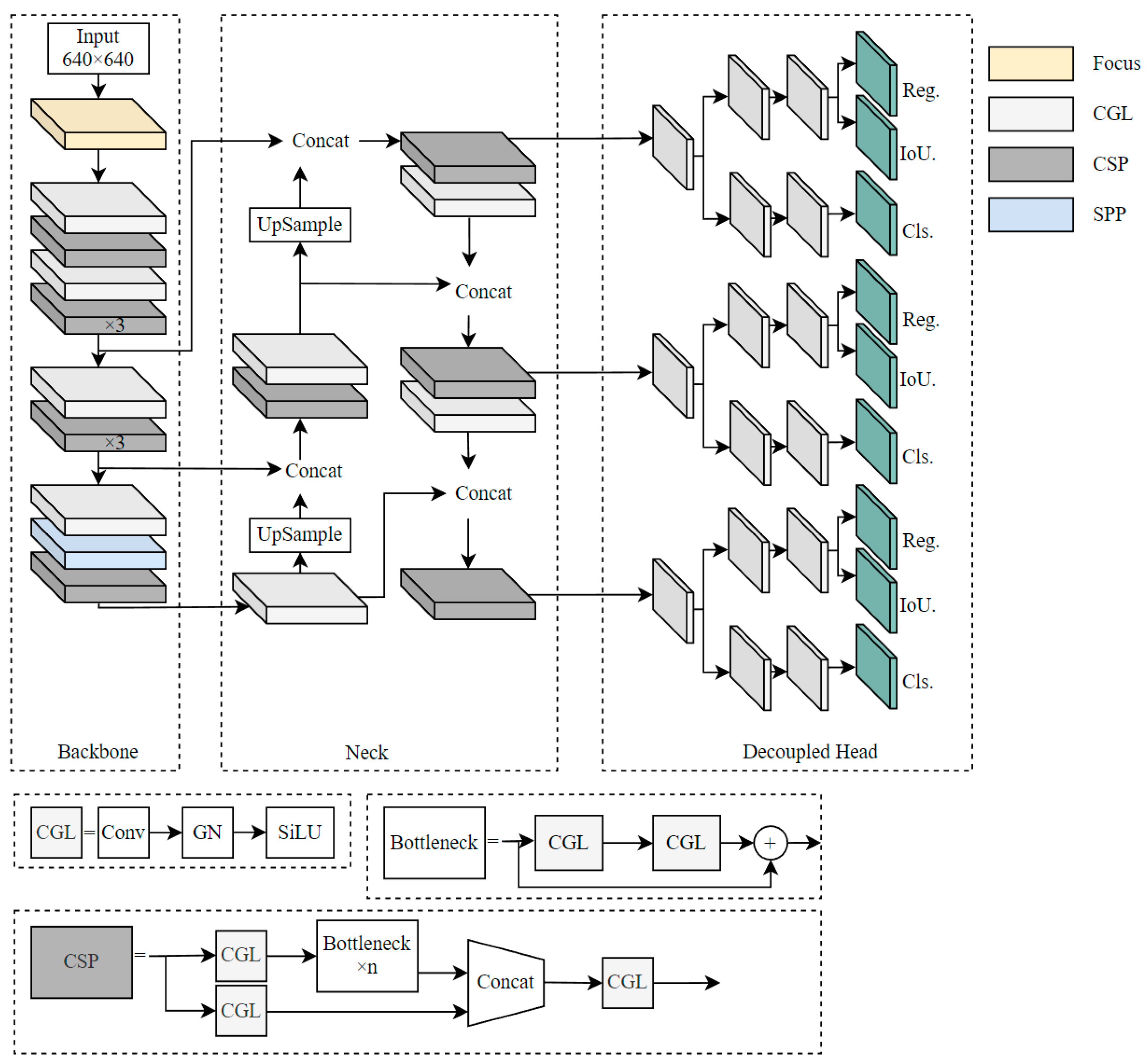
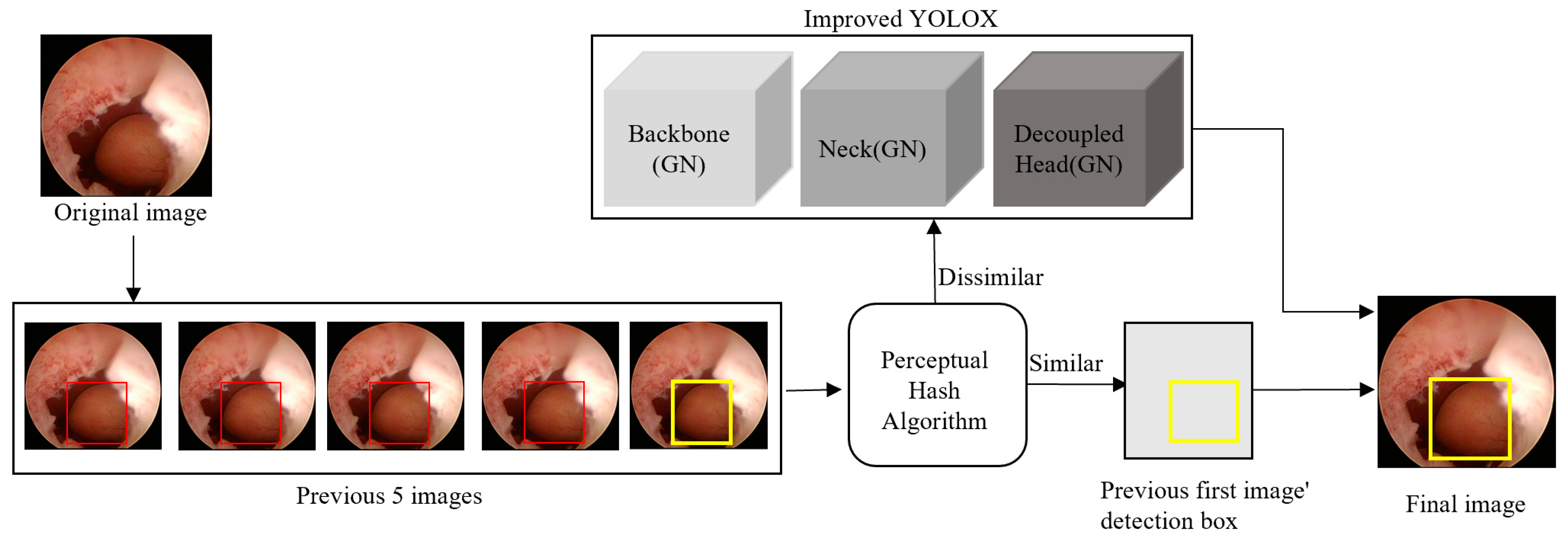
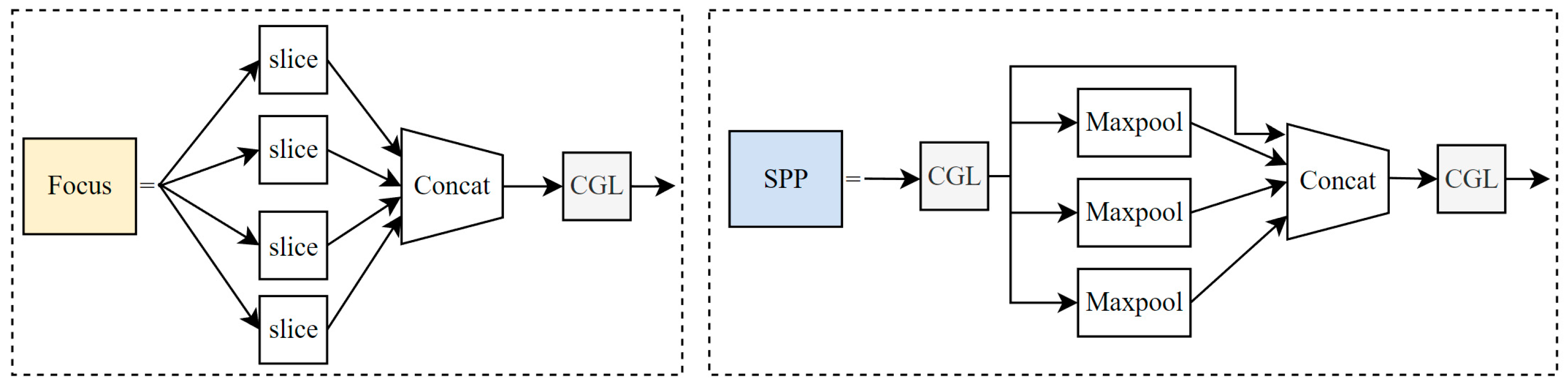
2.3. Improved YOLOX
2.3.1. Group Normalization
2.3.2. VAFA Algorithm
- When five or more adjacent frames are detected as containing a “polyp”, the similarity between the current frame and the next frame is calculated.
- If the similarity is <9, the object detection box of the current frame is assigned to the next frame, until the similarity between frames is no longer <9.
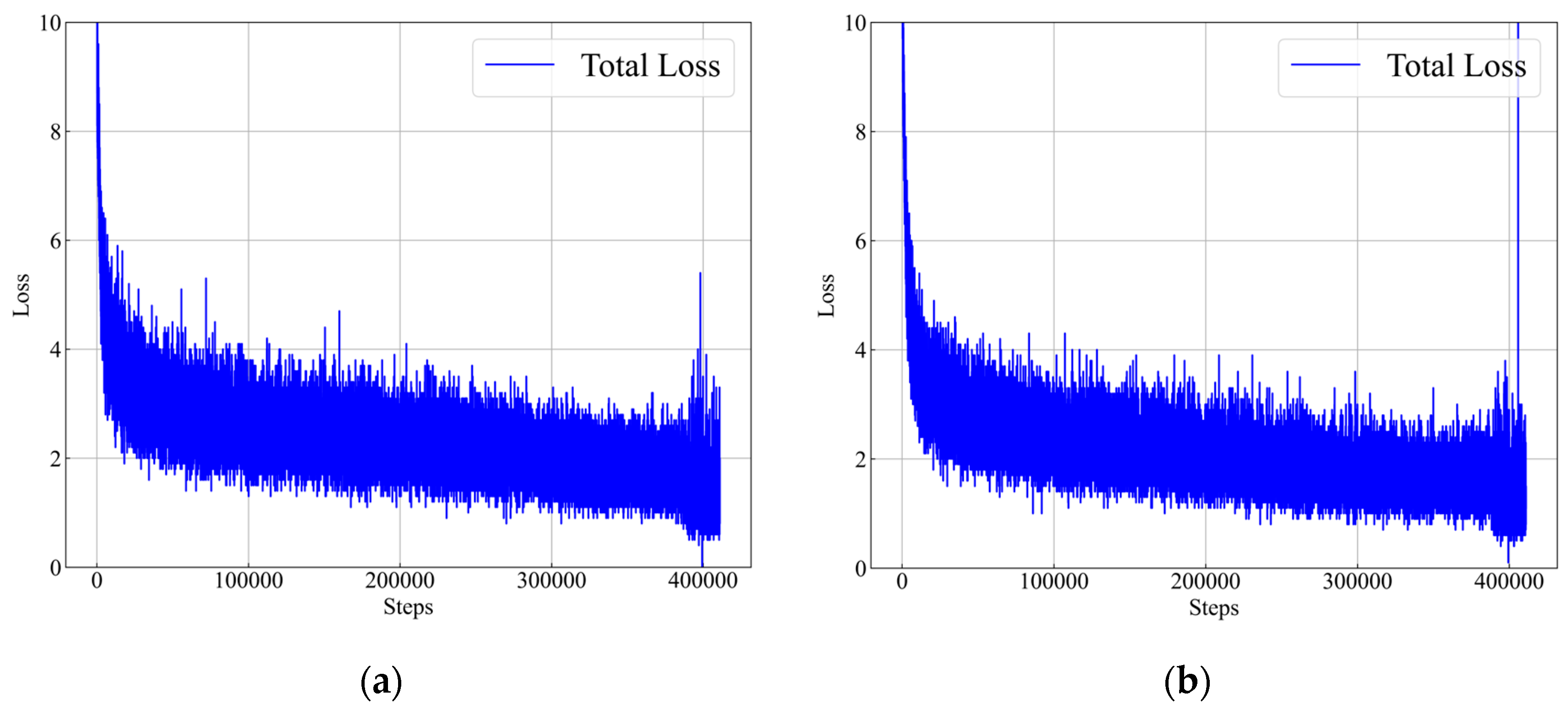
2.4. Model Training
2.5. Evaluation
3. Results
4. Discussion
4.1. Evaluation
4.2. Limitations
- The model showed poor performance in detecting hysteroscopic images with polyps partially occluded by the endometrium.
- A large floating endometrium can be misdiagnosed as a polyp. We expect that problems 1 and 2 can be addressed by increasing the number of occluded polyp images and background images in the training set.
- Deep-learning-based object tracking algorithms, such as Deep SORT, have been employed to address the problem of unsteady detection boxes [32]. However, their performance should be improved further. The proposed VAFA algorithm should also be updated, because the object detection display is insufficiently smooth. Therefore, further research is needed to develop more advanced algorithms that would improve the polyp detection performance.
- A prospective study should be conducted to check that the proposed method performs as expected in real clinical practice.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A.


Appendix B. Comparison with EfficientDet

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Model (Video-Level) | Sensitivity (%) | Specificity (%) | Accuracy (%) | Precision (%) | F1 (%) |
|---|---|---|---|---|---|
| MCH test set | |||||
| EfficientDet | 52.08 | 97.81 | 88.31 | 86.21 | 67.97 |
| YOLOX + GN + VAFA | 100 | 88.52 | 90.91 | 69.57 | 93.91 |
| TJH test set | |||||
| EfficientDet | 50.0 | 98.36 | 88.31 | 88.89 | 66.30 |
| YOLOX + GN + VAFA | 92.0 | 76.0 | 88.0 | 92.0 | 83.24 |
| Model (Image-Level) | Sensitivity (%) | Specificity (%) | Accuracy (%) | Precision (%) | F1 (%) |
| MCH test set | |||||
| EfficientDet | 83.16 | 89.34 | 88.82 | 43.51 | 86.14 |
| YOLOX + GN + VAFA | 98.73 | 84.32 | 85.95 | 44.61 | 90.96 |
| TJH test set | |||||
| EfficientDet | 79.23 | 89.93 | 88.97 | 44.63 | 84.24 |
| YOLOX + GN + VAFA | 92.92 | 70.41 | 84.24 | 83.34 | 80.11 |
References
- Yanhua, Z. Clinical Significance of Gynecological Screening in Early Cervical Cancer Screening. World’s Latest Med. Inf. Dig. 2015, 15, 130. [Google Scholar]
- Hong, J. Study on the Incidence of Endometrial Polyps in Common Gynecological Diseases; Xinjiang Medical University: Xinjiang, China, 2013. [Google Scholar]
- Wenqian, G. Clinical Observation of Hysteroscopy in the Treatment of Endometrial Polyps. Chin. J. Metall. Ind. Med. 2021, 38, 202–203. [Google Scholar]
- Xiang, W.; Qi, Y.; Tian, W.; Zhang, H. Clinicopathological Analysis of Postmenopausal Endometrial Polyps. Chin. J. Obstet. Gyn. 2021, 56, 131–136. [Google Scholar]
- Qin, R.; Gan, J.; Chen, X.; Nong, W. Research Progress of Hysteroscopic Surgery in the Treatment of Uterine Lesions. Med. Rev. 2020, 26, 3282–3286. [Google Scholar]
- Wang, S.; Qunying, Z. Analysis of Reproductive Prognosis of Patients with Different Types of Submucous Myoma Treated by Hysteroscopic Electrotomy. J. Wannan Med. Coll. 2019, 38, 260–263. [Google Scholar]
- Huihong, H.; Wantao, L.; Chunyan, L.; Yiyan, S. Nursing Progress of Complications of Gynecological Hysteroscopic Surgery. Chin. Med. Sci. 2020, 10, 65–68. [Google Scholar]
- Ramamurthy, K.; George, T.T.; Shah, Y.; Sasidhar, P. A Novel Multi-Feature Fusion Method for Classification of Gastrointestinal Diseases Using Endoscopy Images. Diagnostics 2022, 12, 2316. [Google Scholar] [CrossRef]
- Muruganantham, P.; Balakrishnan, S.M. Attention Aware Deep Learning Model for Wireless Capsule Endoscopy Lesion Classification and Localization. J. Med. Biol. Eng. 2022, 42, 157–168. [Google Scholar] [CrossRef]
- Jha, D.; Ali, S.; Tomar, N.K.; Johansen, H.D.; Johansen, D.; Rittscher, J.; Riegler, M.A.; Halvorsen, P. Real-Time Polyp Detection, Localization and Segmentation in Colonoscopy Using Deep Learning. IEEE Access 2021, 9, 40496–40510. [Google Scholar] [CrossRef]
- Durak, S.; Bayram, B.; Bakırman, T.; Erkut, M.; Doğan, M.; Gürtürk, M.; Akpınar, B. Deep Neural Network Approaches for Detecting Gastric Polyps in Endoscopic Images. Med. Biol. Eng. Comput. 2021, 59, 1563–1574. [Google Scholar] [CrossRef]
- Yamada, A.; Niikura, R.; Otani, K.; Aoki, T.; Koike, K. Automatic Detection of Colorectal Neoplasia in Wireless Colon Capsule Endoscopic Images Using a Deep Convolutional Neural Network. Endoscopy 2021, 53, 832–836. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Wang, Y.; Zhang, S. Accuracy of Artificial Intelligence-Assisted Detection of Esophageal Cancer and Neoplasms on Endoscopic Images: A Systematic Review and Meta-Analysis. J. Dig. Dis. 2021, 22, 318–328. [Google Scholar] [CrossRef] [PubMed]
- Hodneland, E.; Dybvik, J.A.; Wagner-Larsen, K.S.; Šoltészová, V.; Munthe-Kaas, A.Z.; Fasmer, K.E.; Krakstad, C.; Lundervold, A.; Lundervold, A.S.; Salvesen, Ø.; et al. Automated Segmentation of Endometrial Cancer on MR Images Using Deep Learning. Sci. Rep. 2021, 11, 179. [Google Scholar] [CrossRef]
- Kurata, Y.; Nishio, M.; Moribata, Y.; Kido, A.; Himoto, Y.; Otani, S.; Fujimoto, K.; Yakami, M.; Minamiguchi, S.; Mandai, M.; et al. Automatic Segmentation of Uterine Endometrial Cancer on Multi-Sequence MRI Using a Convolutional Neural Network. Sci. Rep. 2021, 11, 14440. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Wang, Z.; Zhang, J.; Wang, C.; Wang, Y.; Chen, H.; Shan, L.; Huo, J.; Gu, J.; Ma, X. Deep Learning Model for Classifying Endometrial Lesions. J. Transl. Med. 2021, 19, 10. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, Y.; Sone, K.; Noda, K.; Yoshida, K.; Toyohara, Y.; Kato, K.; Inoue, F.; Kukita, A.; Taguchi, A.; Nishida, H.; et al. Automated System for Diagnosing Endometrial Cancer by Adopting Deep-Learning Technology in Hysteroscopy. PLoS ONE 2021, 16, e0248526. [Google Scholar] [CrossRef] [PubMed]
- Ge, Z.; Liu, S.; Wang, F.; Li, Z.; Sun, J. YOLOX: Exceeding YOLO Series in 2021. arXiv 2021, arXiv:2107.08430. [Google Scholar]
- Ioffe, S.; Szegedy, C. Batch Normalization: Accelerating Deep Network Training by Reducing Internal Covariate Shift. arXiv 2015, arXiv:1502.03167. [Google Scholar]
- Wu, Y.; He, K. Group Normalization. Int. J. Comput. Vis. 2019, 128, 742–755. [Google Scholar] [CrossRef]
- Tan, M.; Pang, R.; Le, Q.V. Efficient Det: Scalable and Efficient Object Detection. In Proceedings of the 2020 IEEE/CVF Conference on Computer Vision and Pattern Recognition (CVPR) IEEE, Virtual, 16–18 June 2020. [Google Scholar]
- Török, P.; Harangi, B. Digital Image Analysis with Fully Connected Convolutional Neural Network to Facilitate Hysteroscopic Fibroid Resection. Gynecol. Obstet. Investig. 2018, 83, 615–619. [Google Scholar] [CrossRef]
- Zhang, Y.; Gong, C.; Zheng, L.; Li, X.; Yang, X. Deep Learning for Intelligent Recognition and Prediction of Endometrial Cancer. J. Healthc. Eng. 2021, 2021, 1148309. [Google Scholar] [CrossRef] [PubMed]
- Dong, H.-C.; Dong, H.-K.; Yu, M.-H.; Lin, Y.-H.; Chang, C.-C. Using Deep Learning with Convolutional Neural Network Approach to Identify the Invasion Depth of Endometrial Cancer in Myometrium Using MR Images: A Pilot Study. Int. J. Environ. Res. Public Health 2020, 17, 5993. [Google Scholar] [CrossRef] [PubMed]
- Xia, Z.; Zhang, L.; Liu, S.; Ran, W.; Liu, Y.; Tu, J. Deep Learning-Based Hysteroscopic Intelligent Examination and Ultrasound Examination for Diagnosis of Endometrial Carcinoma. J. Supercomput. 2021, 78, 11229–11244. [Google Scholar] [CrossRef]
- Wang, X.; Bao, N.; Xin, X.; Tan, J.; Li, H.; Zhou, S.; Liu, H. Automatic Evaluation of Endometrial Receptivity in Three-Dimensional Transvaginal Ultrasound Images Based on 3D U-Net Segmentation. Quant. Imaging Med. Surg. 2022, 12, 4095–4108. [Google Scholar] [CrossRef]
- Dilna, K.T.; Anitha, J.; Angelopoulou, A.; Kapetanios, E.; Chaussalet, T.; Hemanth, D.J. Classification of Uterine Fibroids in Ultrasound Images Using Deep Learning Model. In Proceedings of the 22nd Computational Science–ICCS 2022 International Conference, London, UK, 21–23 June 2022; pp. 50–56. [Google Scholar] [CrossRef]
- Ahmed, Z.; Kareem, M.; Khan, H.; Saman, Z.; Hassan Jaskani, F. Detection of Uterine Fibroids in Medical Images Using Deep Neural Networks. EAI Endorsed Trans. Energy Web. 2022, 1, 13. [Google Scholar] [CrossRef]
- Sundar, S.; Sumathy, S. Transfer Learning Approach in Deep Neural Networks for Uterine Fibroid Detection. Int. J. Comput. Sci. Eng. 2022, 25, 52. [Google Scholar] [CrossRef]
- Luo, Y.-H.; Xi, I.L.; Wang, R.; Abdallah, H.O.; Wu, J.; Vance, A.Z.; Chang, K.; Kohi, M.; Jones, L.; Reddy, S.; et al. Deep Learning Based on MR Imaging for Predicting Outcome of Uterine Fibroid Embolization. J. Vasc. Interv. Radiol. 2020, 31, 1010–1017.e3. [Google Scholar] [CrossRef]
- Chun-ming, T.; Dong, L.I.U.; Xiang, Y.U. MRI Image Segmentation System of Uterine Fibroids Based on AR-Unet Network. Am. Acad. Sci. Res. J. Eng. Tech. Sci. 2020, 71, 1–10. [Google Scholar]
- Wojke, N.; Bewley, A.; Paulus, D. Simple Online and Realtime Tracking with a Deep Association Metric. arXiv 2017, arXiv:1703.07402. [Google Scholar]





| Model | Sensitivity (%) | Specificity (%) | Accuracy (%) | Precision (%) | F1 (%) |
|---|---|---|---|---|---|
| MCH test set | |||||
| YOLOX | 95.83 | 95.08 | 95.24 | 80.70 | 95.46 |
| YOLOX + GN | 100 | 89.62 | 91.77 | 71.64 | 94.52 |
| YOLOX + VAFA | 100 | 86.89 | 88.74 | 65.71 | 92.99 |
| YOLOX + GN + VAFA | 100 | 88.52 | 90.91 | 69.57 | 93.91 |
| TJH test set | |||||
| YOLOX | 77.33 | 96.0 | 82.0 | 98.31 | 85.66 |
| YOLOX + GN | 90.67 | 80.0 | 88.0 | 93.15 | 85.0 |
| YOLOX + VAFA | 91.33 | 76.0 | 87.5 | 91.95 | 82.96 |
| YOLOX + GN + VAFA | 92.0 | 76.0 | 88.0 | 92.0 | 83.24 |
| Model | Sensitivity (%) | Specificity (%) | Accuracy (%) | Precision (%) | F1 (%) |
|---|---|---|---|---|---|
| MCH test set | |||||
| YOLOX | 96.01 | 92.23 | 92.70 | 61.39 | 94.11 |
| YOLOX + GN | 98.02 | 85.54 | 86.96 | 46.45 | 91.36 |
| YOLOX + VAFA | 98.68 | 84.32 | 85.89 | 43.69 | 90.94 |
| YOLOX + GN + VAFA | 98.73 | 84.32 | 85.95 | 44.61 | 90.96 |
| TJH test set | |||||
| YOLOX | 82.07 | 91.38 | 85.66 | 93.81 | 86.47 |
| YOLOX + GN | 89.25 | 72.69 | 82.86 | 83.88 | 80.12 |
| YOLOX + VAFA | 92.91 | 70.73 | 84.40 | 83.59 | 80.32 |
| YOLOX + GN + VAFA | 92.92 | 70.41 | 84.24 | 83.34 | 80.11 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, A.; Du, X.; Yuan, S.; Shen, W.; Zhu, X.; Wang, W. Automated Detection of Endometrial Polyps from Hysteroscopic Videos Using Deep Learning. Diagnostics 2023, 13, 1409. https://doi.org/10.3390/diagnostics13081409
Zhao A, Du X, Yuan S, Shen W, Zhu X, Wang W. Automated Detection of Endometrial Polyps from Hysteroscopic Videos Using Deep Learning. Diagnostics. 2023; 13(8):1409. https://doi.org/10.3390/diagnostics13081409
Chicago/Turabian StyleZhao, Aihua, Xin Du, Suzhen Yuan, Wenfeng Shen, Xin Zhu, and Wenwen Wang. 2023. "Automated Detection of Endometrial Polyps from Hysteroscopic Videos Using Deep Learning" Diagnostics 13, no. 8: 1409. https://doi.org/10.3390/diagnostics13081409