

Research of Prostate Cancer Urinary Diagnostic Biomarkers by Proteomics: The Noteworthy Influence of Inflammation
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients Selection and Classification
2.2. Urinary Samples Preparation
2.3. Proteins Quantification
2.4. Proteomic Analysis
2.5. Enzyme-Linked Immunosorbent Assay (ELISA)
2.6. Statistical Analysis
3. Results
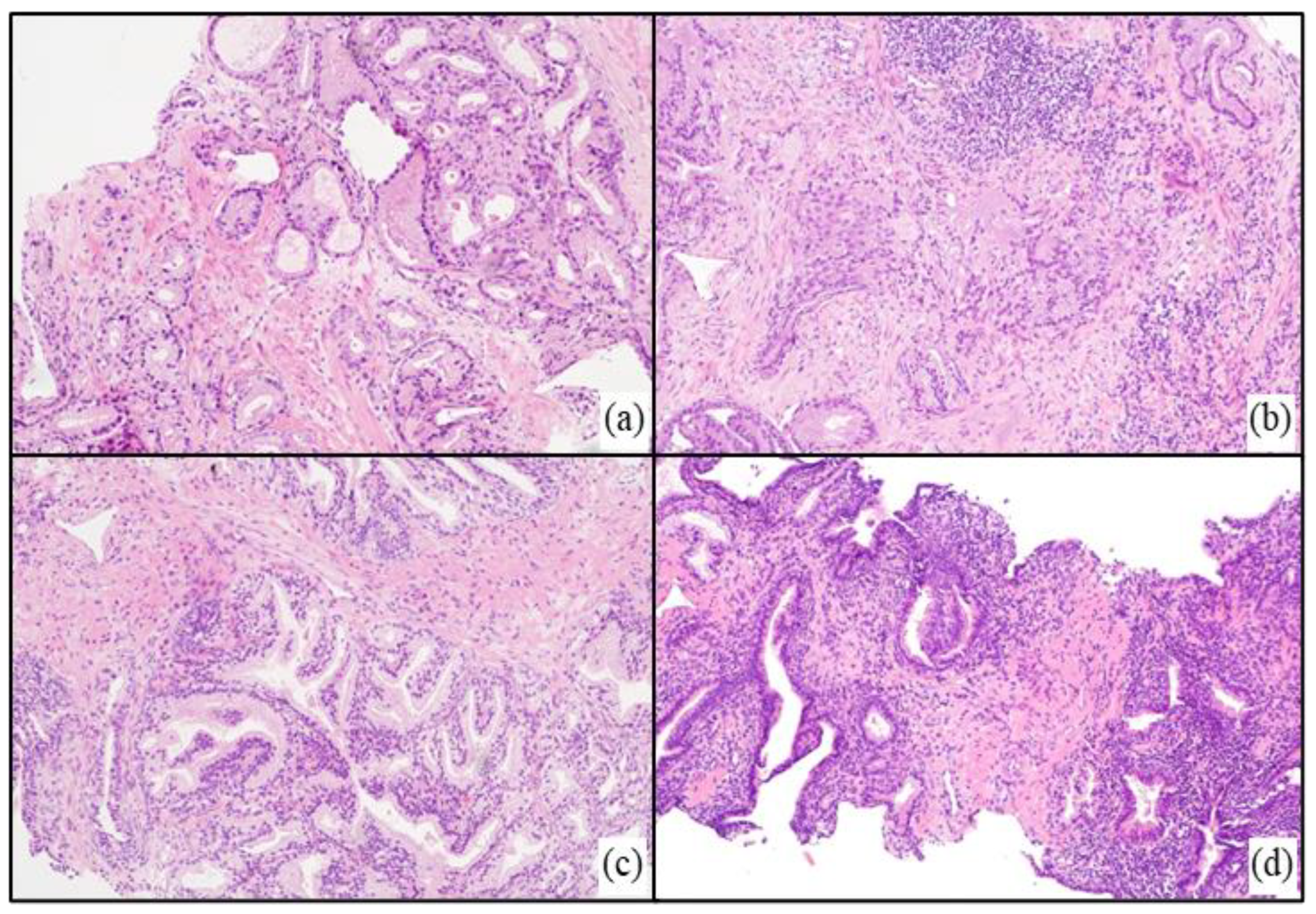
3.1. Histological Examination
3.2. Clinical Data
3.3. Protein Concentration
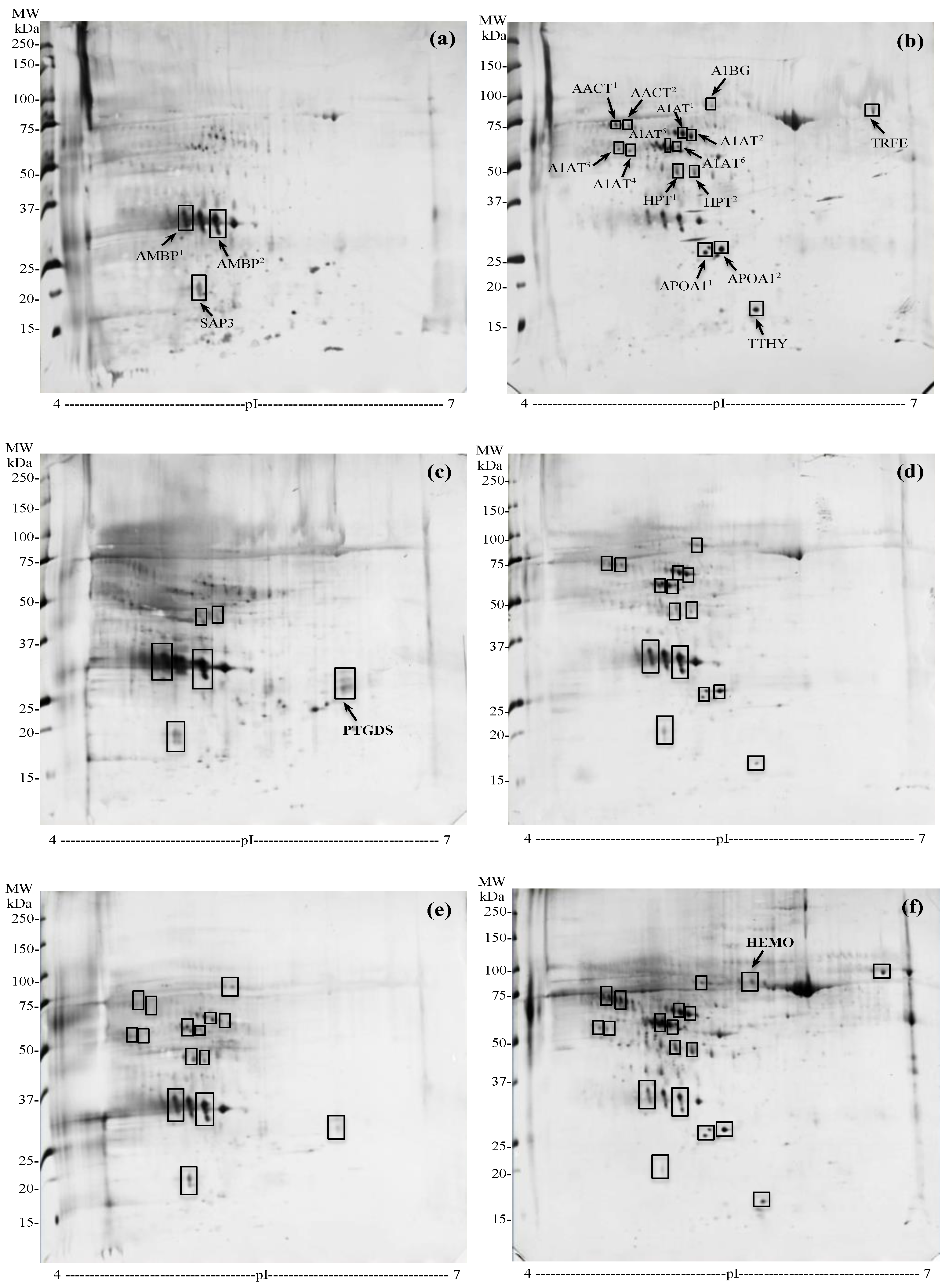
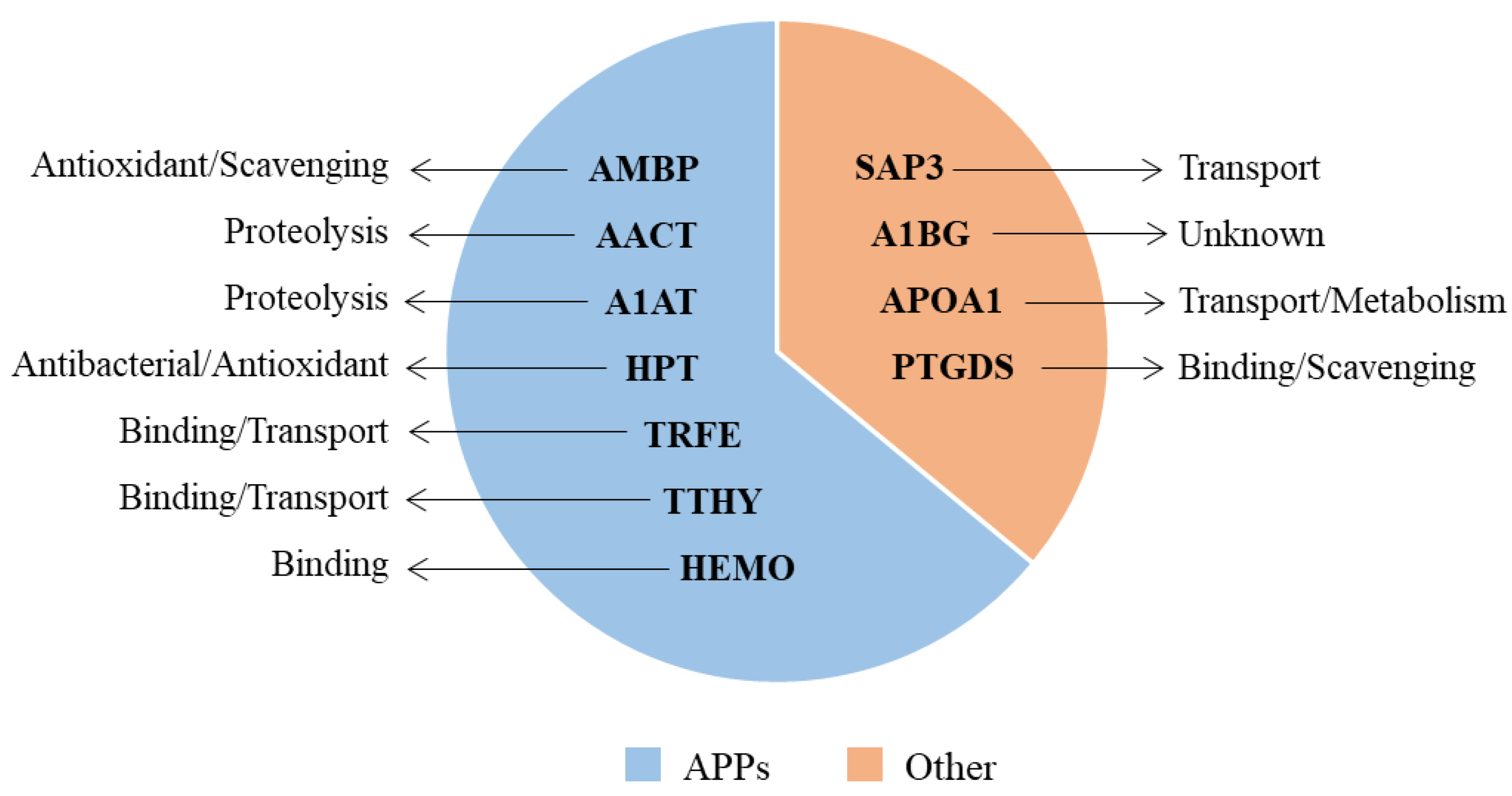
3.4. Proteomic Comparisons
3.4.1. Urinary Protein Expression in PCa and BPH Regardless Inflammation
3.4.2. Urinary Protein Expression in Specimens without Inflammation
3.4.3. Urinary Protein Expression in PCa with and without Inflammation
3.4.4. Urinary Protein Expression in BPH with and without Inflammation
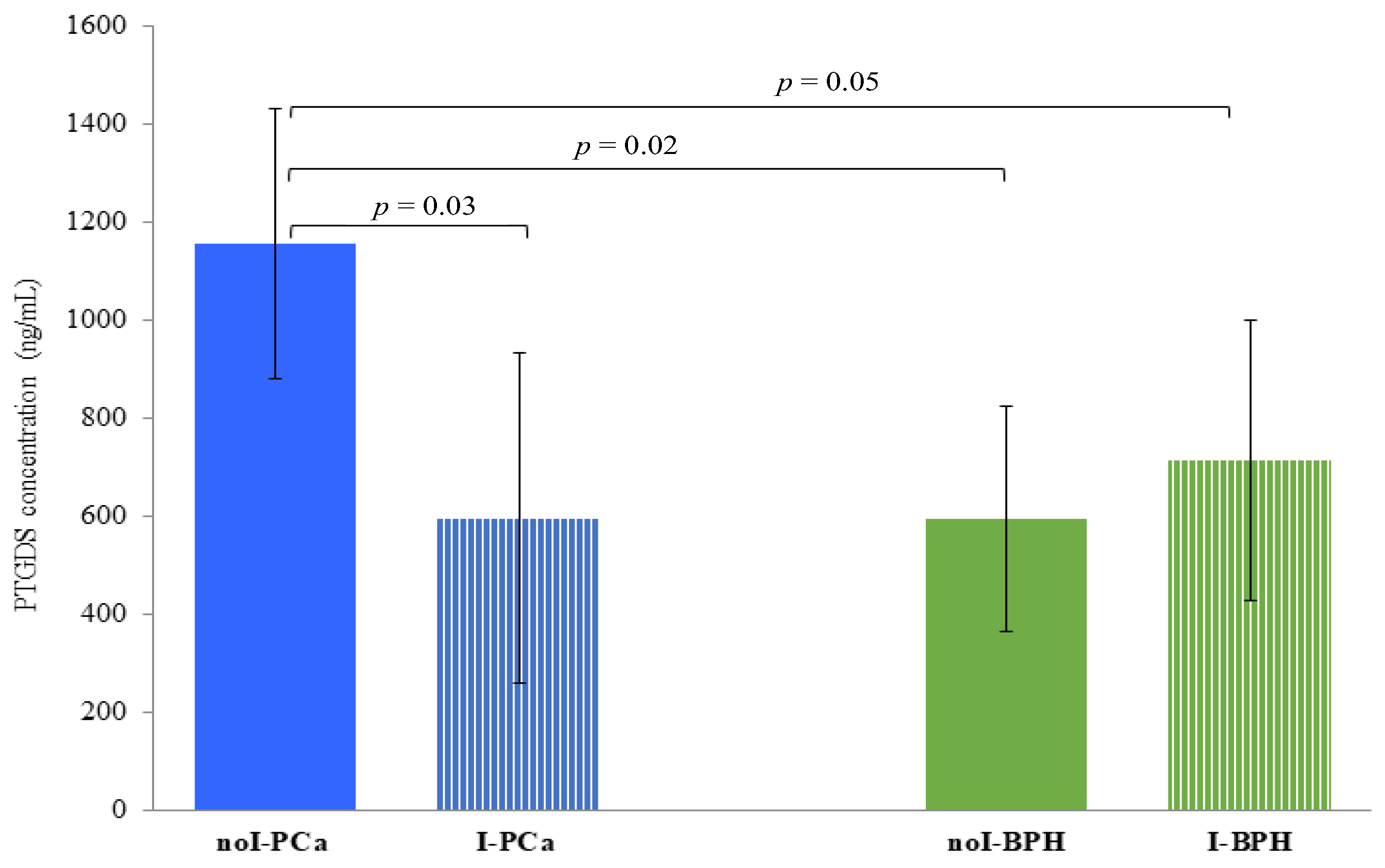
3.5. PTGDS Quantification by ELISA
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| A1AT | Alpha-1-antitrypsin |
| A1BG | Alpha-1-beta-glicoprotein |
| AACT | Alpha-1-antichymotrypsin |
| AMBP | Alpha-1-microglobulin |
| APOA1 | Apolipoprotein A1 |
| APPs | Acute phase proteins |
| BPH | Benign prostatic hyperplasia |
| 2-DE | Two-dimensional gel electrophoresis |
| H&E | Hematoxylin and eosin stain |
| HEMO | Hemopexin |
| HPT | Haptoglobin |
| I-BPH | BPH group with inflammation |
| I-PCa | PCa group with inflammation |
| noI-BPH | BPH group without inflammation |
| noI-PCa | PCa group without inflammation |
| PBx | Prostate needle biopsy |
| PCA | Prostate Cancer |
| PSA | Prostate-specific antigen |
| PTGDS | Prostaglandin-H2 D-isomerase |
| SAP3 | Ganglioside GM2 activator |
| TRFE | Serotransferrin |
| TTHY | Transthyretin |
References
- GLOBOCAN 2020, Cancer Today. International Agency for Research on Cancer. 2023. Available online: http://bit.ly/41XKskq (accessed on 16 March 2023).
- GLOBOCAN 2020, Cancer Tomorrow. International Agency for Research on Cancer. 2023. Available online: http://bit.ly/3YHDZYk (accessed on 16 March 2023).
- Hassanipour-Azgomi, S.; Mohammadian-Hafshejani, A.; Ghoncheh, M.; Towhidi, F.; Jamehshorani, S.; Salehiniya, H. Incidence and mortality of prostate cancer and their relationship with the Human Development Index worldwide. Prostate Int. 2016, 4, 118–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- GLOBOCAN 2020, Cancer Today. International Agency for Research on Cancer. 2023. Available online: http://bit.ly/3ymcAjT (accessed on 16 March 2023).
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer. 2015, 136, E359–E386. [Google Scholar] [CrossRef]
- Paulo, P.; Maia, S.; Pinto, C.; Pinto, P.; Monteiro, A.; Peixoto, A.; Teixeira, M.R. Targeted next generation sequencing identifies functionally deleterious germline mutations in novel genes in early-onset/familial prostate cancer. PLoS Genet. 2018, 14, e1007355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jia, G.; Dong, Z.; Sun, C.; Wen, F.; Wang, H.; Guo, H.; Gao, X.; Xu, C.; Xu, C.; Yang, C.; et al. Alterations in expressed prostate secretion-urine PSA N-glycosylation discriminate prostate cancer from benign prostate hyperplasia. Oncotarget 2017, 8, 76987–76999. [Google Scholar] [CrossRef] [Green Version]
- Rigau, M.; Olivan, M.; Garcia, M.; Sequeiros, T.; Montes, M.; Colas, E.; Llaurado, M.; Planas, J.; de Torres, I.; Morote, J.; et al. The present and future of prostate cancer urine biomarkers. Int. J. Mol. Sci. 2013, 14, 12620–12649. [Google Scholar] [CrossRef] [Green Version]
- McNally, C.J.; Ruddock, M.W.; Moore, T.; McKenna, D.J. Biomarkers that differentiate benign prostatic hyperplasia from prostate cancer: A literature review. Cancer Manag. Res. 2020, 12, 5225–5241. [Google Scholar] [CrossRef]
- Decramer, S.; Gonzalez de Peredo, A.; Breuil, B.; Mischak, H.; Monsarrat, B.; Bascands, J.-L.; Schanstra, J.P. Urine in clinical proteomics. Mol. Cell. Proteomics 2008, 7, 1850–1862. [Google Scholar] [CrossRef] [Green Version]
- Gopalan, G.; Rao, V.S.; Kakkar, V.V. An overview of urinary proteomics applications in human diseases. Int. J. High. Throughput Screen. 2010, 1, 183–192. [Google Scholar] [CrossRef] [Green Version]
- Crocetto, F.; Russo, G.; Di Zazzo, E.; Pisapia, P.; Mirto, B.F.; Palmieri, A.; Pepe, F.; Bellevicine, C.; Russo, A.; La Civita, E.; et al. Liquid biopsy in prostate cancer management—Current challenges and future perspectives. Cancers 2022, 14, 3272. [Google Scholar] [CrossRef] [PubMed]
- Crocetto, F.; Barone, B.; Caputo, V.F.; Fonatana, M.; de Cobelli, O.; Ferro, M. BRCA germline mutations in prostate cancer: The future is tailored. Diagnostics 2021, 11, 908. [Google Scholar] [CrossRef]
- Swensen, A.C.; He, J.; Fang, A.C.; Ye, Y.; Nicora, C.D.; Shi, T.; Liu, A.Y.; Sigdel, T.K.; Sarwal, M.M.; Qian, W.-J. A comprehensive urine proteome database generated from patients with various renal conditions and prostate cancer. Front. Med. 2021, 8, 548212. [Google Scholar] [CrossRef]
- Jedinak, A.; Loughlin, K.R.; Moses, M.A. Approaches to the discovery of non-invasive urinary biomarkers of prostate cancer. Oncotarget 2018, 9, 32534–32550. [Google Scholar] [CrossRef] [PubMed]
- Kowalewska, M.; Nowak, R.; Chechlinska, M. Implications of cancer-associated systemic inflammation for biomarkers study. Biochim. Biophys. Acta 2010, 1806, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Chechlinska, M.; Kowalewska, M.; Nowak, R. Systemic inflammation as a confounding factor in cancer biomarker discovery and validation. Nat. Rev. Cancer 2010, 10, 2–3. [Google Scholar] [CrossRef] [PubMed]
- Bergamini, S.; Bellei, E.; Reggiani Bonetti, L.; Monari, E.; Cuoghi, A.; Borelli, F.; Sighinolfi, M.C.; Bianchi, G.; Ozben, T.; Tomasi, A. Inflammation: An important parameter in the search of prostate cancer biomarkers. Proteome Sci. 2014, 12, 32. [Google Scholar] [CrossRef] [Green Version]
- Epstein, J.I.; Magi-Galluzzi, C.; Zhou, M.; Cubilla, A.L. Tumors of the Prostate Gland, Seminal Vesicles, Penis, and Scrotum; AFIP-ATLAS of Tumor and Non-Tumor Pathology; Series 5; American Registry of Pathology: Washington, DC, USA, 2020. [Google Scholar] [CrossRef]
- Epstein, J.I.; Amin, M.B.; Reuter, V.E.; Humphrey, P.A. Contemporary Gleason grading of prostatic carcinoma: An update with discussion on practical issues to implement the 2014 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma. Am. J. Surg. Pathol. 2017, 41, e1–e7. [Google Scholar] [CrossRef]
- Bradford, M.M. A rapid and sensitive method for the quantitation of microgram quantities of protein utilizing the principle of protein-dye binding. Anal. Biochem. 1976, 72, 248–254. [Google Scholar] [CrossRef]
- Bellei, E.; Bergamini, S.; Monari, E.; Fantoni, L.I.; Cuoghi, A.; Ozben, T.; Tomasi, A. High-abundance proteins depletion for serum proteomic analysis: Concomitant removal of non-targeted proteins. Amino Acids 2011, 40, 145–156. [Google Scholar] [CrossRef] [PubMed]
- Eklund, M.; Jäderling, F.; Discacciati, A.; Bergman, M.; Annerstedt, M.; Aly, M.; Glaessgen, A.; Carlsson, S.; Grönberg, H.; Nordström, T. MRI-targeted or standard biopsy in prostate cancer screening. N. Engl. J. Med. 2021, 385, 908–920. [Google Scholar] [CrossRef]
- Descotes, J.-L. Diagnosis of prostate cancer. Asian J. Urol. 2019, 6, 129–136. [Google Scholar] [CrossRef]
- Prensner, J.R.; Rubin, M.A.; Wei, J.T.; Chinnaiyan, A.M. Beyond PSA: The next generation of prostate cancer biomarkers. Sci. Transl. Med. 2012, 4, 127rv3. [Google Scholar] [CrossRef] [Green Version]
- Matuszczak, M.; Schalken, J.A.; Salagierski, M. Prostate cancer liquid biopsy biomarkers’ clinical utility in diagnosis and prognosis. Cancers 2021, 13, 3373. [Google Scholar] [CrossRef] [PubMed]
- Pin, E.; Fredolini, C.; Petricoin III, E.F. The role of proteomics in prostate cancer research: Biomarker discovery and validation. Clin. Biochem. 2013, 46, 524–538. [Google Scholar] [CrossRef] [PubMed]
- Haj-Ahmad, T.A.; Abdalla, M.A.K.; Haj-Ahmad, Y. Potential urinary protein biomarker candidates for the accurate detection of prostate cancer among benign prostatic hyperplasia patients. J. Cancer 2014, 5, 103–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sousa, A.P.; Costa, R.; Alves, M.G.; Soares, R.; Baylina, P.; Fernandes, R. The impact of metabolic syndrome and type 2 diabetes mellitus on prostate cancer. Front. Cell. Dev. Biol. 2022, 10, 843458. [Google Scholar] [CrossRef]
- De Nunzio, C.; Kramer, G.; Marberger, M.; Montironi, R.; Nelson, W.; Schröder, F.; Sciarra, A.; Tubaro, A. The controversial relationship between benign prostatic hyperplasia and prostate cancer: The role of inflammation. Eur. Urol. 2011, 60, 106–117. [Google Scholar] [CrossRef]
- Kruslin, B.; Tomas, D.; Dzombeta, T.; Milkovic-Perisa, M.; Ulamec, M. Inflammation in prostatic hyperplasia and carcinoma—Basic scientific approach. Front. Oncol. 2017, 7, 77. [Google Scholar] [CrossRef] [Green Version]
- Davalieva, K.; Kiprijanovska, S.; Komina, S.; Petrusevska, G.; Chokrevska Zografska, N.; Polenakovic, M. Proteomics analysis of urine reveals acute phase response proteins as candidate diagnostic biomarkers for prostate cancer. Proteome Sci. 2015, 13, 2. [Google Scholar] [CrossRef] [Green Version]
- Di Domenico, M.; Pozzi, D.; Palchetti, S.; Digiacomo, L.; Iorio, R.; Siciliano, C.; Pinto, F.; Settembre, G.; Pierdiluca, M.; Santini, M.; et al. Alpha-1-microglobulin/bikunin (AMBP) protein corona (PPC) as biomarker for early diagnosis in non-small-cell-lung carcinomas (NSCLC) patients: A case report. Meta Gene 2018, 17, S19. [Google Scholar] [CrossRef]
- Saraswat, M.; Joenväärä, S.; Seppänen, H.; Mustonen, H.; Haglund, C.; Renkonen, R. Comparative proteomic profiling of the serum differentiates pancreatic cancer from chronic pancreatitis. Cancer Med. 2017, 6, 1738–1751. [Google Scholar] [CrossRef]
- Kundu, M.; Mahata, B.; Banerjee, A.; Chakraborty, S.; Debnath, S.; Ray, S.S.; Ghosh, Z.; Biswas, K. Ganglioside GM2 mediates migration of tumor cells by interacting with integrin and modulating the downstream signaling pathway. Biochim. Biophys. Acta 2016, 1863, 1472–1489. [Google Scholar] [CrossRef]
- Shin, J.; Kim, G.; Lee, J.W.; Lee, J.E.; Kim, Y.S.; Yu, J.-H.; Lee, S.-T.; Ahn, S.H.; Kim, H.; Lee, C. Identification of ganglioside GM2 activator playing a role in cancer cell migration through proteomic analysis of breast cancer secretomes. Cancer Sci. 2016, 107, 828–835. [Google Scholar] [CrossRef] [Green Version]
- Sasaki, N.; Toyoda, M.; Ishiwata, T. Gangliosides as signaling regulators in cancer. Int. J. Mol. Sci. 2021, 22, 5076. [Google Scholar] [CrossRef]
- Siltari, A.; Syvälä, H.; Lou, Y.R.; Gao, Y.; Murtola, T.J. Role of lipids and lipid metabolism in prostate cancer progression and the tumor’s immune environment. Cancers 2022, 14, 4293. [Google Scholar] [CrossRef] [PubMed]
- Bergamini, S.; Caramaschi, S.; Monari, E.; Martorana, E.; Salviato, T.; Mangogna, A.; Balduit, A.; Tomasi, A.; Canu, P.; Bellei, E. Urinary proteomic profiles of prostate cancer with different risk of progression and correlation with histopathological features. Ann. Diagn. Pathol. 2021, 51, 151704. [Google Scholar] [CrossRef]
- Jin, Y.; Wang, W.; Wang, Q. Alpha-1-antichymotrypsin as a novel biomarker for diagnosis, prognosis, and therapy prediction in human diseases. Cancer Cell. Int. 2022, 22, 156. [Google Scholar] [CrossRef]
- Tian, M.; Cui, Y.Z.; Song, G.-H.; Zong, M.-J.; Zhou, X.-Y.; Chen, Y.; Han, J.-X. Proteomic analysis identifies MMP-9, DJ-1 and A1BG as overexpressed proteins in pancreatic juice from pancreatic ductal adenocarcinoma patients. BMC Cancer 2008, 8, 241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canales, N.A.G.; Marina, V.M.; Castro, J.S. A1BG and C3 are overexpressed in patients with cervical intraepithelial neoplasia III. Oncol. Lett. 2014, 8, 939–947. [Google Scholar] [CrossRef] [Green Version]
- Kreunin, P.; Zhao, J.; Rosser, C.; Urquidi, V.; Lubman, D.M.; Goodison, S. Bladder cancer associated glycoprotein signatures revealed by urinary proteomic profiling. J. Proteome Res. 2007, 6, 2631–2639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cordeiro, Y.G.; Mulder, L.M.; van Zeijl, R.J.M.; Paskoski, L.B.; van Veelen, P.; de Ru, A.; Strefezzi, R.F.; Heijs, B.; Fukumasu, H. Proteomic analysis identifies FNDC1, A1BG, and antigen processing proteins associated with tumor heterogeneity and malignancy in a canine model of breast cancer. Cancers 2021, 13, 5901. [Google Scholar] [CrossRef]
- Janciauskiene, S.; Wrenger, S.; Günzel, S.; Gründing, A.R.; Golpon, H.; Welte, T. Potential roles of acute phase proteins in cancer: Why do cancer cells produce or take up exogenous acute phase protein alpha-1-antitrypsin? Front. Oncol. 2021, 11, 622076. [Google Scholar] [CrossRef] [PubMed]
- Dong, M.; Lih, T.M.; Chen, S.-Y.; Cho, K.-C.; Eguez, R.V.; Höti, N.; Zhou, Y.; Yang, W.; Mangold, L.; Chan, D.W.; et al. Urinary glycoproteins associated with aggressive prostate cancer. Theranostics 2020, 10, 11892–11907. [Google Scholar] [CrossRef]
- Alaiya, A.A.; Al-Mohanna, M.; Aslam, M.; Shinwari, Z.; Al-Mansouri, L.; Al-Rodayan, M.; Al-Eid, M.; Ahmad, I.; Hanash, K.; Tulbah, A.; et al. Proteomics-based signature for human benign prostate hyperplasia and prostate adenocarcinoma. Int. J. Oncol. 2011, 38, 1047–1057. [Google Scholar] [CrossRef] [PubMed]
- Davalieva, K.; Kiprijanovska, S.; Kostovska, I.M.; Stavridis, S.; Stankov, O.; Komina, S.; Petrusevska, G.; Polenakovic, M. Comparative proteomics analysis of urine reveals down-regulation of acute phase response signaling and LXR/RXR activation pathways in prostate cancer. Proteomes 2018, 6, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Falagario, U.; Selvaggio, O.; Carrieri, G.; Barret, E.; Sanguedolce, F.; Cormio, L. Prostatic inflammation is associated with benign prostatic hyperplasia rather than prostate cancer. J. Gerontol. Geriatr. 2018, 66, 178–182. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups | Age (Years) Median (Range) | Grade Group | PSA (ng/mL) Median (Range) | PSA Comparisons |
|---|---|---|---|---|
| PCa (n = 30) | 68 | G < 7 (n = 14) | 5.80 | PCa vs. BPH, p = 0.03 |
| (59–73) | G ≥ 7 (n = 16) | (0.80–34.36) | ||
| noI-PCa (n = 10) | 68.5 | G < 7 (n = 5) | 5.95 | noI-PCa vs. noI-BPH, p = 0.02 |
| (62–73) | G ≥ 7 (n = 5) | (4.49–34.00) | ||
| I-PCa (n = 20) | 67 | G < 7 (n = 9) | 5.49 | I-PCa vs. I-BPH, p > 0.05 |
| (59–73) | G ≥ 7 (n = 11) | (0.80–34.36) | I-PCa vs. noI-PCa, p > 0.05 | |
| BPH (n = 30) | 68 | - | 3.60 | |
| (59–81) | - | (0.20–25.00) | ||
| noI-BPH (n = 11) | 67 | - | 3.65 | |
| (59–77) | - | (0.20–6.80) | ||
| I-BPH (n = 19) | 69 | - | 3.60 | I-BPH vs. noI-BPH, p > 0.05 |
| (60–81) | - | (0.40–25.00) |
| Groups | Concentration (μg/μL) | Group Comparisons | p-Value |
|---|---|---|---|
| Pca | 1.57 ± 0.48 | Pca vs. BPH | p < 0.001 |
| noI-Pca | 1.74 ± 0.49 | noI-Pca vs. noI-BPH | p ≤ 0.05 |
| I-Pca | 1.49 ± 0.26 | I-Pca vs. I-BPH | p ≤ 0.05 |
| I-Pca vs. noI-PCa | p > 0.05 | ||
| BPH | 4.06 ± 0.57 | ||
| noI-BPH | 2.72 ± 0.34 | ||
| I-BPH | 4.77 ± 1.22 | I-BPH vs. noI-BPH | p ≤ 0.05 |
| Entry Name a | Protein Name b | Acc. No. c | MW (Da) d | Fold-Change of Protein Expression e | |||
|---|---|---|---|---|---|---|---|
| PCa vs. BPH e1 | noI-PCa vs. noI-BPH e2 | I-PCa vs. noI-Pca e3 | I-BPH vs. noI-BPH e4 | ||||
| AMBP1 | Alpha-1-microglobulin | P02760 | 39,886 | +4.40 | +2.39 | −1.51 | −2.28 |
| AMBP2 | Alpha-1-microglobulin | P02760 | 39,886 | +2.06 | +2.70 | −1.64 | −1.83 |
| SAP3 | Ganglioside GM2 activator | P17900 | 21,281 | +3.80 | +2.18 | −1.53 | −2.09 |
| AACT1 | Alpha-1-antichymotrypsin | P01011 | 47,792 | −7.91 | −5.39 | −1.77 | +4.23 |
| AACT2 | Alpha-1-antichymotrypsin | P01011 | 47,792 | −1.50 | / | −2.78 | +3.99 |
| A1BG | Alpha-1-beta-glicoprotein | P04217 | 54,790 | −5.44 | −2.60 | +4.50 | +6.69 |
| TRFE | Serotransferrin | P02787 | 79,294 | −2.18 | ND | ND | +2.14 |
| A1AT1 | Alpha-1-antitrypsin | P01009 | 46,878 | −6.02 | / | / | +2.19 |
| A1AT2 | Alpha-1-antitrypsin | P01009 | 46,878 | −6.31 | −1.91 | +2.11 | +6.35 |
| A1AT3 | Alpha-1-antitrypsin | P01009 | 46,878 | −2.57 | ND | +1.75 | +2.53 |
| A1AT4 | Alpha-1-antitrypsin | P01009 | 46,878 | −1.50 | ND | +1.86 | / |
| A1AT5 | Alpha-1-antitrypsin | P01009 | 46,878 | −10.90 | −2.55 | +3.56 | +10.3 |
| A1AT6 | Alpha-1-antitrypsin | P01009 | 46,878 | −2.32 | −2.30 | +10.8 | +1.61 |
| HPT1 | Haptoglobin | P00738 | 45,861 | −3.34 | / | +2.27 | +2.16 |
| HPT2 | Haptoglobin | P00738 | 45,861 | −2.02 | / | +1.61 | +3.11 |
| APOA11 | Apolipoprotein A1 | P02647 | 30,759 | −6.67 | / | ND | / |
| APOA12 | Apolipoprotein A1 | P02647 | 30,759 | −10.40 | −3.68 | ND | / |
| TTHY | Transthyretin | P02766 | 15,991 | −3.45 | / | ND | +3.46 |
| PTGDS | Prostaglandin-H2 D-isomerase | P41222 | 21,243 | ND | +6.53 | −2.79 | / |
| HEMO | Hemopexin | P02790 | 52,385 | ND | ND | ND | +2.52 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bellei, E.; Caramaschi, S.; Giannico, G.A.; Monari, E.; Martorana, E.; Reggiani Bonetti, L.; Bergamini, S. Research of Prostate Cancer Urinary Diagnostic Biomarkers by Proteomics: The Noteworthy Influence of Inflammation. Diagnostics 2023, 13, 1318. https://doi.org/10.3390/diagnostics13071318
Bellei E, Caramaschi S, Giannico GA, Monari E, Martorana E, Reggiani Bonetti L, Bergamini S. Research of Prostate Cancer Urinary Diagnostic Biomarkers by Proteomics: The Noteworthy Influence of Inflammation. Diagnostics. 2023; 13(7):1318. https://doi.org/10.3390/diagnostics13071318
Chicago/Turabian StyleBellei, Elisa, Stefania Caramaschi, Giovanna A. Giannico, Emanuela Monari, Eugenio Martorana, Luca Reggiani Bonetti, and Stefania Bergamini. 2023. "Research of Prostate Cancer Urinary Diagnostic Biomarkers by Proteomics: The Noteworthy Influence of Inflammation" Diagnostics 13, no. 7: 1318. https://doi.org/10.3390/diagnostics13071318