
Validation of a Machine Learning Expert Supporting System, ImmunoGenius, Using Immunohistochemistry Results of 3000 Patients with Lymphoid Neoplasms
 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
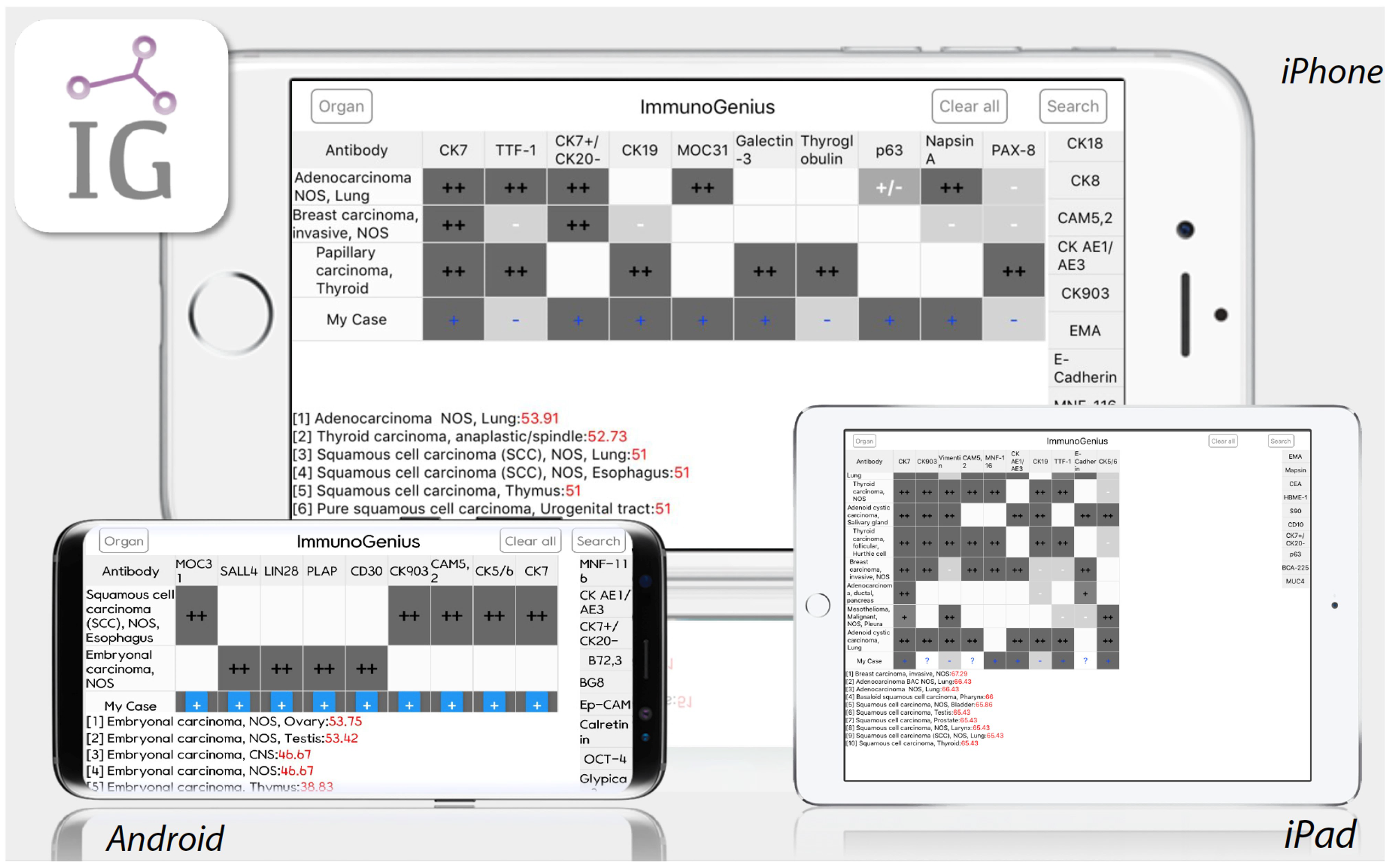
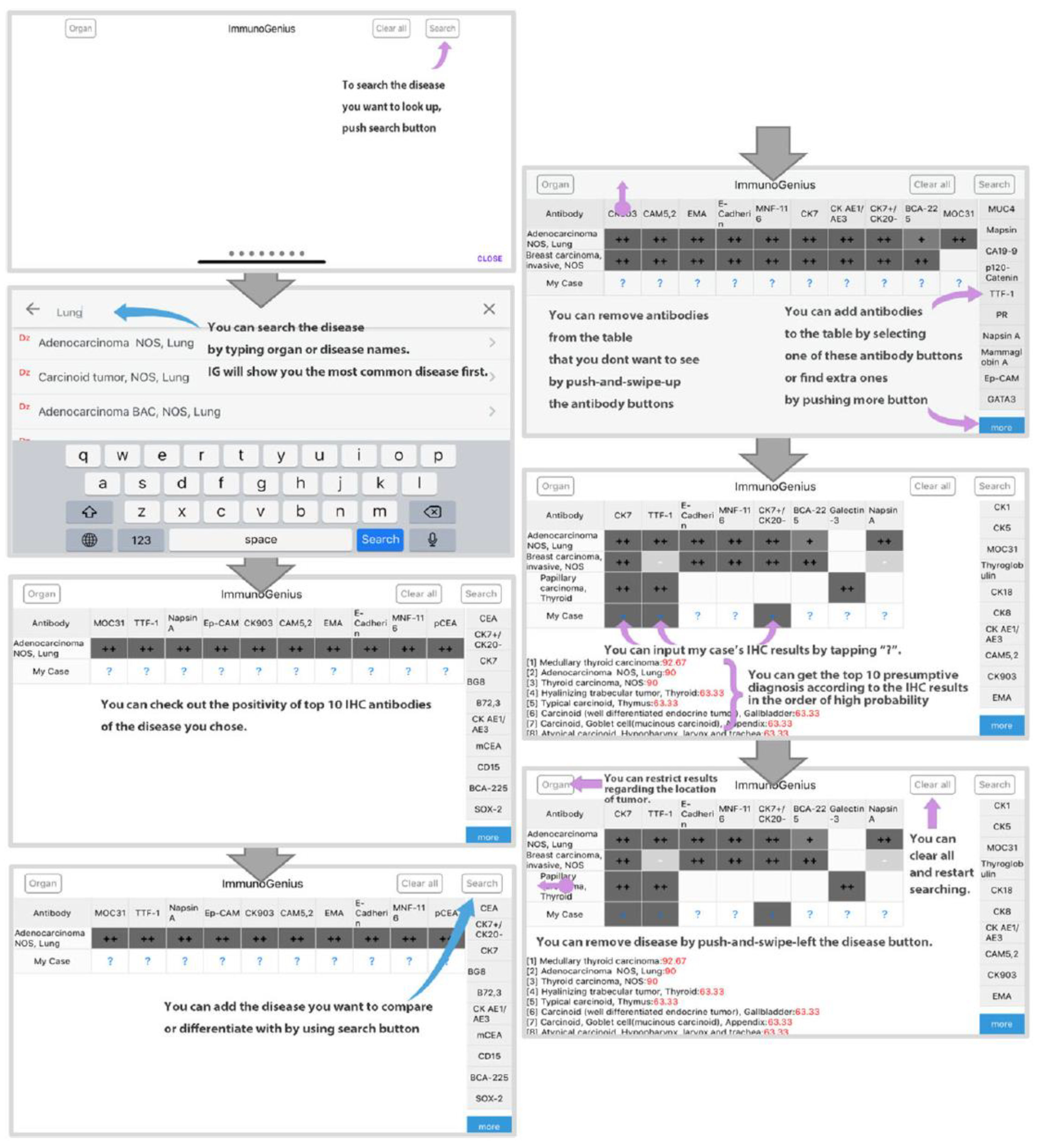
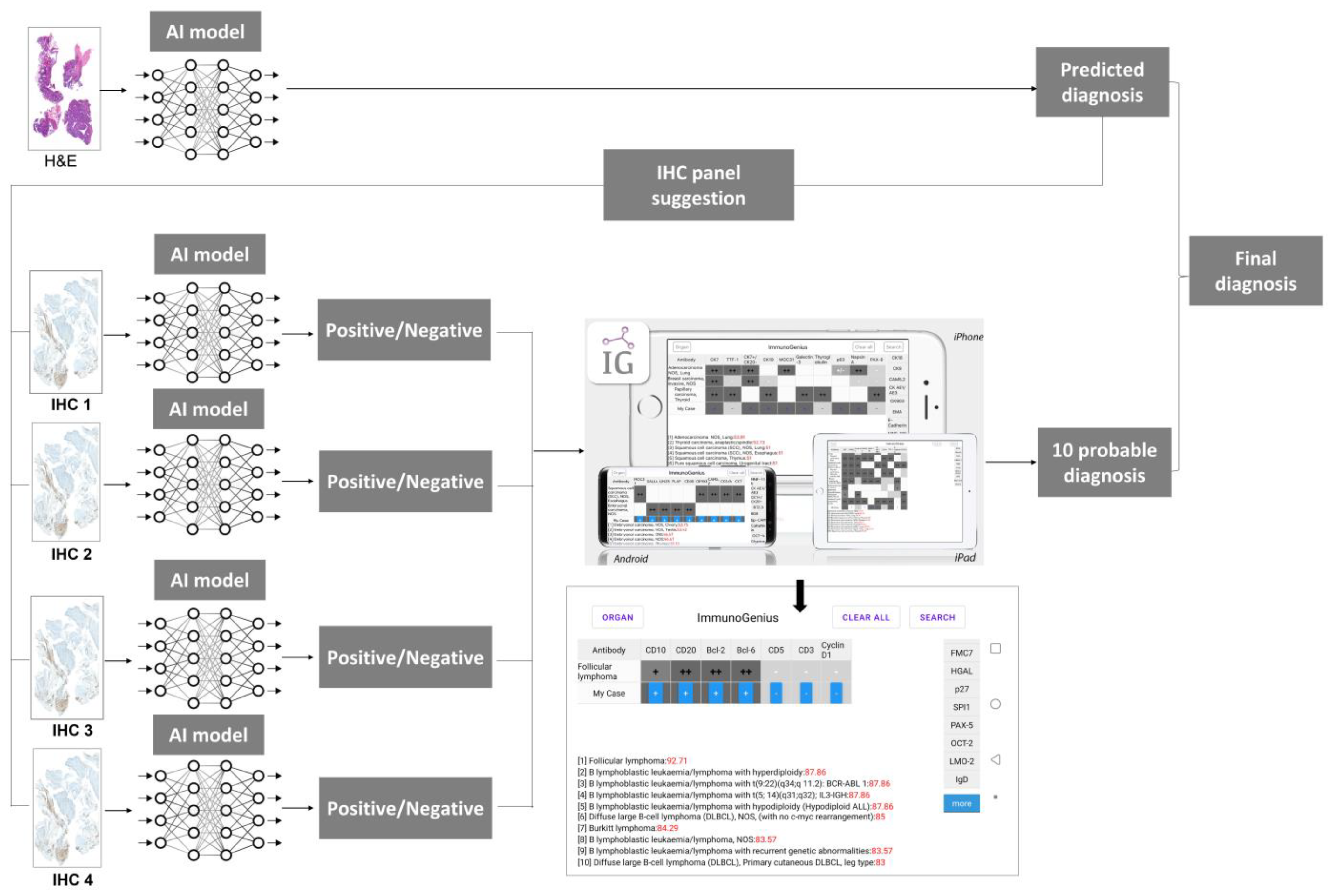
2.1. Machine-Learning Expert Supporting System, ImmunoGenius
2.2. External Validation Using Nationwide IHC Dataset of Lymphoid Neoplasms
2.3. Statistical Analysis
3. Results
3.1. External Validation Data Characteristics
3.2. External Validation Results
3.3. The Presumptive Error Rates between Training, Validation, External Validation Datasets, and Performance in Computational Time
4. Discussion
4.1. Contribution of the Study
4.2. Limitations of the Study
4.3. Future Direction
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Patents
References
- Buchwalow, I.B.; Böcker, W. Immunohistochemistry: Basics and Methods, 1st ed.; Springer: Berlin/Heidelberg, Germany, 2010. [Google Scholar]
- Chong, Y.; Lee, J.Y.; Kim, Y.; Choi, J.; Yu, H.; Park, G.; Cho, M.Y.; Thakur, N. A machine-learning expert-supporting system for diagnosis prediction of lymphoid neoplasms using a probabilistic decision-tree algorithm and immunohistochemistry profile database. J. Pathol. Transl. Med. 2020, 54, 462–470. [Google Scholar] [CrossRef]
- David, J.D. Diagnostic Immunohistochemistry E-Book: Theranostic and Genomic Applications; Elsevier: Amsterdam, The Netherlands, 2022. [Google Scholar]
- Elias, J.M. Immunohistochemistry: A brief historical perspective. J. Histotechnol. 1999, 22, 163–167. [Google Scholar] [CrossRef]
- Kalyuzhny, A.E. Immunohistochemistry: Essential Elements and Beyond, 1st ed.; Springer: Cham, Switzerland, 2016. [Google Scholar]
- Matos, L.L.; Trufelli, D.C.; de Matos, M.G.; da Silva Pinhal, M.A. Immunohistochemistry as an important tool in biomarkers detection and clinical practice. Biomark. Insights 2010, 5, 9–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chong, Y.; Thakur, N.; Lee, J.Y.; Hwang, G.; Choi, M.; Kim, Y.; Yu, H.; Cho, M.Y. Diagnosis prediction of tumours of unknown origin using ImmunoGenius, a machine learning-based expert system for immunohistochemistry profile interpretation. Diagn. Pathol. 2021, 16, 19. [Google Scholar] [CrossRef] [PubMed]
- DeYoung, B.R.; Wick, M.R. Immunohistologic evaluation of metastatic carcinomas of unknown origin: An algorithmic approach. Semin. Diagn. Pathol. 2000, 17, 184–193. [Google Scholar]
- Werner, B.; Campos, A.C.; Nadji, M.; Torres, L.F.B. Practical use of immunohistochemistry in surgical pathology. J. Bras. Patol. Med. Lab. 2005, 41, 353–364. [Google Scholar] [CrossRef]
- Chu, P.; Weiss, L.M. Modern Immunohistochemistry, 2nd ed.; Cambridge University Press: Cambridge, UK, 2014. [Google Scholar]
- Bishop, J.A.; Sharma, R.; Illei, P.B. Napsin A and thyroid transcription factor-1 expression in carcinomas of the lung, breast, pancreas, colon, kidney, thyroid, and malignant mesothelioma. Hum. Pathol. 2010, 41, 20–25. [Google Scholar] [CrossRef]
- El-Maqsoud, N.M.; Tawfiek, E.R.; Abdelmeged, A.; Rahman, M.F.; Moustafa, A.A. The diagnostic utility of the triple markers Napsin A, TTF-1, and PAX8 in differentiating between primary and metastatic lung carcinomas. Tumour. Biol. 2016, 37, 3123–3134. [Google Scholar] [CrossRef]
- Gweon, H.M.; Kim, J.A.; Youk, J.H.; Hong, S.W.; Lim, B.J.; Yoon, S.O.; Park, Y.M.; Son, E.J. Can galectin-3 be a useful marker for conventional papillary thyroid microcarcinoma? Diagn. Cytopathol. 2016, 44, 103–107. [Google Scholar] [CrossRef]
- Kandalaft, P.L.; Gown, A.M. Practical Applications in Immunohistochemistry: Carcinomas of Unknown Primary Site. Arch Pathol. Lab. Med. 2016, 140, 508–523. [Google Scholar] [CrossRef] [Green Version]
- Yu, H.; Li, L.; Liu, D.; Li, W.M. Expression of TTF-1, NapsinA, P63, CK5/6 in Lung Cancer and Its Diagnostic Values for Histological Classification. Sichuan Da Xue Xue Bao Yi Xue Ban 2017, 48, 336–341. [Google Scholar] [PubMed]
- Nam, S.; Chong, Y.; Jung, C.K.; Kwak, T.Y.; Lee, J.Y.; Park, J.; Rho, M.J.; Go, H. Introduction to digital pathology and computer-aided pathology. J. Pathol. Transl. Med. 2020, 54, 125–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, F.; Prichard, J. Handbook of Practical Immunohistochemistry: Frequently Asked Questions; Springer: New York, NY, USA, 2015. [Google Scholar]
- Jung, H.R.; Huh, J.; Ko, Y.H.; Jeon, Y.K.; Yoon, S.O.; Kim, S.H.; Yang, W.I.; Park, G.; Kim, J.H.; Paik, J.H. Classification of malignant lymphoma subtypes in Korean patients: A report of the 4th nationwide study. J. Hematop. 2019, 12, 173–181. [Google Scholar] [CrossRef]
- Rekhtman, N.; Bishop, J.A. Quick Reference Handbook for Surgical Pathologists; Springer: Berlin/Heidelberg, Germany, 2011. [Google Scholar]
- Swerdlow, S.H.; Campo, E.; Harris, N.L.; Jaffe, E.S.; Pileri, S.A.; Stein, H.; Thiele, J.; Vardiman, J.W. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues; International Agency for Research on Cancer: Lyon, France, 2008; Volume 2. [Google Scholar]
- Dorfman, D.M.; Brown, J.A.; Shahsafaei, A.; Freeman, G.J. Programmed death-1 (PD-1) is a marker of germinal center-associated T cells and angioimmunoblastic T-cell lymphoma. Am. J. Surg. Pathol. 2006, 30, 802–810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El Achi, H.; Belousova, T.; Chen, L.; Wahed, A.; Wang, I.; Hu, Z.; Kanaan, Z.; Rios, A.; Nguyen, A.N. Automated diagnosis of lymphoma with digital pathology images using deep learning. Ann. Clin. Lab. Sci. 2019, 49, 153–160. [Google Scholar]
- Mohlman, J.S.; Leventhal, S.D.; Hansen, T.; Kohan, J.; Pascucci, V.; Salama, M.E. Improving augmented human intelligence to distinguish Burkitt lymphoma from diffuse large B-cell lymphoma cases. Am. J. Clin. Pathol. 2020, 153, 743–759. [Google Scholar] [CrossRef]
- Li, D.; Bledsoe, J.R.; Zeng, Y.; Liu, W.; Hu, Y.; Bi, K.; Liang, A.; Li, S. A deep learning diagnostic platform for diffuse large B-cell lymphoma with high accuracy across multiple hospitals. Nat. Commun. 2020, 11, 6004. [Google Scholar] [CrossRef]
- Khan, A.; Brouwer, N.; Blank, A.; Müller, F.; Soldini, D.; Noske, A.; Gaus, E.; Brandt, S.; Nagtegaal, I.; Dawson, H. Computer-Assisted Diagnosis of Lymph Node Metastases in Colorectal Cancers Using Transfer Learning with an Ensemble Model. Mod. Pathol. 2023, 36, 100118. [Google Scholar] [CrossRef]
- Das, P.K.; Meher, S. An efficient deep convolutional neural network based detection and classification of acute lymphoblastic leukemia. Expert Syst. Appl. 2021, 183, 115311. [Google Scholar] [CrossRef]
- Das, P.K.; Sahoo, B.; Meher, S. An Efficient Detection and Classification of Acute Leukemia using Transfer Learning and Orthogonal Softmax Layer-based Model. IEEE/ACM Trans. Comput. Biol. Bioinform. 2022, 1–9. [Google Scholar] [CrossRef]
- Das, P.K.; Meher, S.; Panda, R.; Abraham, A. An efficient blood-cell segmentation for the detection of hematological disorders. IEEE Trans. Cybern. 2021, 52, 10615–10626. [Google Scholar] [CrossRef] [PubMed]
- Sahu, A.; Das, P.K.; Meher, S. High accuracy hybrid CNN classifiers for breast cancer detection using mammogram and ultrasound datasets. Biomed. Signal Process. Control 2023, 80, 104292. [Google Scholar] [CrossRef]
- Bucolo, M.; Fortuna, L.; Nelke, M.; Rizzo, A.; Sciacca, T. Prediction models for the corrosion phenomena in Pulp & Paper plant. Control Eng. Pract. 2002, 10, 227–237. [Google Scholar]
- Kim, H.; Yoon, H.; Thakur, N.; Hwang, G.; Lee, E.J.; Kim, C.; Chong, Y. Deep learning-based histopathological segmentation for whole slide images of colorectal cancer in a compressed domain. Sci. Rep. 2021, 11, 22520. [Google Scholar] [CrossRef]
- Varlatzidou, A.; Pouliakis, A.; Stamataki, M.; Meristoudis, C.; Margari, N.; Peros, G.; Panayiotides, J.G.; Karakitsos, P. Cascaded learning vector quantizer neural networks for the discrimination of thyroid lesions. Anal. Quant. Cytol. Histol. 2011, 33, 323–334. [Google Scholar]
- Gopinath, B. A benign and malignant pattern identification in cytopathological images of thyroid nodules using gabor filter and neural networks. Asian J. Converg. Technol. (AJCT) 2018, 4. [Google Scholar]
- Bejnordi, B.E.; Veta, M.; Van Diest, P.J.; Van Ginneken, B.; Karssemeijer, N.; Litjens, G.; Van Der Laak, J.A.; Hermsen, M.; Manson, Q.F.; Balkenhol, M. Diagnostic assessment of deep learning algorithms for detection of lymph node metastases in women with breast cancer. Jama 2017, 318, 2199–2210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teramoto, A.; Tsukamoto, T.; Kiriyama, Y.; Fujita, H. Automated classification of lung cancer types from cytological images using deep convolutional neural networks. Bio. Med. Res. Int. 2017, 2017, 4067832. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| No. | Name of the Institute | No. of Cases |
|---|---|---|
| 1 | Ajou University Hospital | 456 |
| 2 | Asan Medical Center | 113 |
| 3 | Chonnam National University Hwasun Hospital | 434 |
| 4 | Chonnam National University Hospital | 146 |
| 5 | Dong-A University Hospital | 117 |
| 6 | Eulji University Hospital | 61 |
| 7 | Ewha Womans University Mokdong Hospital | 83 |
| 8 | Gyeongsang National University | 102 |
| 9 | Gyeongsang National University Changwon Hospital | 35 |
| 10 | Hallym University Sacred Heart Hospital | 93 |
| 11 | Inje University Haeundae Paik Hospital | 117 |
| 12 | Inje University Sanggye Paik Hospital | 49 |
| 13 | Jeonbuk National University Hospital | 206 |
| 14 | Keimyung University Dongsan Medical Center | 137 |
| 15 | Konkuk University Hospital | 58 |
| 16 | Korea University Guro Hospital | 160 |
| 17 | Kosin University Gospel Hospital | 95 |
| 18 | Nowon Eulji Medical Center, Eulji University | 16 |
| 19 | Presbyterian Medical Center | 74 |
| 20 | Seoul Metropolitan Government-Seoul National University Boramae Medical Center | 152 |
| 21 | Soonchunhyang University Bucheon Hospital | 112 |
| 22 | Soonchunhyang University Seoul Hospital | 59 |
| 23 | The Catholic University of Korea, Seoul St. Mary’s Hospital | 591 |
| 24 | The Catholic University of Korea, Yeouido St. Mary’s Hospital | 59 |
| 25 | Ulsan University Hospital | 197 |
| Total No. of cases | 3722 |
| Type of Lymphoma | Training Data | Validation Data | External Validation Data | |||
|---|---|---|---|---|---|---|
| Error/No. | % | Error/No. | % | Error/No. | % | |
| B lymphoblastic leukemia/lymphoma | 0/8 | 0 | 0/5 | 0 | 1/20 | 5.0 |
| Chronic lymphocytic leukemia/small lymphocytic lymphoma | 0/20 | 0 | 0/11 | 0 | 1/57 | 1.8 |
| Extranodal marginal zone lymphoma of MALT (lymphoma) | 0/78 | 0 | 0/74 | 0 | 63/436 | 14.4 |
| Nodal marginal zone lymphoma | 0/4 | 0 | 0/5 | 0 | 11/36 | 30.5 |
| Plasma cell myeloma | 0/3 | 0 | 0/0 | 0 | 4/31 | 12.9 |
| Follicular lymphoma | 0/62 | 0 | 0/22 | 0 | 11/203 | 5.4 |
| Mantle cell lymphoma | 1/24 | 4.2 | 0/19 | 0 | 1/73 | 1.4 |
| DLBCL | ||||||
| -NOS | 0/216 | 0 | 0/145 | 0 | 56/1239 | 4.5 |
| -T-cell/histiocyte-rich | 0/2 | 0 | 0/0 | 0 | 0/7 | 0.0 |
| -Primary DLBCL of the CNS | 0/9 | 0 | 0/0 | 0 | 3/60 | 5.0 |
| -Associated with chronic inflammation | - | - | - | - | 0/2 | 0.0 |
| -EBV positive DLBCL of elderly | 0/1 | 0 | 0/0 | 0 | 2/29 | 6.9 |
| -Primary cutaneous DLBCL, leg type | 0/0 | 0 | 0/1 | 0 | 0/3 | 0.0 |
| Primary mediastinal (thymic) large B-cell lymphoma | 0/9 | 0 | 0/3 | 0 | 5/29 | 17.2 |
| Plasmablastic lymphoma | 3/3 | 100 | 0/0 | 0 | 7/11 | 63.6 |
| Primary effusion lymphoma | 0/1 | 0 | 0/0 | 0 | 0/1 | 0.0 |
| Burkitt lymphoma | 0/17 | 0 | 0/11 | 0 | 0/42 | 0.0 |
| B-cell lymphoma, unclassifiable, with features intermediate between DLBCL and Burkitt lymphoma | 0/3 | 0 | 0/0 | 0 | 10/13 | 76.9 |
| Primary cutaneous follicle center lymphoma | 0/0 | 0 | 1/2 | 50 | 2/4 | 50.0 |
| T lymphoblastic leukemia/lymphoma | 0/17 | 0 | 0/7 | 0 | 1/44 | 2.3 |
| Extranodal NK/T-cell lymphoma. nasal type | 0/25 | 0 | 0/15 | 0 | 8/121 | 6.6 |
| Adult T-cell leukemia/ lymphoma | 1/1 | 100 | 0/0 | 0 | 1/2 | 50.0 |
| Enteropathy-associated T-cell lymphoma | ||||||
| -Type 1 | - | - | - | - | 2/2 | 100.0 |
| -Type 2 | - | - | - | - | 5/16 | 31.3 |
| Mycosis fungoides | 0/0 | 0 | 0/3 | 0 | 3/22 | 13.6 |
| Primary cutaneous (CD30-positive T-cell) ALCL | 0/1 | 0 | 0/0 | 0 | 6/12 | 50.0 |
| Primary cutaneous gamma-delta T-cell lymphoma | - | - | - | - | 1/1 | 100.0 |
| Subcutaneous panniculitis-like T-cell lymphoma | 0/0 | 0 | 0/1 | 0 | 2/6 | 33.3 |
| Peripheral T-cell lymphoma, NOS | 9/23 | 34.7 | 4.12 | 33.3 | 13/103 | 12.6 |
| Angioimmunoblastic T-cell lymphoma | 8/16 | 50 | 3/7 | 42.8 | 12/110 | 10.9 |
| ALCL, ALK-positive | 0/5 | 0 | 0/2 | 0 | 0/33 | 0.0 |
| ALCL, ALK-negative | 3/9 | 33.3 | 2/6 | 33.3 | 6/37 | 16.2 |
| Nodular lymphocyte-predominant Hodgkin lymphoma | 0/0 | 0 | 1/2 | 50 | 4/6 | 66.7 |
| Classical Hodgkin lymphoma, NOS | 1/8 | 12.5 | 2/11 | 18.2 | 3/16 | 18.8 |
| Nodular sclerosis classical Hodgkin lymphoma | 3/21 | 14.3 | 1/5 | 20 | 12/69 | 17.3 |
| Mixed cellularity classical Hodgkin lymphoma | 0/7 | 0 | 0/8 | 0 | 9/63 | 14.2 |
| Hepatosplenic T-cell lymphoma | - | - | - | - | 1/1 | 100.0 |
| Lymphocyte rich Classical HL | - | - | - | - | 2/15 | 13.3 |
| Lymphomatoid granulomatosis | - | - | - | - | 3/4 | 75.0 |
| Lymphoplasmacytic lymphoma | - | - | - | - | 2/6 | 33.3 |
| Primary cutaneous CD4 positive small/mediumT-cell lymphoma | - | - | - | - | 3/4 | 75.0 |
| Splenic B-cell lymphoma/leukemia, unclassifiable | - | - | - | - | 0/1 | 0.0 |
| Splenic B-cell marginal zone lymphoma | - | - | - | - | 1/1 | 100.0 |
| Systemic EBV+ T-cell lymphoproliferative disease of childhood | - | - | - | - | 1/2 | 50.0 |
| Total | 32/602 | 5.3 | 17/392 | 4.3 | 278/2993 | 9.2 |
| Precision Diagnosis | Training Data (%) | Validation Data (%) | External Validation Data (%) | Total (%) |
|---|---|---|---|---|
| Accurate results | 570 (94.7) | 365 (95.7) | 2715 (90.7) | 3650 (91.8) |
| Error results | 32 (5.3) | 17 (4.3) | 278 (9.3) | 327 (8.2) |
| Total | 602 (100) | 382 (100) | 2993 (100) | 3977 (100) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdul-Ghafar, J.; Seo, K.J.; Jung, H.-R.; Park, G.; Lee, S.-S.; Chong, Y. Validation of a Machine Learning Expert Supporting System, ImmunoGenius, Using Immunohistochemistry Results of 3000 Patients with Lymphoid Neoplasms. Diagnostics 2023, 13, 1308. https://doi.org/10.3390/diagnostics13071308
Abdul-Ghafar J, Seo KJ, Jung H-R, Park G, Lee S-S, Chong Y. Validation of a Machine Learning Expert Supporting System, ImmunoGenius, Using Immunohistochemistry Results of 3000 Patients with Lymphoid Neoplasms. Diagnostics. 2023; 13(7):1308. https://doi.org/10.3390/diagnostics13071308
Chicago/Turabian StyleAbdul-Ghafar, Jamshid, Kyung Jin Seo, Hye-Ra Jung, Gyeongsin Park, Seung-Sook Lee, and Yosep Chong. 2023. "Validation of a Machine Learning Expert Supporting System, ImmunoGenius, Using Immunohistochemistry Results of 3000 Patients with Lymphoid Neoplasms" Diagnostics 13, no. 7: 1308. https://doi.org/10.3390/diagnostics13071308