
Training and External Validation of a Predict Nomogram for Type 2 Diabetic Peripheral Neuropathy

Abstract
:1. Introduction
2. Methods
2.1. Study Design and Population
2.2. Data Collection
2.3. Training and Assessment of the Nomogram
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
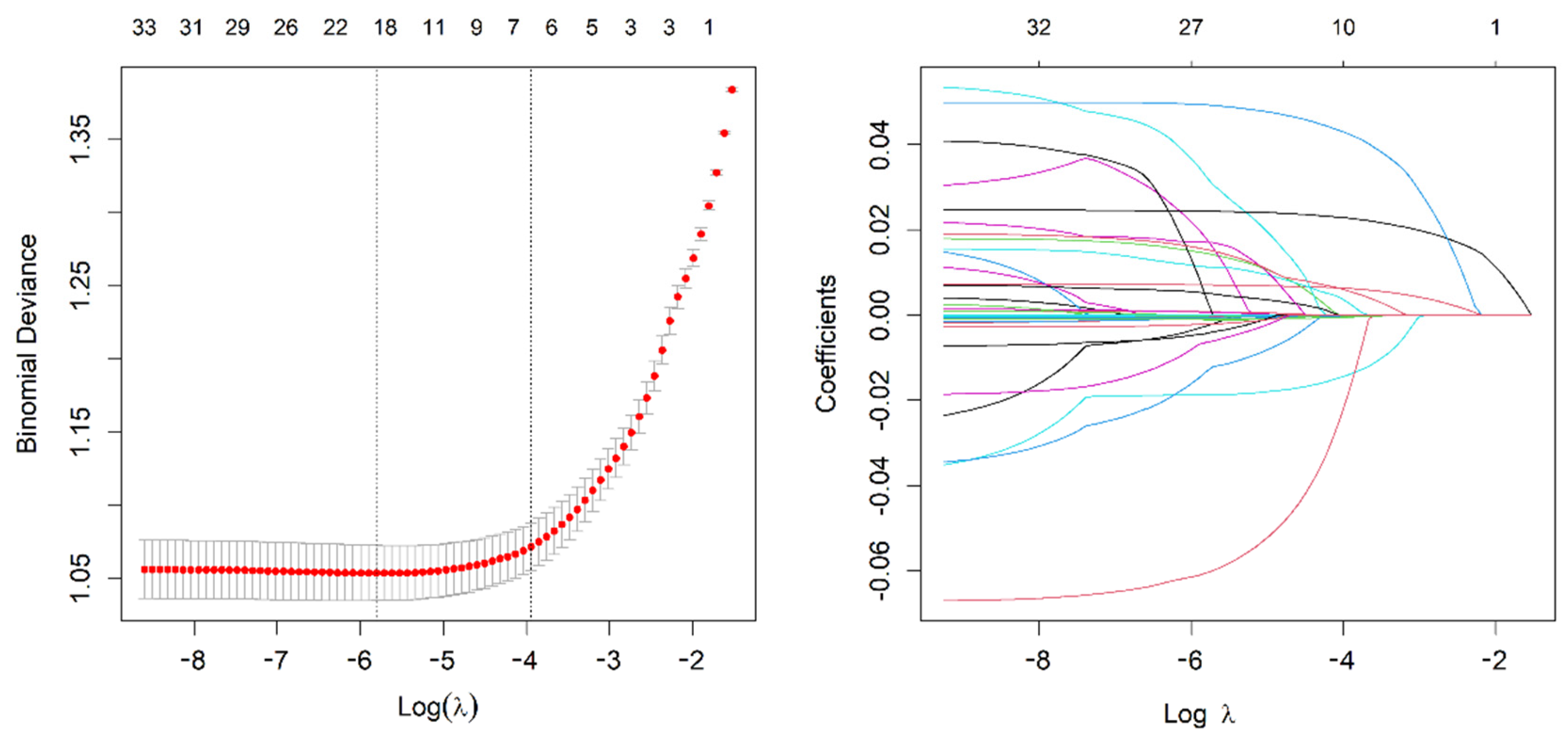
3.2. Screening for Predictive Factors
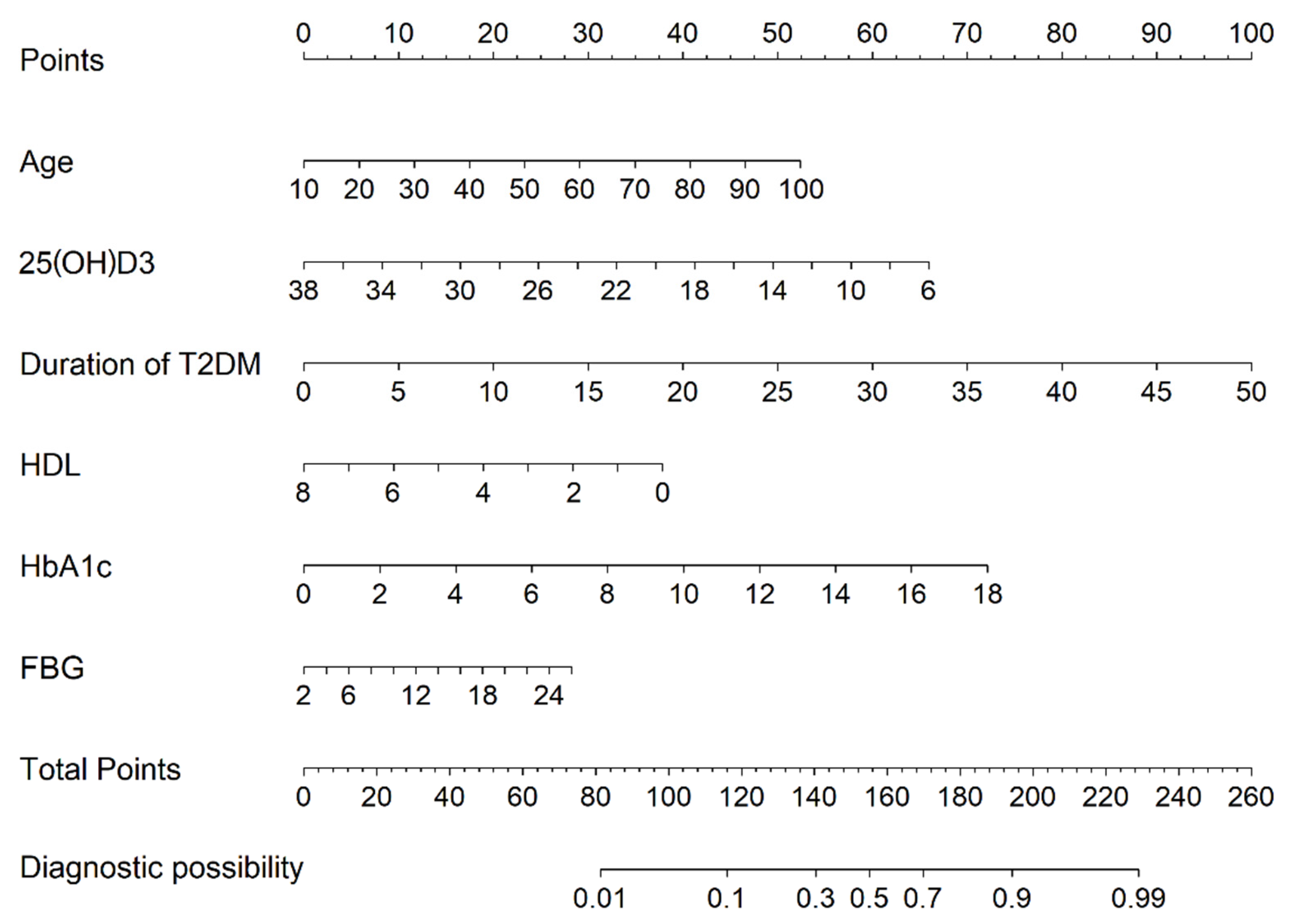
3.3. Risk Prediction Nomogram Development
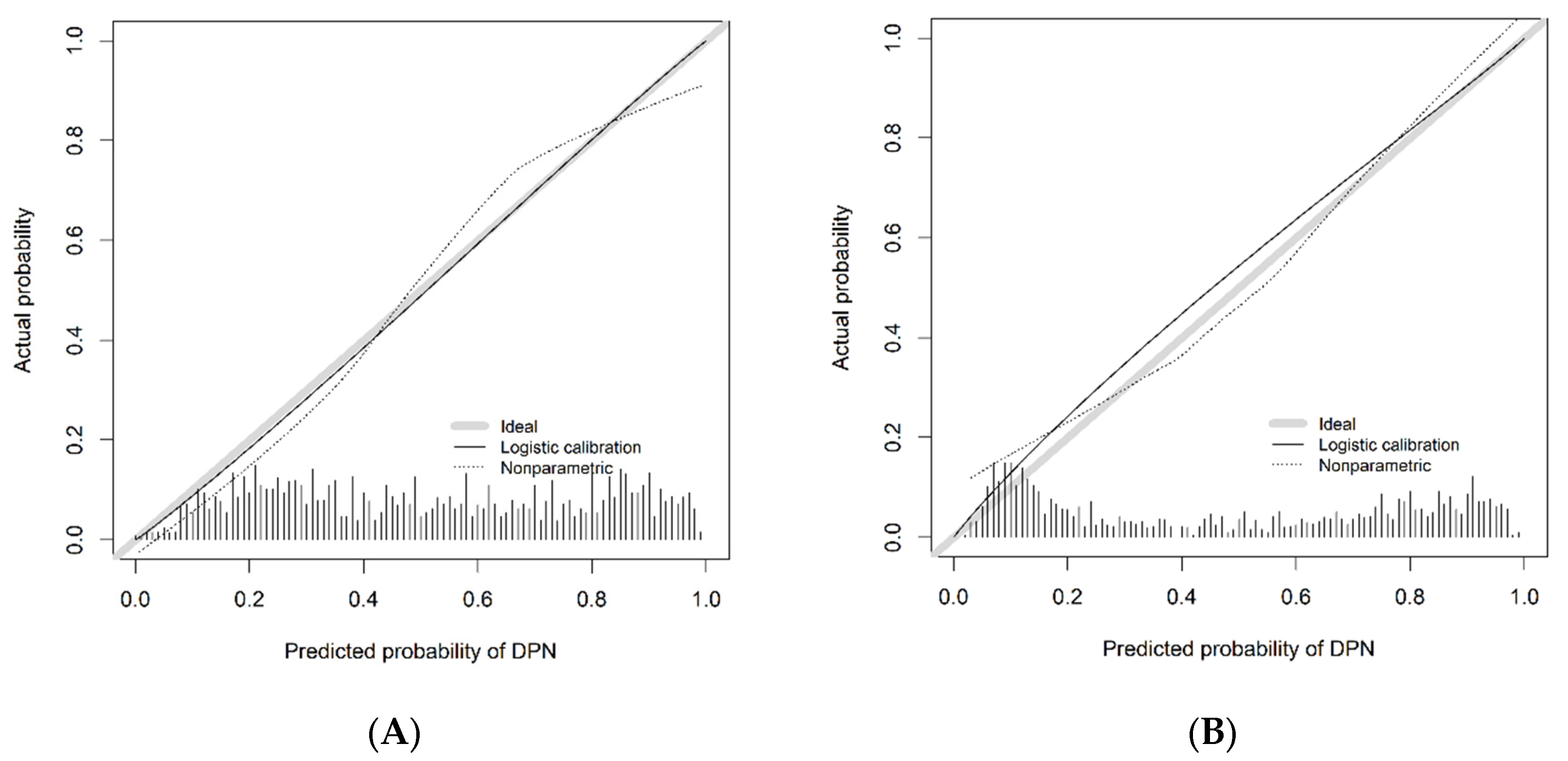
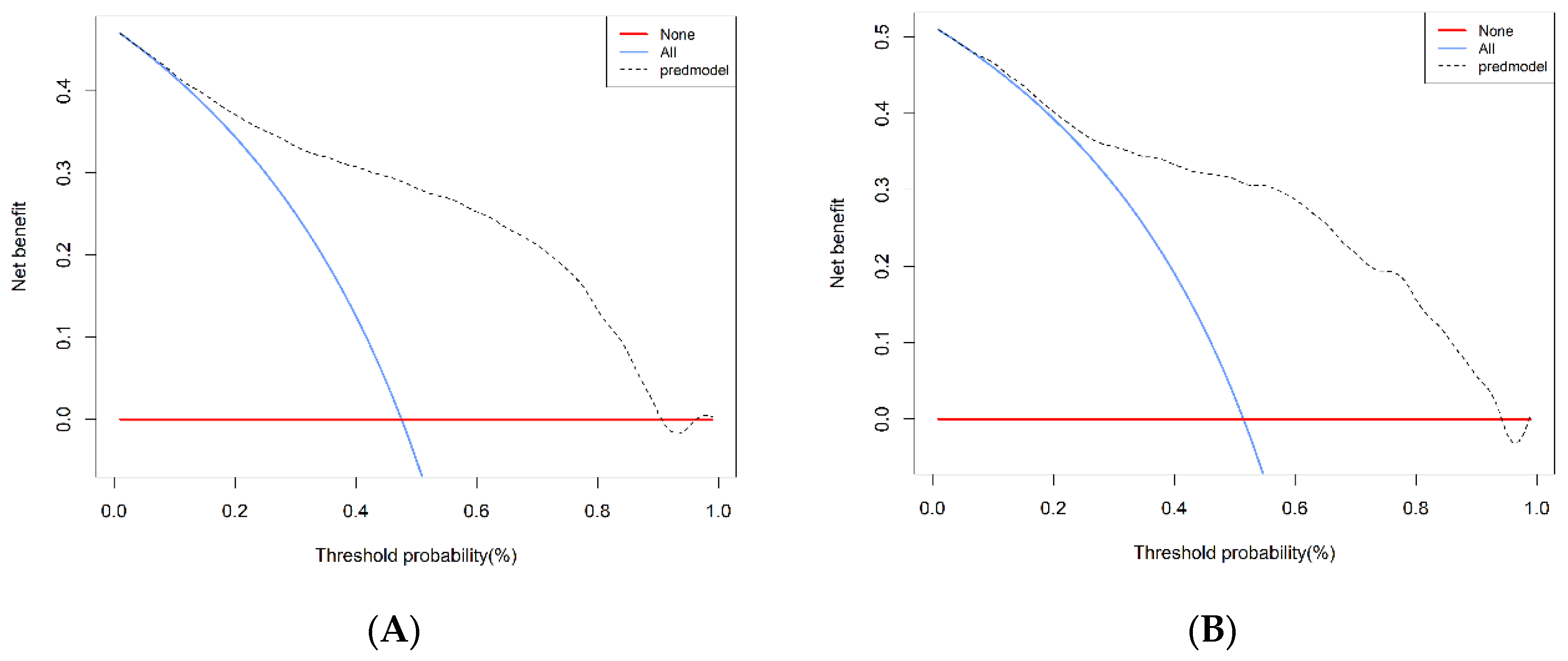
3.4. Predictive Accuracy and Net Benefit of the Nomogram
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lin, X.; Xu, Y.; Pan, X.; Xu, J.; Ding, Y.; Sun, X.; Song, X.; Ren, Y.; Shan, P.F. Global, regional, and national burden and trend of diabetes in 195 countries and territories: An analysis from 1990 to 2025. Sci. Rep. 2020, 10, 14790. [Google Scholar] [CrossRef] [PubMed]
- IDF Congress 2019: Shaping the future of diabetes. Diabetes Res. Clin. Pract. 2019, 158, 107954. [CrossRef] [PubMed]
- Zhu, Y.T.; Hu, P.; Chen, J.; Wang, L.; Dong, H.; Zhu, Z.Y.; Wang, Y.F. Analysis of Related Factors in Diabetic Peripheral Neuropathy. Neural Inj. Funct. Reconstr. 2019, 14, 622–625. [Google Scholar] [CrossRef]
- Jaiswal, M.; Divers, J.; Dabelea, D.; Isom, S.; Bell, R.A.; Martin, C.L.; Pettitt, D.J.; Saydah, S.; Pihoker, C.; Standiford, D.A.; et al. Prevalence of and Risk Factors for Diabetic Peripheral Neuropathy in Youth with Type 1 and Type 2 Diabetes: SEARCH for Diabetes in Youth Study. Diabetes Care 2017, 40, 1226–1232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, R.; Santana, T.; Schillinger, D.; Hecht, F.M.; Chao, M.T. “It Gave Me Hope” Experiences of Diverse Safety Net Patients in a Group Acupuncture Intervention for Painful Diabetic Neuropathy. Health Equity 2020, 4, 225–231. [Google Scholar] [CrossRef]
- Selvarajah, D.; Kar, D.; Khunti, K.; Davies, M.J.; Scott, A.R.; Walker, J.; Tesfaye, S. Diabetic peripheral neuropathy: Advances in diagnosis and strategies for screening and early intervention. Lancet Diabetes Endocrinol. 2019, 7, 938–948. [Google Scholar] [CrossRef] [Green Version]
- Ristikj-Stomnaroska, D.; Risteska-Nejashmikj, V.; Papazova, M. Role of Inflammation in the Pathogenesis of Diabetic Peripheral Neuropathy. Open Access Maced. J. Med. Sci. 2019, 7, 2267–2270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azoulay, D.; Abed, S.; Sfadi, A.; Sheleg, O.; Shaoul, E.; Shehadeh, M.; Kaykov, E.; Nodelman, M.; Bashkin, A. Low brain-derived neurotrophic factor protein levels and single-nucleotide polymorphism Val66Met are associated with peripheral neuropathy in type II diabetic patients. Acta Diabetol. 2020, 57, 891–898. [Google Scholar] [CrossRef] [PubMed]
- Mallet, M.-L.; Hadjivassiliou, M.; Sarrigiannis, P.G.; Zis, P. The Role of Oxidative Stress in Peripheral Neuropathy. J. Mol. Neurosci. 2020, 70, 1009–1017. [Google Scholar] [CrossRef]
- Aleidan, F.A.S.; Ahmad, B.A.; Alotaibi, F.A.; Aleesa, D.H.; Alhefdhi, N.A.; Badri, M.; Abdel Gader, A.G. Prevalence and Risk Factors for Diabetic Peripheral Neuropathy Among Saudi Hospitalized Diabetic Patients: A Nested Case-Control Study. Int. J. Gen. Med. 2020, 13, 881–889. [Google Scholar] [CrossRef]
- Zhao, W.-J.; Xia, X.-Y.; Yin, J. Relationship of serum vitamin D levels with diabetic microvascular complications in patients with type 2 diabetes mellitus. Chin. Med. J. 2021, 134, 814–820. [Google Scholar] [CrossRef] [PubMed]
- Gylfadottir, S.S.; Christensen, D.H.; Nicolaisen, S.K.; Andersen, H.; Callaghan, B.C.; Itani, M.; Khan, K.S.; Kristensen, A.G.; Nielsen, J.S.; Sindrup, S.H.; et al. Diabetic polyneuropathy and pain, prevalence, and patient characteristics: A cross-sectional questionnaire study of 5,514 patients with recently diagnosed type 2 diabetes. Pain 2019, 161, 574–583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Li, C.; Zhao, S.; Yin, Y.; Zhang, X.; Wang, K. Nomogram for Prediction of Diabetic Retinopathy Among Type 2 Diabetes Population in Xinjiang, China. Diabetes Metab. Syndr. Obes. Targets Ther. 2022, 15, 1077–1089. [Google Scholar] [CrossRef]
- Yang, J.; Song, X.; Lai, Y.; Zhao, W.; Zhou, J.; Liu, Q.; Li, W.; Zhang, H.; Wang, H.; Shi, P.; et al. Development and validation of a postoperative nomogram for predicting overall survival after endoscopic surgical management of olfactory neuroblastoma. Eclinicalmedicine 2020, 29–30, 100577. [Google Scholar] [CrossRef]
- Chinese Diabetes Society. Guideline for the prevention and treatment of type 2 diabetes mellitus in China (2013 edition). Chin. J. Diabetes Mellit. 2014, 6, 447–498. [Google Scholar] [CrossRef]
- Pavlou, M.; Ambler, G.; Seaman, S.; De Iorio, M.; Omar, R.Z. Review and evaluation of penalised regression methods for risk prediction in low-dimensional data with few events. Stat. Med. 2015, 35, 1159–1177. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Li, J.; Guo, J.; Shi, Y.; Wang, L. A prediction nomogram for neonatal acute respiratory distress syndrome in late-preterm infants and full-term infants: A retrospective study. Eclinicalmedicine 2022, 50, 101523. [Google Scholar] [CrossRef]
- Huang, Y.; Li, W.; Macheret, F.; Gabriel, R.A.; Ohno-Machado, L. A tutorial on calibration measurements and calibration models for clinical prediction models. J. Am. Med. Inform. Assoc. 2020, 27, 621–633. [Google Scholar] [CrossRef]
- Fitzgerald, M.; Saville, B.R.; Lewis, R.J. Decision Curve Analysis. JAMA 2015, 313, 409–410. [Google Scholar] [CrossRef]
- Shehab, D.; Al-Jarallah, K.; Mojiminiyi, O.A.; Al Mohamedy, H.; Abdella, N.A. Does Vitamin D deficiency play a role in peripheral neuropathy in Type 2 diabetes? Diabet. Med. 2011, 29, 43–49. [Google Scholar] [CrossRef]
- Halawa, M.R.; Ahmed, I.Z.; Abouelezz, N.F.; Mohamed, N.R.; Khalil, N.H.A.; Hendawy, L.M.A. The impact of vitamin D supplementation on peripheral neuropathy in a sample of Egyptian prediabetic individuals. F1000Research 2021, 10, 817. [Google Scholar] [CrossRef]
- Dou, X.J.; Wang, Q.Z.; Han, X.H.; Guo, Y.M.; Hao, H.B.; Zhang, Y.; Lin, R.H.; Ma, A.G. Effect of high dosage of vitamin D3 supplementation on lymphocyte proliferation activity in diabetic rats. Chin. Pharmacol. Bull. 2016, 32, 589–590. [Google Scholar] [CrossRef]
- Filipović, N.; Ferhatović, L.; Marelja, I.; Puljak, L.; Grković, I. Increased vitamin D receptor expression in dorsal root ganglia neurons of diabetic rats. Neurosci. Lett. 2013, 549, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Zheng, H.; Sun, W.; Zhang, Q.; Zhang, Y.; Ji, L.; Liu, X.; Zhu, X.; Ye, H.; Xiong, Q.; Li, Y.; et al. Proinflammatory cytokines predict the incidence of diabetic peripheral neuropathy over 5 years in Chinese type 2 diabetes patients: A prospective cohort study. Eclinicalmedicine 2020, 31, 100649. [Google Scholar] [CrossRef]
- Kabadi, S.M.; Liu, L.; Auchincloss, A.H.; Zakeri, I.F. Multivariate Path Analysis of Serum 25-Hydroxyvitamin D Concentration, Inflammation, and Risk of Type 2 Diabetes Mellitus. Dis. Mrk. 2013, 35, 187–193. [Google Scholar] [CrossRef]
- Khandoker, A.H.; Al-Angari, H.M.; Khalaf, K.; Lee, S.; Almahmeed, W.; Al Safar, H.S.; Jelinek, H.F. Association of diabetes related complications with heart rate variability among a diabetic population in the UAE. PLoS ONE 2017, 12, e0168584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mao, F.; Zhu, X.; Liu, S.; Qiao, X.; Zheng, H.; Lu, B.; Li, Y. Age as an Independent Risk Factor for Diabetic Peripheral Neuropathy in Chinese Patients with Type 2 Diabetes. Aging Dis. 2019, 10, 592–600. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Chen, J.; Wang, J.; Cai, D. Prevalence and risk factors of diabetic peripheral neuropathy in Type 2 diabetes mellitus patients with overweight/obese in Guangdong province, China. Prim. Care Diabetes 2015, 9, 191–195. [Google Scholar] [CrossRef]
- Baderca, F.; Timar, B.; Popescu, S.; Simu, M.; Diaconu, L.; Velea, I.; Timar, R. Age as an independent factor for the development of neuropathy in diabetic patients. Clin. Interv. Aging 2016, 11, 313–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skalli, S.; Muller, M.; Pradines, S.; Halimi, S.; Wion-Barbot, N. Vitamin D deficiency and peripheral diabetic neuropathy. Eur. J. Intern. Med. 2012, 23, e67–e68. [Google Scholar] [CrossRef]
- Xu, J.C.; Hu, H.L.; Ding, W. Association between level of vitamin D in serum and peripheral neuropathy in elderly patients with type 2 diabetes. J. Shanghai Jiaotong Univ. 2017, 37, 684–688. [Google Scholar] [CrossRef]
- Li, Y.S.; Zhang, X.L.; Li, C.; Feng, Z.W.; Wang, K. A Predictive Nomogram for the Risk of Peripheral Neuropathy in Type 2 Diabetes. Chinese General Practice. 2022, 25, 675–681. [Google Scholar] [CrossRef]
- Zhang, Y.; Shen, X.; Yan, S.; Jiang, Y. Can both normal and mildly abnormal albuminuria and glomerular filtration rate be a danger signal for diabetic peripheral neuropathy in type 2 diabetes mellitus? Neurol. Sci. 2017, 38, 1381–1390. [Google Scholar] [CrossRef]
- Tian, L.; Wang, X.L.; Su, X.H.; Sun, K. Three year follow-up study T2DM patients with blood glucose control in Shihezi community. J. Shihezi Univ. (Nat. Sci.) 2018, 36, 21–26. [Google Scholar] [CrossRef]
- Yang, L.; Shao, J.; Bian, Y.; Wu, H.; Shi, L.; Zeng, L.; Li, W.; Dong, J. Prevalence of type 2 diabetes mellitus among inland residents in China (2000–2014): A meta-analysis. J. Diabetes Investig. 2016, 7, 845–852. [Google Scholar] [CrossRef] [Green Version]
- Yang, H.; Shi, R.; Zhu, J.F.; Jia, L.L.; Lou, J.Q.; Long, W.; Feng, Y.; Liang, C.; Zhang, S.B.; Song, D.P.; et al. Existing circumstances research of diabetic peripheral neuropathy of type 2 diabetes mellitus patients based on community population in Shanghai. Chin. Gen. Pract. 2017, 20, 579–585. [Google Scholar] [CrossRef]
- He, Y. Relevant Factor Analysis in Diabetic Peripheral Neuropathy. Master’s thesis, Soochow University, Suzhou, China, 2016. [Google Scholar] [CrossRef]
- Li, M. Analysis of high risk factors of diabetic peripheral neuropathy. Med. J. Commun. 2018, 32, 580–581, 584. [Google Scholar]
- Huang, K.M.; Liu, B.; Zhao, Z. Analysis of electroneurophysiological and correlation factor in 114 patients with type 2 diabetes. Chin. J. Pract. Nerv. Dis. 2016, 3, 17–18. [Google Scholar] [CrossRef]
- Han, X.F.; Zhang, H.H.; Hu, J. Relationships between Inflam mation and Diabetic Neuropathy. Med. Recapitul. 2016, 22, 4585–4589. [Google Scholar] [CrossRef]
- Wang, J.Q.; Liu, Y.; Yu, S.J. Effects of Qidantongluo particles on nerve conduction velocity and levels of MDA, SOD and TAOC in diabetic peripheral neuropathy patients. Chin. J. Biochem. Pharm. 2016, 36, 93–95. [Google Scholar]
- Dai, D.; Shen, Y.; Lu, J.; Wang, Y.; Zhu, W.; Bao, Y.; Hu, G.; Zhou, J. Association between visit-to-visit variability of glycated albumin and diabetic retinopathy among patients with type 2 diabetes—A prospective cohort study. J. Diabetes Its Complicat. 2021, 35, 107971. [Google Scholar] [CrossRef] [PubMed]
- Ye, Z.; Li, X.; Han, Y.; Wu, Y.; Fang, Y. Association of long-term exposure to PM2.5 with hypertension and diabetes among the middle-aged and elderly people in Chinese mainland: A spatial study. BMC Public Health 2022, 22, 1–13. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Training Cohort (n = 3012) Mean (SD)/N (%) | Validation Cohort (n = 901) Mean (SD)/N (%) | p |
|---|---|---|---|
| DPN (%) | 0.003 | ||
| No | 1462 (48.5%) | 489 (54.3%) | |
| Yes | 1550 (51.5%) | 412 (45.7%) | |
| Gender | 0.381 | ||
| Male | 1867 (62.0%) | 573 (63.6%) | |
| Female | 1145 (38.0%) | 328 (36.4%) | |
| Age (years) | 57.123 (12.234) | 56.600 (12.032) | 0.259 |
| WBC (×109) | 7.085 (2.395) | 7.183 (2.845) | 0.305 |
| Neutrophil (×109) | 4.212 (2.024) | 4.301 (2.206) | 0.257 |
| Eosinophil (×109) | 0.171 (0.161) | 0.163 (0.133) | 0.172 |
| Lymphocyte (×109) | 2.168 (0.762) | 2.160 (0.802) | 0.788 |
| Hemoglobin (g/L) | 138.426 (18.945) | 138.410 (19.365) | 0.981 |
| Platelet (×109) | 228.204 (67.877) | 223.174 (66.781) | 0.050 |
| TC (mmol/L) | 4.244 (1.149) | 4.203 (1.057) | 0.331 |
| HDL (mmol/L) | 1.108 (0.359) | 1.089 (0.347) | 0.160 |
| LDL (mmol/L) | 2.704 (0.889) | 2.717 (0.874) | 0.686 |
| DB (U/L) | 3.594 (2.051) | 3.664 (2.309) | 0.389 |
| TB (U/L) | 11.477 (5.730) | 11.839 (6.139) | 0.102 |
| AST (U/L) | 21.035 (14.277) | 21.801 (16.145) | 0.171 |
| ALT (U/L) | 25.506 (21.686) | 26.677 (22.417) | 0.158 |
| BMI (kg/m2) | 26.145 (3.797) | 26.018 (3.780) | 0.379 |
| SBP (mmHg) | 127.893 (16.966) | 126.882 (16.226) | 0.113 |
| DBP (mmHg) | 77.181 (10.099) | 77.068 (9.875) | 0.767 |
| Duration of T2DM | 8.351 (7.213) | 8.255 (7.406) | 0.728 |
| Scr (μmol/L) | 74.457 (30.558) | 72.665 (32.855) | 0.129 |
| HbA1c (%) | 8.748 (2.125) | 8.643 (2.183) | 0.196 |
| GSP (%) | 2.772 (0.716) | 2.743 (0.698) | 0.283 |
| ApoA1 (g/L) | 1.170 (0.253) | 1.158 (0.249) | 0.210 |
| ApoB (g/L) | 0.932 (0.288) | 0.926 (0.279) | 0.621 |
| BG (mmol/L) | 9.521 (4.844) | 9.872 (5.485) | 0.064 |
| FBG (mmol/L) | 8.867 (3.023) | 8.762 (2.849) | 0.354 |
| PBG (mmol/L) | 18.012 (4.528) | 18.048 (4.533) | 0.835 |
| TG (mmol/L) | 2.310 (2.270) | 2.333 (2.020) | 0.788 |
| BUN (mmol/L) | 6.981 (16.624) | 6.198 (8.054) | 0.172 |
| UACR (mg/g) | 38.52 ± 33.109 | 41.803 ± 37.233 | 0.011 |
| 25 (OH)D3 (ng/mL) | 16.491 (8.908) | 15.908 (6.823) | 0.073 |
| Cys C (mg/L) | 2.332 (0.839) | 2.227 (0.798) | 0.081 |
| Hcy (μmol/L) | 12.713 (2.841) | 12.871 (2.632) | 0.137 |
| Variables | OR | 95% CI | p |
|---|---|---|---|
| Age | 1.243 | (1.235, 1.252) | <0.001 |
| 25(OH)D3 | 0.807 | (0.754, 0.851) | <0.001 |
| Duration of T2DM | 1.351 | (1.304, 1.379) | <0.001 |
| HDL | 0.903 | (0.854, 0.957) | <0.001 |
| HbA1c | 1.309 | (1.251, 1.372) | <0.001 |
| FBG | 1.06 | (1.027, 1.094) | 0.003 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Y.; Li, Y.; Deng, N.; Shi, H.; Caika, S.; Sen, G. Training and External Validation of a Predict Nomogram for Type 2 Diabetic Peripheral Neuropathy. Diagnostics 2023, 13, 1265. https://doi.org/10.3390/diagnostics13071265
Li Y, Li Y, Deng N, Shi H, Caika S, Sen G. Training and External Validation of a Predict Nomogram for Type 2 Diabetic Peripheral Neuropathy. Diagnostics. 2023; 13(7):1265. https://doi.org/10.3390/diagnostics13071265
Chicago/Turabian StyleLi, Yongsheng, Yongnan Li, Ning Deng, Haonan Shi, Siqingaowa Caika, and Gan Sen. 2023. "Training and External Validation of a Predict Nomogram for Type 2 Diabetic Peripheral Neuropathy" Diagnostics 13, no. 7: 1265. https://doi.org/10.3390/diagnostics13071265