
Carotid Artery Stenting Using Five-French Distal Radial Vascular Access
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
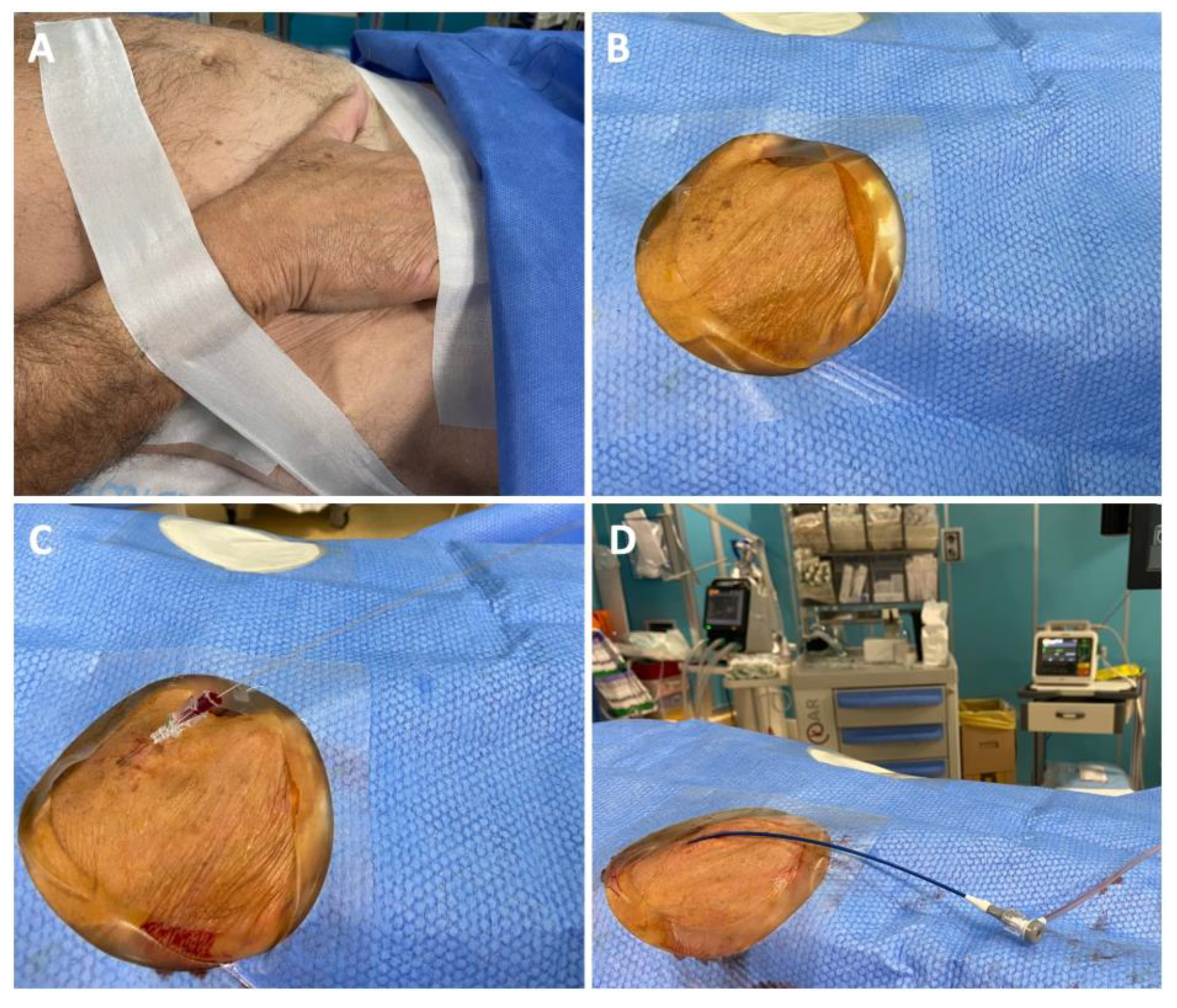
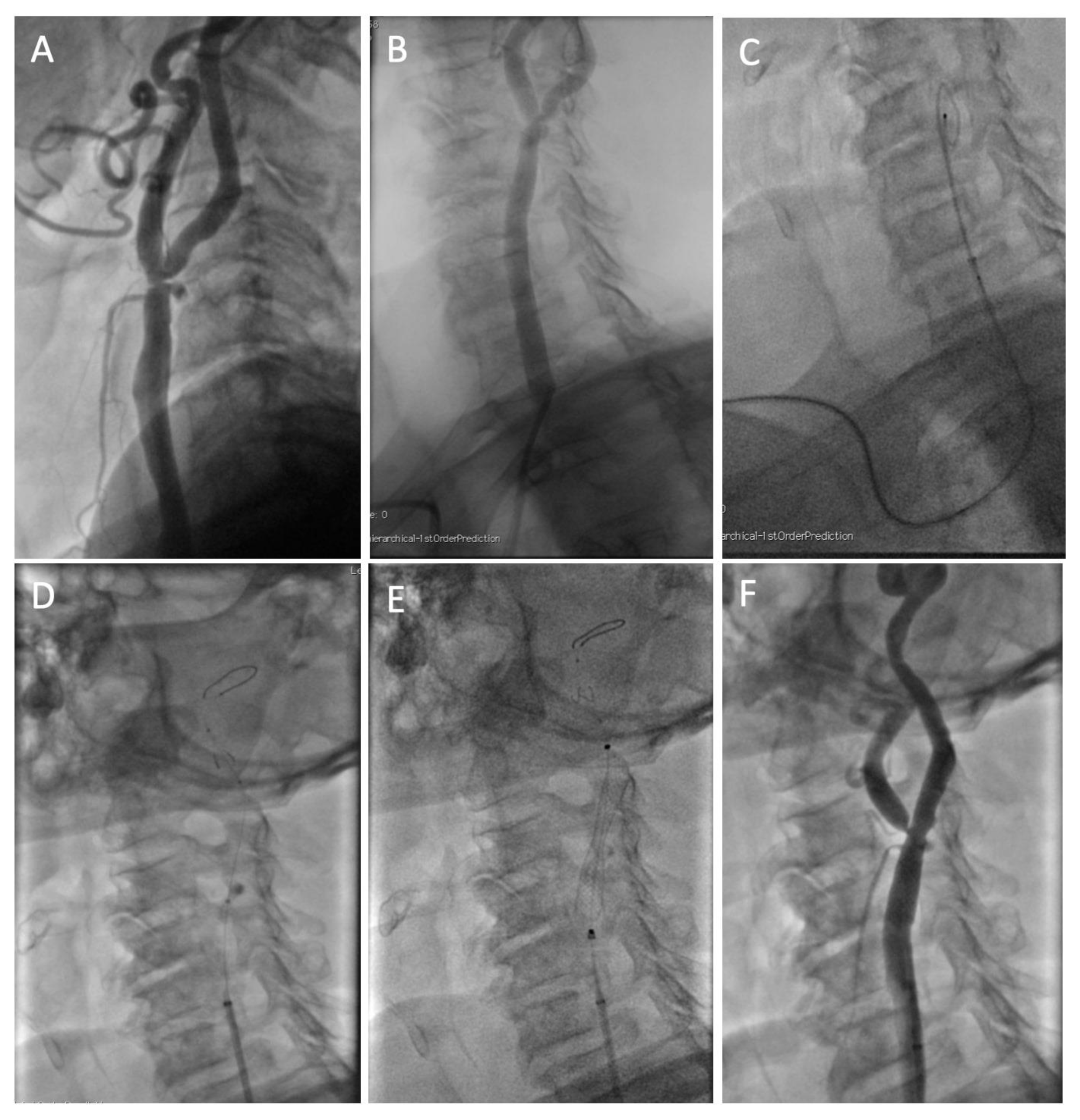
2.1. Interventional Procedure
2.2. Endpoints
2.3. Statistical Analysis
3. Results
3.1. Procedural and Clinical Outcomes
3.2. Learning Curve
4. Discussion
- Success rate for distal radial CAS was around 90%, with a relatively short learning curve;
- The rate of RAO was very low, in line with data on distal radial access for coronary interventions;
- The procedure was safe, with low rates of clinical events at 30 days.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- White, C.J.; Brott, T.G.; Gray, W.A.; Heck, D.; Jovin, T.; Lyden, S.P.; Metzger, D.C.; Rosenfield, K.; Roubin, G.; Sachar, R.; et al. Carotid Artery Stenting: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2022, 80, 155–170. [Google Scholar] [CrossRef] [PubMed]
- Montorsi, P.; Cortese, B.; Cernetti, C.; Lanzellotti, D.; Di Palma, G.; Marchese, A.; Cremonesi, A. Transradial approach for carotid artery stenting: A position paper from the Italian Society of Interventional Cardiology (SICI-GISE). Catheter. Cardiovasc. Interv. 2021, 97, 1440–1451. [Google Scholar] [CrossRef] [PubMed]
- Eid-Lidt, G.; Rodríguez, A.R.; Castellanos, J.J.; Pasos, J.I.F.; López, K.E.E.; Gaspar, J. Distal Radial Artery Approach to Prevent Radial Artery Occlusion Trial. JACC Cardiovasc. Interv. 2021, 14, 378–385. [Google Scholar] [CrossRef] [PubMed]
- Aminian, A.; Sgueglia, G.A.; Wiemer, M.; Kefer, J.; Gasparini, G.L.; Ruzsa, Z.; van Leeuwen, M.A.; Ungureanu, C.; Leibundgut, G.; Vandeloo, B.; et al. Distal Versus Conventional Radial Access for Coronary Angiography and Intervention: The DISCO RADIAL Trial. JACC Cardiovasc. Interv. 2022, 15, 1191–1201. [Google Scholar] [CrossRef] [PubMed]
- Ferrante, G.; Condello, F.; Rao, S.V.; Maurina, M.; Jolly, S.; Stefanini, G.G.; Reimers, B.; Condorelli, G.; Lefèvre, T.; Pancholy, S.B.; et al. Distal vs. Conventional Radial Access for Coronary Angiography and/or Intervention: A Meta-Analysis of Randomized Trials. JACC Cardiovasc. Interv. 2022, 15, 2297–2311. [Google Scholar] [CrossRef] [PubMed]
- Kühn, A.L.; Singh, J.; Moholkar, V.M.; Satti, S.R.; Rodrigues, K.D.M.; Massari, F.; Gounis, M.J.; McGowan, A.; Puri, A.S. Distal radial artery (snuffbox) access for carotid artery stenting—Technical pearls and procedural set-up. Interv. Neuroradiol. 2020, 27, 241–248. [Google Scholar] [CrossRef]
- Andò, G.; Cortese, B.; Russo, F.; Rothenbühler, M.; Frigoli, E.; Gargiulo, G.; Briguori, C.; Vranckx, P.; Leonardi, S.; Guiducci, V.; et al. Acute Kidney Injury After Radial or Femoral Access for Invasive Acute Coronary Syndrome Management: AKI-MATRIX. J. Am. Coll. Cardiol. 2017, 69, 2592–2603. [Google Scholar] [CrossRef]
- Andò, G.; Gragnano, F.; Calabrò, P.; Valgimigli, M. Radial vs. femoral access for the prevention of acute kidney injury (AKI) after coronary angiography or intervention: A systematic review and meta-analysis. Catheter. Cardiovasc. Interv. 2018, 92, E518–E526. [Google Scholar] [CrossRef]
- Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGo clinical practice guideline for acute kidney injury. Kidney Int. Suppl. 2012, 2, 1–138. [Google Scholar]
- Fischer, U.; Baumgartner, A.; Arnold, M.; Nedeltchev, K.; Gralla, J.; De Marchis, G.M.; Kappeler, L.; Mono, M.-L.; Brekenfeld, C.; Schroth, G.; et al. What Is a Minor Stroke? Stroke 2010, 41, 661–666. [Google Scholar] [CrossRef] [Green Version]
- McCullough, P.A.; Young, A.; Shutze, W.P. Acute Kidney Injury After Carotid Artery Stenting. JACC Cardiovasc. Interv. 2015, 8, 1515–1517. [Google Scholar] [CrossRef] [Green Version]
- Polimeni, A.; Passafaro, F.; De Rosa, S.; Sorrentino, S.; Torella, D.; Spaccarotella, C.; Mongiardo, A.; Indolfi, C. Clinical and Procedural Outcomes of 5-French versus 6-French Sheaths in Transradial Coronary Interventions. Medicine 2015, 94, e2170. [Google Scholar] [CrossRef]
- Capodanno, D. Twitterature. Eurointervention 2018, 14, e959–e961. [Google Scholar] [CrossRef] [Green Version]
- Rashid, M.; Kwok, C.S.; Pancholy, S.; Chugh, S.; Kedev, S.A.; Bernat, I.; Ratib, K.; Large, A.; Fraser, D.; Nolan, J.; et al. Radial Artery Occlusion after Transradial Interventions: A Systematic Review and Meta-Analysis. J. Am. Heart Assoc. 2016, 5, e002686. [Google Scholar] [CrossRef] [Green Version]
- Pancholy, S.; Coppola, J.; Patel, T.; Roke-Thomas, M. Prevention of radial artery occlusion-patent hemostasis evaluation trial (PROPHET study): A randomized comparison of traditional versus patency documented hemostasis after transradial catheterization. Catheter. Cardiovasc. Interv. 2008, 72, 335–340. [Google Scholar] [CrossRef]
- Ruzsa, Z.; Nemes, B.; Pintér, L.; Berta, B.; Tóth, K.; Teleki, B.; Nardai, S.; Jambrik, Z.; Szabó, G.; Kolvenbach, R.; et al. A randomised comparison of transradial and transfemoral approach for carotid artery stenting: RADCAR (RADial access for CARotid artery stenting) study. Eurointervention 2014, 10, 381–391. [Google Scholar] [CrossRef]
- Jaroenngarmsamer, T.; Bhatia, K.D.; Kortman, H.; Orru, E.; Krings, T. Procedural success with radial access for carotid artery stenting: Systematic review and meta-analysis. J. NeuroInterv. Surg. 2020, 12, 87–93. [Google Scholar] [CrossRef]
- Stanišić, M.-G.; Majewska, N.; Makałowski, M.; Juszkat, R.; Błaszak, M.; Majewski, W. Patient radiation exposure during carotid artery stenting. Vascular 2014, 23, 154–160. [Google Scholar] [CrossRef]
- Donahue, M.; Visconti, G.; Focaccio, A.; Selvetella, L.; Baldassarre, M.; Anselmi, C.V.; Briguori, C. Acute Kidney Injury in Patients With Chronic Kidney Disease Undergoing Internal Carotid Artery Stent Implantation. JACC Cardiovasc. Interv. 2015, 8, 1506–1514. [Google Scholar] [CrossRef] [Green Version]
- Stiller, K. Safety Issues That Should Be Considered When Mobilizing Critically Ill Patients. Crit. Care Clin. 2007, 23, 35–53. [Google Scholar] [CrossRef]
- Stabile, E.; Garg, P.; Cremonesi, A.; Bosiers, M.; Reimers, B.; Setacci, C.; Cao, P.; Schmidt, A.; Sievert, H.; Peeters, P.; et al. European registry of carotid artery stenting: Results from a prospective registry of eight high volume EUROPEAN institutions. Catheter. Cardiovasc. Interv. 2012, 80, 329–334. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Overall (n = 51) | |
|---|---|
| Age, years | 72 (67, 77) |
| Male sex, n (%) | 33 (65%) |
| Current smoker, n (%) | 13 (25%) |
| Former smoker, n (%) | 12 (23%) |
| Dyslipidemia, n (%) | 34 (67%) |
| Hypertension, n (%) | 40 (78%) |
| Diabetes mellitus, n (%) | 18 (35%) |
| Insulin therapy, n (%) | 6 (12%) |
| Lower limb PAD, n (%) | 6 (12%) |
| Coronary artery disease, n (%) | 28 (55%) |
| Oral anticoagulation, n (%) | 5 (10%) |
| Previous MI, n (%) | 8 (16%) |
| Previous PCI, n (%) | 15 (30%) |
| Previous CABG, n (%) | 5 (10%) |
| Previous stroke, n (%) | 8 (16%) |
| Symptoms, n (%) | 11 (22%) |
| Serum creatinine, mg/dL | 1.0 (0.8, 1.3) |
| Overall (n = 51) | |
|---|---|
| Distal radial access site, n (%) | Right: 48 (94%) Left: 3 (6%) |
| CAG during the same procedure, n (%) | 29 (57%) |
| Aortic arch type, n (%) - Type 1 - Type 2 - Type 3 - Bovine arch - Not available | 21 (42%) 8 (16%) 7 (14%) 11 (22%) 3 (6%) |
| Right ICA culprit stenosis, n (%) | 34 (67%) |
| Diameter stenosis (%) | 80 (75, 85) |
| Contralateral stenosis > 50%, n (%) | 8 (16%) |
| Sheath size, n (%) | 5 Fr: 50 (98%) 6 Fr: 1 (2%) |
| Diagnostic catheter, n (%) | JR 4: 8 (16%) JL 3.5: 3 (6%) Sim 1: 8 (16%) Sim 2: 32 (63%) |
| Guiding sheath, n (%) | Destination 5 Fr × 90 cm: 27 (53%) Destination 6 Fr × 90 cm: 1 (2%) Halo One 5 Fr × 90 cm: 20 (39%) Flexor 5 Fr × 70 cm: 2 (4%) Micro 5 Fr × 130 cm: 1 (2%) |
| Distal embolic protection | Emboshield NAV6: 46 (90%) Spider FX 6 mm: 2 (4%) Spider FX 7 mm: 3 (6%) |
| Predilatation, n (%) | 8 (16%) |
| Stent implanted, n (%) | Wallstent: 24 (47%) Mer: 27 (51%) * X-Act: 1 (2%) |
| Postdilation balloon, n (%) | 5.0 × 20 mm: 27 (53%) 5.5 × 20 mm: 24 (47%) |
| Procedure time, min | 50 (42, 63) |
| Procedure time, excluding CAG, min | 47 (36, 55) |
| X-ray time, min | 23 (17, 27) |
| X-ray time, excluding CAG, min | 18 (14, 24) |
| X-ray dose, mGy | 445 (202, 796) |
| X-ray dose, excluding CAG, mGy | 398 (177, 612) |
| DAP, Gy × cm2 | 44 (27, 75) |
| DAP, excluding CAG, Gy × cm2 | 36 (22, 61) |
| Contrast dose, mL | 120 (100, 140) |
| Contrast dose, excluding CAG, mL | 90 (70, 115) |
| Procedural Outcomes | |
|---|---|
| Procedural success, n (%) | 51 (100%) |
| Crossover to proximal radial, n (%) | 2 (4%) |
| Crossover to femoral, n (%) | 4 (8%) |
| Access site hematoma | 0 (0%) |
| RAO at 24 h | 1 (2%) |
| RAO at 30 days | 1 (2%) |
| AKI at 24–48 h | 3 (6%) |
| Length of hospitalization, days | 2 (2, 2) |
| In-hospital outcomes | |
| Death, n (%) | 0 (0%) |
| Myocardial infarction, n (%) | 0 (0%) |
| Minor stroke, n (%) | 1 (2%) |
| Major stroke, n (%) | 0 (0%) |
| 30-day outcomes | |
| Death, n (%) | 0 (0%) |
| Myocardial infarction, n (%) | 0 (0%) |
| Minor stroke, n (%) | 1 (2%) |
| Major stroke, n (%) | 0 (0%) |
| First Half (n = 25) | Second Half (n = 26) | p Value | |
|---|---|---|---|
| Radial success | |||
| Distal radial success | 20 (80%) | 25 (96%) | 0.07 |
| Procedure time, min | 57.8 (43.5, 63.5) | 49.0 (39, 61.5) | 0.47 |
| X-ray time, min | 24.6 (18.6, 27.4) | 19.8 (16.1, 27.78) | 0.49 |
| X-ray dose, mGy | 452 (152.5, 800.5) | 438 (209, 776) | 0.26 |
| DAP, Gy × cm2 | 46.1 (30.2, 78.9) | 43.4 (25.3, 70.6) | 0.56 |
| Contrast dose, mL | 120 (107, 150) | 110 (70, 140) | 0.045 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Gioia, G.; Salemme, L.; Ferrone, M.; Cioppa, A.; Popusoi, G.; Pucciarelli, A.; Verdoliva, S.; Franzese, M.; Marga, S.; Barbato, E.; et al. Carotid Artery Stenting Using Five-French Distal Radial Vascular Access. Diagnostics 2023, 13, 1266. https://doi.org/10.3390/diagnostics13071266
Di Gioia G, Salemme L, Ferrone M, Cioppa A, Popusoi G, Pucciarelli A, Verdoliva S, Franzese M, Marga S, Barbato E, et al. Carotid Artery Stenting Using Five-French Distal Radial Vascular Access. Diagnostics. 2023; 13(7):1266. https://doi.org/10.3390/diagnostics13071266
Chicago/Turabian StyleDi Gioia, Giuseppe, Luigi Salemme, Marco Ferrone, Angelo Cioppa, Grigore Popusoi, Armando Pucciarelli, Sebastiano Verdoliva, Michele Franzese, Simion Marga, Emanuele Barbato, and et al. 2023. "Carotid Artery Stenting Using Five-French Distal Radial Vascular Access" Diagnostics 13, no. 7: 1266. https://doi.org/10.3390/diagnostics13071266