
A Statistical Approach to the Diagnosis and Prediction of HCC Using CK19 and Glypican 3 Biomarkers
 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
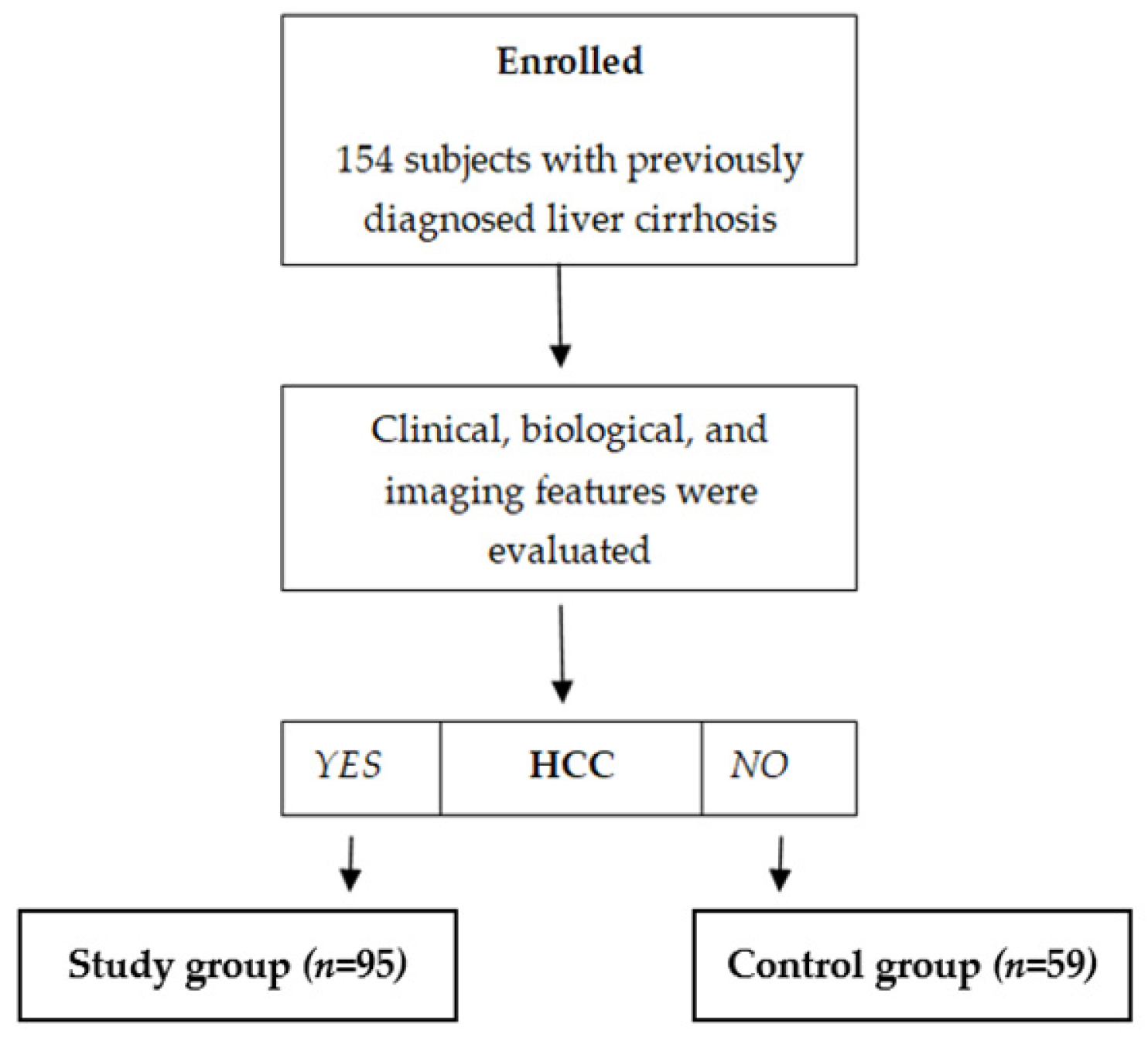
2.1. Patients
2.2. Biomarkers Assessment
2.3. Statistical Method
3. Results
3.1. Demographic and Clinical Characteristics of Patients
3.2. Diagnostic Role of AFP, AFP-F3, DCP, Glypican, and CK-19 Levels
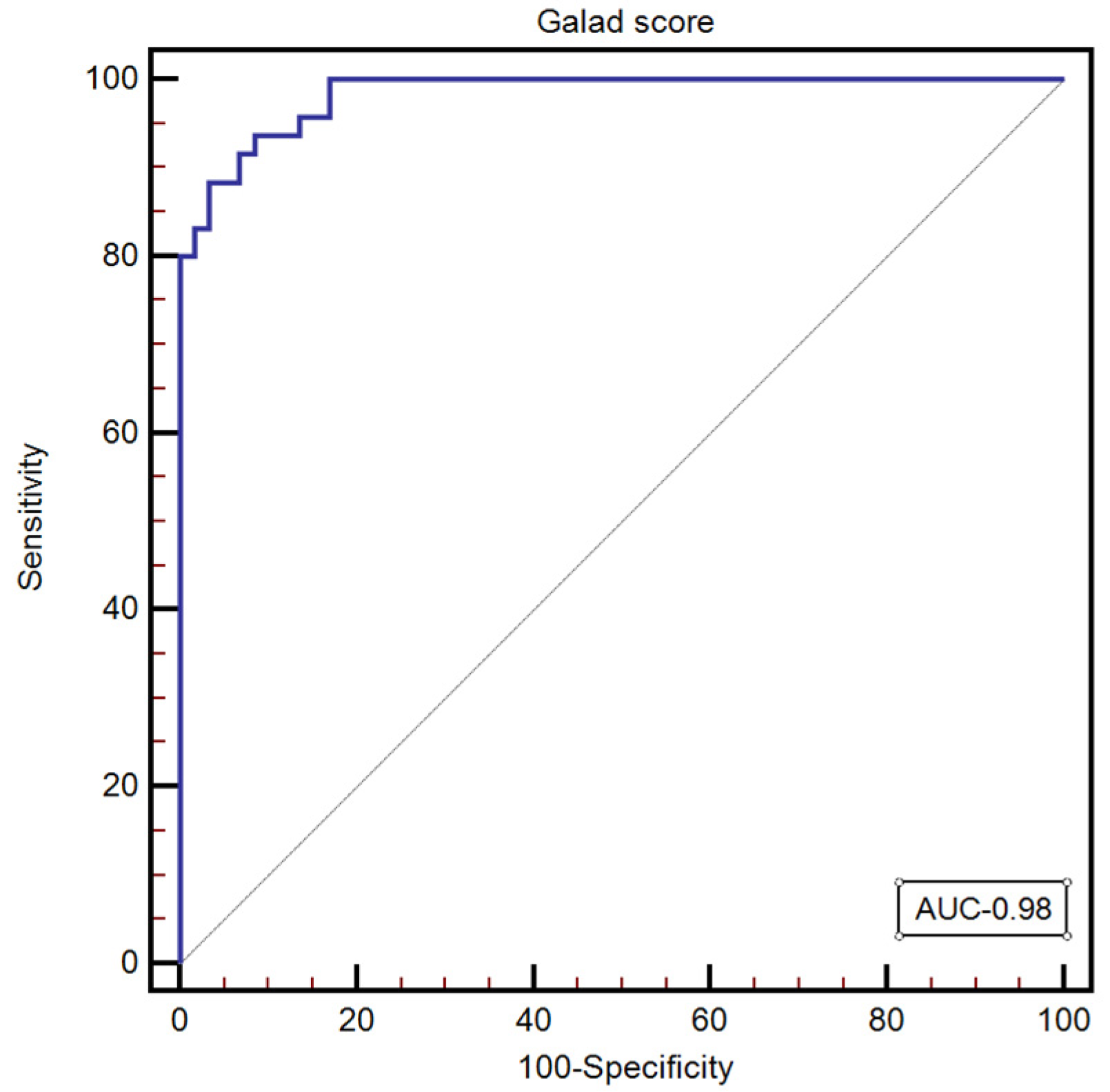
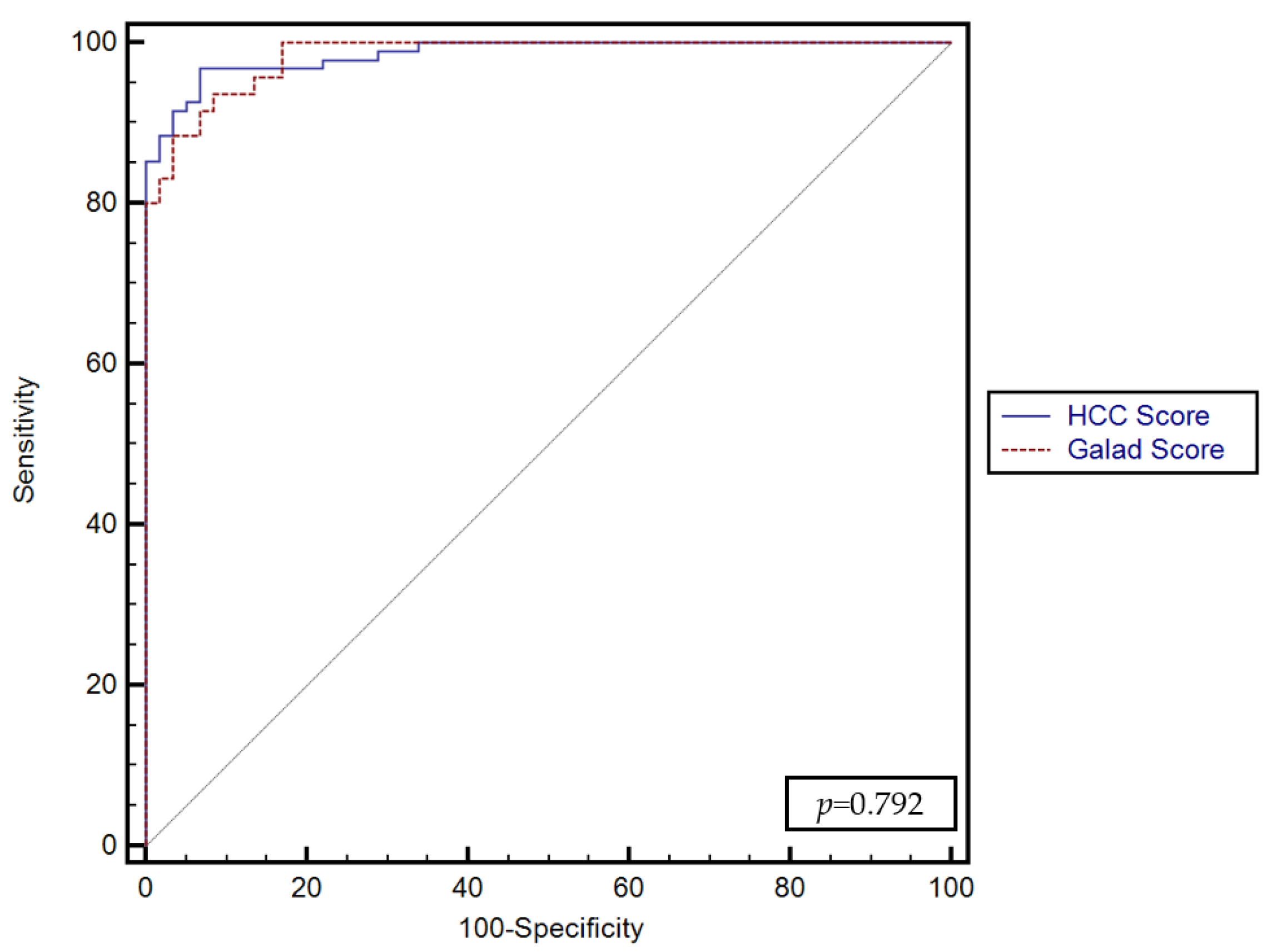
3.3. GALAD and GALKA Scores for Predicting the Presence of HCC
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Cancer. Available online: https://www.who.int/en/news-room/fact-sheets/detail/cancer (accessed on 23 June 2022).
- Global Burden of Disease Liver Cancer Collaboration; Akinyemiju, T.; Abera, S.; Ahmed, M.; Alam, N.; Alemayohu, M.A.; Allen, C.; Al-Raddadi, R.; Alvis-Guzman, N.; Amoako, Y.; et al. The Burden of Primary Liver Cancer and Underlying Etiologies From 1990 to 2015 at the Global, Regional, and National Level: Results from the Global Burden of Disease Study 2015. JAMA Oncol. 2017, 3, 1683–1691. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.L.; Ratziu, V.; Yuen, M.F.; Poynard, T. Viral hepatitis B. Lancet 2003, 362, 2089–2094. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. Electronic address: Easloffice@easloffice.eu; European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ioannou, G.N.; Splan, M.F.; Weiss, N.S.; McDonald, G.B.; Beretta, L.; Lee, S.P. Incidence and predictors of hepatocellular carcinoma in patients with cirrhosis. Clin. Gastroenterol. Hepatol. 2007, 5, 938–945.e4. [Google Scholar] [CrossRef]
- Sangiovanni, A.; Prati, G.M.; Fasani, P.; Ronchi, G.; Romeo, R.; Manini, M.; Del Ninno, E.; Morabito, A.; Colombo, M. The natural history of compensated cirrhosis due to hepatitis C virus: A 17-year cohort study of 214 patients. Hepatology 2006, 43, 1303–1310. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.D.; Roberts, L.R. Hepatocellular carcinoma: A global view. Nat. Rev. Gastroenterol. Hepatol. 2010, 7, 448–458. [Google Scholar] [CrossRef] [Green Version]
- Omata, M.; Cheng, A.L.; Kokudo, N.; Kudo, M.; Lee, J.M.; Jia, J.; Tateishi, R.; Han, K.H.; Chawla, Y.K.; Shiina, S.; et al. Asia-Pacific clinical practice guidelines on the management of hepatocellular carcinoma: A 2017 update. Hepatol. Int. 2017, 11, 317–370. [Google Scholar] [CrossRef] [Green Version]
- Marrero, J.A.; Kulik, L.M.; Sirlin, C.B.; Zhu, A.X.; Finn, R.S.; Abecassis, M.M.; Roberts, L.R.; Heimbach, J.K. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2018, 68, 723–750. [Google Scholar] [CrossRef] [Green Version]
- Lin, O.S.; Keeffe, E.B.; Sanders, G.D.; Owens, D.K. Cost-effectiveness of screening for hepatocellular carcinoma in patients with cirrhosis due to chronic hepatitis C. Aliment. Pharmacol. Ther. 2004, 19, 1159–1172. [Google Scholar] [CrossRef]
- Bruix, J.; Sherman, M.; American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma: An update. Hepatology 2011, 53, 1020–1022. [Google Scholar] [CrossRef] [Green Version]
- Chen, M.; Zhang, C.; Liu, W.; Du, X.; Liu, X.; Xing, B. Long noncoding RNA LINC01234 promotes hepatocellular carcinoma progression through orchestrating aspartate metabolic reprogramming. Mol. Ther. 2022, 30, 2354–2369. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Yang, Y.; Wang, K.; Chen, M.; Lu, M.; Hu, C.; Du, X.; Xing, B.; Liu, X. The Systematic Analyses of RING Finger Gene Signature for Predicting the Prognosis of Patients with Hepatocellular Carcinoma. J. Oncol. 2022, 2022, 2466006. [Google Scholar] [CrossRef]
- Tateishi, R.; Yoshida, H.; Matsuyama, Y.; Mine, N.; Kondo, Y.; Omata, M. Diagnostic accuracy of tumor markers for hepatocellular carcinoma: A systematic review. Hepatol. Int. 2008, 2, 17–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kakisaka, K.; Kataoka, K.; Onodera, M.; Suzuki, A.; Endo, K.; Tatemichi, Y.; Kuroda, H.; Ishida, K.; Takikawa, Y. Alpha-fetoprotein: A biomarker for the recruitment of progenitor cells in the liver in patients with acute liver injury or failure. Hepatol. Res. 2015, 45, E12–E20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.D.; Dai, J.; Singal, A.G.; Gopal, P.; Addissie, B.D.; Nguyen, M.H.; Befeler, A.S.; Reddy, K.R.; Schwartz, M.; Harnois, D.M. Improved Performance of Serum Alpha-Fetoprotein for Hepatocellular Carcinoma Diagnosis in HCV Cirrhosis with Normal Alanine Transaminase. Cancer Epidemiol. Biomark. Prev. 2017, 26, 1085–1092. [Google Scholar] [CrossRef] [Green Version]
- Choi, J.; Kim, G.A.; Han, S.; Lee, W.; Chun, S.; Lim, Y.S. Longitudinal Assessment of Three Serum Biomarkers to Detect Very Early-Stage Hepatocellular Carcinoma. Hepatology 2019, 69, 1983–1994. [Google Scholar] [CrossRef]
- Hann, H.W.; Li, D.; Yamada, H.; Satomura, S.; Coben, R.; DiMarino, A.J. Usefulness of Highly Sensitive AFP-L3 and DCP in Surveillance for Hepatocellular Carcinoma in Patients with a Normal Alpha-Fetoprotein. J. Med. Microbiol. Diagn. 2014, 3, 130. [Google Scholar] [CrossRef] [Green Version]
- Toyoda, H.; Kumada, T.; Tada, T. Highly sensitive Lens culinaris agglutinin-reactive α-fetoprotein: A new tool for the management of hepatocellular carcinoma. Oncology 2011, 81 (Suppl. S1), 61–65. [Google Scholar] [CrossRef]
- Kitano, Y.; Hayashi, H.; Matsumoto, T.; Nakao, Y.; Kaida, T.; Mima, K.; Imai, K.; Yamashita, Y.I.; Baba, H. The efficacy of anatomic resection for hepatocellular carcinoma within Milan criteria: A retrospective single-institution case-matched study. Eur. J. Surg. Oncol. 2022, 48, 2008–2013. [Google Scholar] [CrossRef]
- Marrero, J.A.; Su, G.L.; Wei, W.; Emick, D.; Conjeevaram, H.S.; Fontana, R.J.; Lok, A.S. Des-gamma carboxyprothrombin can differentiate hepatocellular carcinoma from nonmalignant chronic liver disease in American patients. Hepatology 2003, 37, 1114–1121. [Google Scholar] [CrossRef]
- El-Saadany, S.; El-Demerdash, T.; Helmy, A.; Mayah, W.W.; El-Sayed Hussein, B.; Hassanien, M.; Elmashad, N.; Fouad, M.A.; Basha, E.A. Diagnostic Value of Glypican-3 for Hepatocellular Carcinomas. Asian Pac. J. Cancer Prev. 2018, 19, 811–817. [Google Scholar] [CrossRef] [PubMed]
- Capurro, M.; Wanless, I.R.; Sherman, M.; Deboer, G.; Shi, W.; Miyoshi, E.; Filmus, J. Glypican-3: A Novel Serum and Histochemical Marker for Hepatocellular Carcinoma. Gastroenterology 2003, 125, 89–97. [Google Scholar] [CrossRef]
- Zheng, X.; Liu, X.; Lei, Y.; Wang, G.; Liu, M. Glypican-3: A Novel and Promising Target for the Treatment of Hepatocellular Carcinoma. Front. Oncol. 2022, 12, 824208. [Google Scholar] [CrossRef] [PubMed]
- Di Tommaso, L.; Franchi, G.; Park, Y.N.; Fiamengo, B.; Destro, A.; Morenghi, E.; Montorsi, M.; Torzilli, G.; Tommasini, M.; Terracciano, L.; et al. Diagnostic value of HSP70, glypican 3, and glutamine synthetase in hepatocellular nodules in cirrhosis. Hepatology 2007, 45, 725–734. [Google Scholar] [CrossRef] [PubMed]
- Shirakawa, H.; Suzuki, H.; Shimomura, M.; Kojima, M.; Gotohda, N.; Takahashi, S.; Nakagohri, T.; Konishi, M.; Kobayashi, N.; Kinoshita, T.; et al. Glypican-3 expression is correlated with poor prognosis in hepatocellular carcinoma. Cancer Sci. 2009, 100, 1403–1407. [Google Scholar] [CrossRef] [PubMed]
- Durnez, A.; Verslype, C.; Nevens, F.; Fevery, J.; Aerts, R.; Pirenne, J.; Lesaffre, E.; Libbrecht, L.; Desmet, V.; Roskams, T. The clinicopathological and prognostic relevance of cytokeratin 7 and 19 expression in hepatocellular carcinoma. A possible progenitor cell origin. Histopathology 2006, 49, 138–151. [Google Scholar] [CrossRef] [PubMed]
- Zhuo, J.Y.; Lu, D.; Tan, W.Y.; Zheng, S.S.; Shen, Y.Q.; Xu, X. CK19-positive Hepatocellular Carcinoma is a Characteristic Subtype. J. Cancer 2020, 11, 5069–5077. [Google Scholar] [CrossRef]
- Berhane, S.; Toyoda, H.; Tada, T.; Kumada, T.; Kagebayashi, C.; Satomura, S.; Schweitzer, N.; Vogel, A.; Manns, M.P.; Benckert, J.; et al. Role of the GALAD and BALAD-2 Serologic Models in Diagnosis of Hepatocellular Carcinoma and Prediction of Survival in Patients. Clin. Gastroenterol. Hepatol. 2016, 14, 875–886.e6. [Google Scholar] [CrossRef] [Green Version]
- Singal, A.G.; Tayob, N.; Mehta, A.; Marrero, J.A.; El-Serag, H.; Jin, Q.; Saenz de Viteri, C.; Fobar, A.; Parikh, N.D. GALAD demonstrates high sensitivity for HCC surveillance in a cohort of patients with cirrhosis. Hepatology 2022, 75, 541–549. [Google Scholar] [CrossRef]
- Sachan, A.; Kushwah, S.; Duseja, A. GALAD Score for HCC Screening and Surveillance. Clin. Gastroenterol. Hepatol. 2023, 21, 556–557. [Google Scholar] [CrossRef]
- Yang, J.D.; Addissie, B.D.; Mara, K.C.; Harmsen, W.S.; Dai, J.; Zhang, N.; Wongjarupong, N.; Ali, H.M.; Ali, H.A.; Hassan, F.A.; et al. GALAD Score for Hepatocellular Carcinoma Detection in Comparison with Liver Ultrasound and Proposal of GALADUS Score. Cancer Epidemiol. Biomark. Prev. 2019, 28, 531–538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Worland, T.; Harrison, B.; Delmenico, L.; Dowling, D. Hepatocellular Carcinoma Screening Utilising Serum Alpha-Fetoprotein Measurement and Abdominal Ultrasound Is More Effective than Ultrasound Alone in Patients with Non-viral Cirrhosis. J. Gastrointest. Cancer 2018, 49, 476–480. [Google Scholar] [CrossRef] [PubMed]
- Lersritwimanmaen, P.; Nimanong, S. Hepatocellular Carcinoma Surveillance: Benefit of Serum Alfa-fetoprotein in Real-world Practice. Euroasian J. Hepatogastroenterol. 2018, 8, 83–87. [Google Scholar] [CrossRef]
- Tamura, Y.; Igarashi, M.; Kawai, H.; Suda, T.; Satomura, S.; Aoyagi, Y. Clinical advantage of highly sensitive on-chip immunoassay for fucosylated fraction of alpha-fetoprotein in patients with hepatocellular carcinoma. Dig. Dis. Sci. 2010, 55, 2095–2101. [Google Scholar] [CrossRef] [PubMed]
- Kumada, T.; Toyoda, H.; Tada, T.; Kiriyama, S.; Tanikawa, M.; Hisanaga, Y.; Kanamori, A.; Tanaka, J.; Kagebayashi, C.; Satomura, S. High-sensitivity Lens culinaris agglutinin-reactive alpha-fetoprotein assay predicts early detection of hepatocellular carcinoma. J. Gastroenterol. 2014, 49, 555–563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, L.; Lu, F.; Chen, P.; Song, H.; Xu, W.; Guo, J.; Wang, J.; Zhou, J.; Kang, X.; Jin, C.; et al. Validation of the GALAD model and establishment of a new model for HCC detection in Chinese patients. Front. Oncol. 2022, 12, 1037742. [Google Scholar] [CrossRef]
- El Raziky, M.; Abdel Hafez, H.; Elsharkawy, A.; Moneer, T.A.; EL-Sheikh, S.M.; Maher, R.M.; Sharaf, S.A. Serum level of cytokeratin 19 as a diagnostic and prognostic marker in patients with HCV-related hepatocellular carcinoma. Egypt Liver J. 2021, 11, 57. [Google Scholar] [CrossRef]
- Liu, S.; Wang, M.; Zheng, C.; Zhong, Q.; Shi, Y.; Han, X. Diagnostic value of serum glypican-3 alone and in combination with AFP as an aid in the diagnosis of liver cancer. Clin. Biochem. 2020, 79, 54–60. [Google Scholar] [CrossRef]
- Kudo, M.; Kawamura, Y.; Hasegawa, K.; Tateishi, R.; Kariyama, K.; Shiina, S.; Toyoda, H.; Imai, Y.; Hiraoka, A.; Ikeda, M.; et al. Management of Hepatocellular Carcinoma in Japan: JSH Consensus Statements and Recommendations 2021 Update. Liver Cancer 2021, 10, 181–223. [Google Scholar] [CrossRef]
- Marrero, J.A.; Feng, Z.; Wang, Y.; Nguyen, M.H.; Befeler, A.S.; Roberts, L.R.; Reddy, K.R.; Harnois, D.; Llovet, J.M.; Normolle, D.; et al. Alpha-fetoprotein, des-gamma carboxyprothrombin, and lectin-bound alpha-fetoprotein in early hepatocellular carcinoma. Gastroenterology 2009, 137, 110–118. [Google Scholar] [CrossRef] [Green Version]
- Pang, B.Y.; Leng, Y.; Wang, X.; Wang, Y.Q.; Jiang, L.H. A meta-analysis and of clinical values of 11 blood biomarkers, such as AFP, DCP, and GP73 for diagnosis of hepatocellular carcinoma. Ann. Med. 2023, 55, 42–61. [Google Scholar] [CrossRef] [PubMed]
- Schütte, K.; Schulz, C.; Link, A.; Malfertheiner, P. Current biomarkers for hepatocellular carcinoma: Surveillance, diagnosis and prediction of prognosis. World J. Hepatol. 2015, 7, 139–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farinati, F.; Marino, D.; De Giorgio, M.; Baldan, A.; Cantarini, M.; Cursaro, C.; Rapaccini, G.; Del Poggio, P.; Di Nolfo, M.A.; Benvegnù, L.; et al. Diagnostic and prognostic role of alpha-fetoprotein in hepatocellular carcinoma: Both or neither? Am. J. Gastroenterol. 2006, 101, 524–532. [Google Scholar] [CrossRef] [PubMed]
- Carr, B.I.; Akkiz, H.; Üsküdar, O.; Yalçın, K.; Guerra, V.; Kuran, S.; Karaoğullarından, Ü.; Altıntaş, E.; Özakyol, A.; Tokmak, S.; et al. HCC with low- and normal-serum alpha-fetoprotein levels. Clin. Pract. 2018, 15, 453–464. [Google Scholar] [CrossRef] [Green Version]
- Zhou, J.M.; Wang, T.; Zhang, K.H. AFP-L3 for the diagnosis of early hepatocellular carcinoma: A meta-analysis. Medicine 2021, 100, e27673. [Google Scholar] [CrossRef]
- Tada, T.; Kumada, T.; Toyoda, H.; Kiriyama, S.; Sone, Y.; Tanikawa, M.; Hisanaga, Y.; Kitabatake, S.; Kuzuya, T.; Nonogaki, K.; et al. Relationship between Lens culinaris agglutinin-reactive alpha-fetoprotein and pathologic features of hepatocellular carcinoma. Liver Int. 2005, 25, 848–853. [Google Scholar] [CrossRef] [PubMed]
- Piratvisuth, T.; Tanwandee, T.; Thongsawat, S.; Sukeepaisarnjaroen, W.; Esteban, J.I.; Bes, M.; Köhler, B.; He, Y.; Swiatek-de Lange, M.; Morgenstern, D.; et al. Multimarker Panels for Detection of Early Stage Hepatocellular Carcinoma: A Prospective, Multicenter, Case-Control Study. Hepatol. Commun. 2022, 6, 679–691. [Google Scholar] [CrossRef] [PubMed]
- Talebizadeh, Z.; Simon, S.D.; Butler, M.G. X chromosome gene expression in human tissues: Male and female comparisons. Genomics 2006, 88, 675–681. [Google Scholar] [CrossRef]
- Kawai, T.; Yasuchika, K.; Ishii, T.; Katayama, H.; Yoshitoshi, E.Y.; Ogiso, S.; Kita, S.; Yasuda, K.; Fukumitsu, K.; Mizumoto, M.; et al. Keratin 19, a Cancer Stem Cell Marker in Human Hepatocellular Carcinoma. Clin. Cancer Res. 2015, 21, 3081–3091. [Google Scholar] [CrossRef] [Green Version]
- Johnson, P.J.; Pirrie, S.J.; Cox, T.F.; Berhane, S.; Teng, M.; Palmer, D.; Morse, J.; Hull, D.; Patman, G.; Kagebayashi, C.; et al. The detection of hepatocellular carcinoma using a prospectively developed and validated model based on serological biomarkers. Cancer Epidemiol. Biomark. Prev. 2014, 23, 144–153. [Google Scholar] [CrossRef] [Green Version]
- Guan, M.C.; Zhang, S.Y.; Ding, Q.; Li, N.; Fu, T.T.; Zhang, G.X.; He, Q.Q.; Shen, F.; Yang, T.; Zhu, H. The Performance of GALAD Score for Diagnosing Hepatocellular Carcinoma in Patients with Chronic Liver Diseases: A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 949. [Google Scholar] [CrossRef] [PubMed]
- Tayob, N.; Kanwal, F.; Alsarraj, A.; Hernaez, R.; El-Serag, H.B. The Performance of AFP, AFP-3, DCP as Biomarkers for Detection of Hepatocellular Carcinoma (HCC): A Phase 3 Biomarker Study in the United States. Clin. Gastroenterol. Hepatol. 2023, 21, 415–423.e4. [Google Scholar] [CrossRef] [PubMed]
- Lambrecht, J.; Porsch-Özçürümez, M.; Best, J.; Jost-Brinkmann, F.; Roderburg, C.; Demir, M.; Tacke, F.; Mohr, R. The APAC Score: A Novel and Highly Performant Serological Tool for Early Diagnosis of Hepatocellular Carcinoma in Patients with Liver Cirrhosis. J. Clin. Med. 2021, 10, 3392. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Subjects with Hepatocellular Carcinoma | Subjects without Hepatocellular Carcinoma | p-Value |
|---|---|---|---|
| n = 95 | n = 59 | ||
| Age (years) | 67.27 ± 9.31 | 60.98 ± 9.77 | p = 0.001 |
| Gender (%) | |||
| Females | 35 (36.8%) | 18 (30.5%) | 0.532 |
| Males | 60 (63.2%) | 41 (69.5%) | 0.532 |
| Etiology (%) | |||
| ALD | 19 (20%) | 34 (57.5%) | <0.001 |
| HBV | 21 (22.1%) | 3 (5.1%) | 0.009 |
| HCV | 46 (48.4%) | 4 (6.8%) | <0.001 |
| HBV + HDV | 4 (4.2%) | 4 (6.8%) | 0.739 |
| HBV + HCV | 1 (1.1%) | 0 (0%) | 0.841 |
| Viral + ALD | 0 (0%) | 5 (8.5%) | 0.015 |
| NASH | 4 (4.2%) | 5 (8.5%) | 0.452 |
| Others | 0 (0%) | 4 (6.8%) | 0.039 |
| Child-Pugh grade (%) | |||
| A [5,6] | 39 (41%) | 1 (1.7%) | <0.001 |
| B [7–9] | 30 (31.6%) | 19 (32.2%) | 0.920 |
| C [10–15] | 26 (27.4%) | 39 (66.1%) | <0.001 |
| MELD score | 13.26 ± 6.48 | 20.61 ± 6.13 | p < 0.001 |
| Tumor stage (BCLC) | |||
| A | 25 (26.3%) | ||
| B | 17 (17.9%) | ||
| C | 16 (16.9%) | ||
| D | 37 (38.9%) | ||
| Tumor size (cm) | |||
| <5 cm | 40 (42.1%) | ||
| >5 cm | |||
| or multiple nodules | 55 (57.9%) | ||
| PVT | 20 (21%) | 1 (1.7%) | p < 0.001 |
| Parameter | Subjects with Hepatocellular Carcinoma | Subjects without Hepatocellular Carcinoma | p-Value |
|---|---|---|---|
| n = 95 | n = 59 | ||
| CK-19 (ng/mL) | 1.26 [0.13–41.91] | 1.43 [0.16–6.43] | 0.076 |
| AFP (ng/mL) | 134.62 [2.5–1420.0] | 2.47 [0.25–32.96] | <0.001 |
| AFP_L3 (ng/mL) | 14.28 [0.33–98.1] | 0.98 [0.09–30.27] | <0.001 |
| DCP (ng/mL) | 3.12 [0.46–1061] | 0.25 [0.10–0.95] | <0.001 |
| Glypican (pg/mL) | 423.59 [129.48–10,032.18] | 270.81 [29.75–699.96] | <0.001 |
| Serum albumin (g/dL) | 3 [1.2–4.3] | 2.3 [1.3–3.4] | <0.001 |
| ALT (UI/L) | 55 [6–419] | 32 [12–444] | <0.001 |
| AST (UI/L) | 74 [20–687] | 71 [36–1186] | 0.445 |
| TB (mg/dL) | 1.42 [0.40–16.3] | 3.4 [0.2–28] | <0.001 |
| DB (mg/dL) | 0.54 [0.05–13.5] | 2.08 [0.13–18.6] | <0.001 |
| ALP (UI/L) | 117 [36–897] | 118 [35–360] | 0.996 |
| GGT (UI/L) | 100 [14–1363] | 138 [28–1156] | 0.594 |
| Platelet count | 121,000 [40,000–590,000] | 129,000 [36,000–351,900] | 0.872 |
| Parameter | AUC | SE | 95%CI | Se (%) | 95%CI | Sp (%) | 95%CI | NPV | PPV |
|---|---|---|---|---|---|---|---|---|---|
| AFP (ng/mL) | 0.94 | 0.016 | 0.894–0.974 | 74.7 | 64.8–83.1 | 100 | 93.3–100 | 100 | 71.1 |
| AFP-L3 (ng/mL) | 0.914 | 0.022 | 0.858–0.953 | 75.8 | 65.9–84.0 | 91.5 | 81.3–97.2 | 93.5 | 70.1 |
| DCP (ng/mL) | 0.824 | 0.022 | 0.755–0.881 | 84.2 | 75.3–90.9 | 66.1 | 52.6–77.9 | 72.2 | 80 |
| GPC3 (pg/mL) | 0.726 | 0.039 | 0.649–0.795 | 38.95 | 29.1–49.5 | 100 | 93.3–100 | 100 | 50.4 |
| CK-19 (ng/mL) | 0.585 | 0.046 | 0.503–0.664 | 33.7 | 24.3–44.1 | 96.6 | 88.3–99.6 | 94.1 | 47.5 |
| Model | AUC | 95% CI | Sensitivity |
|---|---|---|---|
| Model 1 | 0.912 | 0.889–0.947 | 90.9% |
| Model 2 | 0.931 | 0.912–0.966 | 92.0% |
| Model 3—GALKA | 0.981 | 0.946–0.997 | 96.8% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burciu, C.; Șirli, R.; Bende, R.; Popa, A.; Vuletici, D.; Miuțescu, B.; Rațiu, I.; Popescu, A.; Sporea, I.; Dănilă, M. A Statistical Approach to the Diagnosis and Prediction of HCC Using CK19 and Glypican 3 Biomarkers. Diagnostics 2023, 13, 1253. https://doi.org/10.3390/diagnostics13071253
Burciu C, Șirli R, Bende R, Popa A, Vuletici D, Miuțescu B, Rațiu I, Popescu A, Sporea I, Dănilă M. A Statistical Approach to the Diagnosis and Prediction of HCC Using CK19 and Glypican 3 Biomarkers. Diagnostics. 2023; 13(7):1253. https://doi.org/10.3390/diagnostics13071253
Chicago/Turabian StyleBurciu, Călin, Roxana Șirli, Renata Bende, Alexandru Popa, Deiana Vuletici, Bogdan Miuțescu, Iulia Rațiu, Alina Popescu, Ioan Sporea, and Mirela Dănilă. 2023. "A Statistical Approach to the Diagnosis and Prediction of HCC Using CK19 and Glypican 3 Biomarkers" Diagnostics 13, no. 7: 1253. https://doi.org/10.3390/diagnostics13071253