
Longitudinal Behavior of Left-Ventricular Strain in Fetal Growth Restriction

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
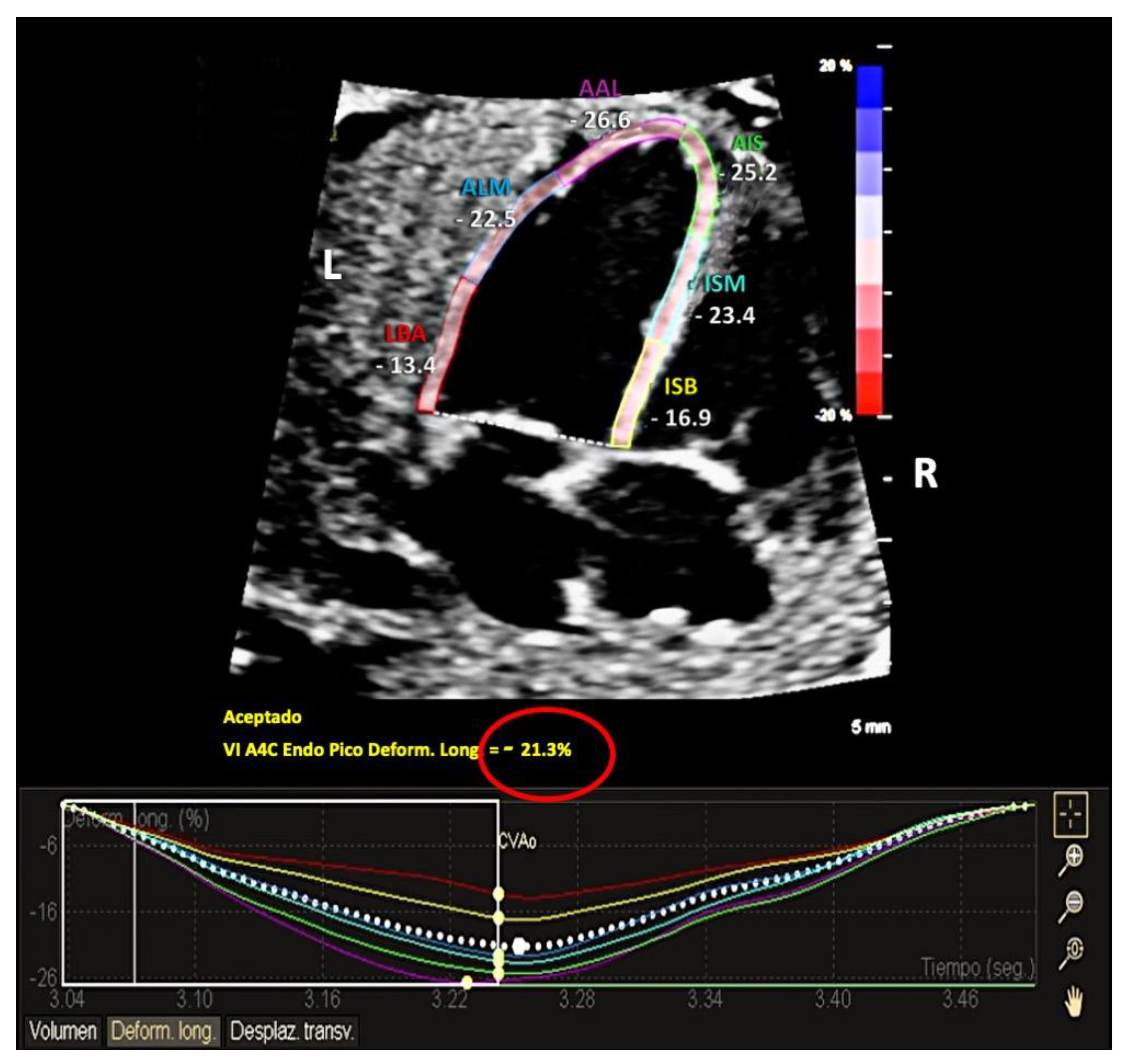
2.2. Ultrasound Acquisition
2.3. Analysis Protocol
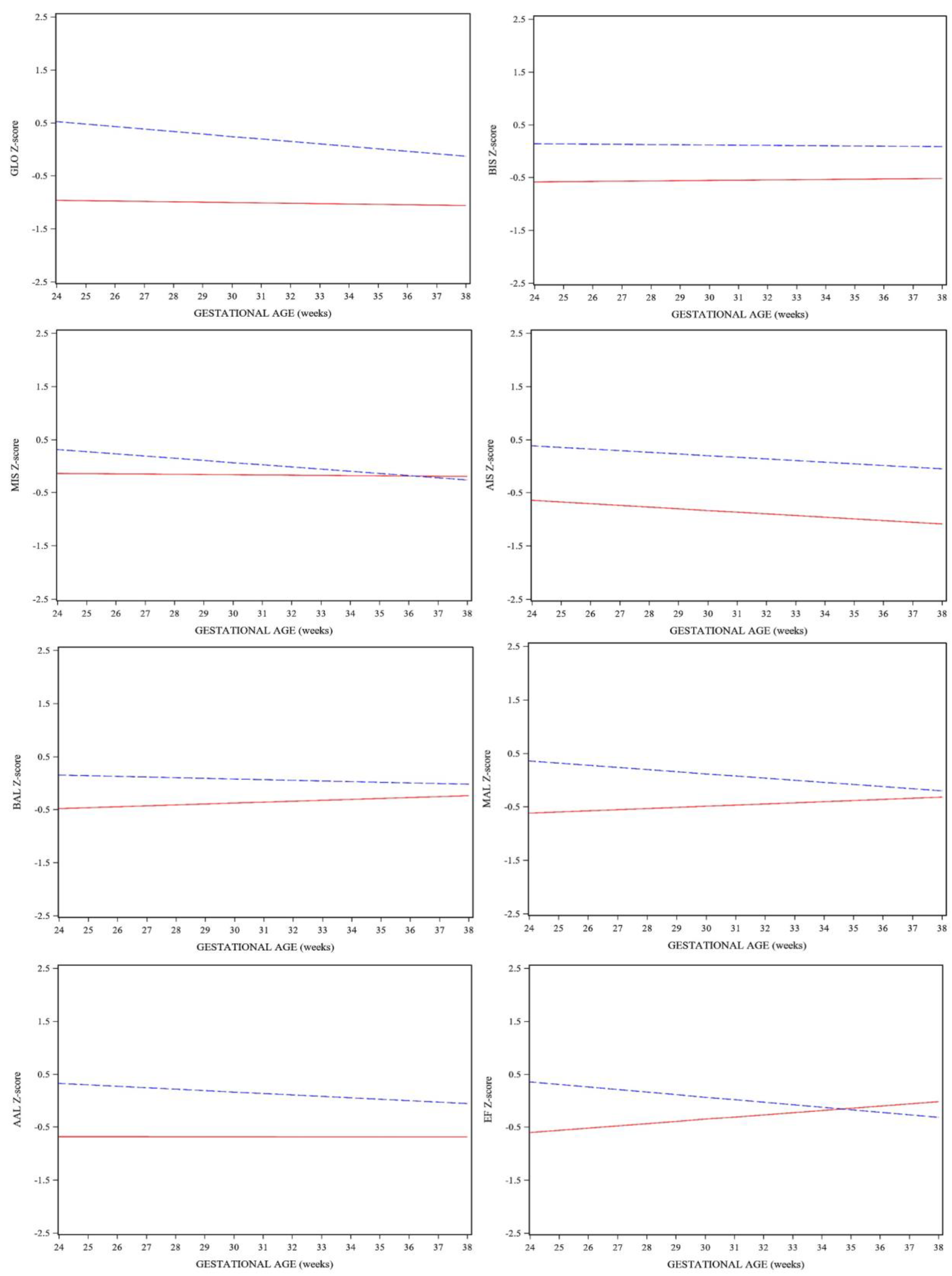
2.4. Statistical Analysis
3. Results
3.1. Basic Characteristics of the Study Population
3.2. Fetal Ultrasound Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Figueras, F.; Gratacós, E. Update on the Diagnosis and Classification of Fetal Growth Restriction and Proposal of a Stage-Based Management Protocol. Fetal Diagn. Ther. 2014, 36, 86–98. [Google Scholar] [CrossRef] [PubMed]
- Hanchate, N.; Ramani, S.; Mathpati, C.S.; Dalvi, V.H. Biomass Gasification Using Dual Fluidized Bed Gasification Systems: A Review. J. Clean. Prod. 2021, 280, 123148. [Google Scholar] [CrossRef]
- Verburg, B.O.; Jaddoe, V.W.V.; Wladimiroff, J.W.; Hofman, A.; Witteman, J.C.M.; Steegers, E.A.P. Fetal Hemodynamic Adaptive Changes Related to Intrauterine Growth the Generation R Study. Circulation 2008, 117, 649–659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naujorks, A.A.; Zielinsky, P.; Beltrame, P.A.; Castagna, R.C.; Petracco, R.; Busato, A.; Nicoloso, A.L.H.; Piccoli, A.; Manica, J.L. Myocardial Tissue Doppler Assessment of Diastolic Function in the Growth-Restricted Fetus. Ultrasound Obstet. Gynecol. 2009, 34, 68–73. [Google Scholar] [CrossRef]
- Crispi, F.; Hernandez-Andrade, E.; Pelsers, M.M.A.L.; Plasencia, W.; Benavides-Serralde, J.A.; Eixarch, E.; Le Noble, F.; Ahmed, A.; Glatz, J.F.C.; Nicolaides, K.H.; et al. Cardiac Dysfunction and Cell Damage across Clinical Stages of Severity in Growth-Restricted Fetuses. Am. J. Obstet. Gynecol. 2008, 199, 254.e1–254.e8. [Google Scholar] [CrossRef]
- Comas, M.; Crispi, F.; Cruz-Martinez, R.; Figueras, F.; Gratacos, E. Tissue Doppler Echocardiographic Markers of Cardiac Dysfunction in Small-for-Gestational Age Fetuses. Am. J. Obstet. Gynecol. 2011, 205, 57.e1–57.e6. [Google Scholar] [CrossRef]
- Cruz-Lemini, M.; Crispi, F.; Valenzuela-Alcaraz, B.; Figueras, F.; Sitges, M.; Gómez, O.; Bijnens, B.; Gratacós, E. Value of Annular M-Mode Displacement vs Tissue Doppler Velocities to Assess Cardiac Function in Intrauterine Growth Restriction. Ultrasound Obstet. Gynecol. 2013, 42, 175–181. [Google Scholar] [CrossRef]
- Ortigosa, N.; Rodriguez-Lopez, M.; Bailón, R.; Sarvari, S.I.; Sitges, M.; Gratacos, E.; Bijnens, B.; Crispi, F.; Laguna, P. Heart Morphology Differences Induced by Intrauterine Growth Restriction and Preterm Birth Measured on the ECG at Preadolescent Age. J. Electrocardiol. 2016, 49, 401–409. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-López, M.; Cruz-Lemini, M.; Valenzuela-Alcaraz, B.; Garcia-Otero, L.; Sitges, M.; Bijnens, B.; Gratacós, E.; Crispi, F. Descriptive Analysis of Different Phenotypes of Cardiac Remodeling in Fetal Growth Restriction. Ultrasound Obstet. Gynecol. 2017, 50, 207–214. [Google Scholar] [CrossRef] [Green Version]
- Llurba, E.; Syngelaki, A.; Sánchez, O.; Carreras, E.; Cabero, L.; Nicolaides, K.H. Maternal Serum Placental Growth Factor at 11-13 Weeks’ Gestation and Fetal Cardiac Defects. Ultrasound Obstet. Gynecol. 2013, 42, 169–174. [Google Scholar] [CrossRef]
- Zhang, S.; Qiu, X.; Wang, T.; Chen, L.; Li, J.; Diao, J.; Li, Y.; Qin, J.; Chen, L.; Jiang, Y. Hypertensive Disorders in Pregnancy Are Associated With Congenital Heart Defects in Offspring: A Systematic Review and Meta-Analysis. Front. Cardiovasc. Med. 2022, 9, 842878. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, B.D.; Barros, T.; Moleiro, M.L.; Guedes-Martins, L. Preeclampsia and Fetal Congenital Heart Defects. Curr. Cardiol. Rev. 2022, 18, 80–91. [Google Scholar] [CrossRef] [PubMed]
- Mazarico, E.; Llurba, E.; Cumplido, R.; Valls, A.; Melchor, J.C.; Iglesias, M.; Gómez-Roig, M.D. Neural Injury Markers in Intrauterine Growth Restriction and Their Relation to Perinatal Outcomes. Pediatr. Res. 2017, 82, 452–457. [Google Scholar] [CrossRef] [PubMed]
- Comas, M.; Crispi, F.; Cruz-Martinez, R.; Martinez, J.M.; Figueras, F.; Gratacós, E. Usefulness of Myocardial Tissue Doppler vs Conventional Echocardiography in the Evaluation of Cardiac Dysfunction in Early-Onset Intrauterine Growth Restriction. Am. J. Obstet. Gynecol. 2010, 203, 45.e1–45.e7. [Google Scholar] [CrossRef]
- Cruz-Lemini, M.; Crispi, F.; Valenzuela-alcaraz, B.; Figueras, F.; Sitges, M.; Bijnens, B.; Grataco, E.; Go, O. A Fetal Cardiovascular Score to Predict Infant Hypertension and Arterial Remodeling in Intrauterine Growth Restriction. Am. J. Obstet. Gynecol. 2014, 210, 552.e1–552.e22. [Google Scholar] [CrossRef]
- Cruz-Lemini, M.; Crispi, F.; Valenzuela-Alcaraz, B.; Figueras, F.; Sitges, M.; Bijnens, B.; Gratacós, E. Fetal Cardiovascular Remodeling Persists at 6 Months in Infants with Intrauterine Growth Restriction. Ultrasound Obstet. Gynecol. 2016, 48, 349–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazarico, E.; Llurba, E.; Cabero, L.; Sánchez, O.; Valls, A.; Martin-Ancel, A.; Cardenas, D.; Gómez Roig, M.D. Association between Neural Injury Markers of Intrauterine Growth-Restricted Infants and Neurodevelopment at 2 Years of Age. J. Matern.-Fetal Neonatal Med. 2018, 32, 3197–3203. [Google Scholar] [CrossRef] [PubMed]
- Crispi, F.; Bijnens, B.; Figueras, F.; Bartrons, J.; Eixarch, E.; Le Noble, F.; Ahmed, A.; Gratacós, E. Fetal Growth Restriction Results in Remodeled and Less Efficient Hearts in Children. Circulation 2010, 121, 2427–2436. [Google Scholar] [CrossRef] [Green Version]
- Sarvari, S.I.; Rodriguez-Lopez, M.; Nuñez-Garcia, M.; Sitges, M.; Sepulveda-Martinez, A.; Camara, O.; Butakoff, C.; Gratacos, E.; Bijnens, B.; Crispi, F. Persistence of Cardiac Remodeling in Preadolescents with Fetal Growth Restriction. Circ. Cardiovasc. Imaging 2017, 10, e005270. [Google Scholar] [CrossRef] [Green Version]
- Mi-Young Lee, H.-S.W. Technique of Fetal Echocardiography. Obstet. Gynecol. Sci. 2013, 56, 217–226. [Google Scholar] [CrossRef]
- Bhide, A.; Acharya, G.; Bilardo, C.M.; Brezinka, C.; Cafici, D.; Hernandez-Andrade, E.; Kalache, K.; Kingdom, J.; Kiserud, T.; Lee, W.; et al. ISUOG Practice Guidelines: Use of Doppler Ultrasonography in Obstetrics. Ultrasound Obstet. Gynecol. 2013, 41, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Rychik, J.; Ayres, N.; Cuneo, B.; Gotteiner, N.; Hornberger, L.; Spevak, P.J.; Van Der Veld, M. American Society of Echocardiography Guidelines and Standards for Performance of the Fetal Echocardiogram. J. Am. Soc. Echocardiogr. 2004, 17, 803–810. [Google Scholar] [CrossRef] [PubMed]
- García-Otero, L.; Gómez, O.; Rodriguez-López, M.; Torres, X.; Soveral, I.; Sepúlveda-Martínez, Á.; Guirado, L.; Valenzuela-Alcaraz, B.; López, M.; Martínez, J.M.; et al. Nomograms of Fetal Cardiac Dimensions at 18-41 Weeks of Gestation. Fetal Diagn. Ther. 2020, 47, 387–398. [Google Scholar] [CrossRef] [PubMed]
- Schneider, C.; McCrindle, B.W.; Carvalho, J.S.; Hornberger, L.K.; McCarthy, K.P.; Daubeney, P.E.F. Development of Z-Scores for Fetal Cardiac Dimensions from Echocardiography. Ultrasound Obstet. Gynecol. 2005, 26, 599–605. [Google Scholar] [CrossRef]
- Ruano, R.; Maeda, M.D.F.Y.; Niigaki, J.I.; Zugaib, M. Pulmonary Artery Diameters in Healthy Fetuses from 19 to 40 Weeks’ Gestation. J. Ultrasound Med. 2007, 26, 309–316. [Google Scholar] [CrossRef]
- Wong, S.F.; Ward, C.; Lee-Tannock, A.; Le, S.; Chan, F.Y. Pulmonary Artery/Aorta Ratio in Simple Screening for Fetal Outflow Tract Abnormalities during the Second Trimester. Ultrasound Obstet. Gynecol. 2007, 30, 275–280. [Google Scholar] [CrossRef]
- Hernandez-andrade, E.; Andres, J. Evaluation of Conventional Doppler Fetal Cardiac Function Parameters: E/A Ratios, Outflow Tracts, and Myocardial Performance Index. Fetal Diagn. Ther. 2012, 32, 22–29. [Google Scholar] [CrossRef]
- Gómez, O.; Figueras, F.; Fernández, S.; Bennasar, M.; Martínez, J.M.; Puerto, B.; Gratacós, E. Reference Ranges for Uterine Artery Mean Pulsatility Index at 11-41 Weeks of Gestation. Ultrasound Obstet. Gynecol. 2008, 32, 128–132. [Google Scholar] [CrossRef]
- Gardiner, H.M.; Pasquini, L.; Wolfenden, J.; Barlow, A.; Li, W.; Kulinskaya, E.; Henein, M. Myocardial Tissue Doppler and Long Axis Function in the Fetal Heart. Int. J. Cardiol. 2006, 113, 39–47. [Google Scholar] [CrossRef]
- Comas, M.; Crispi, F.; Gõmez, O.; Puerto, B.; Figueras, F.; Gratacõs, E. Gestational Age- and Estimated Fetal Weight-Adjusted Reference Ranges for Myocardial Tissue Doppler Indices at 24-41 Weeks’ Gestation. Ultrasound Obstet. Gynecol. 2011, 37, 57–64. [Google Scholar] [CrossRef]
- Cruz-Martnez, R.; Figueras, F.; Bennasar, M.; Garca-Posadas, R.; Crispi, F.; Hernández-Andrade, E.; Gratacós, E. Normal Reference Ranges from 11 to 41 Weeks’ Gestation of Fetal Left Modified Myocardial Performance Index by Conventional Doppler with the Use of Stringent Criteria for Delimitation of the Time Periods. Fetal Diagn. Ther. 2012, 32, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Crispi, F.; Gratacos, E. Fetal Cardiac Function: Technical Considerations and Potential Research and Clinical Applications. Fetal Diagn. Ther. 2012, 32, 47–64. [Google Scholar] [CrossRef]
- Crispi, F.; Valenzuela-Alcaraz, B.; Cruz-Lemini, M.; Gratacós, E. Ultrasound Assessment of Fetal Cardiac Function. Australas. J. Ultrasound Med. 2013, 16, 158–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leitman, M.; Lysyansky, P.; Sidenko, S.; Shir, V.; Peleg, E.; Binenbaum, M.; Kaluski, E.; Krakover, R.; Vered, Z. Two-Dimensional Strain-A Novel Software for Real-Time Quantitative Echocardiographic Assessment of Myocardial Function. J. Am. Soc. Echocardiogr. 2004, 17, 1021–1029. [Google Scholar] [CrossRef]
- Voigt, J.U.; Pedrizzetti, G.; Lysyansky, P.; Marwick, T.H.; Houle, H.; Baumann, R.; Pedri, S.; Ito, Y.; Abe, Y.; Metz, S.; et al. Definitions for a Common Standard for 2D Speckle Tracking Echocardiography: Consensus Document of the EACVI/ASE/Industry Task Force to Standardize Deformation Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 183–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blessberger, H.; Binder, T. Two Dimensional Speckle Tracking Echocardiography: Basic Principles. Heart 2010, 96, 716–722. [Google Scholar] [CrossRef]
- Crispi, F.; Sepulveda-Swatson, E.; Cruz-Lemini, M.; Rojas-Benavente, J.; Garcia-Posada, R.; Dominguez, J.M.; Sitges, M.; Bijnens, B.; Gratacós, E. Feasibility and Reproducibility of a Standard Protocol for 2D Speckle Tracking and Tissue Doppler-Based Strain and Strain Rate Analysis of the Fetal Heart. Fetal Diagn. Ther. 2012, 32, 96–108. [Google Scholar] [CrossRef] [PubMed]
- Di Salvo, G.; Russo, M.G.; Paladini, D.; Felicetti, M.; Castaldi, B.; Tartaglione, A.; Di Pietto, L.; Ricci, C.; Morelli, C.; Pacileo, G.; et al. Two-Dimensional Strain to Assess Regional Left and Right Ventricular Longitudinal Function in 100 Normal Foetuses. Eur. J. Echocardiogr. 2008, 9, 754–756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, X.; Zhao, B.; Chen, Y.; Pan, M.; Wang, B.; Peng, X. Preliminary Results Analysis for Left Ventricular Systolic Function in Normal Fetuses by Automated Cardiac Motion Quantitation. J. Matern.-Fetal Neonatal Med. 2021, 34, 2701–2709. [Google Scholar] [CrossRef]
- Maskatia, S.A.; Pignatelli, R.H.; Ayres, N.A.; Altman, C.A.; Sangi-Haghpeykar, H.; Lee, W. Longitudinal Changes and Interobserver Variability of Systolic Myocardial Deformation Values in a Prospective Cohort of Healthy Fetuses across Gestation and after Delivery. J. Am. Soc. Echocardiogr. 2016, 29, 341–349. [Google Scholar] [CrossRef]
- Domínguez-Gallardo, C.; Ginjaume-Garcia, N.; Ullmo, J.; Trilla, C.; Medina, M.C.; Vazquez, A.; Cruz-Lemini, M.; Llurba, E. Gestational Age-Adjusted Reference Ranges for Fetal Left Ventricle Longitudinal Strain by Automated Cardiac Motion Quantification between 24-37 Weeks’ Gestation. Fetal Diagn. Ther. 2022, 49, 311–320. [Google Scholar] [CrossRef]
- de Waal, K.; Phad, N. A Comparison between Philips and Tomtec for Left Ventricular Deformation and Volume Measurements in Neonatal Intensive Care Patients. Echocardiography 2018, 35, 375–379. [Google Scholar] [CrossRef]
- Day, T.G.; Charakida, M.; Simpson, J.M. Using Speckle-Tracking Echocardiography to Assess Fetal Myocardial Deformation: Are We There Yet? Ultrasound Obstet. Gynecol. 2019, 54, 575–581. [Google Scholar] [CrossRef]
- Wang, Y.; Fan, H.; Zhao, G.; Liu, D.; Du, L.; Wang, Z.; Hu, Y.; Hou, Y. MiR-16 Inhibits the Proliferation and Angiogenesis-Regulating Potential of Mesenchymal Stem Cells in Severe Pre-Eclampsia. FEBS J. 2012, 279, 4510–4524. [Google Scholar] [CrossRef]
- Cruz-Lemini, M.; Valenzuela-Alcaraz, B.; Figueras, F.; Sitges, M.; Gómez, O.; Martínez, J.M.; Bijnens, B.; Gratacós, E.; Crispi, F. Comparison of Two Different Ultrasound Systems for the Evaluation of Tissue Doppler Velocities in Fetuses. Fetal Diagn. Ther. 2016, 40, 35–40. [Google Scholar] [CrossRef]
- Lobmaier, S.M.; Cruz-Lemini, M.; Valenzuela-Alcaraz, B.; Ortiz, J.U.; Martinez, J.M.; Gratacos, E.; Crispi, F. Influence of Equipment and Settings on Myocardial Performance Index Repeatability and Definition of Settings to Achieve Optimal Reproducibility. Ultrasound Obstet. Gynecol. 2014, 43, 632–639. [Google Scholar] [CrossRef]
- van Oostrum, N.H.M.; Derks, K.; van der Woude, D.A.A.; Clur, S.A.; Oei, S.G.; van Laar, J.O.E.H. Two-Dimensional Speckle Tracking Echocardiography in Fetal Growth Restriction: A Systematic Review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 254, 87–94. [Google Scholar] [CrossRef]
- Robinson, H.P.; Sweet, E.M.; Adam, A.H. The Accuracy of Radiological Estimates of Gestational Age Using Early Fetal Crown-Rump Length Measurements By Ultrasound As a Basis for Comparison. BJOG Int. J. Obstet. Gynaecol. 1979, 86, 525–528. [Google Scholar] [CrossRef]
- Figueras, F.; Meler, E.; Iraola, A.; Eixarch, E.; Coll, O.; Figueras, J.; Francis, A.; Gratacos, E.; Gardosi, J. Customized Birthweight Standards for a Spanish Population. Eur. J. Obstet. Gynecol. Reprod. Biol. 2008, 136, 20–24. [Google Scholar] [CrossRef]
- Baschat, A.A.; Cosmi, E.; Bilardo, C.M.; Wolf, H.; Berg, C.; Rigano, S.; Germer, U.; Moyano, D.; Turan, S.; Hartung, J.; et al. Predictors of Neonatal Outcome in Early-Onset Placental Dysfunction. Obstet. Gynecol. 2007, 109, 253–261. [Google Scholar] [CrossRef]
- Gordijn, S.J.; Beune, I.M.; Thilaganathan, B.; Papageorghiou, A.; Baschat, A.A.; Baker, P.N.; Silver, R.M.; Wynia, K.; Ganzevoort, W. Consensus Definition of Fetal Growth Restriction: A Delphi Procedure. Ultrasound Obstet. Gynecol. 2016, 48, 333–339. [Google Scholar] [CrossRef]
- Patey, O.; Carvalho, J.S.; Thilaganathan, B. Perinatal Changes in Cardiac Geometry and Function in Growth-Restricted Fetuses at Term. Ultrasound Obstet. Gynecol. 2019, 53, 655–662. [Google Scholar] [CrossRef]
- van Oostrum, N.H.M.; de Vet, C.M.; van der Woude, D.A.A.; Kemps, H.M.C.; Oei, S.G.; van Laar, J.O.E.H. Fetal Strain and Strain Rate during Pregnancy Measured with Speckle Tracking Echocardiography: A Systematic Review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 250, 178–187. [Google Scholar] [CrossRef]
- Patey, O.; Carvalho, J.S.; Thilaganathan, B. Intervendor Discordance of Fetal and Neonatal Myocardial Tissue Doppler and Speckle-Tracking Measurements. J. Am. Soc. Echocardiogr. 2019, 32, 1339–1349.e23. [Google Scholar] [CrossRef]
- DeVore, G.R.; Gumina, D.L.; Hobbins, J.C. Assessment of Ventricular Contractility in Fetuses with an Estimated Fetal Weight Less than the Tenth Centile. Am. J. Obstet. Gynecol. 2019, 221, 498.e1–498.e22. [Google Scholar] [CrossRef]
- Van Oostrum, N.H.M.; van der Woude, D.A.A.; Clur, S.-A.B.; Oei, G.S.; Van Laar, J.O.E.H. Right Ventricular Dysfunction Identified by Abnormal Strain Values Precedes Evident Growth Restriction in Small for Gestational Age Fetuses. Prenat. Diagn. 2020, 40, 1525–1531. [Google Scholar] [CrossRef]
- Crispi, F.; Bijnens, B.; Sepulveda-Swatson, E.; Cruz-Lemini, M.; Rojas-Benavente, J.; Gonzalez-Tendero, A.; Garcia-Posada, R.; Rodriguez-Lopez, M.; Demicheva, E.; Sitges, M.; et al. Postsystolic Shortening by Myocardial Deformation Imaging as a Sign of Cardiac Adaptation to Pressure Overload in Fetal Growth Restriction. Circ. Cardiovasc. Imaging 2014, 7, 781–787. [Google Scholar] [CrossRef] [Green Version]
- Krause, K.; Möllers, M.; Hammer, K.; Falkenberg, M.K.; Möllmann, U.; Görlich, D.; Klockenbusch, W.; Schmitz, R. Quantification of Mechanical Dyssynchrony in Growth Restricted Fetuses and Normal Controls Using Speckle Tracking Echocardiography (STE). J. Perinat. Med. 2017, 45, 821–827. [Google Scholar] [CrossRef]
- Giussani, D.A. The Fetal Brain Sparing Response to Hypoxia: Physiological Mechanisms. J. Physiol. 2016, 594, 1215–1230. [Google Scholar] [CrossRef] [Green Version]
- Milner, J.; Arezina, J. The Accuracy of Ultrasound Estimation of Fetal Weight in Comparison to Birth Weight: A Systematic Review. Ultrasound 2018, 26, 32–41. [Google Scholar] [CrossRef] [Green Version]
- Oliver, M.; McNally, G.; Leader, L. Accuracy of Sonographic Prediction of Birth Weight. Aust. N. Z. J. Obstet. Gynaecol. 2013, 53, 584–588. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | FGR (n = 45) | AGA (n = 137) | p-Value |
|---|---|---|---|
| Clinical characteristics | |||
| Maternal age, years | 34 ± 5 | 33 ± 5 | 0.551 |
| Caucasian | 80 (36) | 72 (100) | >0.05 |
| Body mass index at inclusion, kg/m2 | 24 ± 5.07 | 22 + 3.04 | 0.110 |
| Nulliparity | 60 (27) | 75 (103) | >0.05 |
| Pregnancy outcome | |||
| Preeclampsia | 11 (5) | 0 (0) | <0.05 |
| GA at delivery | 36 ± 3 | 39 ± 1.03 | 0.001 |
| Vaginal delivery | 50 (23) | 81 (111) | <0.05 |
| Caesarean delivery | 44 (20) | 17 (24) | <0.05 |
| Birth weight, g | 2061 ± 619 | 3315 ± 338 | 0.001 |
| Birth weight centile | 2 ± 2 | 42 ± 25 | 0.001 |
| Variable | Group | Fixed | Random | |||
|---|---|---|---|---|---|---|
| Intercept (Z) | GA (Weeks) (Z) | GA (Weeks) (Z) | Intercept (SE) | Residual (SE) | ||
| GLO | −1.2147 (0.1228) | 0.208 (0.049) | −0.0466 (0.0098) | 0.0396 (0.0317) | 0.0849 | 0.6668 |
| BIS | −0.6659 (0.1325) | 0.117 (0.0528) | −0.00385 (0.0112) | 0.00852 (0.0356) | 0.0681 | 0.8730 |
| MIS | −0.1978 (0.1415) | 0.03415 (0.0567) | −0.0409 (0.0112) | 0.0368 (0.0360) | 0.1231 | 0.8548 |
| AIS | −1.033 (0.1399) | 0.1753 (0.0568) | −0.0310 (0.0096) | −0.00068 (0.0317) | 0.1947 | 0.6155 |
| BAL | −0.4303 (0.1270) | 0.0703 (0.0503) | −0.0125 (0.0117) | 0.0298 (0.03644) | 0.01195 | 0.9664 |
| MAL | −0.5563 (0.1288) | 0.0865 (0.0511) | −0.0399 (0.0113) | 0.0613 (0.0357) | 0.0417 | 0.8977 |
| AAL | −0.8246 (0.0347) | 0.1415 (0.0504) | −0.0272 (0.0110) | 0.0270 (0.0347) | 0.0491 | 0.8428 |
| EF | −0.3457 (0.1382) | 0.0304 (0.0553) | −0.0477 (0.0111) | 0.0895 (0.0357) | 0.1060 | 0.8495 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Domínguez-Gallardo, C.; Ginjaume-García, N.; Ullmo, J.; Fernández-Oliva, A.; Parra, J.; Vázquez, A.; Cruz-Lemini, M.; Llurba, E. Longitudinal Behavior of Left-Ventricular Strain in Fetal Growth Restriction. Diagnostics 2023, 13, 1252. https://doi.org/10.3390/diagnostics13071252
Domínguez-Gallardo C, Ginjaume-García N, Ullmo J, Fernández-Oliva A, Parra J, Vázquez A, Cruz-Lemini M, Llurba E. Longitudinal Behavior of Left-Ventricular Strain in Fetal Growth Restriction. Diagnostics. 2023; 13(7):1252. https://doi.org/10.3390/diagnostics13071252
Chicago/Turabian StyleDomínguez-Gallardo, Carla, Nuria Ginjaume-García, Johana Ullmo, Antonio Fernández-Oliva, Juan Parra, Ana Vázquez, Mónica Cruz-Lemini, and Elisa Llurba. 2023. "Longitudinal Behavior of Left-Ventricular Strain in Fetal Growth Restriction" Diagnostics 13, no. 7: 1252. https://doi.org/10.3390/diagnostics13071252