
Application of Drug Testing Platforms in Circulating Tumor Cells and Validation of a Patient-Derived Xenograft Mouse Model in Patient with Primary Intracranial Ependymomas with Extraneural Metastases
 , , , , , , and
, , , , , , and 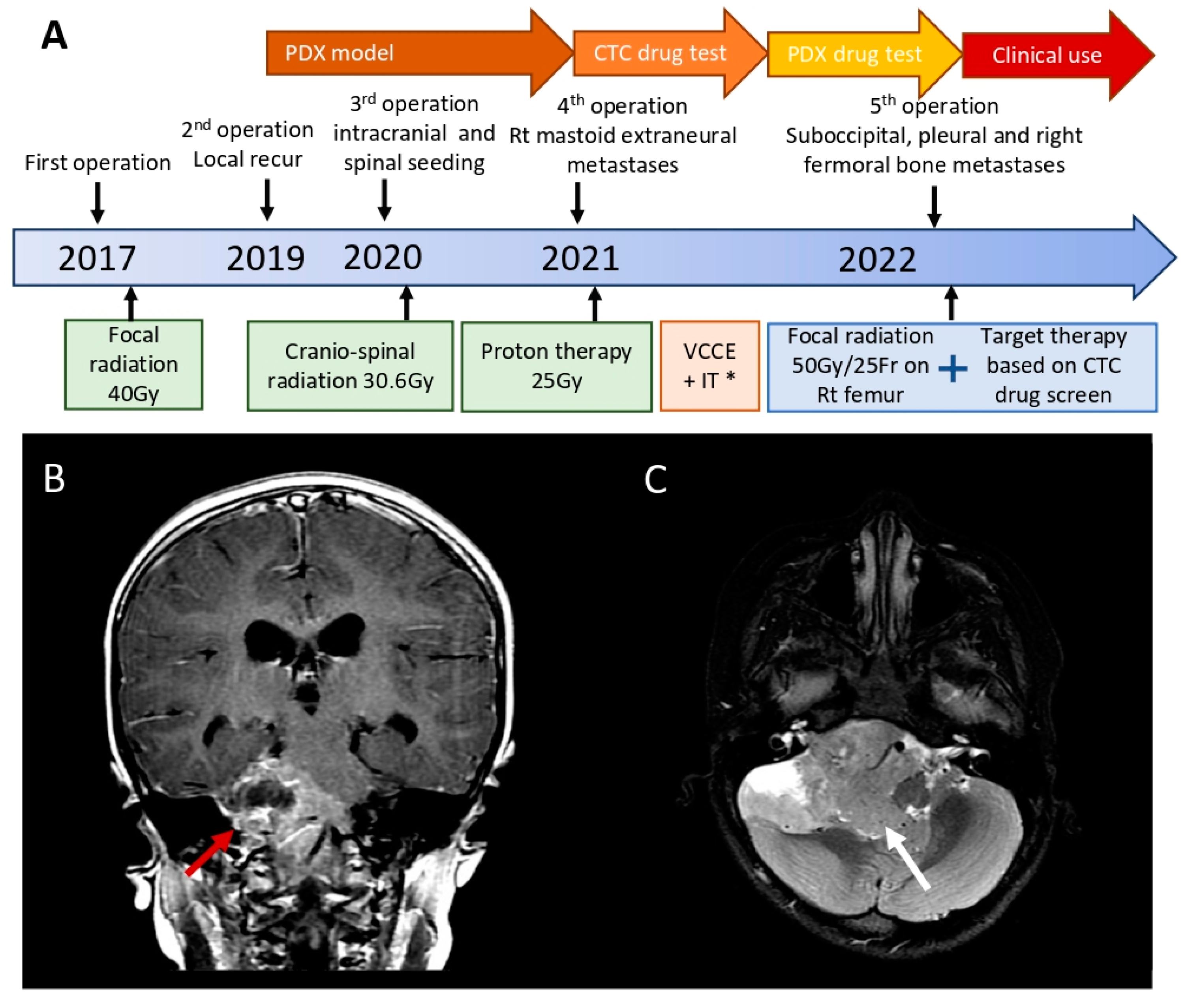{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Data
2.2. Circulating Tumor Cell Sorting and Drug Screening
2.3. Viability Assays for CTC Treatment
2.4. Establishment, Verification, and Drug Testing of the Patient-Derived Xenograft (PDX) Mouse Model
2.5. RNA Sequencing
3. Results
3.1. Clinical Courses and Timeline of Recurrence
3.2. Confirmation of Circulating Tumor Cells in Ependymoma and Potential Efficacy of Entrectinib and Everolimus
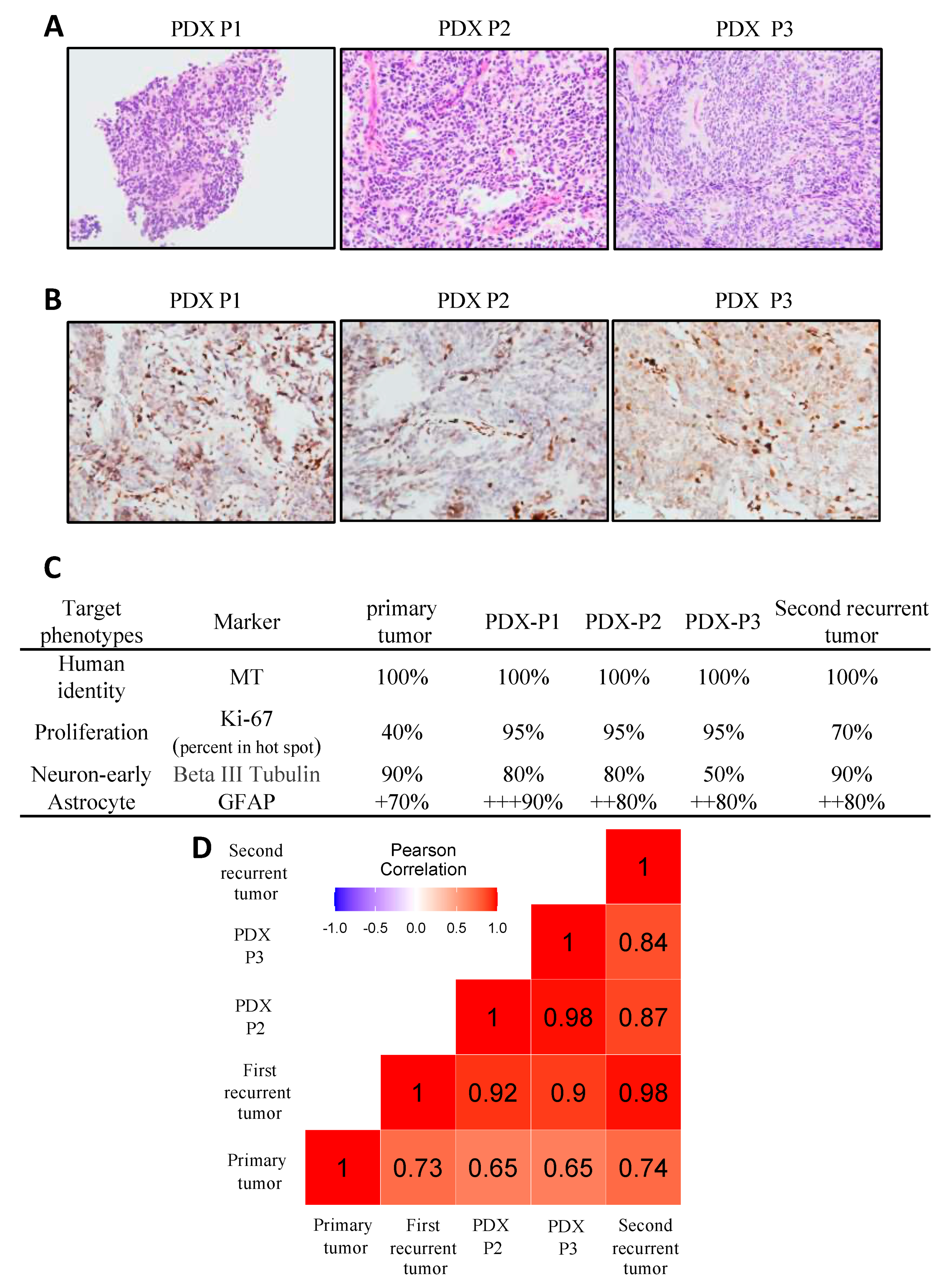
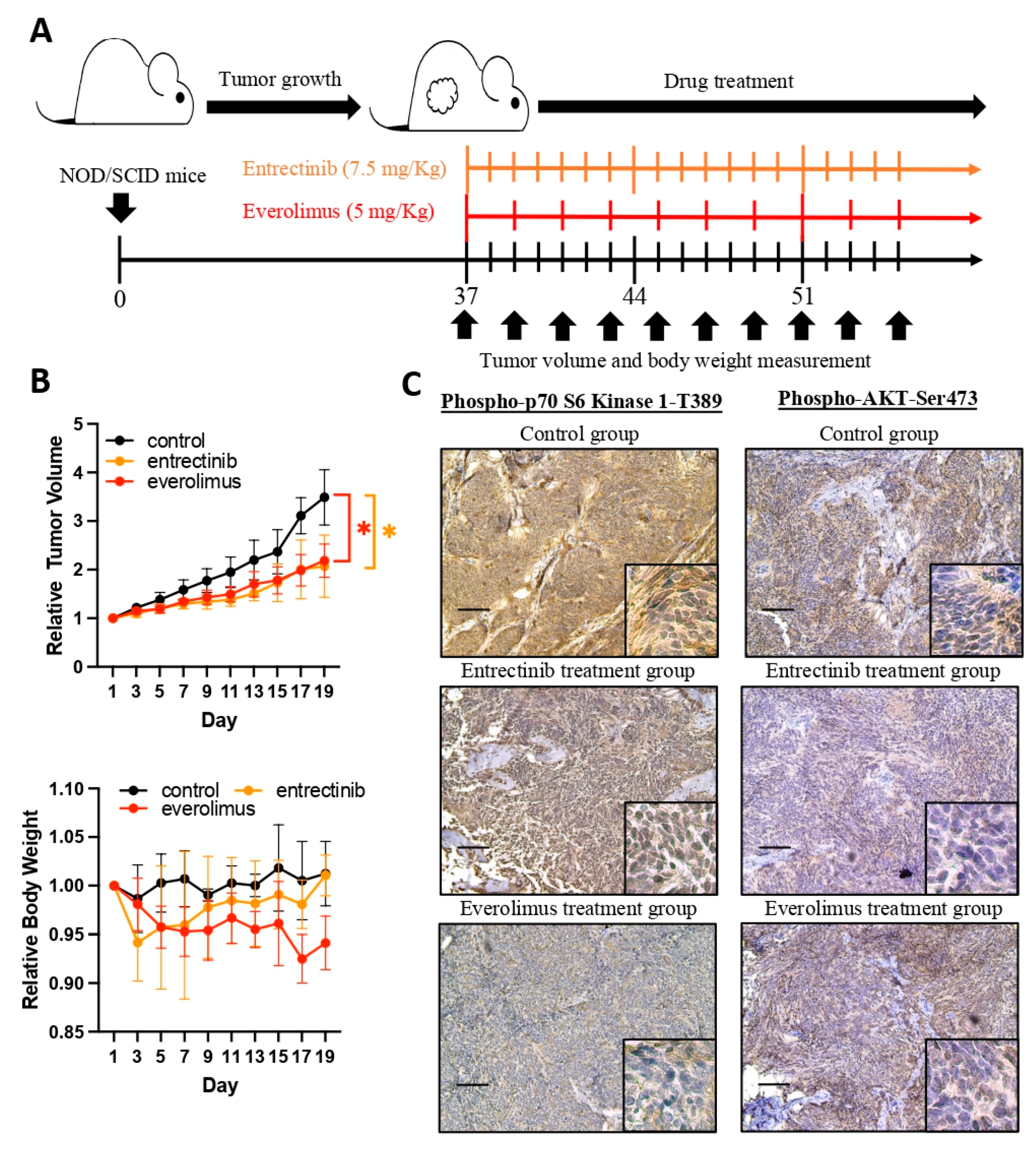
3.3. Validation of the Efficacy of the Selected Drugs in the Patient-Derived Xenograft Ependymoma Model
3.4. Everolimus Showed a Promising Effect When Given in Combined Salvage Therapy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vitanza, N.A.; Partap, S. Pediatric Ependymoma. J. Child. Neurol. 2016, 31, 1354–1366. [Google Scholar] [CrossRef] [PubMed]
- Kilday, J.P.; Rahman, R.; Dyer, S.; Ridley, L.; Lowe, J.; Coyle, B.; Grundy, R. Pediatric ependymoma: Biological perspectives. Mol. Cancer Res. 2009, 7, 765–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villano, J.L.; Parker, C.K.; Dolecek, T.A. Descriptive epidemiology of ependymal tumours in the United States. Br. J. Cancer 2013, 108, 2367–2371. [Google Scholar] [CrossRef] [Green Version]
- Liang, M.L.; Hsieh, T.H.; Liu, Y.R.; Chen, Y.W.; Lee, Y.Y.; Chang, F.C.; Lin, S.C.; Huang, M.C.; Donald Ming-Tak, H.; Wong, T.T.; et al. Significance of cyclin D1 overexpression in progression and radio-resistance of pediatric ependymomas. Oncotarget 2018, 9, 2527–2542. [Google Scholar] [CrossRef] [Green Version]
- Liang, M.L.; Chen, C.H.; Liu, Y.R.; Huang, M.H.; Lin, Y.C.; Wong, T.T.; Lin, S.E.; Chu, S.S.; Ding, Y.H.; Hsieh, T.H. Abemaciclib, A Selective CDK4/6 Inhibitor, Restricts the Growth of Pediatric Ependymomas. Cancers 2020, 12, 3597. [Google Scholar] [CrossRef]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A summary. Neuro-Oncology 2021, 23, 1231–1251. [Google Scholar] [CrossRef]
- Antony, R.; Wong, K.E.; Patel, M.; Olch, A.J.; McComb, G.; Krieger, M.; Gilles, F.; Sposto, R.; Erdreich-Epstein, A.; Dhall, G.; et al. A retrospective analysis of recurrent intracranial ependymoma. Pediatr. Blood Cancer 2014, 61, 1195–1201. [Google Scholar] [CrossRef]
- Ritzmann, T.A.; Rogers, H.A.; Paine, S.M.L.; Storer, L.C.D.; Jacques, T.S.; Chapman, R.J.; Ellison, D.; Donson, A.M.; Foreman, N.K.; Grundy, R.G. A retrospective analysis of recurrent pediatric ependymoma reveals extremely poor survival and ineffectiveness of current treatments across central nervous system locations and molecular subgroups. Pediatr. Blood Cancer 2020, 67, e28426. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.Y.; Chen, Y.W.; Lee, Y.Y.; Chang, F.C.; Chen, H.H.; Lin, S.C.; Ho, D.M.; Huang, M.C.; Yen, S.H.; Wong, T.T.; et al. Irradiation-Induced Secondary Tumors following Pediatric Central Nervous System Tumors: Experiences of a Single Institute in Taiwan (1975–2013). Int. J. Radiat. Oncol. Biol. Phys. 2018, 101, 1243–1252. [Google Scholar] [CrossRef]
- Gupta, T.; Maitre, M.; Gupta, P.; Krishnatry, R.; Chatterjee, A.; Moiyadi, A.; Shetty, P.; Singh, V.; Chinnaswamy, G.; Epari, S.; et al. Extent of re-excision, sequence/timing of salvage re-irradiation and disease-free interval impact upon clinical outcomes in recurrent/progressive ependymoma. J. Neuro-Oncol. 2020, 147, 405–415. [Google Scholar] [CrossRef]
- Merchant, T.E.; Li, C.; Xiong, X.; Kun, L.E.; Boop, F.A.; Sanford, R.A. Conformal radiotherapy after surgery for paediatric ependymoma: A prospective study. Lancet Oncol. 2009, 10, 258–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Netson, K.L.; Conklin, H.M.; Wu, S.; Xiong, X.; Merchant, T.E. A 5-year investigation of children’s adaptive functioning following conformal radiation therapy for localized ependymoma. Int. J. Radiat. Oncol. Biol. Phys. 2012, 84, 217–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerstner, E.R.; Pajtler, K.W. Ependymoma. Semin. Neurol. 2018, 38, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.; Onar-Thomas, A.; Ellison, D.; Owens-Pickle, E.; Wu, S.J.; Leary, S.E.S.; Fouladi, M.; Merchant, T.; Gajjar, A.; Foreman, N. Acns0831, Phase Iii Randomized Trial of Post-Radiation Chemotherapy in Patients with Newly Diagnosed Ependymoma Ages 1 to 21 Years. Neuro-Oncology 2020, 22, 318–319. [Google Scholar] [CrossRef]
- Palmisciano, P.; Ferini, G.; Barone, F.; Chavda, V.; Romano, F.; Amico, P.; Emmanuele, D.; Nicoletti, G.F.; Pompili, G.; Giammalva, G.R.; et al. Extra-Neural Metastases From Primary Intracranial Ependymomas: A Systematic Review. Front. Oncol. 2022, 12, 831016. [Google Scholar] [CrossRef]
- Lin, K.C.; Ting, L.L.; Chang, C.L.; Lu, L.S.; Lee, H.L.; Hsu, F.C.; Chiou, J.F.; Wang, P.Y.; Burnouf, T.; Ho, D.C.; et al. Ex Vivo Expanded Circulating Tumor Cells for Clinical Anti-Cancer Drug Prediction in Patients with Head and Neck Cancer. Cancers 2021, 13, 6076. [Google Scholar] [CrossRef]
- Wu, Y.H.; Hung, Y.P.; Chiu, N.C.; Lee, R.C.; Li, C.P.; Chao, Y.; Shyr, Y.M.; Wang, S.E.; Chen, S.C.; Lin, S.H.; et al. Correlation between drug sensitivity profiles of circulating tumour cell-derived organoids and clinical treatment response in patients with pancreatic ductal adenocarcinoma. Eur. J. Cancer 2022, 166, 208–218. [Google Scholar] [CrossRef]
- Yu, M.; Bardia, A.; Wittner, B.S.; Stott, S.L.; Smas, M.E.; Ting, D.T.; Isakoff, S.J.; Ciciliano, J.C.; Wells, M.N.; Shah, A.M.; et al. Circulating breast tumor cells exhibit dynamic changes in epithelial and mesenchymal composition. Science 2013, 339, 580–584. [Google Scholar] [CrossRef] [Green Version]
- Hofman, V.; Ilie, M.I.; Long, E.; Selva, E.; Bonnetaud, C.; Molina, T.; Vénissac, N.; Mouroux, J.; Vielh, P.; Hofman, P. Detection of circulating tumor cells as a prognostic factor in patients undergoing radical surgery for non-small-cell lung carcinoma: Comparison of the efficacy of the CellSearch Assay™ and the isolation by size of epithelial tumor cell method. Int. J. Cancer 2011, 129, 1651–1660. [Google Scholar] [CrossRef]
- Cieślikowski, W.A.; Antczak, A.; Nowicki, M.; Zabel, M.; Budna-Tukan, J. Clinical Relevance of Circulating Tumor Cells in Prostate Cancer Management. Biomedicines 2021, 9, 1179. [Google Scholar] [CrossRef]
- Qi, Y.; Sun, Q.; Deng, G.; Zhang, H.; Xu, Y.; Li, Y.; Huang, S.; Li, Y.; Ye, Z.; Wang, Y.; et al. Identifying circulating glioma cells and their clusters as diagnostic markers by a novel detection platform. Clin. Transl. Med. 2021, 11, e318. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.L.; Chiou, J.F.; Wang, P.Y.; Lu, L.S.; Shen, C.N.; Hsu, H.L.; Burnouf, T.; Ting, L.L.; Chou, P.C.; Chung, C.L.; et al. Ex Vivo Expansion and Drug Sensitivity Profiling of Circulating Tumor Cells from Patients with Small Cell Lung Cancer. Cancers 2020, 12, 3394. [Google Scholar] [CrossRef] [PubMed]
- Liston, D.R.; Davis, M. Clinically Relevant Concentrations of Anticancer Drugs: A Guide for Nonclinical Studies. Clin. Cancer Res. 2017, 23, 3489–3498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, K.Y.; Lee, K.; Shim, Y.; Park, J.W.; Kim, H.; Kang, J.; Won, J.K.; Kim, S.K.; Phi, J.H.; Park, C.K.; et al. Molecular subtyping of ependymoma and prognostic impact of Ki-67. Brain Tumor Pathol. 2022, 39, 1–13. [Google Scholar] [CrossRef]
- Tsang, D.S.; Burghen, E.; Klimo, P., Jr.; Boop, F.A.; Ellison, D.W.; Merchant, T.E. Outcomes After Reirradiation for Recurrent Pediatric Intracranial Ependymoma. Int. J. Radiat. Oncol. Biol. Phys. 2018, 100, 507–515. [Google Scholar] [CrossRef]
- Garvin, J.H., Jr.; Selch, M.T.; Holmes, E.; Berger, M.S.; Finlay, J.L.; Flannery, A.; Goldwein, J.W.; Packer, R.J.; Rorke-Adams, L.B.; Shiminski-Maher, T.; et al. Phase II study of pre-irradiation chemotherapy for childhood intracranial ependymoma. Children’s Cancer Group protocol 9942: A report from the Children’s Oncology Group. Pediatr. Blood Cancer 2012, 59, 1183–1189. [Google Scholar] [CrossRef]
- Maass, L. Occipital ependymoma with extracranial metastases. J. Neurosurg. 1954, 11, 413–421. [Google Scholar] [CrossRef]
- Mela, A.; Rdzanek, E.; Tysarowski, A.; Sakowicz, M.; Jaroszynski, J.; Furtak-Niczyporuk, M.; Zurek, G.; Poniatowski, L.A.; Jagielska, B. The impact of changing the funding model for genetic diagnostics and improved access to personalized medicine in oncology. Expert. Rev. Pharm. Outcomes Res. 2023, 23, 43–54. [Google Scholar] [CrossRef]
- Mela, A.; Poniatowski, L.A.; Drop, B.; Furtak-Niczyporuk, M.; Jaroszynski, J.; Wrona, W.; Staniszewska, A.; Dabrowski, J.; Czajka, A.; Jagielska, B.; et al. Overview and Analysis of the Cost of Drug Programs in Poland: Public Payer Expenditures and Coverage of Cancer and Non-Neoplastic Diseases Related Drug Therapies from 2015-2018 Years. Front. Pharmacol. 2020, 11, 1123. [Google Scholar] [CrossRef]
- Hou, J.M.; Krebs, M.G.; Lancashire, L.; Sloane, R.; Backen, A.; Swain, R.K.; Priest, L.J.; Greystoke, A.; Zhou, C.; Morris, K.; et al. Clinical significance and molecular characteristics of circulating tumor cells and circulating tumor microemboli in patients with small-cell lung cancer. J. Clin. Oncol. 2012, 30, 525–532. [Google Scholar] [CrossRef]
- Yang, C.; Xia, B.R.; Jin, W.L.; Lou, G. Circulating tumor cells in precision oncology: Clinical applications in liquid biopsy and 3D organoid model. Cancer Cell Int. 2019, 19, 341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, T.J.; Lin, T.W.; Wu, S.P.; Chu, H.T.; Kuo, Y.H.; Chiou, J.F.; Lu, L.S.; Chen, C.C. Patient-Derived Tumor Chemosensitization of GKB202, an Antrodia Cinnamomea Mycelium-Derived Bioactive Compound. Molecules 2021, 26, 6018. [Google Scholar] [CrossRef] [PubMed]
- Zheng, H.; Baranova, K.; Song, J.; Yan, L.; Biswas, S.; Chakrabarti, S.; Zhang, Q. Overexpression of Long Noncoding RNA HOTAIR Is a Unique Epigenetic Characteristic of Myxopapillary Ependymoma. J. Neuropathol. Exp. Neurol. 2020, 79, 1193–1202. [Google Scholar] [CrossRef] [PubMed]
- Hussein, S.A.; Sur, M. Cytokeratin positivity in myxopapillary ependymoma—A potential diagnostic pitfall. Diagn. Pathol. 2008, 3, 40. [Google Scholar] [CrossRef] [Green Version]
- Idowu, M.O.; Rosenblum, M.K.; Wei, X.J.; Edgar, M.A.; Soslow, R.A. Ependymomas of the central nervous system and adult extra-axial ependymomas are morphologically and immunohistochemically distinct—A comparative study with assessment of ovarian carcinomas for expression of glial fibrillary acidic protein. Am. J. Surg. Pathol. 2008, 32, 710–718. [Google Scholar] [CrossRef]
- Franz, D.N.; Belousova, E.; Sparagana, S.; Bebin, E.M.; Frost, M.; Kuperman, R.; Witt, O.; Kohrman, M.H.; Flamini, J.R.; Wu, J.Y.; et al. Efficacy and safety of everolimus for subependymal giant cell astrocytomas associated with tuberous sclerosis complex (EXIST-1): A multicentre, randomised, placebo-controlled phase 3 trial. Lancet 2013, 381, 125–132. [Google Scholar] [CrossRef]
- Lechuga, L.; Franz, D.N. Everolimus as adjunctive therapy for tuberous sclerosis complex-associated partial-onset seizures. Expert. Rev. Neurother. 2019, 19, 913–925. [Google Scholar] [CrossRef]
- DeWire, M.D.; Fuller, C.; Campagne, O.; Lin, T.; Pan, H.; Young Poussaint, T.; Baxter, P.A.; Hwang, E.I.; Bukowinski, A.; Dorris, K.; et al. A Phase I and Surgical Study of Ribociclib and Everolimus in Children with Recurrent or Refractory Malignant Brain Tumors: A Pediatric Brain Tumor Consortium Study. Clin. Cancer Res. 2021, 27, 2442–2451. [Google Scholar] [CrossRef]
- Cole, B.L.; Starr, K.; Lockwood, C.M.; Leary, S.E.S. The "SEED" Study: The Feasibility of Selecting Patient-Specific Biologically Targeted Therapy with Sorafenib, Everolimus, Erlotinib or Dasatinib for Pediatric and Young Adult Patients with Recurrent or Refractory Brain Tumors. Front. Biosci. 2022, 27, 219. [Google Scholar] [CrossRef]
- Doz, F.; van Tilburg, C.M.; Geoerger, B.; Hojgaard, M.; Ora, I.; Boni, V.; Capra, M.; Chisholm, J.; Chung, H.C.; DuBois, S.G.; et al. Efficacy and safety of larotrectinib in TRK fusion-positive primary central nervous system tumors. Neuro-Oncology 2022, 24, 997–1007. [Google Scholar] [CrossRef]
- Mangum, R.; Reuther, J.; Bertrand, K.C.; Chandramohan, R.; Kukreja, M.K.; Paulino, A.C.; Muzny, D.; Hu, J.; Gibbs, R.A.; Curry, D.J.; et al. Durable Response to Larotrectinib in a Child With Histologic Diagnosis of Recurrent Disseminated Ependymoma Discovered to Harbor an NTRK2 Fusion: The Impact of Integrated Genomic Profiling. JCO Precis. Oncol. 2021, 5, 1221–1227. [Google Scholar] [CrossRef] [PubMed]







Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liang, M.-L.; Yeh, T.-C.; Huang, M.-H.; Wu, P.-S.; Wu, S.-P.; Huang, C.-C.; Yen, T.-Y.; Ting, W.-H.; Hou, J.-Y.; Huang, J.-Y.; et al. Application of Drug Testing Platforms in Circulating Tumor Cells and Validation of a Patient-Derived Xenograft Mouse Model in Patient with Primary Intracranial Ependymomas with Extraneural Metastases. Diagnostics 2023, 13, 1232. https://doi.org/10.3390/diagnostics13071232
Liang M-L, Yeh T-C, Huang M-H, Wu P-S, Wu S-P, Huang C-C, Yen T-Y, Ting W-H, Hou J-Y, Huang J-Y, et al. Application of Drug Testing Platforms in Circulating Tumor Cells and Validation of a Patient-Derived Xenograft Mouse Model in Patient with Primary Intracranial Ependymomas with Extraneural Metastases. Diagnostics. 2023; 13(7):1232. https://doi.org/10.3390/diagnostics13071232
Chicago/Turabian StyleLiang, Muh-Lii, Ting-Chi Yeh, Man-Hsu Huang, Pao-Shu Wu, Shih-Pei Wu, Chun-Chao Huang, Tsung-Yu Yen, Wei-Hsin Ting, Jen-Yin Hou, Jia-Yun Huang, and et al. 2023. "Application of Drug Testing Platforms in Circulating Tumor Cells and Validation of a Patient-Derived Xenograft Mouse Model in Patient with Primary Intracranial Ependymomas with Extraneural Metastases" Diagnostics 13, no. 7: 1232. https://doi.org/10.3390/diagnostics13071232