
Automated Identification and Segmentation of Ellipsoid Zone At-Risk Using Deep Learning on SD-OCT for Predicting Progression in Dry AMD

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Imaging and Data Collection
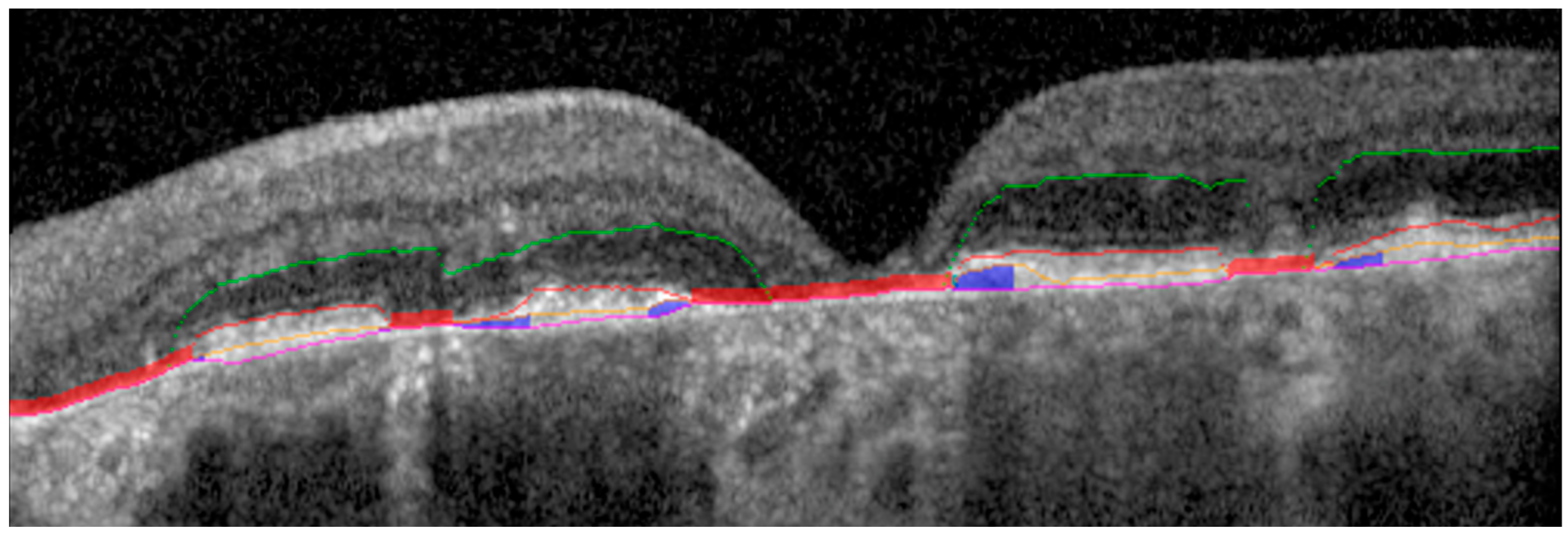
2.2. Ground Truth Retinal Layer Segmentation
2.3. Ellipsoid Zone At-Risk Detection Model
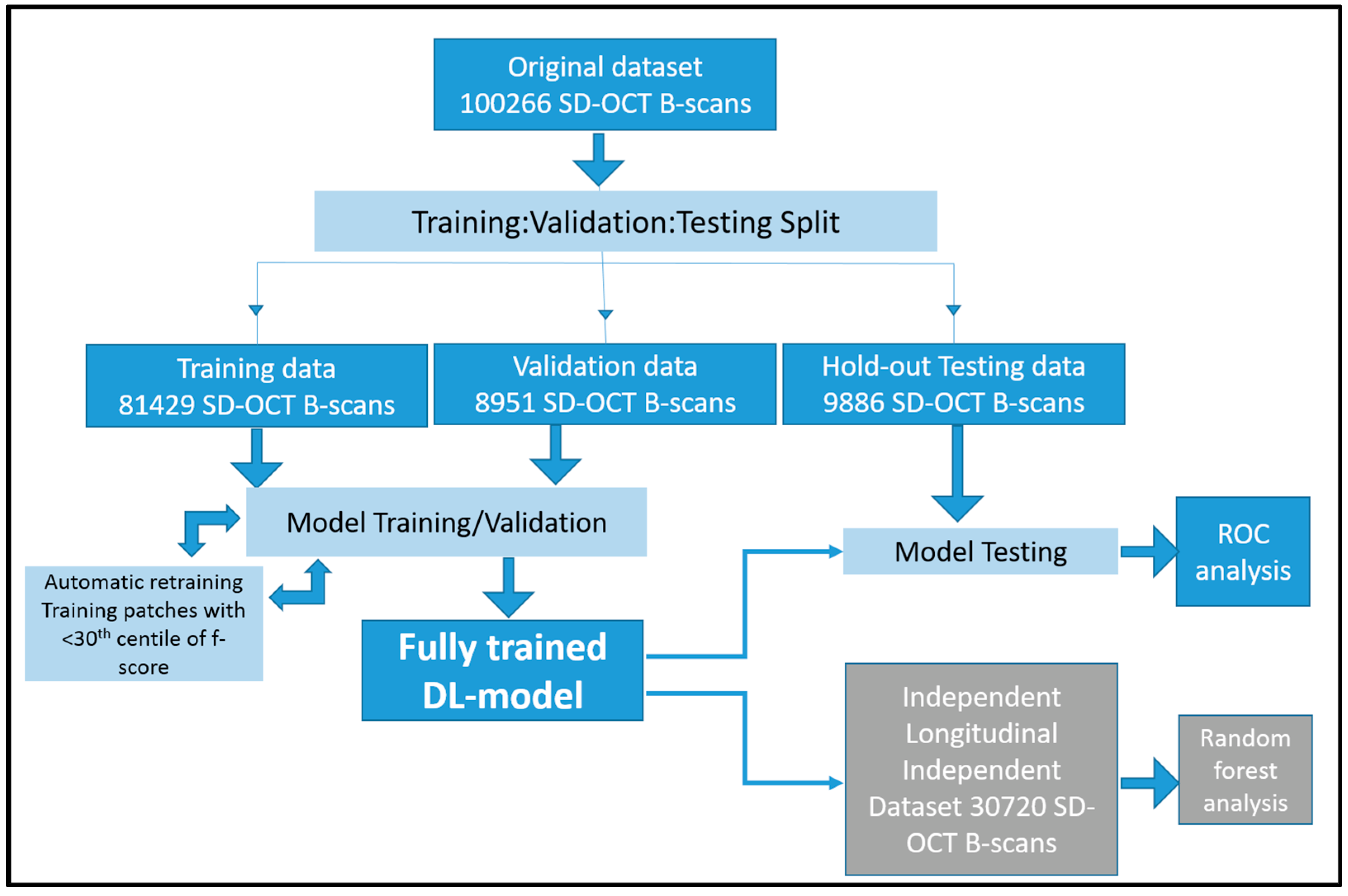
2.4. Training and Validation Data
2.5. Testing Data
2.6. Deep Learning Architecture
2.7. Automatic Retraining
2.8. Statistical Analysis
3. Results
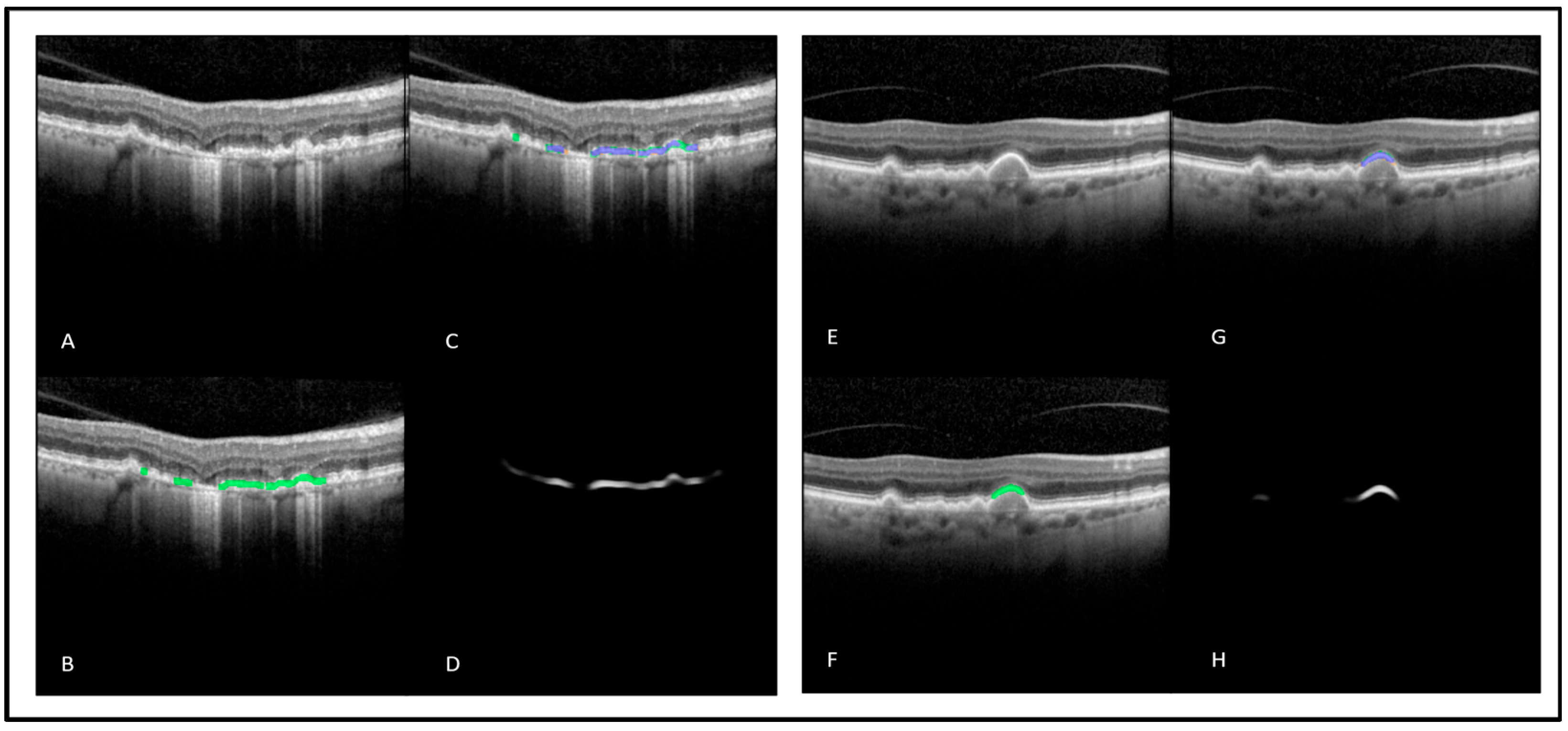
3.1. DL-Based Automated Detection and Measurement of Regions with EZ At-Risk
3.2. Correlation with Growth of GA Lesions
3.3. Random Forest Prediction of Sub-Foveal GA
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bressler, N.M.; Bressler, S.B.; Congdon, N.G.; Ferris, F.L., 3rd; Friedman, D.S.; Klein, R.; Lindblad, A.S.; Milton, R.C.; Seddon, J.M. Potential public health impact of Age-Related Eye Disease Study results: AREDS report no. 11. Arch. Ophthalmol. 2003, 121, 1621–1624. [Google Scholar] [PubMed]
- Wong, W.L.; Su, X.; Li, X.; Cheung, C.M.G.; Klein, R.; Cheng, C.Y.; Wong, T.Y. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: A systematic review and meta-analysis. Lancet Glob. Health 2014, 2, e106–e116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colijn, J.M.; Buitendijk, G.H.; Prokofyeva, E.; Alves, D.; Cachulo, M.L.; Khawaja, A.P.; Cougnard-Gregoire, A.; Merle, B.M.; Korb, C.; Erke, M.G.; et al. Prevalence of age-related macular degeneration in Europe: The past and the future. Ophthalmology 2017, 124, 1753–1763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmidt-Erfurth, U.; Bogunovic, H.; Grechenig, C.; Bui, P.; Fabianska, M.; Waldstein, S.; Reiter, G.S. Role of Deep Learning–Quantified Hyperreflective Foci for the Prediction of Geographic Atrophy Progression. Am. J. Ophthalmol. 2020, 216, 257–270. [Google Scholar] [CrossRef] [PubMed]
- Christenbury, J.G.; Folgar, F.A.; O’Connell, R.V.; Chiu, S.J.; Farsiu, S.; Toth, C.A. Progression of Intermediate Age-Related Macular Degeneration with Proliferation and Inner Retinal Migration of Hyperreflective Foci. Ophthalmology 2013, 120, 1038–1045. [Google Scholar] [CrossRef] [Green Version]
- Folgar, F.A.; Yuan, E.L.; Sevilla, M.B.; Chiu, S.J.; Farsiu, S.; Chew, E.Y.; Toth, C.A. Drusen Volume and Retinal Pigment Epithelium Abnormal Thinning Volume Predict 2-Year Progression of Age-Related Macular Degeneration. Ophthalmology 2015, 123, 39–50.e1. [Google Scholar] [CrossRef]
- Schmidt-Erfurth, U.; Waldstein, S.M.; Klimscha, S.; Sadeghipour, A.; Hu, X.; Gerendas, B.S.; Osborne, A.; Bogunovic, H. Prediction of Individual Disease Conversion in Early AMD Using Artificial Intelligence. Investig. Opthalmol. Vis. Sci. 2018, 59, 3199–3208. [Google Scholar] [CrossRef] [Green Version]
- Guymer, R.H.; Rosenfeld, P.J.; Curcio, C.A.; Holz, F.G.; Staurenghi, G.; Freund, K.B.; Schmitz-Valckenberg, S.; Sparrow, J.; Spaide, R.F.; Tufail, A.; et al. Incomplete Retinal Pigment Epithelial and Outer Retinal Atrophy in Age-Related Macular Degeneration: Classification of Atrophy Meeting Report 4. Ophthalmology 2019, 127, 394–409. [Google Scholar] [CrossRef]
- Litts, K.; Zhang, Y.; Freund, K.B.; Curcio, C.A. Optical Coherence Tomography and Histology of Age-Related Macular Degeneration Support Mitochondria as Reflectivity Sources. Retina 2018, 38, 445–461. [Google Scholar] [CrossRef]
- Niu, S.; de Sisternes, L.; Chen, Q.; Rubin, D.L.; Leng, T. Fully Automated Prediction of Geographic Atrophy Growth Using Quantitative Spectral-Domain Optical Coherence Tomography Biomarkers. Ophthalmology 2016, 123, 1737–1750. [Google Scholar] [CrossRef]
- Fleckenstein, M.; Mitchell, P.; Freund, K.B.; Sadda, S.; Holz, F.G.; Brittain, C.; Henry, E.C.; Ferrara, D. The Progression of Geographic Atrophy Secondary to Age-Related Macular Degeneration. Ophthalmology 2018, 125, 369–390. [Google Scholar] [CrossRef] [PubMed]
- Sarici, K.; Abraham, J.R.; Sevgi, D.D.; Lunasco, L.; Srivastava, S.K.; Whitney, J.; Cetin, H.; Hanumanthu, A.; Bell, J.M.; Reese, J.L.; et al. Risk Classification for Progression to Subfoveal Geographic Atrophy in Dry Age-Related Macular Degeneration Using Machine Learning–Enabled Outer Retinal Feature Extraction. Ophthalmic Surg. Lasers Imaging Retin. 2022, 53, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Kar, S.S.; Cetin, H.; Abraham, J.; Srivastava, S.K.; Madabhushi, A.; Ehlers, J.P. OCT-Derived SubRPE Compartment Radiomics Features Are Associated with the Development of Subfoveal Geographic Atrophy. Investig. Ophthalmol. Vis. Sci. 2022, 63, 363-F0194. [Google Scholar]
- Le, P.H.; Sharma, S.; Baynes, K.; Le, T.K.; Sarici, K.; Lunasco, L.; Kalra, G.; Wise, K.; Calabrise, C.; LaMunyon, N.; et al. Geographic atrophy measured by machine learning and manual segmentation on optical coherence tomography in non-neovascular age-related macular degeneration. Investig. Ophthalmol. Vis. Sci. 2022, 63, 3022-F0292. [Google Scholar]
- Reiter, G.S.; Told, R.; Schranz, M.; Baumann, L.; Mylonas, G.; Sacu, S.; Pollreisz, A.; Schmidt-Erfurth, U. Subretinal Drusenoid Deposits and Photoreceptor Loss Detecting Global and Local Progression of Geographic Atrophy by SD-OCT Imaging. Investig. Ophthalmol. Vis. Sci. 2020, 61, 11. [Google Scholar] [CrossRef]
- Nunes, R.P.; Gregori, G.; Yehoshua, Z.; Stetson, P.F.; Feuer, W.; Moshfeghi, A.A.; Rosenfeld, P.J. Predicting the Progression of Geographic Atrophy in Age-Related Macular Degeneration With SD-OCT En Face Imaging of the Outer Retina. Ophthalmic Surg. Lasers Imaging Retin. 2013, 44, 344–359. [Google Scholar] [CrossRef] [Green Version]
- Pfau, M.; von der Emde, L.; de Sisternes, L.; Hallak, J.A.; Leng, T.; Schmitz-Valckenberg, S.; Holz, F.G.; Fleckenstein, M.; Rubin, D.L. Progression of photoreceptor degeneration in geographic atrophy secondary to age-related macular degeneration. JAMA Ophthalmol. 2020, 138, 1026–1034. [Google Scholar] [CrossRef]
- Abraham, J.R.; Jaffe, G.J.; Kaiser, P.K.; Chiu, S.J.; Loo, J.; Farsiu, S.; Bouckaert, L.; Karageozian, V.; Sarayba, M.; Srivastava, S.K.; et al. Impact of Baseline Quantitative OCT Features on Response to Risuteganib for the Treatment of Dry Age-Related Macular Degeneration: The Importance of Outer Retinal Integrity. Ophthalmol. Retin. 2022, 6, 1019–1027. [Google Scholar] [CrossRef]
- Abraham, J.R.; Sil Kar, S.; Cetin, H.; Srivastava, S.K.; Madabhushi, A.; Ehlers, J.P. Exploration of Machine Learning-Enhanced Ellipsoid Zone Mapping and Radiomics-Based Textural Features as Biomarkers for Risk of Geographic Atrophy Development in Dry AMD. Investig. Ophthalmol. Vis. Sci. 2022, 63, 3020-F0290. [Google Scholar]
- Sunness, J.S.; Bressler, N.M.; Tian, Y.; Alexander, J.; Applegate, C.A. Measuring geographic atrophy in advanced age-related macular degeneration. Investig. Ophthalmol. Vis. Sci. 1999, 40, 1761–1769. [Google Scholar]
- Ehlers, J.P.; Uchida, A.; Hu, M.; Figueiredo, N.; Kaiser, P.K.; Heier, J.S.; Brown, D.M.; Boyer, D.S.; Do, D.V.; Gibson, A.; et al. Higher-Order Assessment of OCT in Diabetic Macular Edema from the VISTA Study: Ellipsoid Zone Dynamics and the Retinal Fluid Index. Ophthalmol. Retin. 2019, 3, 1056–1066. [Google Scholar] [CrossRef]
- Ehlers, J.P.; Zahid, R.; Kaiser, P.K.; Heier, J.S.; Brown, D.M.; Meng, X.; Reese, J.; Le, T.K.; Lunasco, L.; Hu, M.; et al. Longitudinal Assessment of Ellipsoid Zone Integrity, Subretinal Hyperreflective Material, and Subretinal Pigment Epithelium Disease in Neovascular Age-Related Macular Degeneration. Ophthalmol. Retin. 2021, 5, 1204–1213. [Google Scholar] [CrossRef]
- Itoh, Y.; Vasanji, A.; Ehlers, J.P. Volumetric ellipsoid zone mapping for enhanced visualisation of outer retinal integrity with optical coherence tomography. Br. J. Ophthalmol. 2015, 100, 295–299. [Google Scholar] [CrossRef] [Green Version]
- Arepalli, S.; Traboulsi, E.I.; Ehlers, J.P. Ellipsoid zone mapping and outer retinal assessment in stargardt disease. Retina 2018, 38, 1427–1431. [Google Scholar] [CrossRef]
- Ehlers, J.P.; Clark, J.; Uchida, A.; Figueiredo, N.; Babiuch, A.; Talcott, K.E.; Lunasco, L.; Le, T.K.; Meng, X.; Hu, M.; et al. Longitudinal Higher-Order OCT Assessment of Quantitative Fluid Dynamics and the Total Retinal Fluid Index in Neovascular AMD. Transl. Vis. Sci. Technol. 2021, 10, 29. [Google Scholar] [CrossRef]
- Kalra, G.; Talcott, K.E.; Kaiser, S.; Ugwuegbu, O.; Hu, M.; Srivastava, S.K.; Ehlers, J.P. Machine Learning–Based Automated Detection of Hydroxychloroquine Toxicity and Prediction of Future Toxicity Using Higher-Order OCT Biomarkers. Ophthalmol. Retin. 2022, 6, 1241–1252. [Google Scholar] [CrossRef]
- Kalra, G.; Cetin, H.; Whitney, J.; Yordi, S.; Cakir, Y.; McConville, C.; Whitmore, V.; Bonnay, M.; Lunasco, L.; Sassine, A.; et al. Machine Learning-Based Automated Detection and Quantification of Geographic Atrophy and Hypertransmission Defects Using Spectral Domain Optical Coherence Tomography. J. Pers. Med. 2022, 13, 37. [Google Scholar] [CrossRef]
- Zhu, W.; Chen, H.; Zhao, H.; Tian, B.; Wang, L.; Shi, F.; Xiang, D.; Luo, X.; Gao, E.; Zhang, L.; et al. Automatic Three-Dimensional Detection of Photoreceptor Ellipsoid Zone Disruption Caused by Trauma in the OCT. Sci. Rep. 2016, 6, 25433. [Google Scholar] [CrossRef] [Green Version]
- De Silva, T.; Jayakar, G.; Grisso, P.; Hotaling, N.; Chew, E.Y.; Cukras, C.A. Deep Learning-Based Automatic Detection of Ellipsoid Zone Loss in Spectral-Domain OCT for Hydroxychloroquine Retinal Toxicity Screening. Ophthalmol. Sci. 2021, 1, 100060. [Google Scholar] [CrossRef]
- Wang, Z.; Camino, A.; Zhang, M.; Wang, J.; Hwang, T.S.; Wilson, D.J.; Huang, D.; Li, D.; Jia, Y. Automated detection of photoreceptor disruption in mild diabetic retinopathy on volumetric optical coherence tomography. Biomed. Opt. Express 2017, 8, 5384–5398. [Google Scholar] [CrossRef] [Green Version]
- Orlando, J.I.; Gerendas, B.S.; Riedl, S.; Grechenig, C.; Breger, A.; Ehler, M.; Waldstein, S.M.; Bogunović, H.; Schmidt-Erfurth, U. Automated Quantification of Photoreceptor alteration in macular disease using Optical Coherence Tomography and Deep Learning. Sci. Rep. 2020, 10, 5619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vogl, W.-D.; Riedl, S.; Mai, J.; Reiter, G.S.; Lachinov, D.; Bogunović, H.; Schmidt-Erfurth, U. Predicting Topographic Disease Progression and Treatment Response of Pegcetacoplan in Geographic Atrophy Quantified by Deep Learning. Ophthalmol. Retin. 2023, 7, 4–13. [Google Scholar] [CrossRef] [PubMed]
- Ehlers, J.P.; Yordi, S.F.; Cetin, H.; Srivastava, S.K.; Madabhushi, A.; Ehlers, J.P. (Eds.) Exploration of Machine Learning-Enhanced Compartmental Retinal Integrity Assessment for Progression Risk and Treatment Response in the GATHER1 Study. In Proceedings of the Macula Soceity 45th Annual Meeting, Berlin, Germany, 8–11 June 2022. [Google Scholar]
- Srivastava, S.K.; Yordi, S.F.; Kalra, G.; Cakir, Y.; Cetin, H.; McConville, C.; Whitmore, V.; Abbruscato, A.; Ehlers, J.P. Ellipsoid Zone Preservation in Patients with Age-Related Macular Degeneration Treated with Subcutaneous Elamipretide. In Proceedings of the American Academy of Ophthalmology Annual Meeting, Chicago, IL, USA, 27–30 October 2022. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| Detection performance at the level of overall OCT volume | |
| Accuracy | 99% |
| Sensitivity | 99% |
| Specificity | 100% |
| Detection performance at the level of individual OCT-B scans | |
| Accuracy | 87% |
| Sensitivity | 96% |
| Specificity | 73% |
| Measurement performance at the level of individual OCT-B scans | |
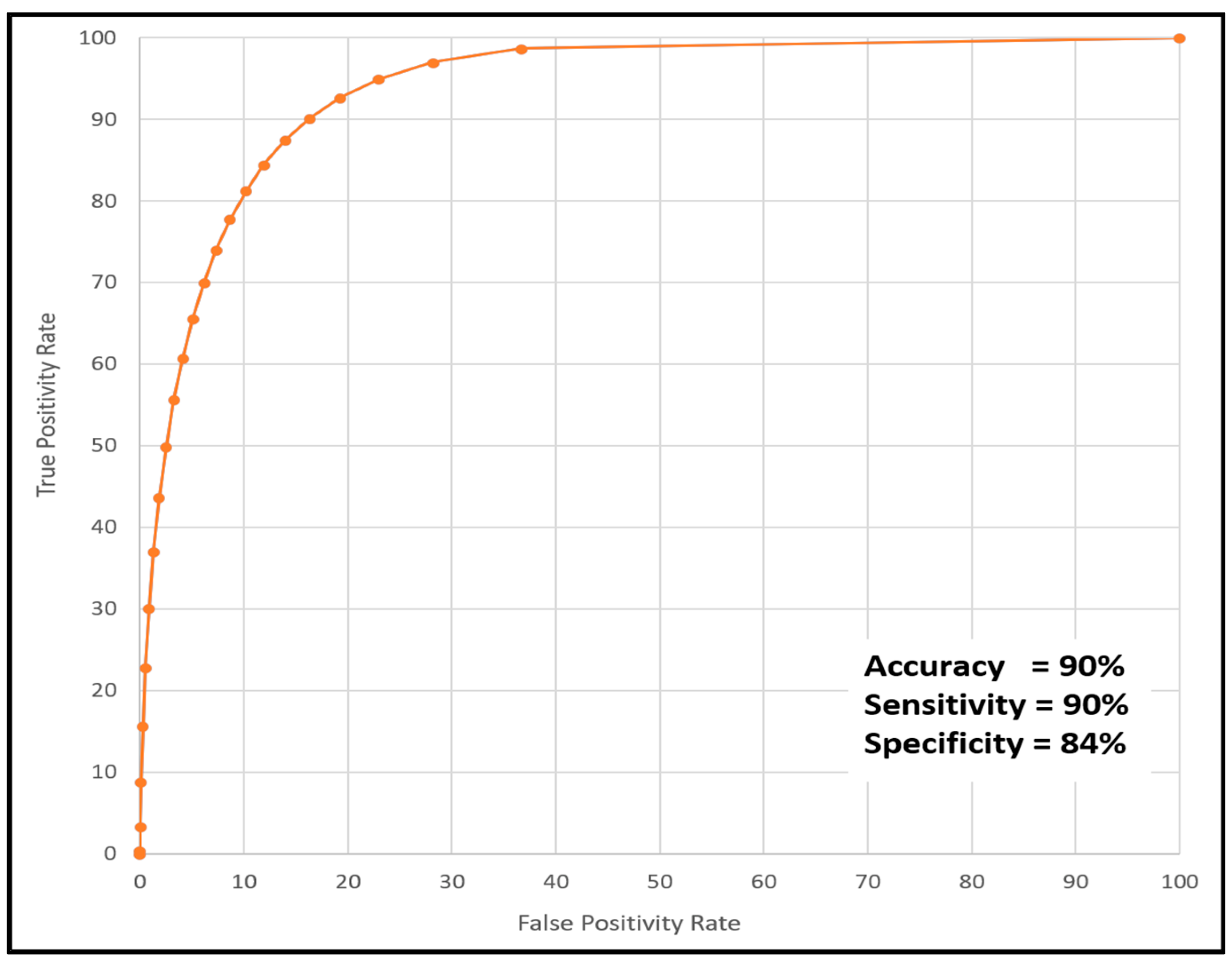
| AUC | 97% |
| Accuracy | 90% |
| Sensitivity | 90% |
| Specificity | 84% |
| ICC | 0.83 (p < 0.001) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kalra, G.; Cetin, H.; Whitney, J.; Yordi, S.; Cakir, Y.; McConville, C.; Whitmore, V.; Bonnay, M.; Reese, J.L.; Srivastava, S.K.; et al. Automated Identification and Segmentation of Ellipsoid Zone At-Risk Using Deep Learning on SD-OCT for Predicting Progression in Dry AMD. Diagnostics 2023, 13, 1178. https://doi.org/10.3390/diagnostics13061178
Kalra G, Cetin H, Whitney J, Yordi S, Cakir Y, McConville C, Whitmore V, Bonnay M, Reese JL, Srivastava SK, et al. Automated Identification and Segmentation of Ellipsoid Zone At-Risk Using Deep Learning on SD-OCT for Predicting Progression in Dry AMD. Diagnostics. 2023; 13(6):1178. https://doi.org/10.3390/diagnostics13061178
Chicago/Turabian StyleKalra, Gagan, Hasan Cetin, Jon Whitney, Sari Yordi, Yavuz Cakir, Conor McConville, Victoria Whitmore, Michelle Bonnay, Jamie L. Reese, Sunil K. Srivastava, and et al. 2023. "Automated Identification and Segmentation of Ellipsoid Zone At-Risk Using Deep Learning on SD-OCT for Predicting Progression in Dry AMD" Diagnostics 13, no. 6: 1178. https://doi.org/10.3390/diagnostics13061178