
Initial Serum Levels of Magnesium and Calcium as Predictors of Mortality in Traumatic Brain Injury Patients: A Retrospective Study
 ,
,
Abstract
:1. Introduction
Methods
2. Statistical Analysis
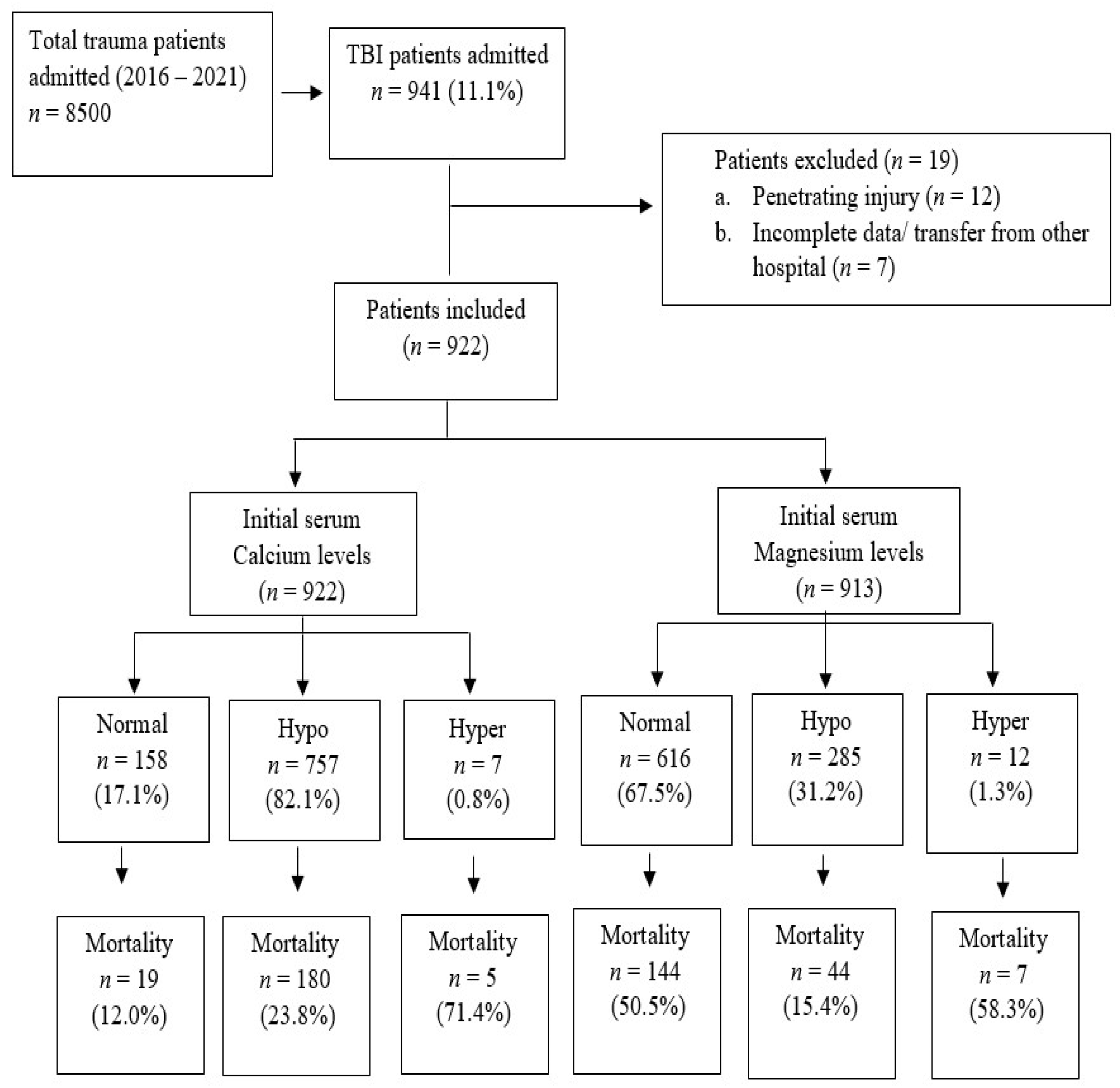
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rodriguez, S.R.; Mallonee, S.; Archer, P.; Gofton, J. Evaluation of death certificate-based surveillance for traumatic brain injurye—Oklahoma 2002. Public Health Rep. 2006, 121, 282–289. [Google Scholar] [CrossRef]
- Faul, M.D.; Wald, M.M.; Xu, L.; Coronado, V.G. Traumatic Brain Injury in the United States; Emergency Department Visits, Hospitalizations, and Deaths, 2002–2006; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2010. [Google Scholar]
- Bruns, J., Jr.; Hauser, W.A. The epidemiology of traumatic brain injury: A review. Epilepsia 2003, 44 (Suppl. 10), 2–10. [Google Scholar] [CrossRef] [PubMed]
- Fleminger, S.; Ponsford, J. Long term outcome after traumatic brain injury. BMJ 2005, 331, 1419–1420. [Google Scholar] [CrossRef] [PubMed]
- Rafiq, M.F.; Ahmed, N.; Khan, A.A. Serum electrolyte derangements in patients with traumatic brain injury. J. Ayub. Med. Coll. Abbottabad. 2013, 25, 162–164. [Google Scholar]
- Suman, S.; Kumar, N.; Singh, Y.; Kumar, V.; Yadav, G.; Gupta, B.K.; Pandey, A.R.; Pandey, S. Evaluation of Serum Electrolytes in Traumatic Brain Injury Patients: Prospective Randomized Observational Study. J. Anesth. Crit. Care Open Access 2016, 5, 00184. [Google Scholar]
- Holcomb, J.B.; McMullin, N.R.; Pearse, L.; Caruso, J.; Wade, C.E.; Oetjen-Gerdes, L.; Champion, H.R.; Lawnick, M.; Farr, W.; Rodriguez, S.; et al. Causes of death in, U.S. Special Operations Forces in the global war on terrorism: 2001–2004. Ann Surg. 2007, 245, 986–991. [Google Scholar] [CrossRef]
- Ditzel, R.M., Jr.; Anderson, J.L.; Eisenhart, W.J.; Rankin, C.J.; DeFeo, D.R.; Oak, S.; Siegler, J. A review of transfusion- and traumainduced hypocalcemia: Is it time to change the lethal triad to the lethal diamond? J. Trauma Acute Care Surg. 2020, 88, 434–439. [Google Scholar] [CrossRef]
- Cannon, J.W.; Khan, M.A.; Raja, A.S.; Cohen, M.J.; Como, J.J.; Cotton, B.A.; Dubose, J.J.; Erin, E.; Inaba, K.; Duchesne, J.C.; et al. Damage control resuscitation in patients with severe traumatic hemorrhage. J. Trauma Acute Care Surg. 2017, 82, 605–617. [Google Scholar] [CrossRef] [Green Version]
- Wray, J.P.; Bridwell, R.E.; Schauer, S.G.; Shackelford, S.A.; Bebarta, V.S.; Wright, F.L.; Bynum, J.; Long, B. The diamond of death: Hypocalcemia in trauma and resuscitation. Am. J. Emerg. Med. 2021, 41, 104–109. [Google Scholar] [CrossRef]
- Fox, C.; Ramsoomair, D.; Carter, C. Magnesium: Its proven and potential clinical significance. South Med. J. 2001, 94, 1195–1202. [Google Scholar] [CrossRef]
- Ozgurtas, T.; Kahraman, S. State of the art of new data on the role of magnesium in brain injury: Clinical interest of measurements of total and ionized magnesium. Magnes Res. 2004, 17, 327–334. [Google Scholar]
- Teasdale, G.; Jennett, B. Assessment of coma and impaired consciousness: A practical scale. Lancet 1974, 2, 81–84. [Google Scholar] [CrossRef] [PubMed]
- Copes, W.S.; Champion, H.R.; Sacco, W.J.; Lawnick, M.M.; Gann, D.S.; Gennarelli, T.; MacKenzie, E.; Schwaitzberg, S. Progress in characterizing anatomic injury. J. Trauma 1990, 30, 1200–1207. [Google Scholar] [CrossRef] [PubMed]
- Baker, S.P.; O’Neill, B.; Haddon, W., Jr.; Long, W.B. The injury severity score: A method for describing patients with multiple injuries and evaluating emergency care. J. Trauma 1974, 14, 187–196. [Google Scholar] [CrossRef]
- Cherry, R.A.; Bradburn, E.; Carney, D.E.; Shaffer, M.L.; Gabbay, R.A.; Cooney, R.N. Do early ionized calcium levels really matter in trauma patients? J. Trauma 2006, 61, 774–779. [Google Scholar] [CrossRef]
- Magnotti, L.J.; Bradburn, E.H.; Webb, D.L.; Berry, S.D.; Fischer, P.E.; Zarzaur, B.L.; Schroeppel, T.J.; Fabian, T.C.; Croce, M.A. Admission ionized calcium levels predict the need for multiple transfusions: A prospective study of 591 critically ill trauma patients. J. Trauma 2011, 70, 391–395. [Google Scholar] [CrossRef]
- Vasudeva, M.; Mathew, J.K.; Fitzgerald, M.C.; Cheung, Z.; Mitra, B. Hypocalcaemia and traumatic coagulopathy: An observational analysis. Vox Sang. 2020, 115, 189–195. [Google Scholar] [CrossRef]
- Sen, A.P.; Gulati, A. Use of magnesium in traumatic brain injury. Neurotherapeutics 2010, 7, 91–99. [Google Scholar] [CrossRef] [Green Version]
- Vinas-Rios, J.M.; Sanchez-Aguilar, M.; Sanchez-Rodriguez, J.J.; Gonzalez-Aguirre, D.; Heinen, C.; Meyer, F.; Kretschmer, T. Hypocalcaemia as a prognostic factor of early mortality in moderate and severe traumatic brain injury. Neurol. Res. 2014, 36, 102–106. [Google Scholar] [CrossRef]
- Manuel, V.R.; Martin, S.A.; Juan, S.R.; Fernando, M.A.; Frerk, M.; Thomas, K.; Christian, H. Hypocalcemia as a prognostic factor in mortality and morbidity in moderate and severe traumatic brain injury. Asian J. Neurosurg. 2015, 10, 190–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polderman, K.H.; Bloemers, F.W.; Peerdeman, S.M.; Girbes, A.R. Hypomagnesemia and hypophosphatemia at admission in patients with severe head injury. Crit. Care Med. 2000, 28, 2022–2025. [Google Scholar] [CrossRef] [PubMed]
- Mendez, D.R.; Corbett, R.; Macias, C.; Laptook, A. Total and ionized plasma magnesium concentrations in children after traumatic brain injury. Pediatr. Res. 2005, 57, 347–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, R.; He, M.; Xu, J. Initial Serum Magnesium Level Is Associated with Mortality Risk in Traumatic Brain Injury Patients. Nutrients 2022, 14, 4174. [Google Scholar] [CrossRef]
- Laupland, K.B.; Tabah, A.; Jacobs, N.; Ramanan, M. Determinants of serum magnesium abnormalities and outcome among admissions to the intensive care unit. Anaesth. Crit Care Pain Med. 2020, 39, 793–797. [Google Scholar] [CrossRef] [PubMed]
- Dey, S.; Kumar, R.; Tarat, A. Evaluation of Electrolyte Imbalance in Patients with Traumatic Brain Injury Admitted in the Central ICU of a Tertiary Care Centre: A Prospective Observational Study. Cureus 2021, 28, e17517. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Value |
|---|---|
| Age [mean± standard deviation (SD)] | 32.2 ± 15.0 |
| Males | 863 (93.6%) |
| TBI types | |
| Epidural hematoma | 204 (22.1%) |
| Subdural hematoma | 321 (34.8%) |
| Subarachnoid hemorrhage | 387 (42.0%) |
| Compression of basal cisterns | 110 (11.9%) |
| Effacement of Sulci | 171 (18.5%) |
| Midline Shifts | 206 (22.3%) |
| Injury Severity Score [median (interquartile range, IQR)] | 27 (18–34) |
| Glasgow Coma Scale [median (IQR)] | 3 (3–9) |
| Shock index [median (IQR)] | 0.8 (0.7–1.0) |
| Abbreviated Injury Scale (AIS) (mean ± SD) | |
| Head AIS | 3.9 ± 0.97 |
| Chest AIS | 2.78 ± 0.70 |
| Abdomen AIS | 2.65 ± 1.0 |
| Cervical spine AIS | 2.26 ± 0.67 |
| Thoracic spine AIS | 2.16 ± 0.65 |
| Lumbar spine AIS | 2.01 ± 0.09 |
| Laboratory findings [median (IQR)] | |
| Initial serum Sodium | 141.0 (139–143) |
| Initial serum Potassium | 3.8 (3.4–4.1) |
| Initial serum Calcium | 2.0 (1.8–2.1) |
| Initial serum Magnesium | 0.7 (0.6–0.8) |
| Initial serum Phosphate | 0.9 (0.7–1.2) |
| Initial serum Bicarbonate | 19.6 (16.7–23.0) |
| Initial serum Lactic acid | 2.9 (2.0–4.3) |
| Prothrombin time [median (IQR)] | 12.0 (11.1–13.5) |
| Activated partial thromboplastin time [median (IQR)] | 26.2 (24.0–31.0) |
| International normalized ratio [median (IQR)] | 1.1 (1.1–1.3) |
| Initial serum hemoglobin [median (IQR)] | 13.0 (11.3–14.4) |
| Initial serum glucose [median (IQR)] | 8.0 (6.7–10.1) |
| Intubation | 827 (89.7%) |
| Massive transfusion protocol activation | 138 (15.0%) |
| Ventilator associated pneumonia | 121 (13.1%) |
| Mechanical ventilator days [median (IQR)] | 5 (2–11) |
| Intensive care unit days [median (IQR)] | 9 (4–17) |
| Hospital length of stay [median (IQR)] | 17 (7–32) |
| In-hospital mortality | 204 (22.1%) |
| Mild GCS (13–15) (n = 88) | Moderate (9–12) (n = 144) | Severe (3–8) (n = 681) | Total | |
|---|---|---|---|---|
| Initial serum calcium (Ca) levels at admission | ||||
| Normal | 29 (33.0%) | 49 (34.0%) | 79 (11.6%) | 157 (17.2%) |
| Hypocalcemia | 59 (67.0%) | 94 (65.3%) | 596 (87.5%) | 749 (82.0%) |
| Hypercalcemia | 0 | 1 (0.7%) | 6 (0.9%) | 7 (0.8%) |
| Total | 88 (100%) | 144 (100%) | 681 (100%) | 913 (100%) * |
| Initial serum magnesium (Mg) levels at admission | ||||
| Normal | 64 (72.7%) | 97 (67.4%) | 449 (66.8%) | 610 (67.5%) |
| Hypomagnesemia | 24 (27.3%) | 46 (31.9%) | 212 (31.5%) | 282 (31.2%) |
| Hypermagnesemia | 0 | 1 (0.7%) | 11 (1.6%) | 12 (1.3%) |
| Total | 88 (100%) | 144 (100%) | 672 (100%) | 904 (100%) * |
| Initial Calcium Imbalance | ||||||||
| Normal (n = 158) | Hypercalcemia (n = 7) | Hypocalcemia (n = 757) | Total (n = 922) | |||||
| TBI Types | ||||||||
| Epidural hemorrhage | 41 | 25.9% | 1 | 14.3% | 162 | 21.4% | 204 | 22.1% |
| Subdural hemorrhage | 43 | 27.2% | 1 | 14.3% | 277 | 36.6% | 321 | 34.8% |
| Subarachnoid hemorrhage | 51 | 32.3% | 2 | 28.6% | 334 | 44.1% | 387 | 42.0% |
| Compression of basal cisterns | 18 | 11.4% | 2 | 28.6% | 90 | 11.9% | 110 | 11.9% |
| Effacement of sulci | 35 | 22.2% | 4 | 57.1% | 132 | 17.4% | 171 | 18.5% |
| Midline shift | 34 | 21.5% | 1 | 14.3% | 171 | 22.6% | 206 | 22.3% |
| Initial Magnesium imbalance | ||||||||
| Normal (n = 616) | Hypermagnesemia (n = 12) | Hypomagnesemia (n = 285) | Total (n = 913) | |||||
| TBI Types | ||||||||
| Epidural hemorrhage | 145 | 23.5% | 1 | 8.3% | 58 | 20.4% | 204 | 22.3% |
| Subdural hemorrhage | 205 | 33.3% | 3 | 25.0% | 111 | 38.9% | 319 | 34.9% |
| Subarachnoid hemorrhage | 250 | 40.6% | 7 | 58.3% | 128 | 44.9% | 385 | 42.2% |
| Compression of basal cisterns | 80 | 13.0% | 3 | 25.0% | 24 | 8.4% | 107 | 11.7% |
| Effacement of sulci | 112 | 18.2% | 4 | 33.3% | 54 | 18.9% | 170 | 18.6% |
| Midline shift | 136 | 22.1% | 3 | 25.0% | 67 | 23.5% | 206 | 22.6% |
| Variables | Normal Ca Level (n = 158, 17.3%) | Hypocalcemia (n = 757, 82.7%) | p-Value | Normal Mg Level (n = 616, 68.4%) | Hypomagnesemia (n = 285, 31.6%) | p-Value |
|---|---|---|---|---|---|---|
| Age | 32.5 ± 17.2 | 32.2 ± 14.5 | 0.843 | 32.0 ± 15.3 | 32.5 ± 14.1 | 0.645 |
| Males | 144 (91.1) | 713 (94.2) | 0.153 | 580 (94.2) | 264 (92.6) | 0.382 |
| Epidural hematoma | 41 (25.9) | 162 (21.4) | 0.211 | 145 (23.5) | 58 (20.4) | 0.287 |
| Subdural hematoma | 43 (27.2) | 277 (36.6) | 0.025 | 205 (33.3) | 111 (38.9) | 0.097 |
| Subarachnoid hemorrhage | 51 (32.3) | 334 (44.1) | 0.006 | 250 (40.6) | 128 (44.9) | 0.221 |
| Compression of basal cisterns | 18 (11.4) | 90 (11.9) | 0.860 | 80 (13.0) | 24 (8.4) | 0.046 |
| Effacement of sulci | 35 (22.2) | 132 (17.4) | 0.163 | 112 (18.2) | 54 (18.9) | 0.076 |
| Midline shifts | 34 (21.5) | 171 (22.6) | 0.769 | 136 (22.1) | 57 (23.5) | 0.633 |
| Intubation | 121 (76.6) | 699 (92.3) | 0.001 | 537 (87.2) | 269 (94.4) | 0.001 |
| Massive transfusion protocol | 9 (6.7) | 127 (16.8) | 0.001 | 83 (13.5) | 45 (15.8) | 0.355 |
| Craniotomy/craniectomy | 30 (19.0) | 160 (21.1) | 0.545 | 120 (19.5) | 70 (24.6) | 0.082 |
| Ventilator associated pneumonia | 11 (7.0) | 109 (14.4) | 0.012 | 77 (12.5) | 44 (15.4) | 0.229 |
| Glasgow Coma Scale | 8 (3–12) | 3 (3–8) | 0.001 | 3 (3–9) | 3 (3–8) | 0.208 |
| Head AIS | 3.97 ± 0.97 | 3.91 ± 0.97 | 0.702 | 3.9 ± 0.9 | 3.9 ± 1.0 | 0.951 |
| Injury Severity Score | 22.8 ± 10.5 | 27.7 ± 10.2 | 0.001 | 26.3 ± 10.4 | 28.0 ± 10.5 | 0.024 |
| Mechanical ventilator days | 2 (1–7.5) | 6 (2–12) | 0.001 | 4 (1–11) | 7 (3–12) | 0.001 |
| Intensive care unit days | 6 (2–12) | 8 (3–17) | 0.012 | 7 (3–14) | 10.5 (5–18) | 0.001 |
| Hospital length of stay in days | 12 (5–22) | 17 (7–31) | 0.003 | 14 (6–28) | 20.5 (10–35) | 0.001 |
| In-hospital mortality | 19 (12.0) | 180 (23.8) | 0.001 | 144 (23.4) | 44 (15.4) | 0.006 |
| Variables | Normal Ca Level (n = 158, 17.3%) | Hypocalcemia (n = 757, 82.7%) | p-Value | Normal Mg Level (n = 616, 68.4%) | Hypomagnesemia (n = 285, 31.6%) | p-Value |
|---|---|---|---|---|---|---|
| Initial serum sodium | 140.0 ± 4.0 | 141.3 ± 4.9 | 0.002 | 140.9 ± 4.5 | 141.2 ± 4.4 | 0.382 |
| Initial serum potassium | 3.8 ± 0.6 | 3.8 ± 0.7 | 0.175 | 3.82 ± 0.6 | 3.77 ± 0.6 | 0.273 |
| Initial serum calcium | 2.34 ± 0.23 | 1.90 ± 0.20 | 0.001 | 2.01 ± 0.26 | 1.90 ± 0.24 | 0.001 |
| Initial serum magnesium | 0.75 ± 0.13 | 0.69 ± 0.11 | 0.001 | 0.74 ± 0.07 | 0.59 ± 0.05 | 0.001 |
| Initial serum phosphate | 1.0 ± 0.4 | 1.0 ± 0.5 | 0.763 | 1.04 ± 0.46 | 0.93 ± 0.35 | 0.001 |
| Initial serum bicarbonate | 21.5 ± 4.5 | 19.0 ± 4.1 | 0.001 | 4.17 ± 0.16 | 3.95 ± 0.23 | 0.092 |
| Initial serum lactic acid | 3.8 ± 2.9 | 3.7 ± 2.7 | 0.680 | 3.80 ± 2.81 | 3.24 ± 1.88 | 0.001 |
| Initial serum hemoglobin | 13.7 ± 2.4 | 12.5 ± 2.3 | 0.001 | 12.80 ± 2.32 | 12.53 ± 2.42 | 0.120 |
| Initial serum glucose | 11.5 ± 4.9 | 8.5 ± 3.8 | 0.001 | 9.08 ± 3.96 | 8.71 ± 3.43 | 0.175 |
| Prothrombin time | 12.1 ± 3.3 | 13.8 ± 9.3 | 0.001 | 13.29 ± 6.76 | 12.60 ± 3.13 | 0.036 |
| Activated partial thromboplastin time | 29.3 ± 16.8 | 32.8 ± 23.0 | 0.030 | 31.39 ± 18.55 | 30.23 ± 16.77 | 0.369 |
| International normalized ratio | 3.8 ± 2.9 | 1.3 ± 0.8 | 0.001 | 1.27 ± 0.58 | 1.23 ± 0.28 | 0.039 |
| Odds Ratio | 95% CI Lower | 95% CI Upper | p-Value | |
|---|---|---|---|---|
| Initial serum sodium | 1.024 | 0.974 | 1.077 | 0.345 |
| Initial serum potassium | 1.112 | 0.792 | 1.563 | 0.539 |
| Initial serum calcium | 0.523 | 0.202 | 1.355 | 0.182 |
| Initial serum bicarbonate | 0.926 | 0.869 | 0.987 | 0.018 |
| Initial serum phosphate | 0.963 | 0.596 | 1.555 | 0.877 |
| Initial serum magnesium | 16.315 | 2.381 | 111.771 | 0.004 |
| Initial serum hemoglobin | 1.034 | 0.933 | 1.146 | 0.526 |
| Injury severity score | 1.052 | 1.028 | 1.077 | 0.001 |
| GCS on admission | 0.887 | 0.824 | 0.955 | 0.001 |
| Prothrombin time | 1.034 | 0.859 | 1.244 | 0.726 |
| Activated partial thromboplastin time | 1.049 | 1.022 | 1.077 | 0.001 |
| International normalized ratio | 2.34 | 0.294 | 18.632 | 0.422 |
| Initial serum lactate level | 1.156 | 1.053 | 1.269 | 0.002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mekkodathil, A.; El-Menyar, A.; Hakim, S.; Al Jogol, H.; Parchani, A.; Peralta, R.; Rizoli, S.; Al-Thani, H. Initial Serum Levels of Magnesium and Calcium as Predictors of Mortality in Traumatic Brain Injury Patients: A Retrospective Study. Diagnostics 2023, 13, 1172. https://doi.org/10.3390/diagnostics13061172
Mekkodathil A, El-Menyar A, Hakim S, Al Jogol H, Parchani A, Peralta R, Rizoli S, Al-Thani H. Initial Serum Levels of Magnesium and Calcium as Predictors of Mortality in Traumatic Brain Injury Patients: A Retrospective Study. Diagnostics. 2023; 13(6):1172. https://doi.org/10.3390/diagnostics13061172
Chicago/Turabian StyleMekkodathil, Ahammed, Ayman El-Menyar, Suhail Hakim, Hisham Al Jogol, Ashok Parchani, Ruben Peralta, Sandro Rizoli, and Hassan Al-Thani. 2023. "Initial Serum Levels of Magnesium and Calcium as Predictors of Mortality in Traumatic Brain Injury Patients: A Retrospective Study" Diagnostics 13, no. 6: 1172. https://doi.org/10.3390/diagnostics13061172