


Early Changes in Acute Myocardial Infarction in Pigs: Achieving Early Detection with Wearable Devices

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
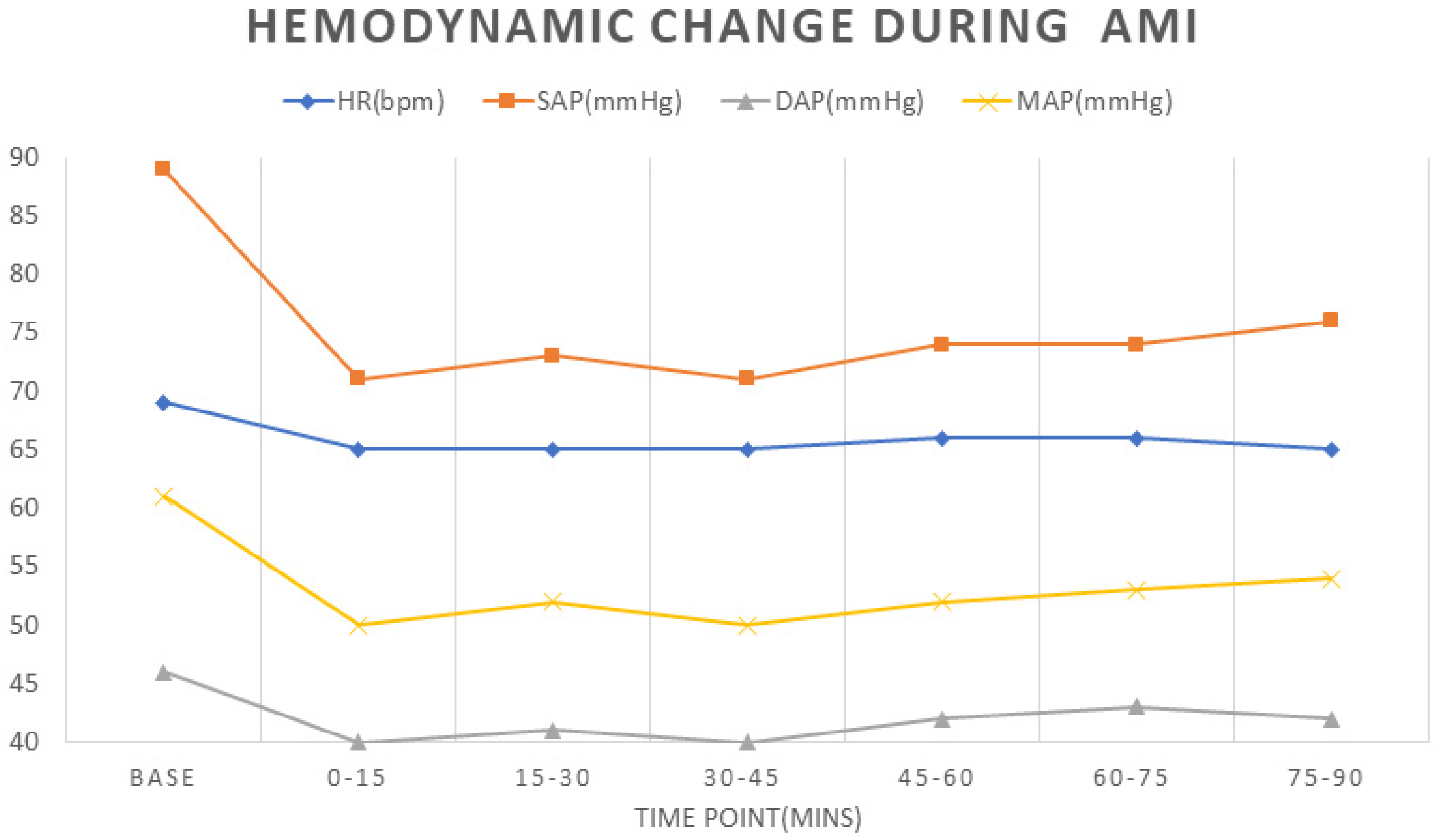
3.1. Hemodynamic Data
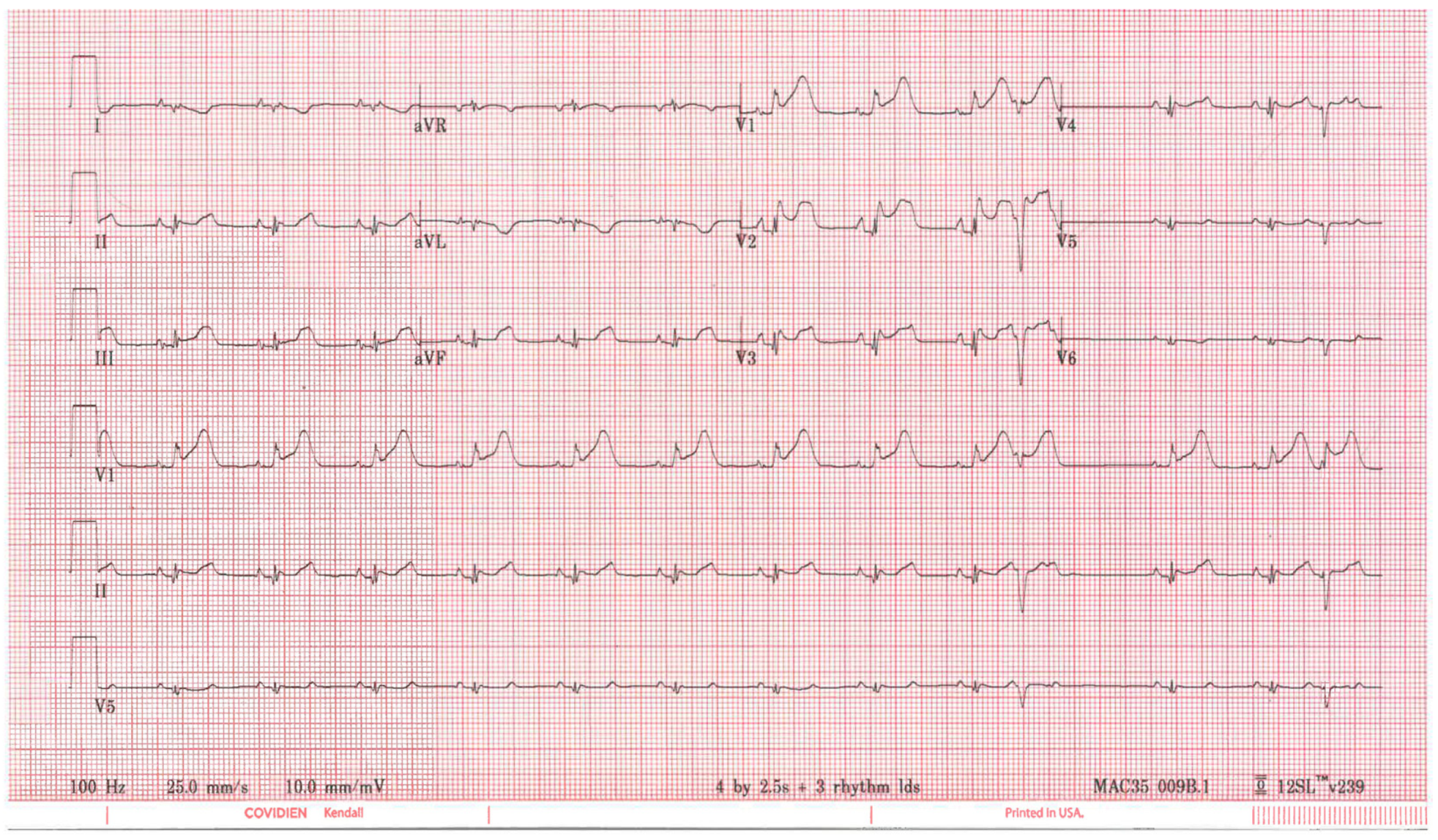
3.2. ECG
3.3. Biomarkers
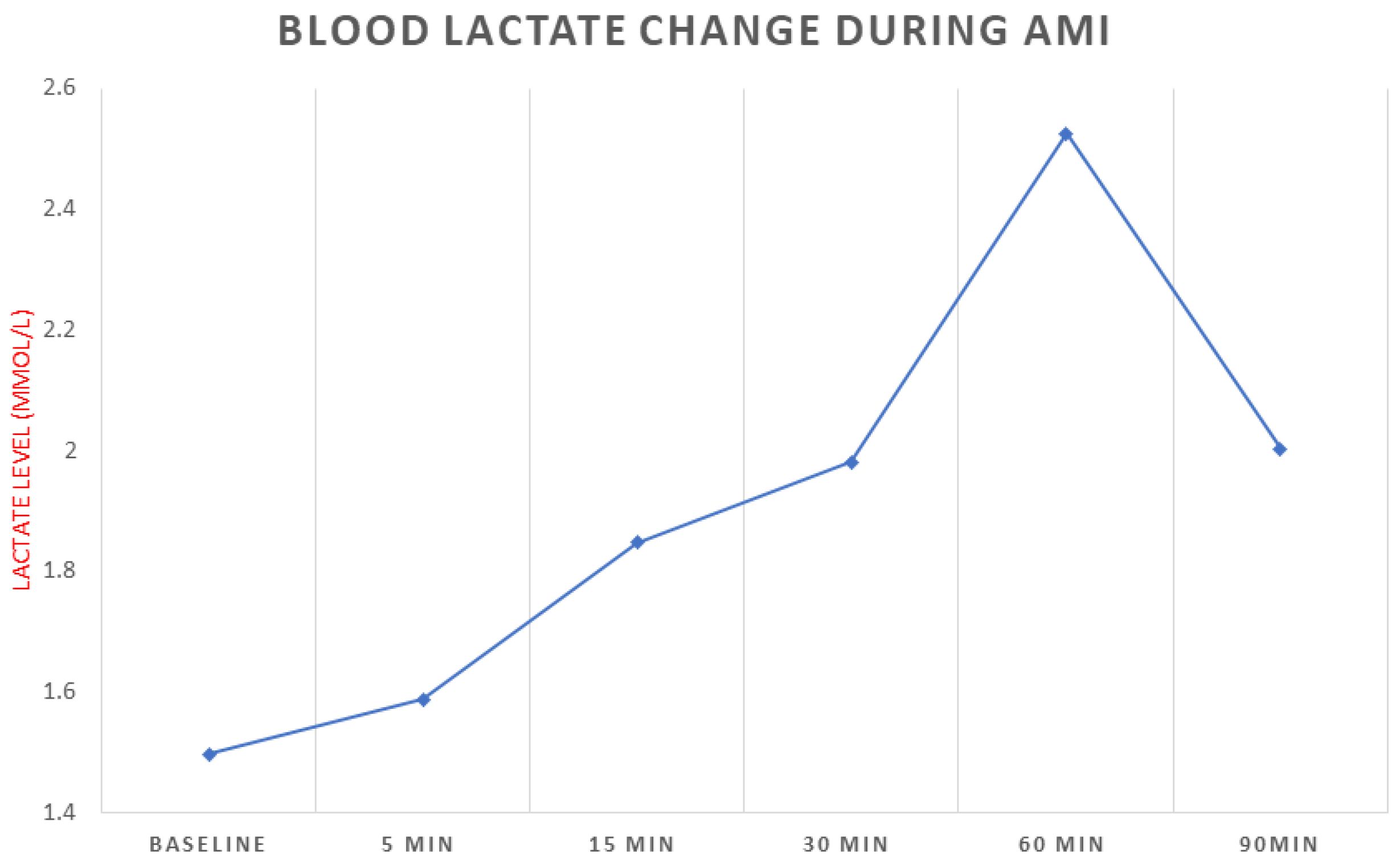
3.3.1. Blood Lactate
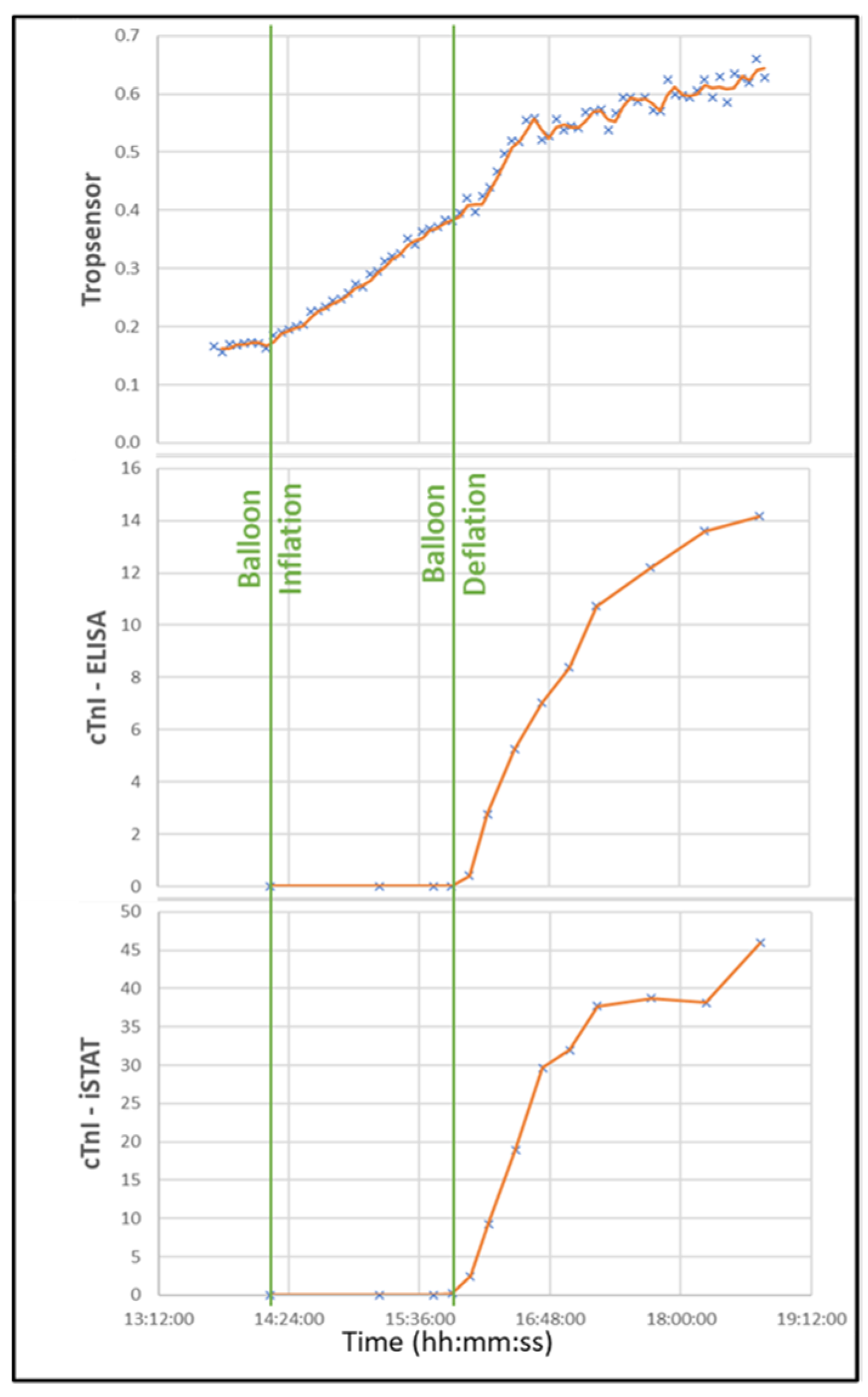
3.3.2. Troponin
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Twerenbold, R.; Reichlin, T.; Reiter, M.; Muller, C. High-sensitive cardiac troponin: Friend or foe? Swiss Med. Wkly. 2011, 141, w13202. [Google Scholar] [CrossRef] [PubMed]
- Thygesen, K.; Mair, J.; Giannitsis, E.; Mueller, C.; Lindahl, B.; Blankenberg, S.; Huber, K.; Plebani, M.; Biasucci, L.M.; Tubaro, M.; et al. How to use high-sensitivity cardiac troponins in acute cardiac care. Eur. Heart J. 2012, 33, 2252–2257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Denktas, A.E.; Anderson, H.V.; McCarthy, J.; Smalling, R.W. Total ischemic time: The correct focus of attention for optimal ST-segment elevation myocardial infarction care. JACC Cardiovasc. Interv. 2011, 4, 599–604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finn, J.C.; Bett, J.H.; Shilton, T.R.; Cunningham, C.; Thompson, P.L.; National Heart Foundation of Australia Chest Pain Every Minute Counts Working Group. Patient delay in responding to symptoms of possible heart attack: Can we reduce time to care? Med. J. Aust. 2007, 187, 293–298. [Google Scholar] [CrossRef]
- Hand, M.; Brown, C.; Horan, M.; Simons-Morton, D. The National Heart Attack Alert Program: Progress at 5 years in educating providers, patients, and the public and future directions. J. Thromb. Thrombolysis 1998, 6, 9–17. [Google Scholar] [CrossRef]
- Rubini Gimenez, M.; Twerenbold, R.; Reichlin, T.; Wildi, K.; Haaf, P.; Schaefer, M.; Zellweger, C.; Moehring, B.; Stallone, F.; Sou, S.M.; et al. Direct comparison of high-sensitivity-cardiac troponin I vs. T for the early diagnosis of acute myocardial infarction. Eur. Heart J. 2014, 35, 2303–2311. [Google Scholar] [CrossRef] [Green Version]
- Moser, D.K.; Kimble, L.P.; Alberts, M.J.; Alonzo, A.; Croft, J.B.; Dracup, K.; Evenson, K.R.; Go, A.S.; Hand, M.M.; Kothari, R.U.; et al. Reducing delay in seeking treatment by patients with acute coronary syndrome and stroke: A scientific statement from the American Heart Association Council on cardiovascular nursing and stroke council. Circulation 2006, 114, 168–182. [Google Scholar] [CrossRef] [Green Version]
- Danchin, N.; Blanchard, D.; Steg, P.G.; Sauval, P.; Hanania, G.; Goldstein, P.; Cambou, J.P.; Gueret, P.; Vaur, L.; Boutalbi, Y.; et al. Impact of prehospital thrombolysis for acute myocardial infarction on 1-year outcome: Results from the French Nationwide USIC 2000 Registry. Circulation 2004, 110, 1909–1915. [Google Scholar] [CrossRef] [Green Version]
- Arnadottir, A.; Pedersen, S.; Bo Hasselbalch, R.; Goetze, J.P.; Friis-Hansen, L.J.; Bloch-Munster, A.M.; Skov Jensen, J.; Bundgaard, H.; Iversen, K. Temporal release of high-sensitivity cardiac troponin t and i and copeptin after brief induced coronary artery balloon occlusion in humans. Circulation 2021, 143, 1095–1104. [Google Scholar] [CrossRef]
- De Luca, G.; Suryapranata, H.; Ottervanger, J.P.; Antman, E.M. Time delay to treatment and mortality in primary angioplasty for acute myocardial infarction: Every minute of delay counts. Circulation 2004, 109, 1223–1225. [Google Scholar] [CrossRef] [Green Version]
- Gersh, B.J.; Stone, G.W.; White, H.D.; Holmes, D.R., Jr. Pharmacological facilitation of primary percutaneous coronary intervention for acute myocardial infarction: Is the slope of the curve the shape of the future? JAMA 2005, 293, 979–986. [Google Scholar] [CrossRef] [PubMed]
- Simoons, M.L.; Serruys, P.W.; van den Brand, M.; Res, J.; Verheugt, F.W.; Krauss, X.H.; Remme, W.J.; Bar, F.; de Zwaan, C.; van der Laarse, A.; et al. Early thrombolysis in acute myocardial infarction: Limitation of infarct size and improved survival. J. Am. Coll. Cardiol. 1986, 7, 717–728. [Google Scholar] [CrossRef] [Green Version]
- Krumholz, H.M.; Normand, S.T.; Wang, Y. Twenty-year trends in outcomes for older adults with acute myocardial infarction in the United States. JAMA Netw. Open 2019, 2, e191938. [Google Scholar] [CrossRef] [PubMed]
- Itelman, E.; Shlomai, G.; Leibowitz, A.; Weinstein, S.; Yakir, M.; Tamir, I.; Sagiv, M.; Muhsen, A.; Perelman, M.; Kant, D.; et al. Assessing the usability of a novel wearable remote patient monitoring device for the early detection of in-hospital patient deterioration: Observational study. JMIR Form. Res. 2022, 6, e36066. [Google Scholar] [CrossRef] [PubMed]
- Barrett, P.M.; Komatireddy, R.; Haaser, S.; Topol, S.; Sheard, J.; Encinas, J.; Fought, A.J.; Topol, E.J. Comparison of 24-hour Holter monitoring with 14-day novel adhesive patch electrocardiographic monitoring. Am. J. Med. 2014, 127, 95.e11–95.e17. [Google Scholar] [CrossRef] [Green Version]
- Lazzeri, C.; Valente, S.; Chiostri, M.; Gensini, G.F. Clinical significance of lactate in acute cardiac patients. World J. Cardiol. 2015, 26, 483–489. [Google Scholar] [CrossRef] [PubMed]
- Gjesdal, G.; Braun, O.Ö.; Smith, J.G.; Scherstén, F.; Tydén, P. Blood lactate is a predictor of short-term mortality in patients with myocardial infarction complicated by heart failure but without cardiogenic shock. BMC Cardiovasc. Disord. 2018, 18, 8. [Google Scholar] [CrossRef] [Green Version]
- Park, I.H.; Cho, H.K.; Oh, J.H.; Chun, W.J.; Park, Y.H.; Lee, M.; Kim, M.S.; Choi, K.H.; Kim, J.; Song, Y.B.; et al. Clinical significance of serum lactate in acute myocardial infarction: A cardiac magnetic resonance imaging study. J. Clin. Med. 2021, 10, 5278. [Google Scholar] [CrossRef]
- Titus, J.; Wu, A.H.B.; Biswal, S.; Burman, A.; Sengupta, S.P.; Sengupta, P.P. Development and preliminary validation of infrared spectroscopic device for transdermal assessment of elevated cardiac troponin. Commun. Med. 2022, 2, 42. [Google Scholar] [CrossRef] [PubMed]
- Raine, D. Rockley Photonics and Medtronic Collaborate to Deliver the Next Generation of Wearable Healthcare Monitoring Devices. Available online: https://investors.rockleyphotonics.com/news/news-details/2022/Rockley-photonics-and-Medtronic-Collaborate-to-Deliver-the-Next-Generation-of-Wearable-Healthcare-Monitoring-Devices/default.aspx (accessed on 14 October 2022).
- Redon, P.; Shahzad, A.; Iqbal, T.; Wijns, W. Development of a new detection algorithm to identify acute coronary syndrome using electrochemical biosensors for real-world long-term monitoring. Bioengineering 2021, 8, 28. [Google Scholar] [CrossRef]
- Chien, M.-N.; Fan, S.-H.; Huang, C.-H.; Wu, C.-C.; Huang, J.-T. Continuous lactate monitoring system based on percutaneous microneedle array. Sensors 2022, 22, 1468. [Google Scholar] [CrossRef]
- Fung, E.; Jarvelin, M.R.; Doshi, R.N.; Shinbane, J.S.; Carlson, S.K.; Grazette, L.P.; Chang, P.M.; Sangha, R.S.; Huikuri, H.V.; Peters, N.S. Electrocardiographic patch devices and contemporary wireless cardiac monitoring. Front. Physiol. 2015, 6, 149. [Google Scholar] [CrossRef] [Green Version]
- Take an ECG with the ECG App on Apple Watch. Available online: https://support.apple.com/en-us/HT208955 (accessed on 14 October 2022).
- Avila, C.O. Novel use of Apple Watch 4 to obtain 3-lead electrocardiogram and detect cardiac ischemia. Perm. J. 2019, 23, 19–025. [Google Scholar] [CrossRef] [Green Version]
- Cobos Gil, M. Standard and precordial leads obtained with an Apple Watch. Ann. Intern. Med. 2020, 172, 436–437. [Google Scholar] [CrossRef]
- Drexler, M.; Elsner, C.; Gabelmann, V.; Gori, T.; Munzel, T. Apple Watch detecting coronary ischaemia during chest pain episodes or an apple a day may keep myocardial infarction away. Eur. Heart J. 2020, 41, 2224. [Google Scholar] [CrossRef] [PubMed]
- Spaccarotella, C.A.M.; Polimeni, A.; Migliarino, S.; Principe, E.; Curcio, A.; Mongiardo, A.; Sorrentino, S.; De Rosa, S.; Indolfi, C. Multichannel electrocardiograms obtained by a smartwatch for the diagnosis of ST-segment changes. JAMA Cardiol. 2020, 5, 1176–1180. [Google Scholar] [CrossRef]
- Stark, K.; Czermak, T.; Massberg, S.; Orban, M. Watch out for ST-elevation myocardial infarction: A case report of ST-elevation in single-lead electrocardiogram tracing of a smartwatch. Eur. Heart J. Case Rep. 2020, 4, 1–4. [Google Scholar] [CrossRef]
- Li, K.; Elgalad, A.; Cardoso, C.; Perin, E.C. Using the Apple Watch to record multiple-lead electrocardiograms in detecting myocardial infarction: Where are we now? Tex. Heart Inst. J. 2022, 49, e227845. [Google Scholar] [CrossRef] [PubMed]
- Han, C.; Song, Y.; Lim, H.S.; Tae, Y.; Jang, J.H.; Lee, B.T.; Lee, Y.; Bae, W.; Yoon, D. Automated detection of acute myocardial infarction using asynchronous electrocardiogram signals-preview of implementing artificial intelligence with multichannel electrocardiographs obtained from smartwatches: Retrospective study. J. Med. Internet Res. 2021, 23, e31129. [Google Scholar] [CrossRef] [PubMed]
- Sopic, D.; Aminifar, A.; Aminifar, A.; Atienza, D. Real-time event-driven classification technique for early detection and prevention of myocardial infarction on wearable systems. IEEE Trans. Biomed. Circuits Syst. 2018, 12, 982–992. [Google Scholar] [CrossRef] [Green Version]
- Chandrasekaran, R.; Katthula, V.; Moustakas, E. Patterns of use and key predictors for the use of wearable health care devices by US Adults: Insights from a national survey. J. Med. Internet Res. 2020, 22, e22443. [Google Scholar] [CrossRef] [PubMed]
- Wearable Devices Market Share. Available online: https://www.idc.com/promo/wearablevendor (accessed on 14 October 2022).
- Healthcare Analytics Market Share, Size, Trends, Industry Analysis Report, by Type (Descriptive Analytics, Predictive Analytics, Prescriptive Analytics), by Application (Clinical, Financial, Operational & Administrative), by End-Use; by Delivery Mode; by Regions; Segment Forecast, 2021–2028. Available online: https://www.polarismarketresearch.com/industry-analysis/healthcare-analytics-market (accessed on 14 October 2022).
- Worldwide Quarterly Wearable Device Tracker. Available online: https://www.idc.com/getdoc.jsp?containerId=IDC_P31315 (accessed on 14 October 2022).
- Sandoval, Y.; Apple, F.S.; Mahler, S.A.; Body, R.; Collinson, P.O.; Jaffe, A.S.; International Federation of Clinical Chemistry and Laboratory Medicine Committee on the Clinical Application of Cardiac Biomarkers. High-sensitivity cardiac troponin and the 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR guidelines for the evaluation and diagnosis of acute chest pain. Circulation 2022, 146, 569–581. [Google Scholar] [CrossRef]
- McCord, J.; Aurora, L.; Lindahl, B.; Giannitsis, E.; Calle-Muller, C.; Nowak, R.; Body, R.; Christ, M.; deFilippi, C.R.; Christenson, R.H.; et al. Symptoms predictive of acute myocardial infarction in the troponin era: Analysis from the TRAPID-AMI study. Crit. Pathw. Cardiol. 2019, 18, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Shi, J.; Pommier, T.; Cottin, Y.; Salomon, M.; Decourselle, T.; Lalande, A.; Couturier, R. Prediction of myocardial infarction from patient features with machine learning. Front. Cardiovasc. Med. 2022, 9, 754609. [Google Scholar] [CrossRef]
- Lubitz, S.A.; Faranesh, A.Z.; Atlas, S.J.; McManus, D.D.; Singer, D.E.; Pagoto, S.; Pantelopoulos, A.; Foulkes, A.S. Rationale and design of a large population study to validate software for the assessment of atrial fibrillation from data acquired by a consumer tracker or smartwatch: The Fitbit heart study. Am. Heart J. 2021, 238, 16–26. [Google Scholar] [CrossRef] [PubMed]
- Perez, M.V.; Mahaffey, K.W.; Hedlin, H.; Rumsfeld, J.S.; Garcia, A.; Ferris, T.; Balasubramanian, V.; Russo, A.M.; Rajmane, A.; Cheung, L.; et al. Large-scale assessment of a smartwatch to identify atrial fibrillation. N. Engl. J. Med. 2019, 381, 1909–1917. [Google Scholar] [CrossRef]
- Eysenck, W.; Freemantle, N.; Sulke, N. A randomized trial evaluating the accuracy of AF detection by four external ambulatory ECG monitors compared to permanent pacemaker AF detection. J. Interv. Card. Electrophysiol. 2020, 57, 361–369. [Google Scholar] [CrossRef]
- Hannun, A.Y.; Rajpurkar, P.; Haghpanahi, M.; Tison, G.H.; Bourn, C.; Turakhia, M.P.; Ng, A.Y. Cardiologist-level arrhythmia detection and classification in ambulatory electrocardiograms using a deep neural network. Nat. Med. 2019, 25, 65–69. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food & Drug Administration. Letter to Rich Laguna. Available online: https://www.accessdata.fda.gov/cdrh_docs/pdf18/K181502.pdf (accessed on 14 October 2022).
- Bayoumy, K.; Gaber, M.; Elshafeey, A.; Mhaimeed, O.; Dineen, E.H.; Marvel, F.A.; Martin, S.S.; Muse, E.D.; Turakhia, M.P.; Tarakji, K.G.; et al. Smart wearable devices in cardiovascular care: Where we are and how to move forward. Nat. Rev. Cardiol. 2021, 18, 581–599. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Heart Rate | Blood Pressure | ECG | |
|---|---|---|---|
| Apple Watch 8 | √ | √ | |
| Fitbit Sense 2 | √ | √ | |
| Google Pixel Watch | √ | √ | |
| Samsung Galaxy Watch 5 * | √ | √ | √ |
| Omeron+Alivcor Complete | √ | √ | √ |
| Omron Heart Guide | √ | √ | |
| Biobeat BB-613WP | √ | √ | √ (with patch) |
| iRhythm Zio Patch | √ | √ | |
| Zephyr BioHarness | √ | √ | |
| Preventice Solutions Body Guardian | √ | √ | |
| Corventist Nuvant MCT | √ | √ | |
| BradyDx CAM | √ | √ | |
| BioTel Heart | √ | √ | |
| Medibio Sense MBS | √ | √ | |
| Amazfit GTR 3 Pro * | √ | √ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, K.; Morales-Garza, M.; Cardoso, C.; Moctezuma-Ramirez, A.; Burman, A.; Titus, J.; Elgalad, A.; Perin, E. Early Changes in Acute Myocardial Infarction in Pigs: Achieving Early Detection with Wearable Devices. Diagnostics 2023, 13, 1006. https://doi.org/10.3390/diagnostics13061006
Li K, Morales-Garza M, Cardoso C, Moctezuma-Ramirez A, Burman A, Titus J, Elgalad A, Perin E. Early Changes in Acute Myocardial Infarction in Pigs: Achieving Early Detection with Wearable Devices. Diagnostics. 2023; 13(6):1006. https://doi.org/10.3390/diagnostics13061006
Chicago/Turabian StyleLi, Ke, Marco Morales-Garza, Cristiano Cardoso, Angel Moctezuma-Ramirez, Atandra Burman, Jitto Titus, Abdelmotagaly Elgalad, and Emerson Perin. 2023. "Early Changes in Acute Myocardial Infarction in Pigs: Achieving Early Detection with Wearable Devices" Diagnostics 13, no. 6: 1006. https://doi.org/10.3390/diagnostics13061006