
Enhancing the Reliability of Intraoperative Ultrasound in Pediatric Space-Occupying Brain Lesions
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dixon, L.; Lim, A.; Grech-Sollars, M.; Nandi, D.; Camp, S. Intraoperative Ultrasound in Brain Tumor Surgery: A Review and Implementation Guide. Neurosurg. Rev. 2022, 45, 2503–2515. [Google Scholar] [CrossRef]
- de Laurentis, C.; Bteich, F.; Beuriat, P.A.; Mottolese, C.; Giussani, C.; Szathmari, A.; Vinchon, M.; Di Rocco, F. Sodium Fluorescein in Pediatric Neurosurgery: A Systematic Review with Technical Considerations and Future Perspectives. Childs Nerv. Syst. 2022, 1–12. [Google Scholar] [CrossRef] [PubMed]
- de Laurentis, C.; Höhne, J.; Cavallo, C.; Restelli, F.; Falco, J.; Broggi, M.; Bosio, L.; Vetrano, I.G.; Schiariti, M.; Zattra, C.M.; et al. The Impact of Fluorescein-Guided Technique in the Surgical Removal of CNS Tumors in a Pediatric Population: Results from a Multicentric Observational Study. J. Neurosurg. Sci. 2019, 63, 679–687. [Google Scholar] [CrossRef] [PubMed]
- Falco, J.; Broggi, M.; Schiariti, M.; Vetrano, I.G.; Esposito, S.; Ferroli, P.; Acerbi, F. The Role of Sodium Fluorescein in Pediatric Supratentorial Intra-Axial Tumor Resection: New Insights from a Monocentric Series of 33 Consecutive Patients. Childs Nerv. Syst. 2022, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Stummer, W.; Tonn, J.-C.; Goetz, C.; Ullrich, W.; Stepp, H.; Bink, A.; Pietsch, T.; Pichlmeier, U. 5-Aminolevulinic Acid-Derived Tumor Fluorescence: The Diagnostic Accuracy of Visible Fluorescence Qualities as Corroborated by Spectrometry and Histology and Postoperative Imaging. Neurosurgery 2014, 74, 310–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, L.P.; Deepa, S.F.A.J.; Moinca, I.; Suresh, P.; Naidu, K.V.J.R. Medulloblastoma: A Common Pediatric Tumor: Prognostic Factors and Predictors of Outcome. Asian J. Neurosurg. 2015, 10, 50. [Google Scholar] [CrossRef] [Green Version]
- McCrea, H.J.; Bander, E.D.; Venn, R.A.; Reiner, A.S.; Iorgulescu, J.B.; Puchi, L.A.; Schaefer, P.M.; Cederquist, G.; Greenfield, J.P. Sex, Age, Anatomic Location, and Extent of Resection Influence Outcomes in Children with High-Grade Glioma. Neurosurgery 2015, 77, 443–453. [Google Scholar] [CrossRef]
- Roth, J.; Biyani, N.; Beni-Adani, L.; Constantini, S. Real-Time Neuronavigation with High-Quality 3D Ultrasound SonoWand in Pediatric Neurosurgery. Pediatr. Neurosurg. 2007, 43, 185–191. [Google Scholar] [CrossRef]
- Souweidane, M.M. The Evolving Role of Surgery in the Management of Pediatric Brain Tumors. J. Child Neurol. 2009, 24, 1366–1374. [Google Scholar] [CrossRef]
- Sun, M.Z.; Ivan, M.E.; Clark, A.J.; Oh, M.C.; Delance, A.R.; Oh, T.; Safaee, M.; Kaur, G.; Bloch, O.; Molinaro, A.; et al. Gross Total Resection Improves Overall Survival in Children with Choroid Plexus Carcinoma. J. Neurooncol. 2014, 116, 179–185. [Google Scholar] [CrossRef] [Green Version]
- Ullrich, N.J.; Pomeroy, S.L.; Kapur, K.; Manley, P.E.; Goumnerova, L.C.; Loddenkemper, T. Incidence, Risk Factors, and Longitudinal Outcome of Seizures in Long-Term Survivors of Pediatric Brain Tumors. Epilepsia 2015, 56, 1599–1604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avula, S.; Mallucci, C.L.; Pizer, B.; Garlick, D.; Crooks, D.; Abernethy, L.J. Intraoperative 3-Tesla MRI in the Management of Paediatric Cranial Tumours—Initial Experience. Pediatr. Radiol. 2012, 42, 158–167. [Google Scholar] [CrossRef] [PubMed]
- El Beltagy, M.A.; Aggag, M.; Kamal, M. Role of Intraoperative Ultrasound in Resection of Pediatric Brain Tumors. Childs Nerv. Syst. 2010, 26, 1189–1193. [Google Scholar] [CrossRef] [PubMed]
- Lam, C.H.; Hall, W.A.; Truwit, C.L.; Liu, H. Intra-Operative MRI-Guided Approaches to the Pediatric Posterior Fossa Tumors. Pediatr. Neurosurg. 2001, 34, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Moriarty, T.M.; Titsworth, W.L. The Evolution of IMRI Utilization for Pediatric Neurosurgery: A Single Center Experience. Acta Neurochir. Suppl. 2011, 109, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Mutchnick, I.; Moriarty, T.M. Intraoperative MRI in Pediatric Neurosurgery—An Update. Transl. Pediatr. 2014, 3, 236–246. [Google Scholar] [CrossRef]
- Chacko, A.G.; Kumar, N.K.S.; Chacko, G.; Athyal, R.; Rajshekhar, V. Intraoperative Ultrasound in Determining the Extent of Resection of Parenchymal Brain Tumours—A Comparative Study with Computed Tomography and Histopathology. Acta Neurochir. 2003, 145, 743–748, discussion 748. [Google Scholar] [CrossRef]
- Unsgaard, G.; Ommedal, S.; Muller, T.; Gronningsaeter, A.; Nagelhus Hernes, T.A. Neuronavigation by Intraoperative Three-Dimensional Ultrasound: Initial Experience during Brain Tumor Resection. Neurosurgery 2002, 50, 804–812, discussion 812. [Google Scholar] [CrossRef] [Green Version]
- Ulrich, N.H.; Burkhardt, J.-K.; Serra, C.; Bernays, R.-L.; Bozinov, O. Resection of Pediatric Intracerebral Tumors with the Aid of Intraoperative Real-Time 3-D Ultrasound. Childs Nerv. Syst. 2012, 28, 101–109. [Google Scholar] [CrossRef] [Green Version]
- Moiyadi, A.; Shetty, P. Objective Assessment of Utility of Intraoperative Ultrasound in Resection of Central Nervous System Tumors: A Cost-Effective Tool for Intraoperative Navigation in Neurosurgery. J. Neurosci. Rural Pract. 2011, 2, 4–11. [Google Scholar] [CrossRef]
- Choudhri, A.F.; Klimo, P.; Auschwitz, T.S.; Whitehead, M.T.; Boop, F.A. 3T Intraoperative MRI for Management of Pediatric CNS Neoplasms. Am. J. Neuroradiol. 2014, 35, 2382–2387. [Google Scholar] [CrossRef] [Green Version]
- Roth, J.; Beni-Adani, L.; Biyani, N.; Constantini, S. Classical and Real-Time Neuronavigation in Pediatric Neurosurgery. Childs Nerv. Syst. 2006, 22, 1065–1071. [Google Scholar] [CrossRef]
- Giussani, C.; Trezza, A.; Ricciuti, V.; Di Cristofori, A.; Held, A.; Isella, V.; Massimino, M. Intraoperative MRI versus Intraoperative Ultrasound in Pediatric Brain Tumor Surgery: Is Expensive Better than Cheap? A Review of the Literature. Childs Nerv. Syst. 2022, 38, 1445–1454. [Google Scholar] [CrossRef]
- Mosteiro, A.; Di Somma, A.; Ramos, P.R.; Ferrés, A.; De Rosa, A.; González-Ortiz, S.; Enseñat, J.; González, J.J. Is Intraoperative Ultrasound More Efficient than Magnetic Resonance in Neurosurgical Oncology? An Exploratory Cost-Effectiveness Analysis. Front. Oncol. 2022, 12, 1016264. [Google Scholar] [CrossRef]
- Barzaghi, L.R.; Capitanio, J.F.; Giudice, L.; Panni, P.; Acerno, S.; Mortini, P. Usefulness of Ultrasound-Guided Microsurgery in Cavernous Angioma Removal. World Neurosurg. 2018, 116, e414–e420. [Google Scholar] [CrossRef]
- Prada, F.; Del Bene, M.; Moiraghi, A.; Casali, C.; Legnani, F.G.; Saladino, A.; Perin, A.; Vetrano, I.G.; Mattei, L.; Richetta, C.; et al. From Grey Scale B-Mode to Elastosonography: Multimodal Ultrasound Imaging in Meningioma Surgery-Pictorial Essay and Literature Review. Biomed Res. Int. 2015, 2015, 925729. [Google Scholar] [CrossRef]
- Prada, F.; Perin, A.; Martegani, A.; Aiani, L.; Solbiati, L.; Lamperti, M.; Casali, C.; Legnani, F.; Mattei, L.; Saladino, A.; et al. Intraoperative Contrast-Enhanced Ultrasound for Brain Tumor Surgery. Neurosurgery 2014, 74, 542–552, discussion 552. [Google Scholar] [CrossRef] [Green Version]
- Sweeney, J.F.; Smith, H.; Taplin, A.; Perloff, E.; Adamo, M.A. Efficacy of Intraoperative Ultrasonography in Neurosurgical Tumor Resection. J. Neurosurg. Pediatr. 2018, 21, 504–510. [Google Scholar] [CrossRef] [PubMed]
- Carai, A.; De Benedictis, A.; Calloni, T.; Onorini, N.; Paternò, G.; Randi, F.; Colafati, G.S.; Mastronuzzi, A.; Marras, C.E. Intraoperative Ultrasound-Assisted Extent of Resection Assessment in Pediatric Neurosurgical Oncology. Front. Oncol. 2021, 11, 660805. [Google Scholar] [CrossRef] [PubMed]
- El Beltagy, M.A.; Atteya, M.M.E. The Benefits of Navigated Intraoperative Ultrasonography during Resection of Fourth Ventricular Tumors in Children. Childs Nerv. Syst. 2013, 29, 1079–1088. [Google Scholar] [CrossRef] [PubMed]
- Gosal, J.S.; Tiwari, S.; Sharma, T.; Agrawal, M.; Garg, M.; Mahal, S.; Bhaskar, S.; Sharma, R.K.; Janu, V.; Jha, D.K. Simulation of Surgery for Supratentorial Gliomas in Virtual Reality Using a 3D Volume Rendering Technique: A Poor Man’s Neuronavigation. Neurosurg. Focus 2021, 51, E23. [Google Scholar] [CrossRef] [PubMed]
- Gaudino, S.; Marziali, G.; Pezzullo, G.; Guadalupi, P.; Giordano, C.; Infante, A.; Benenati, M.; Ramaglia, A.; Massimi, L.; Gessi, M.; et al. Role of Susceptibility-Weighted Imaging and Intratumoral Susceptibility Signals in Grading and Differentiating Pediatric Brain Tumors at 1.5 T: A Preliminary Study. Neuroradiology 2020, 62, 705–713. [Google Scholar] [CrossRef] [PubMed]
- Gaudino, S.; Martucci, M.; Botto, A.; Ruberto, E.; Leone, E.; Infante, A.; Ramaglia, A.; Caldarelli, M.; Frassanito, P.; Triulzi, F.M.; et al. Brain DSC MR Perfusion in Children: A Clinical Feasibility Study Using Different Technical Standards of Contrast Administration. Am. J. Neuroradiol. 2019, 40, 359–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosado, E.; Riccabona, M. Off-Label Use of Ultrasound Contrast Agents for Intravenous Applications in Children: Analysis of the Existing Literature. J. Ultrasound. Med. 2016, 35, 487–496. [Google Scholar] [CrossRef] [PubMed]
- Sidhu, P.S.; Cantisani, V.; Deganello, A.; Dietrich, C.F.; Duran, C.; Franke, D.; Harkanyi, Z.; Kosiak, W.; Miele, V.; Ntoulia, A.; et al. Role of Contrast-Enhanced Ultrasound (CEUS) in Paediatric Practice: An EFSUMB Position Statement. J. Ultrasound 2017, 38, 33–43. [Google Scholar] [CrossRef] [Green Version]
- Saß, B.; Zivkovic, D.; Pojskic, M.; Nimsky, C.; Bopp, M.H.A. Navigated Intraoperative 3D Ultrasound in Glioblastoma Surgery: Analysis of Imaging Features and Impact on Extent of Resection. Front. Neurosci. 2022, 16, 883584. [Google Scholar] [CrossRef]
- Keleş, A.; Türe, U. Cottonoid-Guided Intraoperative Ultrasonography in Neurosurgery: A Proof-of-Concept Single Surgeon Case Series. Neurosurg. Rev. 2022, 45, 2289–2303. [Google Scholar] [CrossRef]
- Selbekk, T.; Jakola, A.S.; Solheim, O.; Johansen, T.F.; Lindseth, F.; Reinertsen, I.; Unsgård, G. Ultrasound Imaging in Neurosurgery: Approaches to Minimize Surgically Induced Image Artefacts for Improved Resection Control. Acta Neurochir. 2013, 155, 973–980. [Google Scholar] [CrossRef] [Green Version]
- Šteňo, A.; Karlík, M.; Mendel, P.; Čík, M.; Šteňo, J. Navigated Three-Dimensional Intraoperative Ultrasound-Guided Awake Resection of Low-Grade Glioma Partially Infiltrating Optic Radiation. Acta Neurochir. 2012, 154, 1255–1262. [Google Scholar] [CrossRef]
- Unsgård, G.; Sagberg, L.M.; Müller, S.; Selbekk, T. A New Acoustic Coupling Fluid with Ability to Reduce Ultrasound Imaging Artefacts in Brain Tumour Surgery—A Phase I Study. Acta Neurochir. 2019, 161, 1475–1486. [Google Scholar] [CrossRef] [Green Version]
- Piscaglia, F.; Nolsøe, C.; Dietrich, C.F.; Cosgrove, D.O.; Gilja, O.H.; Bachmann Nielsen, M.; Albrecht, T.; Barozzi, L.; Bertolotto, M.; Catalano, O.; et al. The EFSUMB Guidelines and Recommendations on the Clinical Practice of Contrast Enhanced Ultrasound (CEUS): Update 2011 on Non-Hepatic Applications. Ultraschall Med. 2012, 33, 33–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prada, F.; Bene, M.D.; Fornaro, R.; Vetrano, I.G.; Martegani, A.; Aiani, L.; Sconfienza, L.M.; Mauri, G.; Solbiati, L.; Pollo, B.; et al. Identification of Residual Tumor with Intraoperative Contrast-Enhanced Ultrasound during Glioblastoma Resection. Neurosurg. Focus 2016, 40, E7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erdoğan, N.; Tucer, B.; Mavili, E.; Menkü, A.; Kurtsoy, A. Ultrasound Guidance in Intracranial Tumor Resection: Correlation with Postoperative Magnetic Resonance Findings. Acta Radiol. 2005, 46, 743–749. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of cases | 45 |
| M:F | 23:22 |
| Age | 3m–18 years (median 6.4 years) |
| Pathology | 16 LG gliomas 12 HG gliomas 8 gangliogliomas 7 DNTs 5 cavernomas 5 other (2 FCDs, 1 meningioma, 1 SEGA, 1 histiocytosis) |
| Size | 24 (<2 cm) 21 (>2 cm) |
| Site | 15 temporal > 8 frontal > 6 parietal > 5 intraventricular > 4 occipital–4 diencephalic > 2 thalamic > 1 insular |
| Pre-IOUS | Problems | Solutions |
|---|---|---|
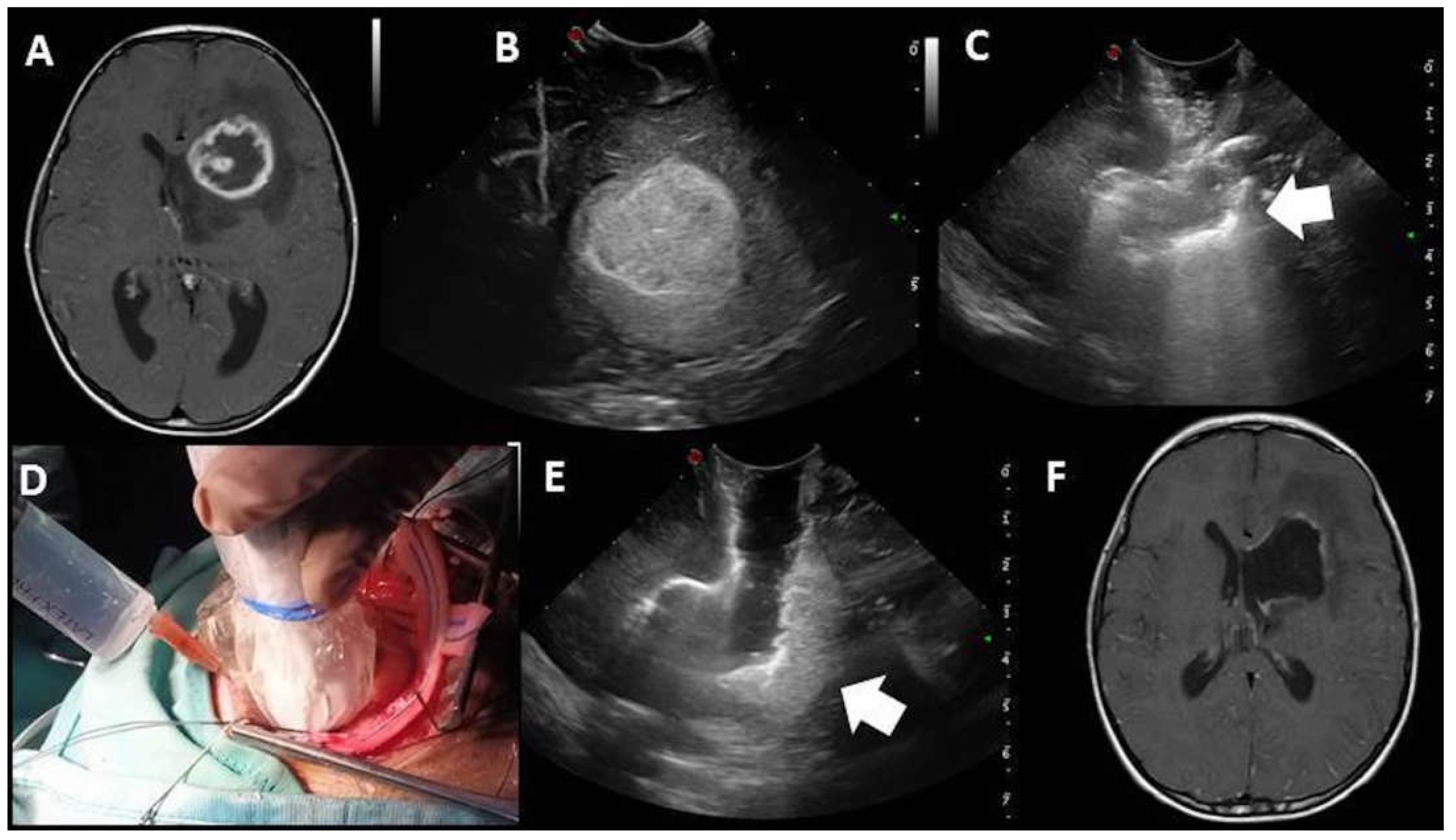
| Localization | Deep-seated lesion |
|
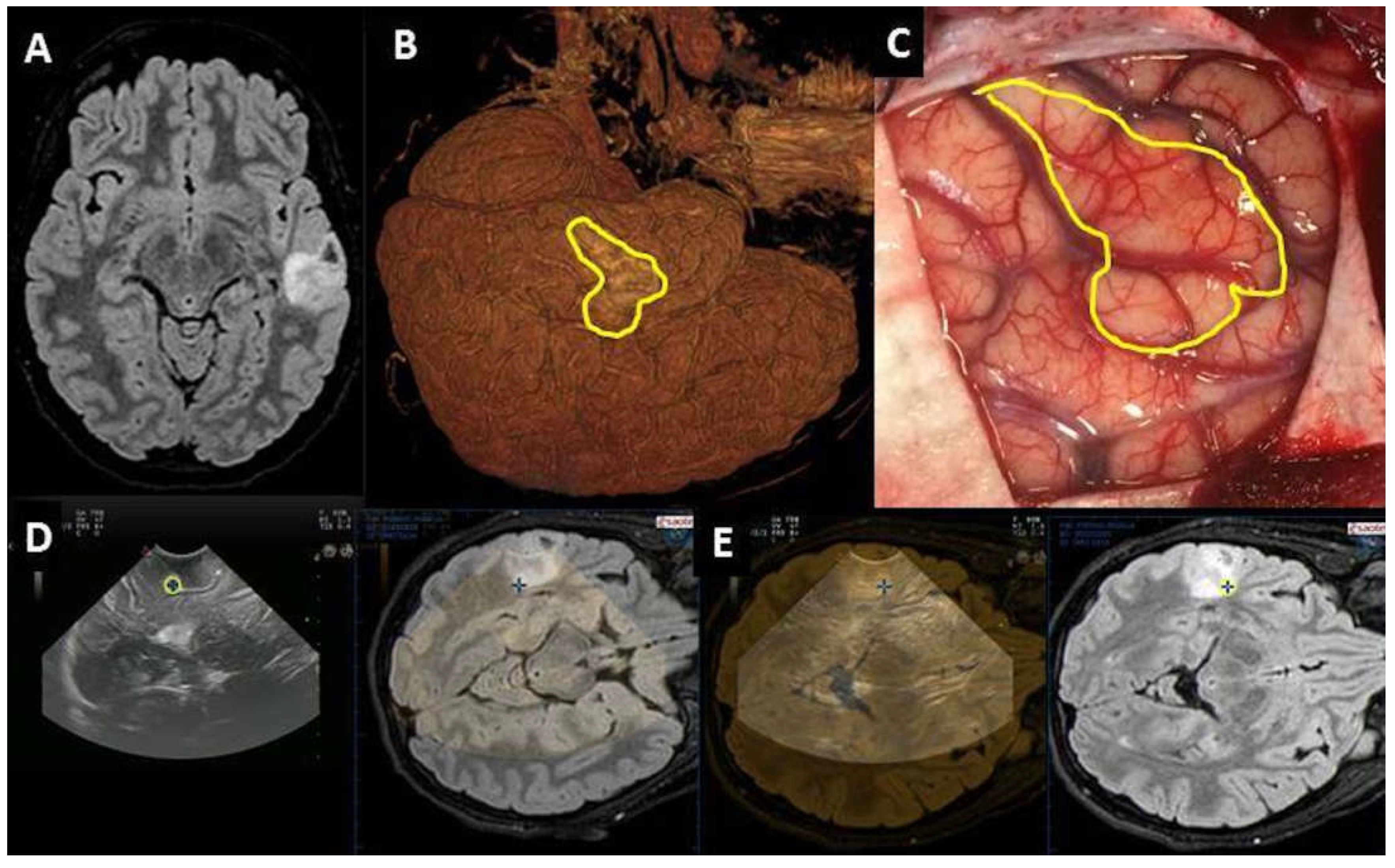
| Localization | Superficial lesion not distinguishable from brain parenchyma |
|
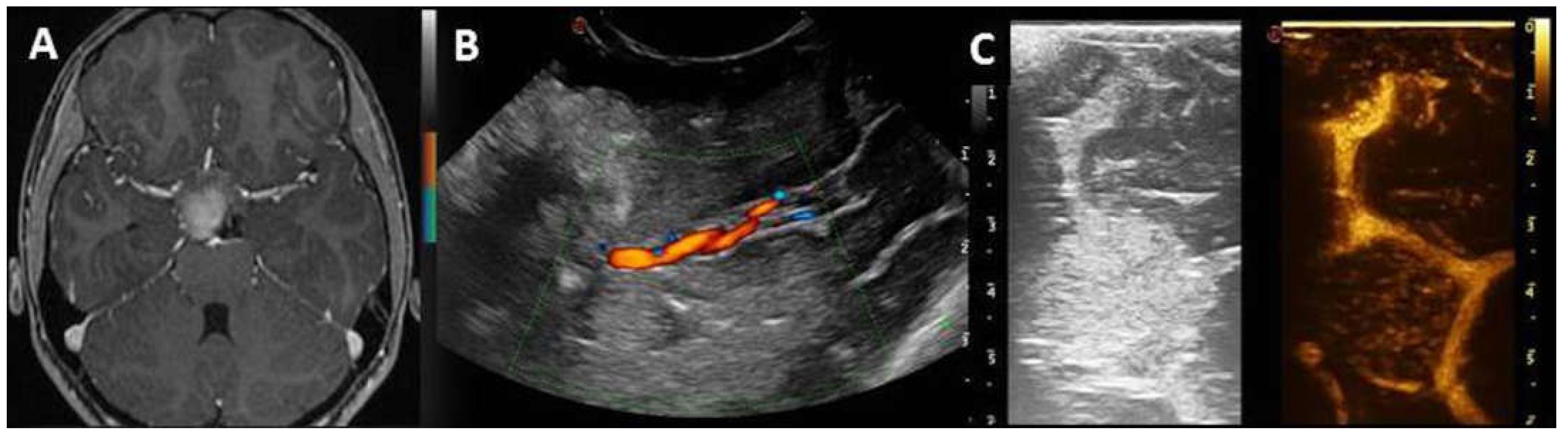
| Definition | Vascular relationship |
|
| Definition | Vascular pattern |
|
| Surgical route | Deep-seated lesion |
|
| Post-IOUS | ||
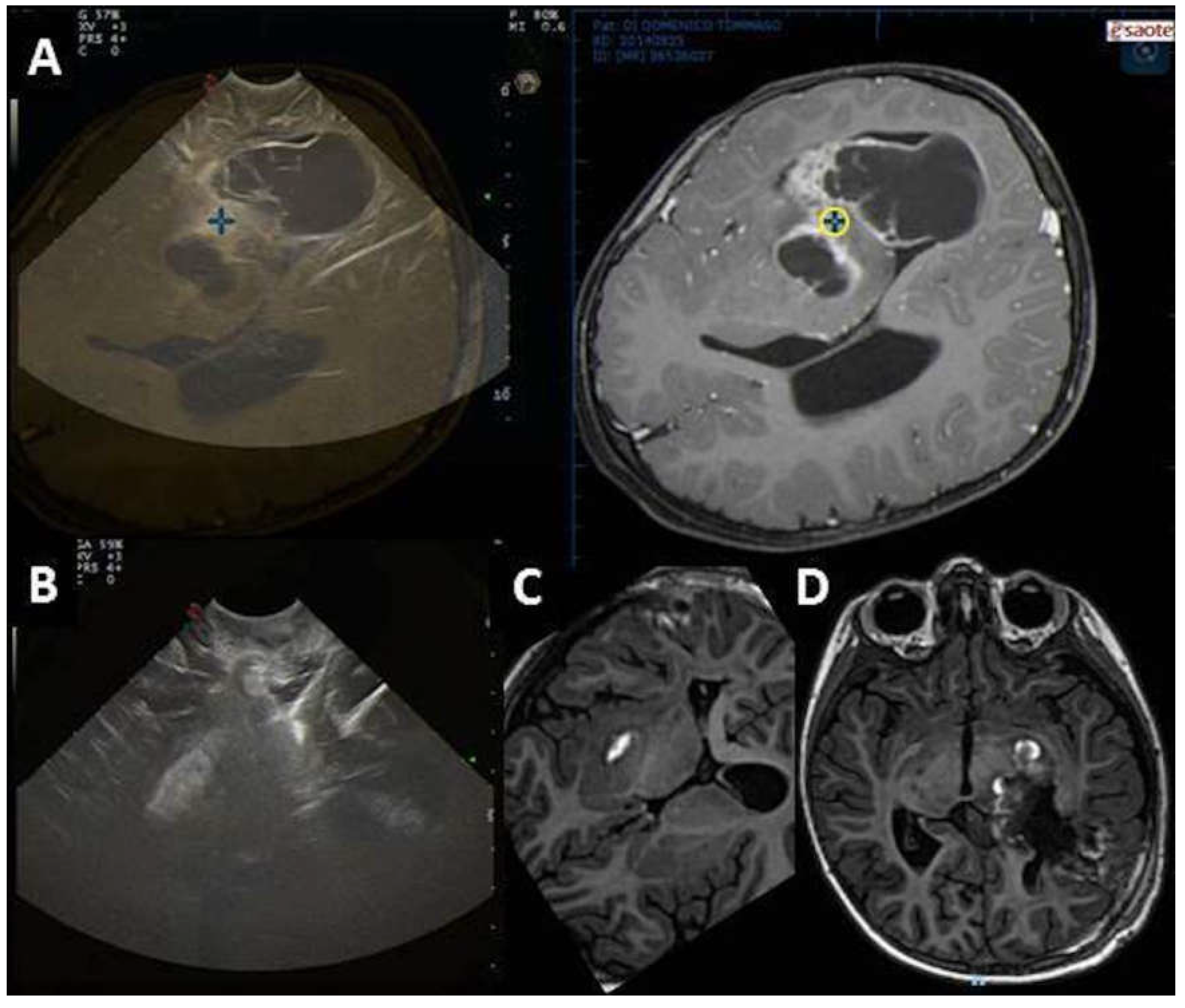
| EOR | Collapsed surgical cavity |
|
| EOR | Open ventricle |
|
| EOR | Artifacts |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frassanito, P.; Stifano, V.; Bianchi, F.; Tamburrini, G.; Massimi, L. Enhancing the Reliability of Intraoperative Ultrasound in Pediatric Space-Occupying Brain Lesions. Diagnostics 2023, 13, 971. https://doi.org/10.3390/diagnostics13050971
Frassanito P, Stifano V, Bianchi F, Tamburrini G, Massimi L. Enhancing the Reliability of Intraoperative Ultrasound in Pediatric Space-Occupying Brain Lesions. Diagnostics. 2023; 13(5):971. https://doi.org/10.3390/diagnostics13050971
Chicago/Turabian StyleFrassanito, Paolo, Vito Stifano, Federico Bianchi, Gianpiero Tamburrini, and Luca Massimi. 2023. "Enhancing the Reliability of Intraoperative Ultrasound in Pediatric Space-Occupying Brain Lesions" Diagnostics 13, no. 5: 971. https://doi.org/10.3390/diagnostics13050971