
Do NAAT-Based Methods Increase the Diagnostic Sensitivity of Streptococcus agalactiae Carriage Detection in Pregnant Women?
 , , and
, , and
Abstract
:1. Introduction
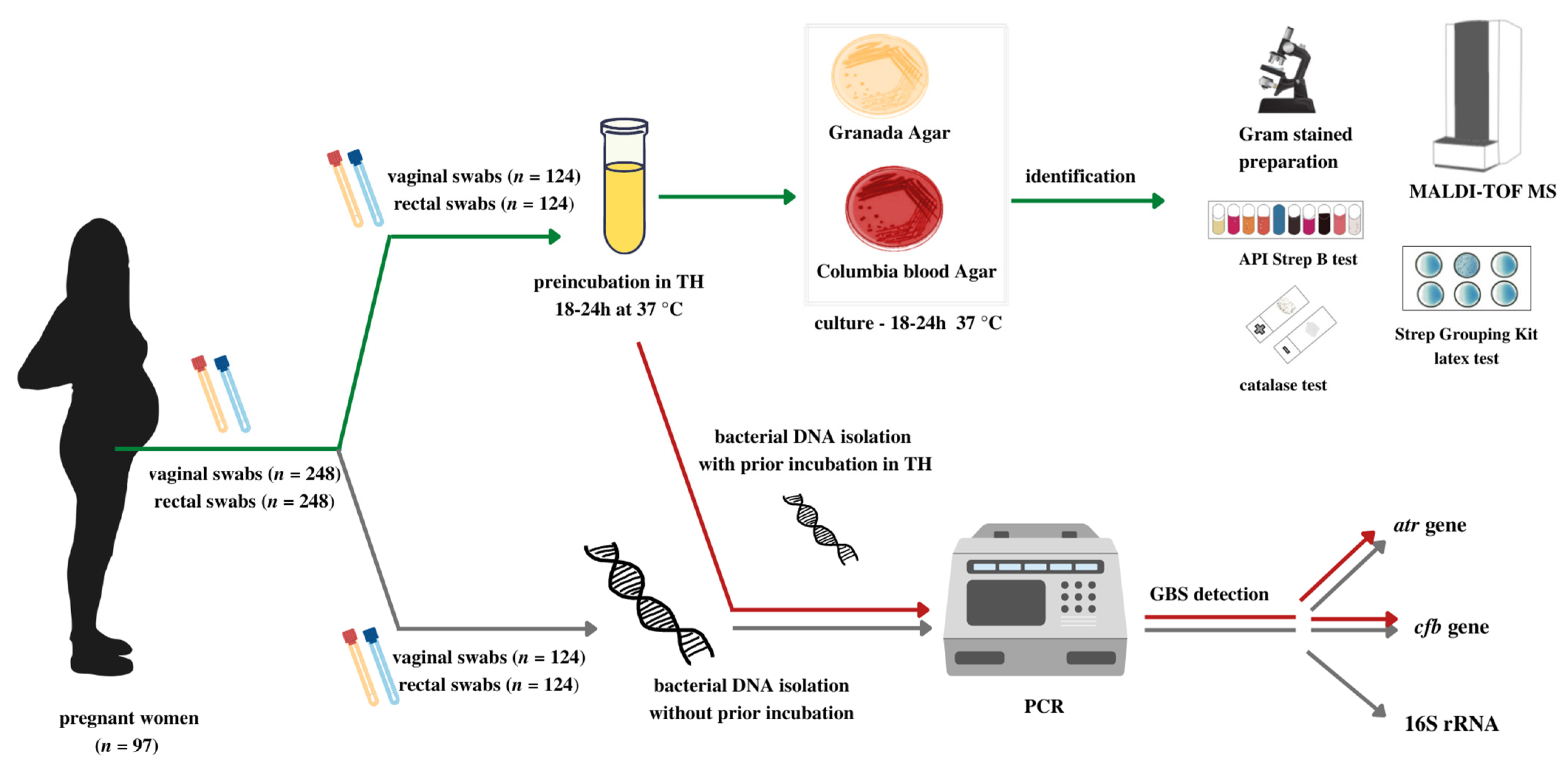
2. Materials and Methods
2.1. Patients
2.2. Samples
2.3. The Culture and Other Identification Tests
2.4. Isolation of Bacterial DNA
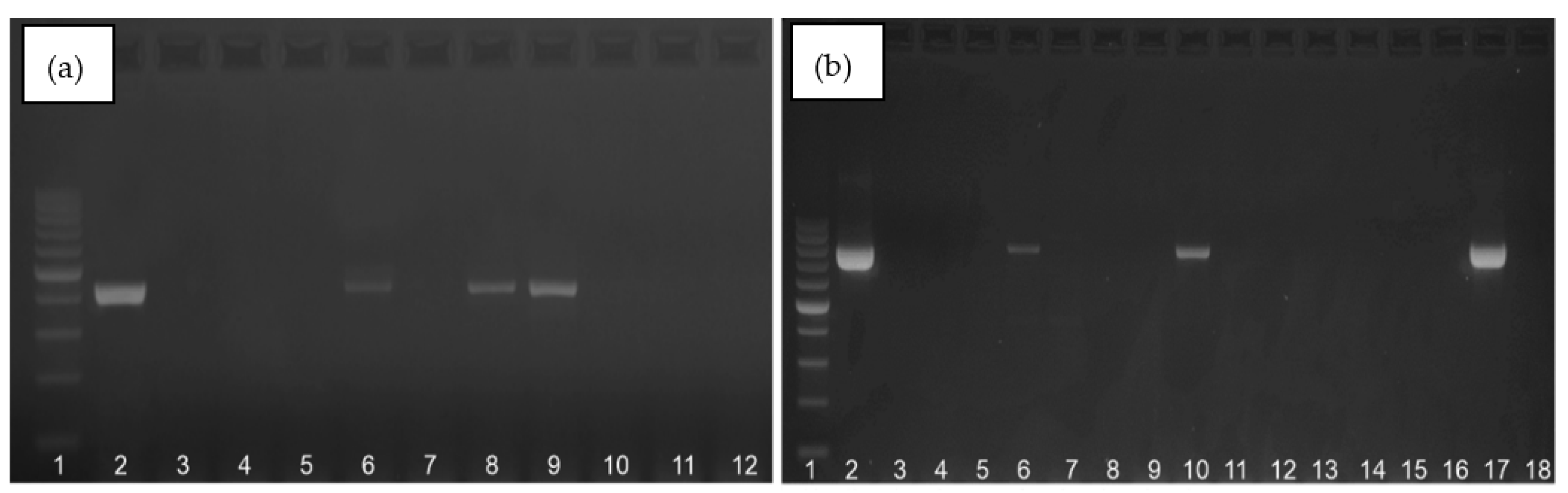
2.5. PCR Protocols
3. Results
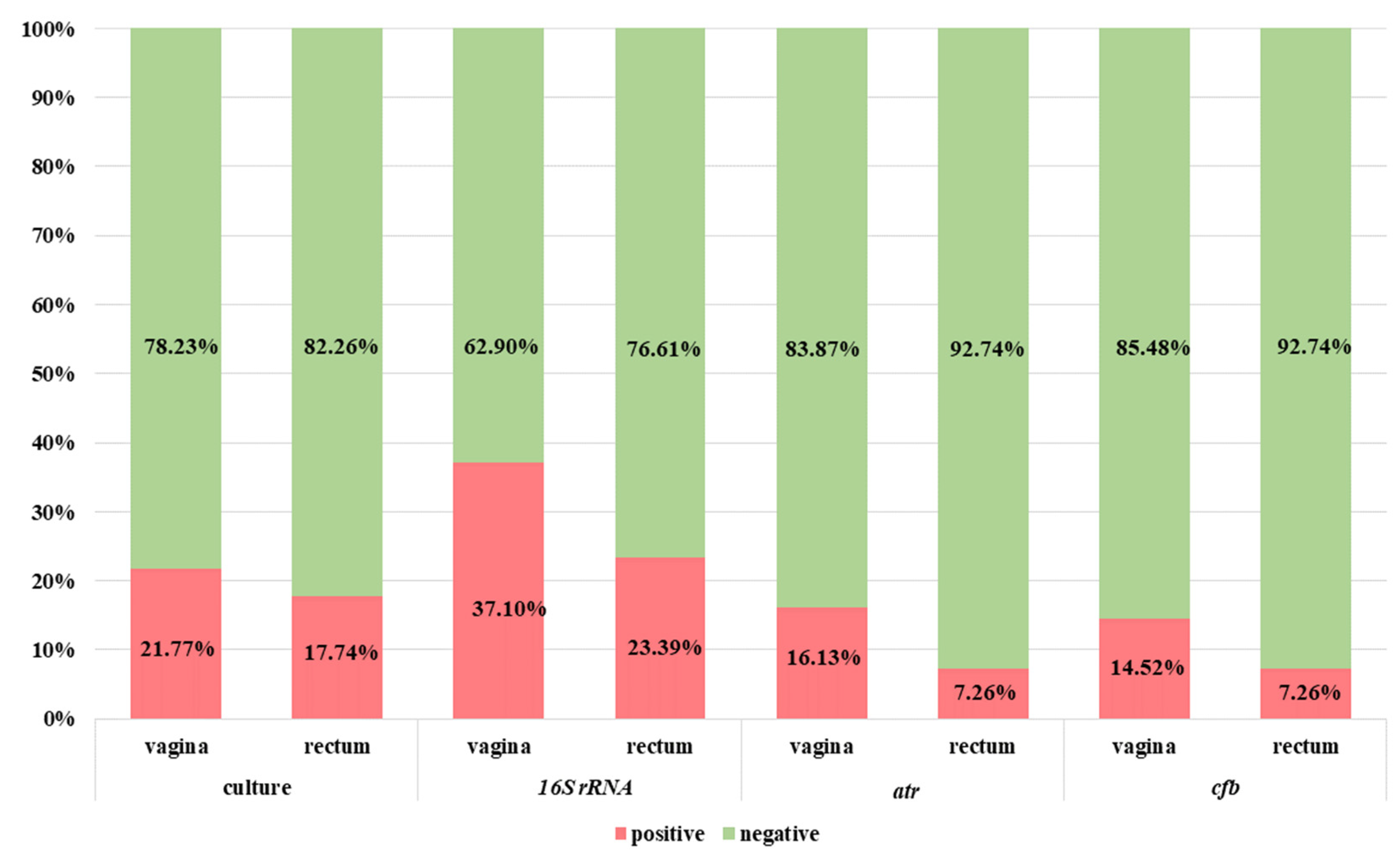
3.1. Diagnostics of Patients with the Use of Classic Microbiological Methods
3.2. Diagnostics of Patients with the Use of Standard NAAT-Based Methods
3.3. Statistical Analysis
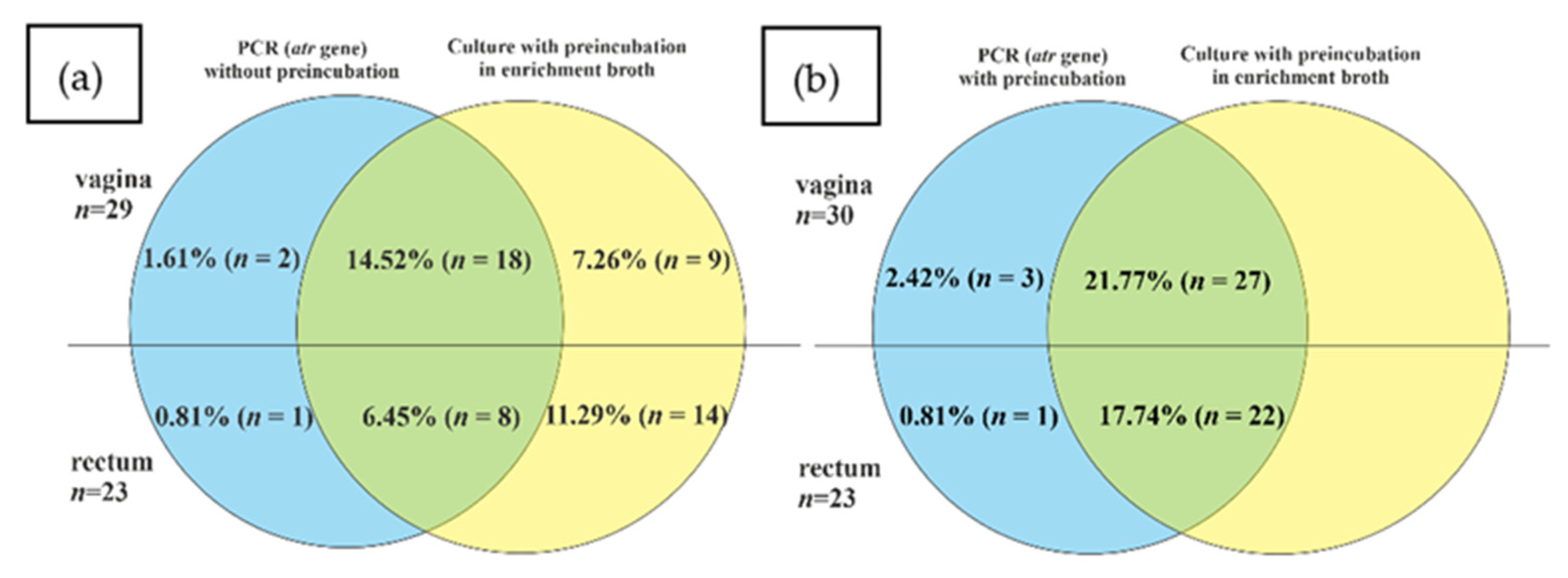
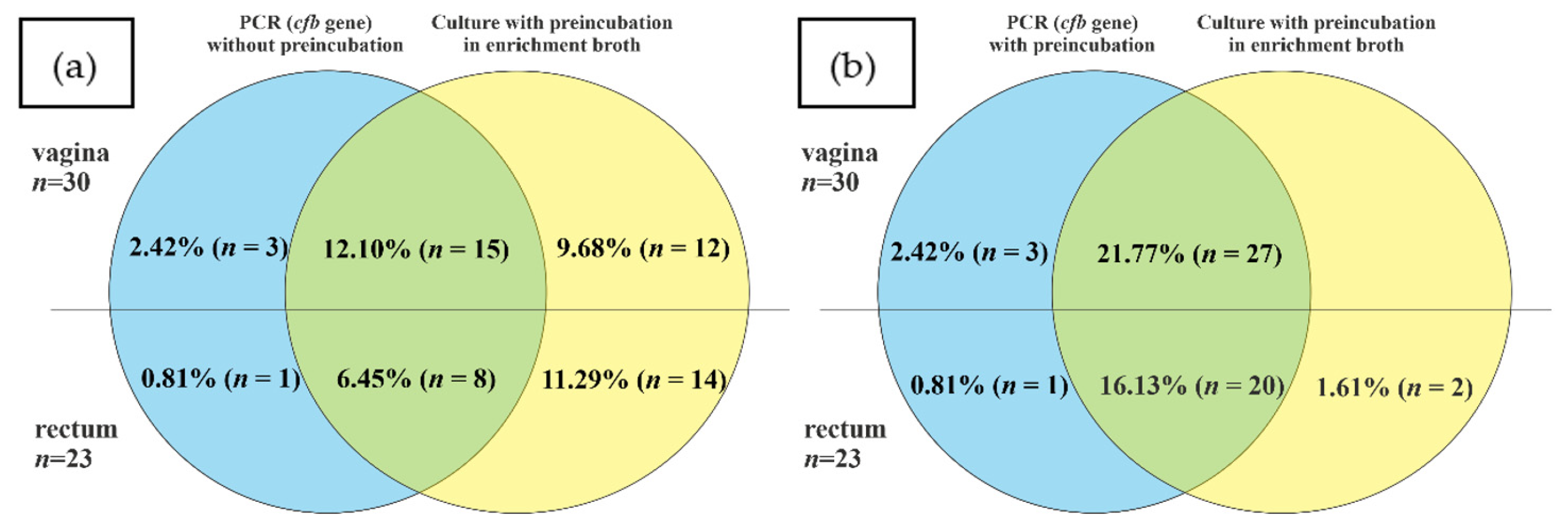
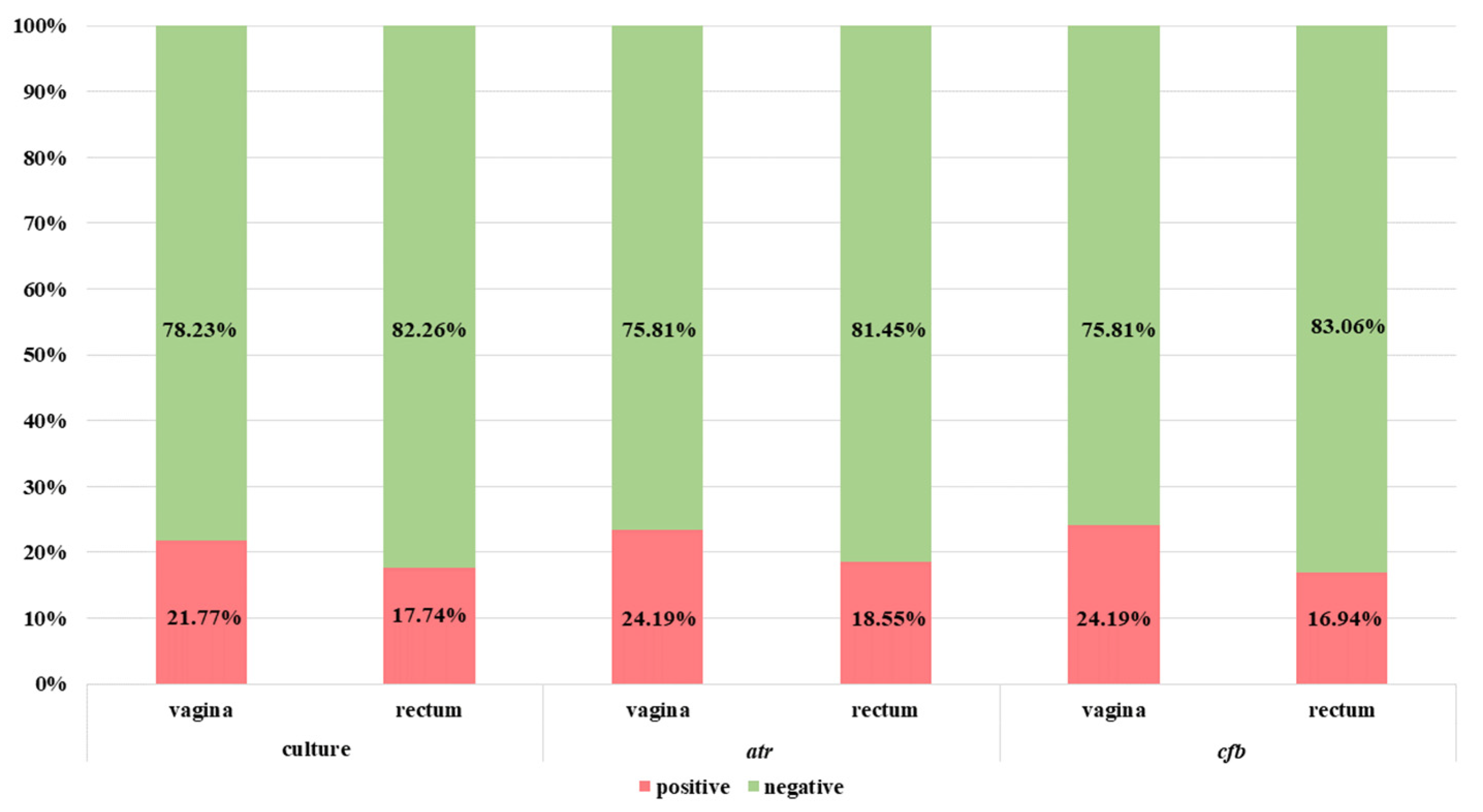
3.4. Comparison of NAAT and Culture Methods in Relation to GBS Carriers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Society for Microbiology—Guidelines for the Detection and Identification of Group B Streptococcus. Available online: https://asm.org/Guideline/Guidelines-for-the-Detection-and-Identification-of (accessed on 19 December 2022).
- Brzychczy-Włoch, M.; Pabian, W.; Majewska, E.; Żuk, M.; Kiełbik, J.; Gosiewski, T.; Bulanda, M. Dynamics of colonization with group B streptococci in relation to normal flora in women during subsequent trimesters of pregnancy. New Microbiol. 2014, 37, 307–319. [Google Scholar]
- Sroka-Oleksiak, A.; Gosiewski, T.; Pabian, W.; Gurgul, A.; Kapusta, P.; Ludwig-Słomczyńska, A.H.; Wołkow, P.P.; Brzychczy-Włoch, M. Next-Generation Sequencing as a Tool to Detect Vaginal Microbiota Disturbances during Pregnancy. Microorganisms 2020, 8, 1813. [Google Scholar] [CrossRef] [PubMed]
- Brzychczy-Wloch, M.; Wojkowska-Mach, J.; Helwich, E.; Heczko, P.B. Incidence of maternal GBS colonization and neonatal GBS disease among Very Low Birth Weight Polish neonates. Med. Sci. Monit. 2013, 19, 34–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brzychczy-Wloch, M.; Gosiewski, T.; Bulanda, M. Multilocus Sequence Types of Invasive and Colonizing Neonatal Group B Streptococci in Poland. Med. Princ. Pract. 2014, 23, 323–330. [Google Scholar] [CrossRef]
- Centers for Diseases Control and Prevention—Streptococcus Laboratory. Available online: https://www.cdc.gov/streplab/groupb-strep/index.html (accessed on 19 August 2022).
- Tickler, I.A.; Tenover, F.C.; Dewell, S.; Le, V.M.; Blackman, R.N.; Goering, R.V.; Rogers, A.E.; Piwonka, H.; Jung-Hynes, B.D.; Chen, D.J.; et al. Streptococcus agalactiae Strains with Chromosomal Deletions Evade Detection with Molecular Methods. J. Clin. Microbiol. 2019, 57, e02040-18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosa-Fraile, M.; Spellerberg, B. Reliable Detection of Group B Streptococcus in the Clinical Laboratory. J. Clin. Microbiol. 2017, 55, 2590–2598. [Google Scholar] [CrossRef] [Green Version]
- Gerolymatos, G.; Karlovasiti, P.; Sianou, A.; Logothetis, E.; Kaparos, G.; Grigoriadis, C.; Baka, S. Antenatal group B streptococcus detection in pregnant women: Culture or PCR? J. Infect. Dev. Ctries. 2018, 31, 631–635. [Google Scholar] [CrossRef]
- Bogiel, T.; Depka, D.; Zalas-Więcek, P.; Rzepka, M.; Kruszyńska, E.; Gospodarek-Komkowska, E. Application of the appropriate molecular biology-based method significantly increases the sensitivity of group B streptococcus detection results. J. Hosp. Infect. 2021, 112, 21–26. [Google Scholar] [CrossRef]
- Kimura, K.; Yanagisawa, H.; Wachino, J.-I.; Shibayama, K.; Arakawa, Y. Rapid and Reliable Loop-Mediated Isothermal Amplification Method for Detecting Streptococcus agalactiae. Jpn. J. Infect. Dis. 2013, 66, 546–548. [Google Scholar] [CrossRef] [Green Version]
- Hu, S.; Zhong, H.; Huang, W.; Zhan, W.; Yang, X.; Tang, B.; Chen, K.; Wang, J.; Hu, T.; Zhang, C.; et al. Rapid and visual detection of Group B streptococcus using recombinase polymerase amplification combined with lateral flow strips. Diagn. Microbiol. Infect. Dis. 2019, 93, 9–13. [Google Scholar] [CrossRef]
- Clarke, C.; O’Connor, L.; Carré-Skinner, H.; Piepenburg, O.; Smith, T.J. Development and performance evaluation of a recombinase polymerase amplification assay for the rapid detection of group B streptococcus. BMC Microbiol. 2016, 16, 221. [Google Scholar] [CrossRef] [Green Version]
- Bidgani, S.; Navidifar, T.; Najafian, M.; Amin, M. Comparison of group B streptococci colonization in vaginal and rectal specimens by culture method and polymerase chain reaction technique. J. Chin. Med. Assoc. 2016, 79, 141–145. [Google Scholar] [CrossRef] [PubMed]
- Bakhtiari, R.; Dallal, M.S.; Mehrabadi, J.; Heidarzadeh, S. Pourmand Evaluation of Culture and PCR Methods for Diagnosis of Group B Streptococcus Carriage in Iranian Pregnant Women. Iran. J. Public Health 2012, 41, 65–70. [Google Scholar] [PubMed]
- Martinez, G.; Harel, J.; Gottschalk, M. Specific detection by PCR of Streptococcus agalactiae in milk. Can. J. Vet. Res. 2001, 65, 68–72. [Google Scholar] [PubMed]
- Munari, F.M.; De-Paris, F.; Salton, G.D.; Lora, P.S.; Giovanella, P.; Machado, A.B.M.P.; Laybauer, L.S.; Oliveira, K.R.P.; Ferri, C.; Silveira, J.L.S.; et al. A Combined Enrichment/Polymerase Chain Reaction Based Method for the Routine Screening of Streptococcus agalactiae in Pregnant Women. Braz. J. Microbiol. 2012, 43, 253–260. [Google Scholar] [CrossRef]
- Diaz, M.H.; Waller, J.L.; Napoliello, R.A.; Islam, S.; Wolff, B.J.; Burken, D.J.; Holden, R.L.; Srinivasan, V.; Arvay, M.; McGee, L.; et al. Optimization of Multiple Pathogen Detection Using the TaqMan Array Card: Application for a Population-Based Study of Neonatal Infection. PLoS ONE 2013, 8, e66183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carrillo-Ávila, J.A.; Gutiérrez-Fernández, J.; González-Espín, A.I.; García-Triviño, E.; Giménez-Lirola, L.G. Comparison of qPCR and culture methods for group B Streptococcus colonization detection in pregnant women: Evaluation of a new qPCR assay. BMC Infect. Dis. 2018, 18, 305. [Google Scholar] [CrossRef] [Green Version]
- Mousavi, S.M.; Hosseini, S.M.; Yousefimashouf, R.; Arabestani, M. Identification of Group B Streptococci Using 16S rRNA, cfb, scpB, and atr Genes in Pregnant Women by PCR. Acta Med. Iran. 2016, 54, 765–770. [Google Scholar]
- Vieira, L.L.; Perez, A.V.; Machado, M.M.; Kayser, M.L.; Vettori, D.V.; Alegretti, A.P.; Ferreira, C.F.; Vettorazzi, J.; Valério, E.G. Group B Streptococcus detection in pregnant women: Comparison of qPCR assay, culture, and the Xpert GBS rapid test. BMC Pregnancy Childbirth 2019, 19, 532. [Google Scholar] [CrossRef] [Green Version]
- Park, J.S.; Cho, D.-H.; Yang, J.H.; Kim, M.Y.; Shin, S.M.; Kim, E.-C.; Park, S.S.; Seong, M.-W. Usefulness of a Rapid Real-time PCR Assay in Prenatal Screening for Group B Streptococcus Colonization. Ann. Lab. Med. 2013, 33, 39–44. [Google Scholar] [CrossRef] [Green Version]
- Helmig, R.B.; Gertsen, J.B. Diagnostic accuracy of polymerase chain reaction for intrapartum detection of group B streptococcus colonization. Acta Obstet. Gynecol. Scand. 2017, 96, 1070–1074. [Google Scholar] [CrossRef] [PubMed]
- Rabaan, A.A.; Saunar, J.V.; Bazzi, A.M.; Soriano, J.L. Modified use of real-time PCR detection of group B Streptococcus in pregnancy. J. Med. Microbiol. 2017, 66, 1516–1520. [Google Scholar] [CrossRef] [PubMed]
- De-Paris, F.; Mombach, A.B.; Machado, P.; Gheno, T.C.; Ascoli, A.M.; de Oliveira, K.R.P.; Barth, A.L. Group B Streptococcus detection: Comparison of PCR assay and culture as a screening method for pregnant women. Braz. J. Infect. Dis. 2011, 15, 323–327. [Google Scholar] [CrossRef] [Green Version]
- Marconi, C.; Rocchetti, T.T.; Rall, V.L.M.; De Carvalho, L.R.; Borges, V.T.M.; Da Silva, M.G. Detection of Streptococcus agalactiae colonization in pregnant women by using combined swab cultures: Cross-sectional prevalence study. Sao Paulo Med. J. 2010, 128, 60–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferreira, M.B.; De-Paris, F.; Paiva, R.M.; Nunes, L.D.S. Assessment of conventional PCR and real-time PCR compared to the gold standard method for screening Streptococcus agalactiae in pregnant women. Braz. J. Infect. Dis. 2018, 22, 449–454. [Google Scholar] [CrossRef]
- Wollheim, C.; Sperhacke, R.D.; Fontana, S.K.R.; Vanni, A.C.; Kato, S.K.; De Araújo, P.R.; Barth, A.L.; Madi, J.M. Group B Streptococcus detection in pregnant women via culture and PCR methods. Rev. Soc. Bras. Med. Trop. 2017, 50, 179–183. [Google Scholar] [CrossRef] [Green Version]
- Yeung, S.-W.; Cheung, P.-T.; Chau, S.-L.; Ip, M.; Lao, T.T.-H.; Leung, T.-Y.; Tam, W.-H. Evaluation of an in-house real-time polymerase chain reaction method to identify group B streptococcus colonization in pregnancy. J. Obstet. Gynaecol. Res. 2015, 41, 1357–1362. [Google Scholar] [CrossRef]
- Martín, V.; Mediano, P.; Del Campo, R.; Rodríguez, J.; Marín, M. Streptococcal Diversity of Human Milk and Comparison of Different Methods for the Taxonomic Identification of Streptococci. J. Hum. Lact. 2016, 32, NP84–NP94. [Google Scholar] [CrossRef]
- Dunne, W.M.; Holland-Staley, C.A. Comparison of NNA Agar Culture and Selective Broth Culture for Detection of Group B Streptococcal Colonization in Women. J. Clin. Microbiol. 1998, 36, 2298–2300. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Primer Pairs | Sequence 5′ → 3′ | Source |
|---|---|---|
| 16S rRNA | F: GAGTTTGATCATGGCTCAG | [16] |
| R: ACCAACATGTGTTAATTACTC | ||
| atr | F: CGATTCTCTCAGCTTTGTTA | [17] |
| R: AAGAAATCTCTTGTGCGGAT | ||
| cfb | F: GGGAACAGATTATGAAAAACCG | [18] |
| R: AAGGCTTCTACACGACTACCAA | ||
| P: FAM-AGACTTCATGCGTGCCAACCCTGAGAC-3′-BHQ1 |
| Gene | Source | Sensitivity | Confidence Interval | Specificity | Confidence Interval | |
|---|---|---|---|---|---|---|
| PCR from samples without preincubation in TH enrichment broth | 16S rRNA | vagina | 70.4% | (49.8–86.2%) | 72.2% | (62.1–80.8%) |
| rectum | 40.9% | (20.7–63.6%) | 80.4% | (71.4–87.6%) | ||
| atr | vagina | 66.7% | (46.0–83.5%) | 97.9% | (92.7–99.7%) | |
| rectum | 36.4% | (17.2–59.3%) | 99% | (94.7–100%) | ||
| cfb | vagina | 55.6% | (35.3–74.5%) | 96.9% | (91.1–99.4%) | |
| rectum | 36.4% | (17.2–59.3%) | 99% | 94.7–100%) | ||
| PCR from samples preincubated in TH enrichment broth | atr | vagina | 100% | (87.2–100%) | 96.9% | (91.2–99.4%) |
| rectum | 100% | (84.6–100%) | 99% | (94.7–100%) | ||
| cfb | vagina | 100% | (87.2–100%) | 96.9% | (91.2–99.4%) | |
| rectum | 90.9% | (70.8–98.9%) | 99% | (94.7–100%) |
| Culture Methods | NAAT Directly form Clinical Materials | NAAT after Preincubation in TH Broth | |||||
|---|---|---|---|---|---|---|---|
| atr | cfb | atr + cfb | atr | cfb | atr + cfb | ||
| vagina | 7.14% (n = 6) | 11.90% (n = 10) | 8.33% (n = 7) | 10.71% (n = 9) | 7.14% (n = 6) | 8.33% (n = 7) | 7.14% (n = 6) |
| rectum | 1.19% (n = 1) | 4.76% (n = 4) | 3.57% (n = 3) | 4.76% (n = 4) | 1.19% (n = 1) | 0% (n = 0) | 1.19% (n = 1) |
| vagina + rectum | 14.29% (n = 12) | 3.57% (n = 3) | 3.57% (n = 3) | 5.95% (n = 5) | 15.48% (n = 13) | 14.29% (n = 12) | 16.67% (n = 14) |
| total GBS positive | 22.62% (n = 19) | 20.24% (n = 17) | 15.48% (n = 13) | 21.43% (n = 18) | 23.81% (n = 20) | 22.62% (n = 19) | 25% (n = 21) |
| total GBS negative | 77.38% (n = 65) | 79.76% (n = 67) | 84.52% (n = 71) | 78.57% (n = 66) | 76.19% (n = 64) | 77.38% (n = 65) | 75% (n = 63) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sroka-Oleksiak, A.; Pabian, W.; Sobońska, J.; Drożdż, K.; Bogiel, T.; Brzychczy-Włoch, M. Do NAAT-Based Methods Increase the Diagnostic Sensitivity of Streptococcus agalactiae Carriage Detection in Pregnant Women? Diagnostics 2023, 13, 863. https://doi.org/10.3390/diagnostics13050863
Sroka-Oleksiak A, Pabian W, Sobońska J, Drożdż K, Bogiel T, Brzychczy-Włoch M. Do NAAT-Based Methods Increase the Diagnostic Sensitivity of Streptococcus agalactiae Carriage Detection in Pregnant Women? Diagnostics. 2023; 13(5):863. https://doi.org/10.3390/diagnostics13050863
Chicago/Turabian StyleSroka-Oleksiak, Agnieszka, Wojciech Pabian, Joanna Sobońska, Kamil Drożdż, Tomasz Bogiel, and Monika Brzychczy-Włoch. 2023. "Do NAAT-Based Methods Increase the Diagnostic Sensitivity of Streptococcus agalactiae Carriage Detection in Pregnant Women?" Diagnostics 13, no. 5: 863. https://doi.org/10.3390/diagnostics13050863