
Timing of Early Postoperative MRI following Primary Glioblastoma Surgery—A Retrospective Study of Contrast Enhancements in 311 Patients
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. MRI
2.3. Timing of Early Postoperative MRI
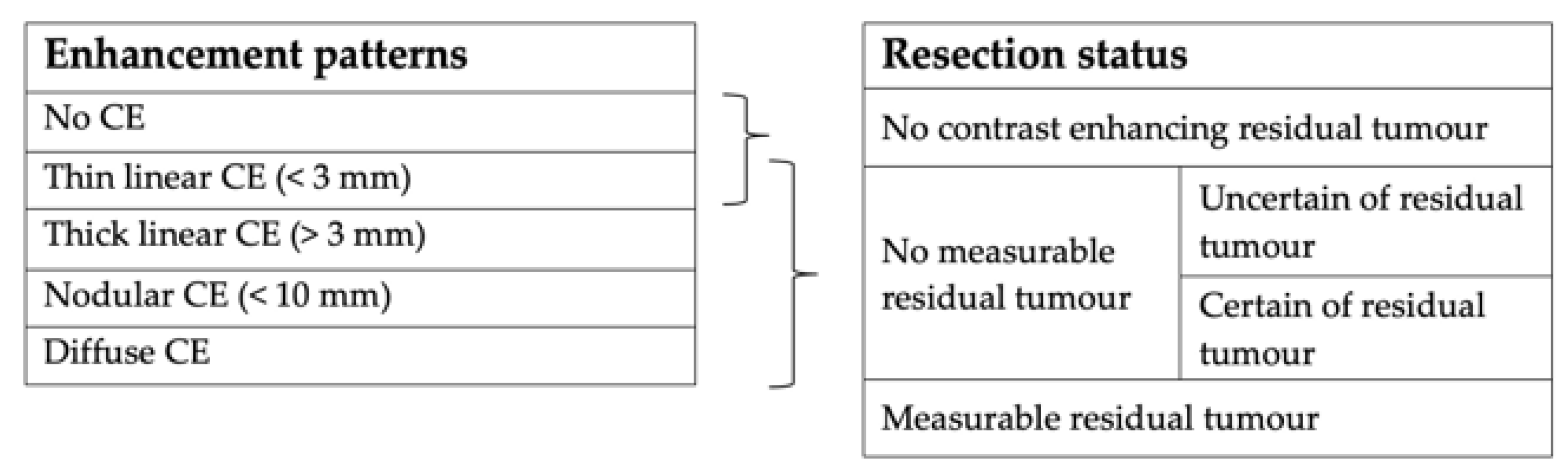
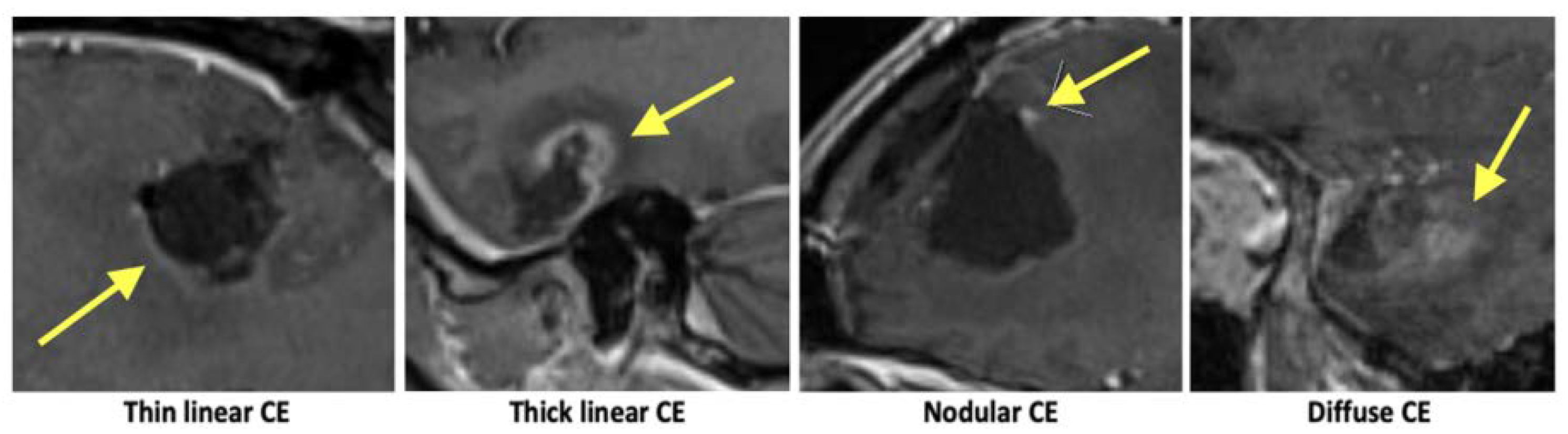
2.4. Image Analysis
2.5. Recorded Patient Clinical Parameters
2.6. Statistical Analysis
3. Results
3.1. Timing
3.2. Contrast Enhancements
3.3. Resection Status
3.4. Clinical Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thust, S.C.; Heiland, S.; Falini, A.; Jäger, H.R.; Waldman, A.D.; Sundgren, P.C.; Godi, C.; Katsaros, V.K.; Ramos, A.; Bargallo, N.; et al. Glioma Imaging in Europe: A Survey of 220 Centres and Recommendations for Best Clinical Practice. Eur. Radiol. 2018, 28, 3306–3317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Booth, T.C.; Luis, A.; Brazil, L.; Thompson, G.; Daniel, R.A.; Shuaib, H.; Ashkan, K.; Pandey, A. Glioblastoma Post-Operative Imaging in Neuro-Oncology: Current UK Practice (GIN CUP Study). Eur. Radiol. 2021, 31, 2933–2943. [Google Scholar] [CrossRef] [PubMed]
- Albert, F.K.; Forsting, M.; Sartor, K.; Adams, H.P.; Kunze, S. Early Postoperative Magnetic Resonance Imaging after Resection of Malignant Glioma: Objective Evaluation of Residual Tumor and Its Influence on Regrowth and Prognosis. Neurosurgery 1994, 34, 45–60; discussion 60–61. [Google Scholar] [CrossRef]
- Leao, D.J.; Craig, P.G.; Godoy, L.F.; Leite, C.C.; Policeni, B. Response Assessment in Neuro-Oncology Criteria for Gliomas: Practical Approach Using Conventional and Advanced Techniques. Am. J. Neuroradiol. 2020, 41, 10–20. [Google Scholar] [CrossRef]
- McGirt, M.J.; Chaichana, K.L.; Gathinji, M.; Attenello, F.J.; Than, K.; Olivi, A.; Weingart, J.D.; Brem, H.; Quiñones-Hinojosa, A.R. Independent Association of Extent of Resection with Survival in Patients with Malignant Brain Astrocytoma. J. Neurosurg. 2009, 110, 156–162. [Google Scholar] [CrossRef] [Green Version]
- Chaichana, K.L.; Jusue-Torres, I.; Navarro-Ramirez, R.; Raza, S.M.; Pascual-Gallego, M.; Ibrahim, A.; Hernandez-Hermann, M.; Gomez, L.; Ye, X.; Weingart, J.D.; et al. Establishing Percent Resection and Residual Volume Thresholds Affecting Survival and Recurrence for Patients with Newly Diagnosed Intracranial Glioblastoma. Neuro Oncol. 2014, 16, 113–122. [Google Scholar] [CrossRef]
- Brown, T.J.; Brennan, M.C.; Li, M.; Church, E.W.; Brandmeir, N.J.; Rakszawski, K.L.; Patel, A.S.; Rizk, E.B.; Suki, D.; Sawaya, R.; et al. Association of the Extent of Resection With Survival in Glioblastoma: A Systematic Review and Meta-Analysis. JAMA Oncol. 2016, 2, 1460–1469. [Google Scholar] [CrossRef] [Green Version]
- Miskin, N.; Unadkat, P.; Carlton, M.E.; Golby, A.J.; Young, G.S.; Huang, R.Y. Frequency and Evolution of New Postoperative Enhancement on 3 Tesla Intraoperative and Early Postoperative Magnetic Resonance Imaging. Neurosurgery 2020, 87, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Wirtz, C.R.; Knauth, M.; Staubert, A.; Bonsanto, M.M.; Sartor, K.; Kunze, S.; Tronnier, V.M. Clinical Evaluation and Follow-up Results for Intraoperative Magnetic Resonance Imaging in Neurosurgery. Neurosurgery 2000, 46, 1112–1120; discussion 1120–1122. [Google Scholar] [CrossRef]
- Forsting, M.; Albert, F.K.; Kunze, S.; Adams, H.P.; Zenner, D.; Sartor, K. Extirpation of Glioblastomas: MR and CT Follow-up of Residual Tumor and Regrowth Patterns. Am. J. Neuroradiol. 1993, 14, 77–87. [Google Scholar]
- Rykkje, A.M.; Li, D.; Skjøth-Rasmussen, J.; Larsen, V.A.; Nielsen, M.B.; Hansen, A.E.; Carlsen, J.F. Surgically Induced Contrast Enhancements on Intraoperative and Early Postoperative MRI Following High-Grade Glioma Surgery: A Systematic Review. Diagnostics 2021, 11, 1344. [Google Scholar] [CrossRef]
- Bette, S.; Gempt, J.; Huber, T.; Boeckh-Behrens, T.; Ringel, F.; Meyer, B.; Zimmer, C.; Kirschke, J.S. Patterns and Time Dependence of Unspecific Enhancement in Postoperative Magnetic Resonance Imaging after Glioblastoma Resection. World Neurosurg. 2016, 90, 440–447. [Google Scholar] [CrossRef] [PubMed]
- Masuda, Y.; Akutsu, H.; Ishikawa, E.; Matsuda, M.; Masumoto, T.; Hiyama, T.; Yamamoto, T.; Kohzuki, H.; Takano, S.; Matsumura, A. Evaluation of the Extent of Resection and Detection of Ischemic Lesions with Intraoperative MRI in Glioma Surgery: Is Intraoperative MRI Superior to Early Postoperative MRI? J. Neurosurg. 2019, 131, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Vogelbaum, M.A.; Jost, S.; Aghi, M.K.; Heimberger, A.B.; Sampson, J.H.; Wen, P.Y.; Macdonald, D.R.; Van den Bent, M.J.; Chang, S.M. Application of Novel Response/Progression Measures for Surgically Delivered Therapies for Gliomas: Response Assessment in Neuro-Oncology (RANO) Working Group. Neurosurgery 2012, 70, 234–243; discussion 243–244. [Google Scholar] [CrossRef] [Green Version]
- Weller, M.; van den Bent, M.; Preusser, M.; Le Rhun, E.; Tonn, J.C.; Minniti, G.; Bendszus, M.; Balana, C.; Chinot, O.; Dirven, L.; et al. EANO Guidelines on the Diagnosis and Treatment of Diffuse Gliomas of Adulthood. Nat. Rev. Clin. Oncol. 2021, 18, 170–186. [Google Scholar] [CrossRef]
- Lescher, S.; Schniewindt, S.; Jurcoane, A.; Senft, C.; Hattingen, E. Time Window for Postoperative Reactive Enhancement after Resection of Brain Tumors: Less than 72 Hours. Neurosurg. Focus 2014, 37, E3. [Google Scholar] [CrossRef] [Green Version]
- Majos, C.; Cos, M.; Castaner, S.; Gil, M.; Plans, G.; Lucas, A.; Bruna, J.; Aguilera, C. Early Post-Operative Magnetic Resonance Imaging in Glioblastoma: Correlation among Radiological Findings and Overall Survival in 60 Patients. Eur. Radiol. 2016, 26, 1048–1055. [Google Scholar] [CrossRef] [PubMed]
- Ekinci, G.; Akpinar, I.N.; Baltacioğlu, F.; Erzen, C.; Kiliç, T.; Elmaci, I.; Pamir, N. Early-Postoperative Magnetic Resonance Imaging in Glial Tumors: Prediction of Tumor Regrowth and Recurrence. Eur. J. Radiol. 2003, 45, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Smets, T.; Lawson, T.M.; Grandin, C.; Jankovski, A.; Raftopoulos, C. Immediate Post-Operative MRI Suggestive of the Site and Timing of Glioblastoma Recurrence after Gross Total Resection: A Retrospective Longitudinal Preliminary Study. Eur. Radiol. 2013, 23, 1467–1477. [Google Scholar] [CrossRef] [PubMed]
- Wen, P.Y.; Macdonald, D.R.; Reardon, D.A.; Cloughesy, T.F.; Sorensen, A.G.; Galanis, E.; Degroot, J.; Wick, W.; Gilbert, M.R.; Lassman, A.B.; et al. Updated Response Assessment Criteria for High-Grade Gliomas: Response Assessment in Neuro-Oncology Working Group. J. Clin. Oncol. 2010, 28, 1963–1972. [Google Scholar] [CrossRef] [PubMed]
- Inada-Kim, M.; Knight, T.; Sullivan, M.; Ainsworth-Smith, M.; Pike, N.; Richardson, M.; Hayward, G.; Lasserson, D. The Prognostic Value of National Early Warning Scores (NEWS) during Transfer of Care from Community Settings to Hospital: A Retrospective Service Evaluation. BJGP Open 2020, 4, bjgpopen20X101071. [Google Scholar] [CrossRef]
- Teasdale, G.; Maas, A.; Lecky, F.; Manley, G.; Stocchetti, N.; Murray, G. The Glasgow Coma Scale at 40 Years: Standing the Test of Time. Lancet Neurol. 2014, 13, 844–854. [Google Scholar] [CrossRef] [PubMed]
- Forsyth, P.A.; Petrov, E.; Mahallati, H.; Cairncross, J.G.; Brasher, P.; MacRae, M.E.; Hagen, N.A.; Barnes, P.; Sevick, R.J. Prospective Study of Postoperative Magnetic Resonance Imaging in Patients with Malignant Gliomas. J. Clin. Oncol. 1997, 15, 2076–2081. [Google Scholar] [CrossRef] [PubMed]
- Knauth, M.; Wirtz, C.R.; Tronnier, V.M.; Aras, N.; Kunze, S.; Sartor, K. Intraoperative MR Imaging Increases the Extent of Tumor Resection in Patients with High-Grade Gliomas. Am. J. Neuroradiol. 1999, 20, 1642–1646. [Google Scholar] [PubMed]
- Schneider, J.P.; Trantakis, C.; Rubach, M.; Schulz, T.; Dietrich, J.; Winkler, D.; Renner, C.; Schober, R.; Geiger, K.; Brosteanu, O.; et al. Intraoperative MRI to Guide the Resection of Primary Supratentorial Glioblastoma Multiforme—A Quantitative Radiological Analysis. Neuroradiology 2005, 47, 489–500. [Google Scholar] [CrossRef] [PubMed]
- Senft, C.; Bink, A.; Franz, K.; Vatter, H.; Gasser, T.; Seifert, V. Intraoperative MRI Guidance and Extent of Resection in Glioma Surgery: A Randomised, Controlled Trial. Lancet Oncol. 2011, 12, 997–1003. [Google Scholar] [CrossRef] [PubMed]
- Abedi, A.A.; Grunnet, K.; Christensen, I.J.; Michaelsen, S.R.; Muhic, A.; Møller, S.; Hasselbalch, B.; Poulsen, H.S.; Urup, T. A Prognostic Model for Glioblastoma Patients Treated with Standard Therapy Based on a Prospective Cohort of Consecutive Non-Selected Patients from a Single Institution. Front. Oncol. 2021, 11, 597587. [Google Scholar] [CrossRef]
- Garcia-Ruiz, A.; Naval-Baudin, P.; Ligero, M.; Pons-Escoda, A.; Bruna, J.; Plans, G.; Calvo, N.; Cos, M.; Majós, C.; Perez-Lopez, R. Precise Enhancement Quantification in Post-Operative MRI as an Indicator of Residual Tumor Impact Is Associated with Survival in Patients with Glioblastoma. Sci. Rep. 2021, 11, 695. [Google Scholar] [CrossRef]
- Wen, P.Y.; Kesari, S. Malignant Gliomas in Adults. N. Engl. J. Med. 2008, 359, 492–507. [Google Scholar] [CrossRef] [Green Version]
- Asthagiri, A.R.; Pouratian, N.; Sherman, J.; Ahmed, G.; Shaffrey, M.E. Advances in Brain Tumor Surgery. Neurol Clin 2007, 25, 975–1003, viii–ix. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| CE (48-h DIVIDE) | 0–47 h | 48-h | p-Value (Chi-Sq) | ||||
|---|---|---|---|---|---|---|---|
| Patients, n (of Total) | Present (%) | Patients, n (of Total) | Present (%) | ||||
| No CE | 41/183 | 22.4% | 7/81 | 8.6% | 0.008 | ||
| Thin linear | 93/183 | 50.8% | 56/81 | 69.1% | 0.006 | ||
| Thick linear | 66/183 | 36.1% | 32/81 | 39.5% | 0.594 | ||
| Nodular | 52/183 | 28.4% | 24/81 | 29.6% | 0.841 | ||
| Diffuse | 31/183 | 16.9% | 20/81 | 24.7% | 0.141 | ||
| CE (36- AND 60-h DIVIDE) | 0–36 h | 37–59 h | 60-h | p-Value (Chi-Sq) | |||
| Patients, n (of Total) | Present (%) | Patients, n (of Total) | Present (%) | Patients, n (of Total) | Present (%) | ||
| No CE | 22/60 | 36.7% | 25/182 | 13.7% | 1/22 | 4.5% | <0.001 |
| Thin linear | 24/60 | 40.0% | 108/182 | 59.3% | 17/22 | 77.3% | 0.004 |
| Thick linear | 19/60 | 31.7% | 70/182 | 38.5% | 9/22 | 40.9% | 0.594 |
| Nodular | 12/60 | 20% | 57/182 | 31.3% | 7/22 | 31.8% | 0.231 |
| Diffuse | 7/60 | 11.7% | 34/182 | 18.7% | 10/22 | 45.5% | 0.003 |
| RESECTION STATUS | 0–47-h | 48-h | p-Value (Chi-Sq) | ||
|---|---|---|---|---|---|
| Patients, n (of Total) | Present (%) | Patients, n (of Total) | Present (%) | ||
| No CE tumour | 66/218 | 30.3% | 24/93 | 25.8% | 0.426 |
| No measurable tumour | 117/218 | 53.7% | 57/93 | 61.3% | 0.215 |
| Measurable tumour | 35/218 | 16.1% | 12/93 | 12.9% | 0.477 |
| No measurable tumour: Certain or uncertain of residual tumour | |||||
| Certain | 90/117 | 76.9% | 38/57 | 66.7% | 0.150 |
| Uncertain | 27/117 | 23.1% | 19/57 | 33.3% | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rykkje, A.M.; Larsen, V.A.; Skjøth-Rasmussen, J.; Nielsen, M.B.; Carlsen, J.F.; Hansen, A.E. Timing of Early Postoperative MRI following Primary Glioblastoma Surgery—A Retrospective Study of Contrast Enhancements in 311 Patients. Diagnostics 2023, 13, 795. https://doi.org/10.3390/diagnostics13040795
Rykkje AM, Larsen VA, Skjøth-Rasmussen J, Nielsen MB, Carlsen JF, Hansen AE. Timing of Early Postoperative MRI following Primary Glioblastoma Surgery—A Retrospective Study of Contrast Enhancements in 311 Patients. Diagnostics. 2023; 13(4):795. https://doi.org/10.3390/diagnostics13040795
Chicago/Turabian StyleRykkje, Alexander Malcolm, Vibeke Andrée Larsen, Jane Skjøth-Rasmussen, Michael Bachmann Nielsen, Jonathan Frederik Carlsen, and Adam Espe Hansen. 2023. "Timing of Early Postoperative MRI following Primary Glioblastoma Surgery—A Retrospective Study of Contrast Enhancements in 311 Patients" Diagnostics 13, no. 4: 795. https://doi.org/10.3390/diagnostics13040795