
Guided Internet-Based Cognitive Behavioral Therapy for Insomnia: Prognostic and Treatment-Predictive Factors
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Dependent Variable
2.3. Prognostic and Treatment-Predictive Factors
2.3.1. Baseline Demographic and Medical History Variables
2.3.2. Variables on Sleep and Psychopathology
2.3.3. Intervention Adherence
2.4. Statistical Methods
3. Results
3.1. Baseline Differences
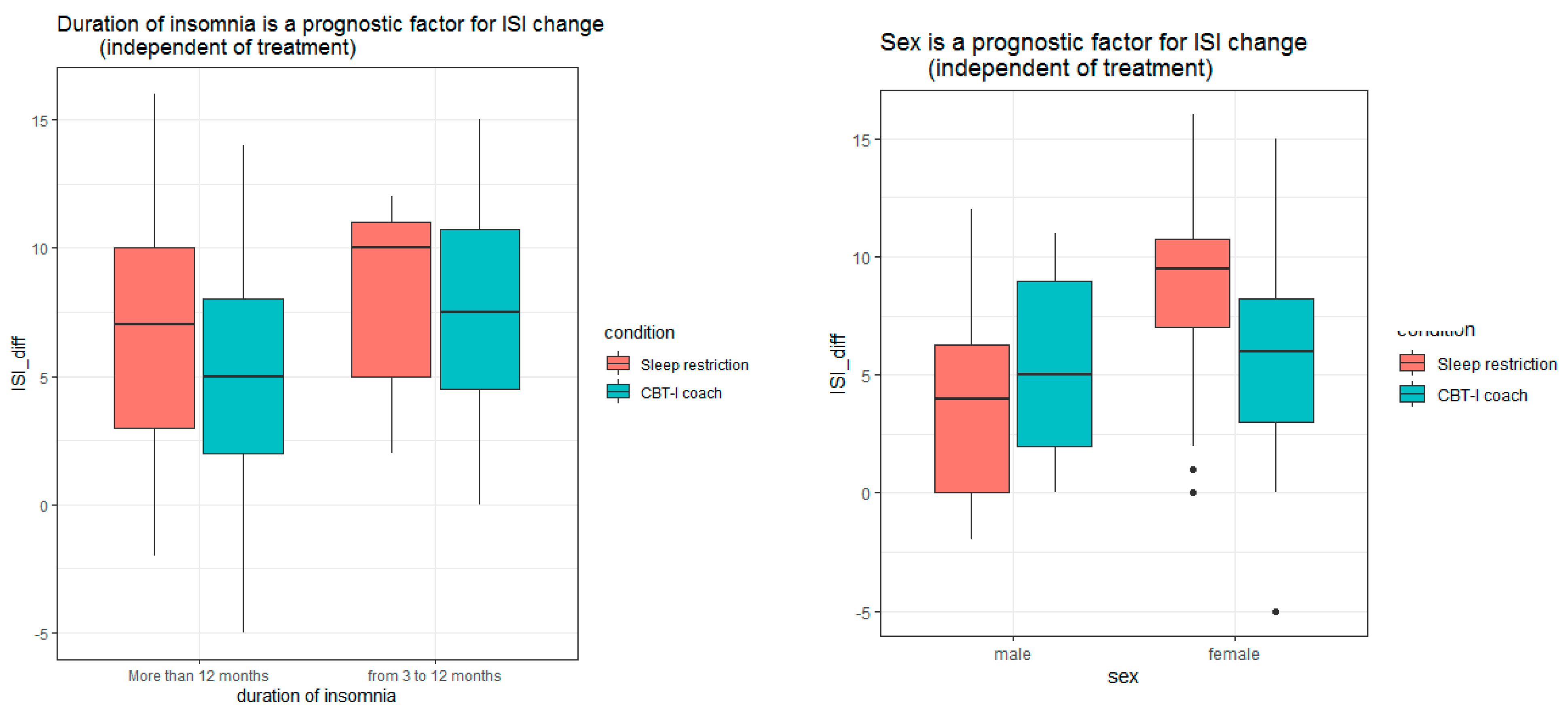
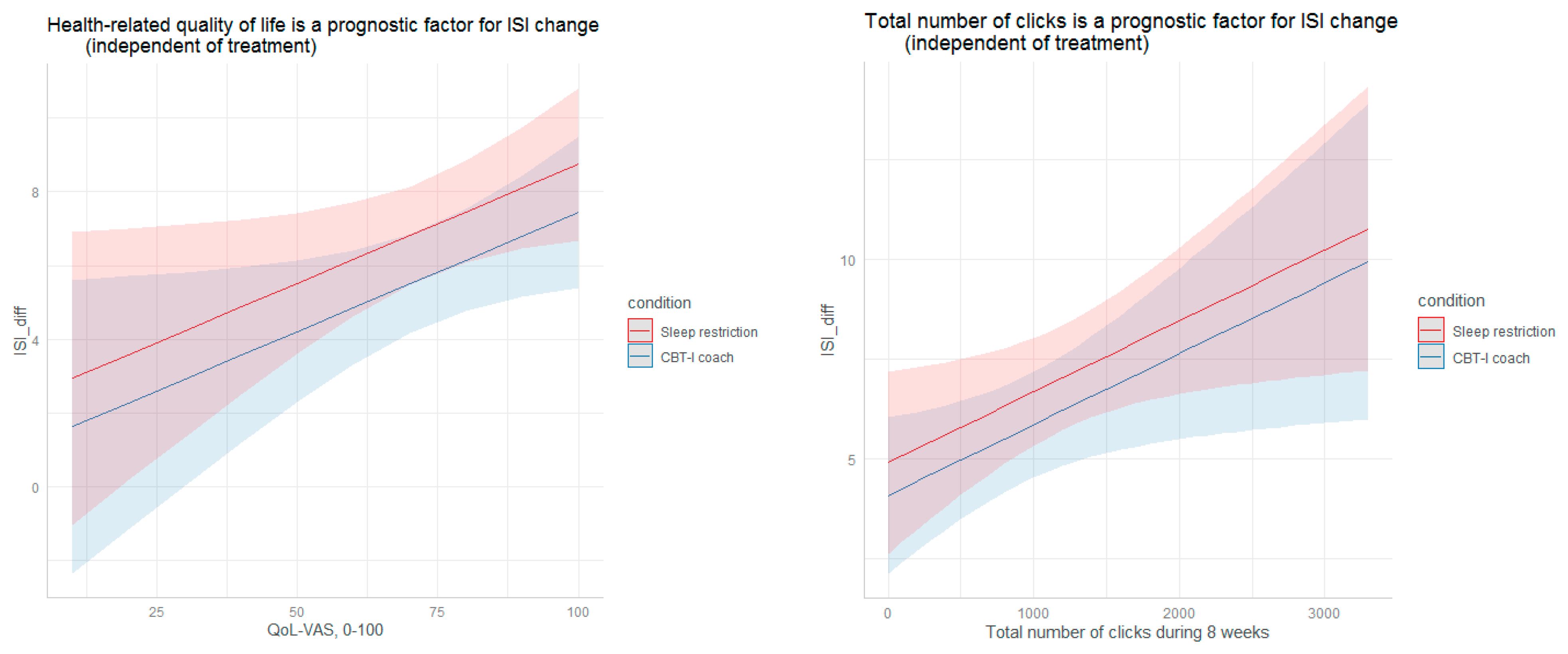
3.2. Prognostic Analysis
3.2.1. ISI Change from Pre-Treatment to Post-treatment
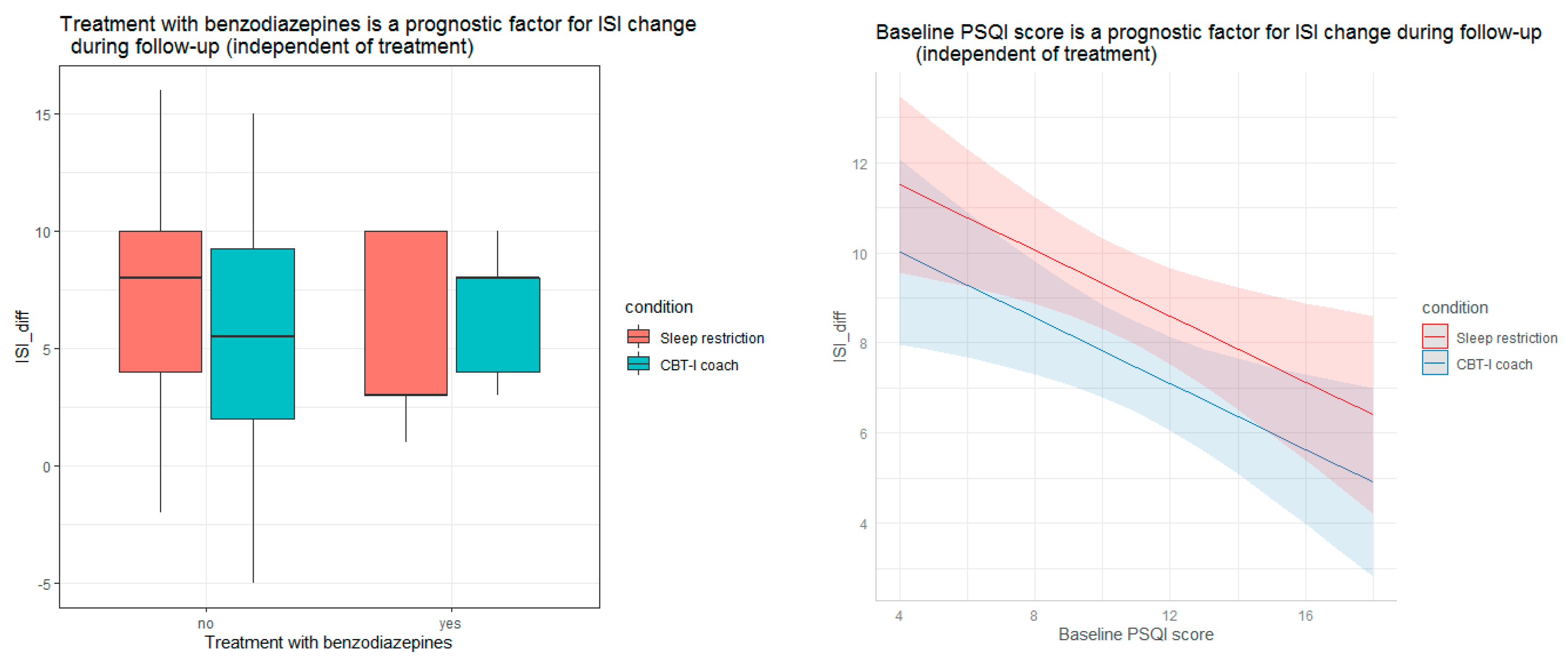
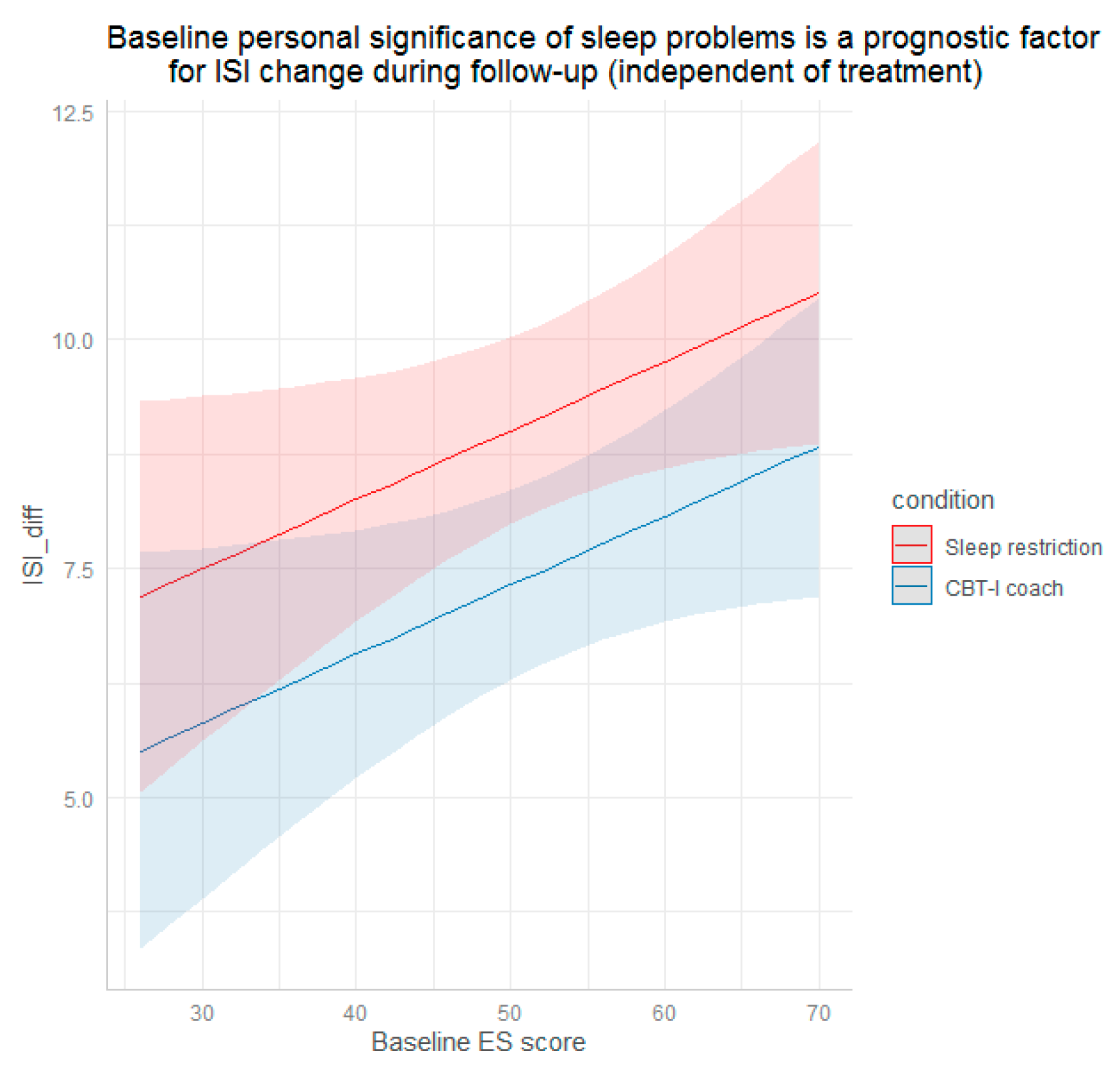
3.2.2. ISI Change from Pre-Treatment to Follow-Up
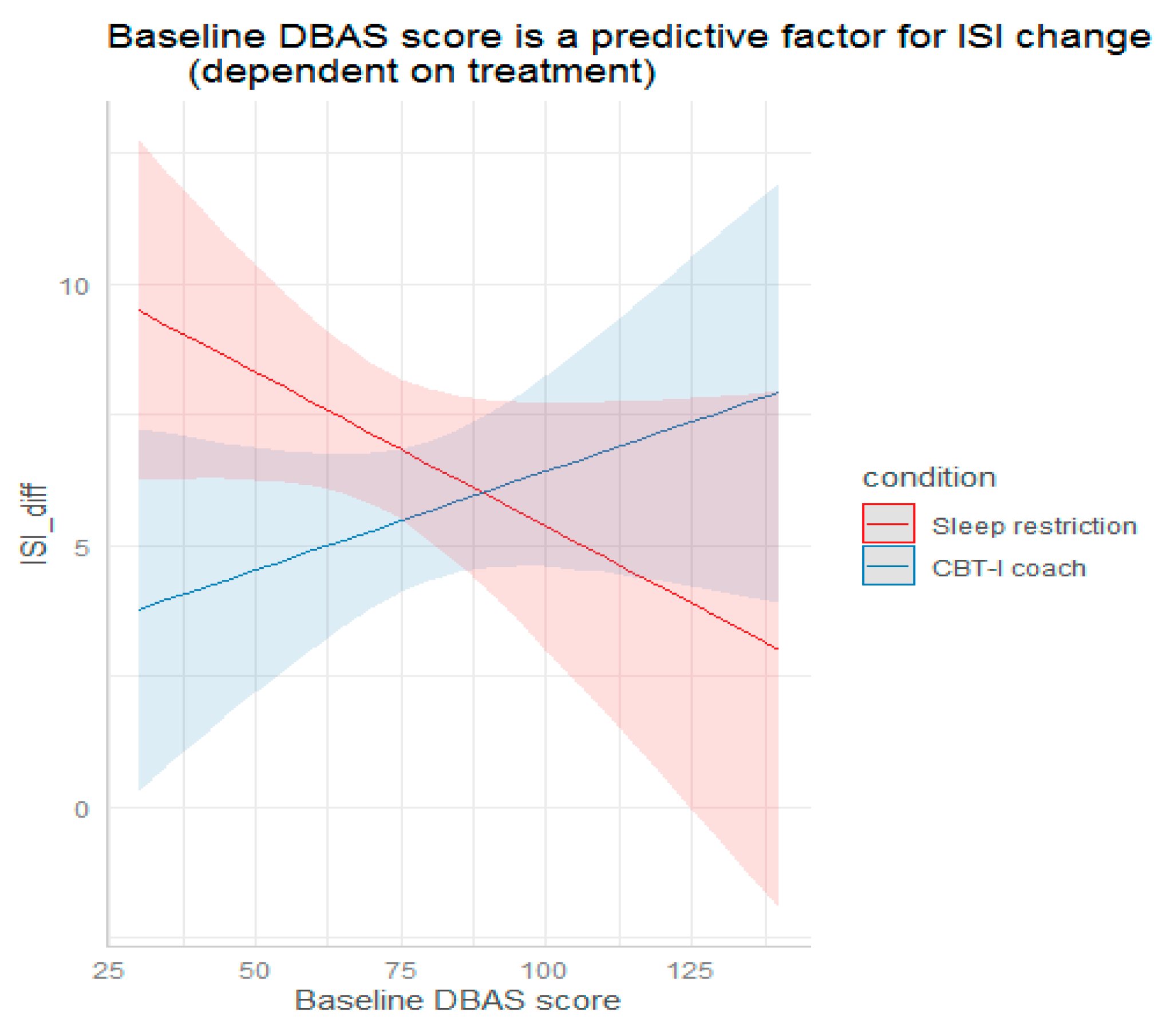
3.3. Predictive Analysis
ISI Change from Pre-Treatment to Post-Treatment and from Pre-Treatment to Follow-Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Riemann, D.; Baglioni, C.; Bassetti, C.; Bjorvatn, B.; Groselj, L.D.; Ellis, J.G.; Espie, C.A.; Garcia-Borreguero, D.; Gjerstad, M.; Gonçalves, M.; et al. European guideline for the diagnosis and treatment of insomnia. J. Sleep Res. 2017, 26, 675–700. [Google Scholar] [CrossRef] [PubMed]
- Wilson, S.; Anderson, K.; Baldwin, D.; Dijk, D.-J.; Espie, A.; Espie, C.; Gringras, P.; Krystal, A.; Nutt, D.; Selsick, H.; et al. British Association for Psychopharmacology consensus statement on evidence-based treatment of insomnia, parasomnias and circadian rhythm disorders: An update. J. Psychopharmacol. 2019, 33, 923–947. [Google Scholar] [CrossRef]
- Perlis, M.L.; Jungquist, C.; Smith, M.T.; Posner, D. Cognitive Behavioral Treatment of Insomnia: A Session-by-Session Guide, 1st ed.; Springer: New York, NY, USA, 2005. [Google Scholar] [CrossRef]
- Perlis, M.L.; Aloia, M.; Kuhn, B. Behavioral Treatments for Sleep Disorders; Academic Press: Cambridge, MA, USA, 2010. [Google Scholar]
- Morin, C.M.; Bootzin, R.R.; Buysse, D.J.; Edinger, J.D.; Espie, C.A.; Lichstein, K.L. Psychological and behavioral treatment on insomnia: An update of recent evidence. Sleep 2006, 29, 1398–1414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larsson, B.P.M.; Kaldo, V.; Broberg, A.G. Similarities and differences between practitioners of psychotherapy in Sweden: A comparison of attitudes between psychodynamic, cognitive, cognitive–behavioral and integrative therapists. J. Psychother. Integr. 2009, 19, 34–66. [Google Scholar] [CrossRef] [Green Version]
- Cuijpers, P.; van Straten, A.; Warmerdam, L. Are individual and group treatments equally effective in the treatment of depression in adults? A meta-analysis. Eur. J. Psychiatry 2008, 22, 38–51. [Google Scholar] [CrossRef] [Green Version]
- Everitt, H.; McDermott, L.; Leydon, G.; Yules, H.; Baldwin, D.; Little, P. GPs’ management strategies for patients with insomnia: A survey and qualitative interview study. Br. J. Gen. Pract. 2014, 64, e112–e119. [Google Scholar] [CrossRef] [Green Version]
- Linder, S.; Duss, S.B.; Dvořák, C.; Merlo, C.; Essig, S.; Tal, K.; Del Giovane, C.; Syrogiannouli, L.; Heinzer, R.; Nissen, C.; et al. Treating insomnia in Swiss primary care practices: A survey study based on case vignettes. J. Sleep Res. 2021, 30, e13169. [Google Scholar] [CrossRef]
- Seyffert, M.; Lagisetty, P.; Landgraf, J.; Chopra, V.; Pfeiffer, P.N.; Conte, M.; Rogers, M. Internet-Delivered Cognitive Behavioral Therapy to Treat Insomnia: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0149139. [Google Scholar] [CrossRef]
- Zachariae, R.; Lyby, M.S.; Ritterband, L.M.; O’Toole, M.S. Efficacy of internet-delivered cognitive-behavioral therapy for insomnia—A systematic review and meta-analysis of randomized controlled trials. Sleep Med. Rev. 2016, 30, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Baglioni, C.; Altena, E.; Bjorvatn, B.; Blom, K.; Bothelius, K.; Devoto, A.; Espie, C.A.; Frase, L.; Gavriloff, D.; Tuuliki, H.; et al. The European Academy for Cognitive Behavioural Therapy for Insomnia: An initiative of the European Insomnia Network to promote implementation and dissemination of treatment. J. Sleep Res. 2020, 29, e12967. [Google Scholar] [CrossRef] [Green Version]
- Lorenzo-Luaces, L.; Johns, E.; Keefe, J.R. The Generalizability of Randomized Controlled Trials of Self-Guided Internet-Based Cognitive Behavioral Therapy for Depressive Symptoms: Systematic Review and Meta-Regression Analysis. J. Med. Internet Res. 2018, 20, e10113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ritterband, L.M.; Thorndike, F.P.; Ingersoll, K.; Lord, H.R.; Gonder-Frederick, L.; Frederick, C.; Quigg, M.S.; Cohn, W.F.; Morin, C.M. Effect of a Web-Based Cognitive Behavior Therapy for Insomnia Intervention with 1-Year Follow-up. JAMA Psychiatry 2017, 74, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Vgontzas, A.N.; Liao, D.; Bixler, E.O.; Chrousos, G.P.; Vela-Bueno, A. Insomnia with Objective Short Sleep Duration is Associated with a High Risk for Hypertension. Sleep 2009, 32, 491–497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galbiati, A.; Sforza, M.; Fasiello, E. Impact of Phenotypic Heterogeneity of Insomnia on The Patients’ Response to Cognitive-Behavioral Therapy for Insomnia: Current Perspectives. Nat. Sci. Sleep 2019, 11, 367–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Batterham, P.J.; Christensen, H.; Mackinnon, A.J.; Gosling, J.A.; Thorndike, F.P.; Ritterband, L.M.; Glozier, N.; Griffiths, K.M. Trajectories of change and long-term outcomes in a randomised controlled trial of internet-based insomnia treatment to prevent depression. BJPsych Open 2017, 3, 228–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Constantino, M.J.; Manber, R.; Ong, J.; Kuo, T.F.; Huang, J.S.; Arnow, B.A. Patient Expectations and Therapeutic Alliance as Predictors of Outcome in Group Cognitive-Behavioral Therapy for Insomnia. Behav. Sleep Med. 2007, 5, 210–228. [Google Scholar] [CrossRef]
- Yeung, W.-F.; Chung, K.-F.; Ho, F.Y.-Y.; Ho, L.-M. Predictors of dropout from internet-based self-help cognitive behavioral therapy for insomnia. Behav. Res. Ther. 2015, 73, 19–24. [Google Scholar] [CrossRef]
- Troxel, W.M.; Conrad, T.S.; Germain, A.; Buysse, D.J. Predictors of Treatment Response to Brief Behavioral Treatment of Insomnia (BBTI) in Older Adults. J. Clin. Sleep Med. 2013, 9, 1281–1289. [Google Scholar] [CrossRef] [Green Version]
- Espie, C.A.; Inglis, S.J.; Harvey, L. Predicting clinically significant response to cognitive behavior therapy for chronic insomnia in general medical practice: Analyses of outcome data at 12 months posttreatment. J. Consult. Clin. Psychol. 2001, 69, 58–66. [Google Scholar] [CrossRef]
- Horsch, C.; Lancee, J.; Beun, R.J.; Neerincx, M.A.; Brinkman, W.-P. Adherence to Technology-Mediated Insomnia Treatment: A Meta-Analysis, Interviews and Focus Groups. J. Med. Internet Res. 2015, 17, e214. [Google Scholar] [CrossRef] [Green Version]
- Gosling, J.A.; Batterham, P.; Ritterband, L.; Glozier, N.; Thorndike, F.; Griffiths, K.M.; Mackinnon, A.; Christensen, H.M. Online insomnia treatment and the reduction of anxiety symptoms as a secondary outcome in a randomised controlled trial: The role of cognitive-behavioural factors. Aust. N. Z. J. Psychiatry 2018, 52, 1183–1193. [Google Scholar] [CrossRef] [PubMed]
- Schutte-Rodin, S.; Broch, L.; Buysse, D.; Dorsey, C.; Sateia, M. Clinical Guideline for the Evaluation and Management of Chronic Insomnia in Adults. J. Clin. Sleep Med. 2008, 4, 487–504. [Google Scholar] [CrossRef] [PubMed]
- Harvey, A.G.; Bélanger, L.; Talbot, L.; Eidelman, P.; Beaulieu-Bonneau, S.; Fortier-Brochu, E.; Ivers, H.; Lamy, M.; Hein, K.; Soehner, A.M.; et al. Comparative efficacy of behavior therapy, cognitive therapy, and cognitive behavior therapy for chronic insomnia: A randomized controlled trial. J. Consult. Clin. Psychol. 2014, 82, 670–683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morin, C.M. Insomnia: Psychological Assessment and Management; Guildford Press: New York, NY, USA, 1993. [Google Scholar]
- Miller, C.B.; Espie, C.A.; Epstein, D.R.; Friedman, L.; Morin, C.M.; Pigeon, W.R.; Spielman, A.J.; Kyle, S.D. The evidence base of sleep restriction therapy for treating insomnia disorder. Sleep Med. Rev. 2014, 18, 415–424. [Google Scholar] [CrossRef]
- Epstein, D.R.; Sidani, S.; Bootzin, R.R.; Belyea, M.J. Dismantling Multicomponent Behavioral Treatment for Insomnia in Older Adults: A Randomized Controlled Trial. Sleep 2012, 35, 797–805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krieger, T.; Urech, A.; Duss, S.B.; Blättler, L.; Schmitt, W.; Gast, H.; Bassetti, C.; Berger, T. A randomized controlled trial comparing guided internet-based multi-component treatment and internet-based guided sleep restriction treatment to care as usual in insomnia. Sleep Med. 2019, 62, 43–52. [Google Scholar] [CrossRef]
- American Academy of Sleep Medicine. The International Classification of Sleep Disorders, Revised: Diagnostic and Coding Manual; American Academy of Sleep Medicine: Chicago, IL, USA, 2014. [Google Scholar]
- Gerber, M.; Lang, C.; Lemola, S.; Colledge, F.; Kalak, N.; Holsboer-Trachsler, E.; Pühse, U.; Brand, S. Validation of the German version of the insomnia severity index in adolescents, young adults and adult workers: Results from three cross-sectional studies. BMC Psychiatry 2016, 16, 174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kent, P.; Cancelliere, C.; Boyle, E.; Cassidy, J.D.; Kongsted, A. A conceptual framework for prognostic research. BMC Med. Res. Methodol. 2020, 20, 172. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F., III; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Riemann, D.; Backhaus, J. Behandlung von Schlafstörungen; Psychologie. Verlags Union: Weinheim, Germany, 1996. [Google Scholar]
- Morin, C.M.; Vallières, A.; Ivers, H. Dysfunctional Beliefs and Attitudes about Sleep (DBAS): Validation of a Brief Version (DBAS-16). Sleep 2007, 30, 1547–1554. [Google Scholar] [CrossRef] [Green Version]
- Weingartz, S.; Pillmann, F. Meinungen-zum-Schlaf-Fragebogen. Somnologie-Schlafforsch Schlafmed. 2009, 13, 29–36. [Google Scholar] [CrossRef]
- Radloff, L. The CES-D scale: A self report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Hautzinger, M.; Bailer, M. Allgemeine Depressions-Skala; Beltz Verlag: Weinheim, Germany, 1993. [Google Scholar]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donkin, L.; Christensen, H.; Naismith, S.L.; Neal, B.; Hickie, I.B.; Glozier, N. A Systematic Review of the Impact of Adherence on the Effectiveness of e-Therapies. J. Med. Internet Res. 2011, 13, e52. [Google Scholar] [CrossRef] [PubMed]
- van Buuren, S.; Groothuis-oudshoorn, K. mice: Multivariate Imputation by Chained. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar]
- Ellis, J.G.; Perlis, M.L.; Espie, C.A.; Grandner, M.A.; Bastien, C.H.; Barclay, N.L.; Altena, E.; Gardani, M. The natural history of insomnia: Predisposing, precipitating, coping, and perpetuating factors over the early developmental course of insomnia. Sleep 2021, 44, zsab095. [Google Scholar] [CrossRef]
- Morin, C.M.; Bélanger, L.; LeBlanc, M.; Ivers, H.; Savard, J.; Espie, C.A.; Mérette, C.; Baillargeon, L.; Grégoire, J.-P. The Natural History of Insomnia. Arch. Intern. Med. 2015, 169, 447–453. [Google Scholar] [CrossRef] [Green Version]
- Gagné, A.; Morin, C.M. Predicting Treatment Response in Older Adults with Insomnia. J. Clin. Geropsychol. 2001, 7, 131–143. [Google Scholar] [CrossRef]
- Van Houdenhove, L.; Buyse, B.; Gabriëls, L.; Bergh, O.V.D. Treating Primary Insomnia: Clinical Effectiveness and Predictors of Outcomes on Sleep, Daytime Function and Health-Related Quality of Life. J. Clin. Psychol. Med. Settings 2011, 18, 312–321. [Google Scholar] [CrossRef] [PubMed]
- Bathgate, C.J.; Edinger, J.D.; Krystal, A.D. Insomnia Patients with Objective Short Sleep Duration Have a Blunted Response to Cognitive Behavioral Therapy for Insomnia. Sleep 2017, 40, zsw012. [Google Scholar] [CrossRef] [Green Version]
- Chow, P.I.; Ingersoll, K.S.; Thorndike, F.P.; Lord, H.R.; Gonder-Frederick, L.; Morin, C.M.; Ritterband, L.M. Cognitive mechanisms of sleep outcomes in a randomized clinical trial of internet-based cognitive behavioral therapy for insomnia. Sleep Med. 2018, 47, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Morin, C.M.; Edinger, J.D.; Beaulieu-Bonneau, S.; Ivers, H.; Krystal, A.D.; Guay, B.; Bélanger, L.; Cartwright, A.; Simmons, B.; Lamy, M.; et al. Effectiveness of Sequential Psychological and Medication Therapies for Insomnia Disorder A Randomized Clinical Trial. JAMA Psychiatry 2020, 77, 1107–1115. [Google Scholar] [CrossRef]
- Vallières, A.; Morin, C.M.; Guay, B. Sequential combinations of drug and cognitive behavioral therapy for chronic insomnia: An exploratory study. Behav. Res. Ther. 2005, 43, 1611–1630. [Google Scholar] [CrossRef] [PubMed]
- Morin, C.M.; Vallières, A.; Guay, B.; Ivers, H.; Savard, J.; Mérette, C.; Bastien, C.; Baillargeon, L. Cognitive Behavioral Therapy, Singly and Combined with Medication, for Persistent Insomnia. JAMA 2009, 301, 2005–2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frase, L.; Nissen, C.; Riemann, D.; Spiegelhalder, K. Making sleep easier: Pharmacological interventions for insomnia. Expert Opin. Pharmacother. 2018, 19, 1465–1473. [Google Scholar] [CrossRef]
- Lancee, J.; Effting, M.; van der Zweerde, T.; van Daal, L.; van Straten, A.; Kamphuis, J. Cognitive processes mediate the effects of insomnia treatment: Evidence from a randomized wait-list controlled trial. Sleep Med. 2019, 54, 86–93. [Google Scholar] [CrossRef]
- Lancee, J.; Eisma, M.C.; Van Straten, A.; Kamphuis, J.H. Sleep-Related Safety Behaviors and Dysfunctional Beliefs Mediate the Efficacy of Online CBT for Insomnia: A Randomized Controlled Trial. Cogn. Behav. Ther. 2015, 44, 406–422. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MCT n = 42 | SRT n = 41 | Statistic | |
|---|---|---|---|
| Age, years; mean, SD | 42.17 (12.40) | 46.59 (17.52) | t = −1.32, p = 0.19 |
| Body mass index, kg/m2; mean, SD | 23.60 (3.64) | 24.23 (5.20) | t = −0.64, p = 0.52 |
| Sex, n (%) | |||
| Female | 26 (61.9%) | 28 (68.3%) | X2 = 0.14, p = 0.70 |
| Male | 16 (38.1%) | 13 (31.7%) | |
| Consumption of medical help within the last 3 months, n (%) | |||
| yes | 16 (38.1%) | 13 (31.7%) | X2 = 0.14, p = 0.70 |
| no | 26 (61.9%) | 28 (68.3%) | |
| Treatment with benzodiazepines, n (%) | |||
| yes | 9 (22) | 5 (11.9) | X2 = 0.86, p = 0.35 |
| no | 32 (78) | 37 (88.1) | |
| Treatment with antidepressants, n (%) | |||
| yes | 3 (7.3) | 4 (9.5) | X2 < 0.01, p = 1.00 |
| no | 38 (92.3) | 38 (90.5) | |
| Treatment with natural medicines, n (%) | |||
| yes | 5 (12.2) | 11 (26.2) | X2 = 1.79, p = 0.18 |
| no | 36 (87.8) | 31 (73.8) | |
| Duration of insomnia, n (%) | |||
| More than 3 months | 5 (11.9%) | 10 (24.4%) | X2 = 1.42, p = 0.23 |
| More than 1 year | 37 (88.1%) | 31 (75.6%) | |
| Marital status, n (%) | |||
| Single | 11 (26.2%) | 9 (22.0%) | X2 = 3.26, p = 0.35 |
| Having a partner | 9 (21.4%) | 13 (31.7%) | |
| Divorced | 2 (4.8%) | 5 (12.2%) | |
| Married | 20 (47.6%) | 14 (34.1%) | |
| Widowed | 0 (0.0%) | 0 (0.0%) | |
| Employment, n (%) | |||
| Retired | 1 (2.4%) | 4 (9.8%) | X2 = 4.11, p = 0.39 |
| Homemaker | 0 (0.00%) | 0 (0.00%) | |
| Student | 5 (11.9%) | 6 (14.6%) | |
| Full-time employed | 24 (57.1%) | 17 (41.5%) | |
| Part-time employed | 12 (28.6%) | 13 (31.7%) | |
| Education, n (%) | |||
| No education | 0 (0.0%) | 2 (4.9%) | X2 = 2.35, p = 0.50 |
| Vocational training | 11 (26.2%) | 12 (29.3%) | |
| Higher secondary school | 4 (9.5%) | 3 (7.3%) | |
| University education | 27 (64.3%) | 24 (58.5%) | |
| ISI; mean, SD | 16.20 (3.75) | 17.37 (3.44) | t = −1.47, p = 0.15 |
| PSQI; mean, SD | 10.12 (3.13) | 11.05 (3.14) | t = −1.35, p = 0.18 |
| DBAS; mean, SD | 70.63 (21.83) | 80.63 (21.40) | t = −2.12, p = 0.04 |
| ADS-K; mean, SD | 12.83 (6.33) | 13.05 (5.42) | t = −0.04, p = 0.97 |
| QoL_total; mean, SD | 74.27 (17.62) | 73.00 (15.25) | t = −0.45, p = 0.65 |
| QoL-VAS; mean, SD | 1.37 (0.40) | 1.4 (0.37) | t = 0.32, p = 0.75 |
| Success expectancy; mean, SD | 5.07 (1.88) | 5.29 (1.59) | t = −0.65, p = 0.52 |
| Personal significance of sleep problems; mean, SD | 51.9 (10.45) | 52.32 (9.48) | t = −0.05, p = 0.96 |
| Sleep efficiency, %; mean, SD | 76.02 (13.89) | 77.49 (11.35) | t = 0.53, p = 0.60 |
| Total sleep time, minutes; mean, SD | 364.05 (72.61) | 371.47 (57.75) | t = 0.51, p = 0.61 |
| Sleep latency, minutes; mean, SD | 40.83 (43.21) | 24.32 (23.39) | t = −2.16, p = 0.03 |
| Wake after sleep onset, minutes; mean, SD | 50.28 (40.92) | 55.53 (46.09) | t = 0.55, p = 0.58 |
| Time spent online, minutes; median (Q1;Q3) | 481 (282; 907.35) | 392 (183.43; 591.57) | t = 2.58, p = 0.01 |
| Total number of clicks; mean, SD | 1470.76 (1535.67) | 1064.0 (664.06) | t = 2.124, p = 0.04 |
| Prognostic Analysis ISI_diff1~ISI_t0 + Var_Predictor + Condition | Prognostic Analysis ISI_diff2~ISI_t0 + Var_Predictor + Condition | |||
|---|---|---|---|---|
| Estimate (SE) for the Main Effect of Variable | p Value | Estimate (SE) for the Effect of Variable | p Value | |
| Intercept | 0.79 (2.32) | 0.735 | −0.60 (1.82) | 0.743 * |
| ISI_total_t0 | 0.33 (0.14) | 0.018 * | 0.53 (0.11) | 3.82 × 10−6 * |
| Condition | −1.30 (0.98) | 0.189 | −1.65 (0.75) | 0.039 * |
| Age, years | 0.01 (0.03) | 0.855 | 0.01 (0.76) | 0.814 |
| Sex, male (29) | 1.00 (0.00) | 0.032 * | 1.00 (0.00) | 0.153 |
| female (54) | 2.20 (1.00) | 1.13 (0.78) | ||
| Weight | −0.06 (0.03) | 0.069 | −0.01 (0.03) | 0.653 |
| BMI | −0.15 (0.11) | 0.180 | −0.06 (0.08) | 0.516 |
| Marital status | F = 1.763 | 0.161 | F = 1.45 | 0.080 |
| Employment | F = 1.614 | 0.179 | F = 0.97 | 0.428 |
| Education | 0.65 (0.53) | 0.225 | 0.02 (0.41) | 0.964 |
| Consumption of medicine last 3 months | ||||
| yes (29) | 1.00 (0.00) | 0.960 | 1.00 (0.00) | 0.174 |
| no (54) | −0.05 (1.03) | 1.07 (0.78) | ||
| Treatment with benzodiazepines | ||||
| yes (14) | 1.00 (0.00) | 0.368 | 1.00 (0.00) | 0.014 * |
| no (69) | −1.23 (1.35) | −2.51 (1.01) | ||
| Treatment with antidepressants | ||||
| yes (7) | 1.00 (0.00) | 0.350 | 1.00 (0.00) | 0.096 |
| no (76) | 1.52 (1.75) | 2.23 (1.32) | ||
| Treatment with natural medicine | ||||
| yes (16) | 1.00 (0.00) | 0.790 | 1.00 (0.00) | 0.797 |
| no (67) | 0.33 (1.26) | 0.25 (0.96) | ||
| Duration of insomnia | ||||
| 3 to 12 months (15) | 1.00 (0.00) | 0.011 * | 1.00 (0.00) | 0.293 |
| More than 1 year (68) | −3.27 (1.27) | 1.07 (1.07) | ||
| PSQI | −0.12 (0.18) | 0.490 | −0.37 (0.13) | 0.007 * |
| DBAS | −0.01 (0.03) | 0.830 | 0.002 (0.02) | 0.277 |
| ADS | 0.105 (0.09) | 0.229 | −0.10 (0.07) | 0.156 |
| QoL | −1.33 (1.36) | 0.330 | −0.14 (1.03) | 0.167 |
| QoL health related VAS, 0–100 | 0.06 (0.03) | 0.036 * | 0.03 (0.02) | 0.162 |
| Success expectancy, 0–9 | 0.37 (0.29) | 0.200 | 0.21 (0.22) | 0.339 |
| Personal significance of sleep problems, 10–70 | 0.01 (0.05) | 0.913 | 0.08 (0.04) | 0.044 * |
| Total number of clicks | 0.002 (0.001) | 0.029 * | 0.0005 (0.001) | 0.477 |
| Time spent online, hours | 0.09 (0.05) | 0.092 | 0.07 (0.04) | 0.081 |
| Sleep efficiency, % | 0.001 (0.004) | 0.988 | 0.02 (0.03) | 0.513 |
| Total sleep time, min | 0.01 (0.01) | 0.452 | −0.003 (0.01) | 0.632 |
| Sleep onset latency, min | 0.002 (0.02) | 0.910 | −0.01 (0.01) | 0.623 |
| Wake after sleep onset, min | −0.01 (0.01) | 0.353 | −0.0004 (0.01) | 0.963 |
| Predictive Analysis ISI_diff1~ISI_t0 + Var_Predictor * Condition | Predictive Analysis ISI_diff2~ISI_t0 + Var_Predictor * Condition | |||
|---|---|---|---|---|
| Estimate (SE) for the Effect of Interaction Variable: Condition | p Value | Estimate (SE) for the Effect of Interaction Variable: Condition | p Value | |
| Intercept | 0.79 (2.32) | 0.735 | −0.60 (1.82) | 0.743 * |
| ISI_total_t0 | 0.33 (0.14) | 0.018 * | 0.53 (0.11) | 3.82 × 10−6 * |
| Condition | −1.30 (0.98) | 0.189 | −1.65 (0.75) | 0.039 * |
| Age, years | 0.01 (0.07) | 0.873 | 0.03 (0.05) | 0.590 |
| Sex, male (29) | 1.00 (0.00) | 0.102 | 1.00 (0.00) | 0.257 |
| female (54) | −3.30 (1.99) | −1.79 (1.57) | ||
| Weight | 0.11 (0.07) | 0.090 | 0.09 (0.05) | 0.081 |
| BMI | 0.39 (0.23) | 0.089 | 0.31 (0.18) | 0.080 |
| Social status | F = 1.152 | 0.334 | F = 1.71 | 0.172 |
| Working status | F = 0.576 | 0.632 | F = 0.465 | 0.708 |
| Education | −1.54 (1.05) | 0.149 | −0.40 (0.82) | 0.632 |
| Medications use | ||||
| yes (29) | 1.00 (0.00) | 0.96 | 1.00 (0.00) | 0.745 |
| no (54) | −2.51 (2.04) | 0.51 (1.56) | ||
| Benzodiazepines | ||||
| yes (14) | 1.00 (0.00) | 0.249 | 1.00 (0.00) | 0.834 |
| no (69) | 3.13 (2.69) | −0.42 (2.02) | ||
| Antidepressants | ||||
| yes (7) | 1.00 (0.00) | 0.109 | 1.00 (0.00) | 0.401 |
| no (76) | 5.64 (3.48) | 2.26 (2.67) | ||
| Natural medicine | ||||
| yes (16) | 1.00 (0.00) | 0.160 | 1.00 (0.00) | 0.156 |
| no (67) | 3.69 (2.61) | 2.86 (2.00) | ||
| Duration of insomnia | ||||
| 3 to 12 months (15) | 1.00 (0.00) | 0.704 | 1.00 (0.00) | 0.982 |
| More than 1 year (68) | 0.98 (2.57) | 0.05 (2.04) | ||
| PSQI | −0.05 (0.32) | 0.878 | −0.001 (0.23) | 0.998 |
| DBAS | 0.10 (0.05) | 0.040 * | 0.04 (0.04) | 0.345 |
| ADS | −0.26 (0.17) | 0.12 | −0.14 (0.13) | 0.270 |
| QoL | −3.73 (2.54) | 0.146 | −3.29 (1.93) | 0.092 |
| QoL health-related VAS, 0–100 | −0.02 (0.06) | 0.740 | 0.03 (0.05) | 0.520 |
| Success expectancy, 0–9 | −0.33 (0.57) | 0.564 | 0.10 (0.44) | 0.820 |
| Personal significance of sleep problems, 10–70 | 0.002 (0.10) | 0.986 | 0.07 (0.07) | 0.323 |
| Total number of clicks | −0.0005 (0.002) | 0.795 | −0.001 (0.001) | 0.546 |
| Time spent online, hours | 0.08 (0.18) | 0.655 | 0.05 (0.13) | 0.741 |
| Sleep efficiency, % | 0.05 (0.08) | 0.566 | 0.02 (0.06) | 0.731 |
| Total sleep time, min | 0.01 (0.02) | 0.550 | −0.01 (0.01) | 0.539 |
| Sleep onset latency, min | −0.01 (0.03) | 0.810 | −0.01 (0.03) | 0.746 |
| Wake after sleep onset, min | −0.03 (0.02) | 0.233 | −0.03 (0.02) | 0.132 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pchelina, P.; Duss, S.B.; Bernasconi, C.; Berger, T.; Krieger, T.; Bassetti, C.L.A.; Urech, A. Guided Internet-Based Cognitive Behavioral Therapy for Insomnia: Prognostic and Treatment-Predictive Factors. Diagnostics 2023, 13, 781. https://doi.org/10.3390/diagnostics13040781
Pchelina P, Duss SB, Bernasconi C, Berger T, Krieger T, Bassetti CLA, Urech A. Guided Internet-Based Cognitive Behavioral Therapy for Insomnia: Prognostic and Treatment-Predictive Factors. Diagnostics. 2023; 13(4):781. https://doi.org/10.3390/diagnostics13040781
Chicago/Turabian StylePchelina, Polina, Simone B. Duss, Corrado Bernasconi, Thomas Berger, Tobias Krieger, Claudio L. A. Bassetti, and Antoine Urech. 2023. "Guided Internet-Based Cognitive Behavioral Therapy for Insomnia: Prognostic and Treatment-Predictive Factors" Diagnostics 13, no. 4: 781. https://doi.org/10.3390/diagnostics13040781