1. Introduction
Prostate cancer is the second leading cause of cancer death in men, with an estimated 1,414,259 new deaths in 2020 worldwide [
1]. Prostate MRI is widely used to diagnose clinically significant prostate cancer in biopsy-naïve patients. It has been shown that prebiopsy MRI is superior to systematic biopsy in prostate cancer detection [
2]. Multiparametric magnetic resonance imaging (mpMRI), including T2-weighted, diffusion-weighted, and dynamic contrast-enhanced scans, plays an integral role in enhanced visualization of prostate cancer, improved biopsy targeting, and monitoring proactive signs of disease progression [
2]. In addition, MRI-guided biopsy is also increasingly adopted clinically for risk assessment, replacing the conventional transrectal ultrasound-guided biopsy [
3].
The demand for prostate MRI is growing due to mounting evidence and guideline recommendations, and radiologists are facing a substantial increase in referrals [
4]. The prostate imaging reporting and data system (PI-RADS) provides fundamental guidelines for assessing prostate MRI by classifying lesions into risk significance as the score increases [
5]. PI-RADSv2 has been shown to help radiologists and specialists detect high-grade prostate lesions with high sensitivity [
6]. However, PI-RADS has been hindered by poor inter-reader and intra-reader agreement [
7]. Furthermore, PI-RADS reporting requires substantial expert knowledge, and radiologists with less experience had more significant inter-reader variability in PI-RADS scoring [
8].
With recent developments in deep learning, convolutional neural networks (CNNs) exceeded human performance in natural image analysis [
9], especially in image classification [
9] and segmentation [
10]. Deep learning-based artificial intelligence (AI) algorithms have shown great promise in medical image segmentation, detection, and classification [
11,
12,
13] in recent years.
Deep learning-based lesion detection and PI-RADS classification algorithms are needed for prostate MRI reporting in clinical practice. Recent studies have shown the feasibility of detecting prostate cancer on mpMRI, using deep neural networks [
14,
15,
16,
17]. Some networks distinguished prostate cancer from normal tissues and provided the likelihood of prostate cancer [
18,
19,
20]. Some studies compared the performance of network predictions with radiologists’ PI-RADS reports [
18,
21]. However, the existing method for PI-RADS classification is semi-automated, as manual lesion contours must be inputted into the model [
22]. Additionally, these CNNs require a large amount of annotated data and data augmentation, alleviating class imbalance. Few of them addressed lesion detection and classification tasks jointly in one network [
23,
24] taking spatial relation between prostate lesion and zonal area into consideration which might be important for PI-RADS classification. The recent study only achieved reasonable performance at a PI-RADS cutoff value ≥ 4 [
24] with three independent networks for lesion detection and classification which was time-consuming and required more data to train multiple networks. Therefore, this study aimed to solve above-mentioned issues and develop a multi-task network to segment and predict PI-RADS category efficiently by exploiting spatial relation between the prostate lesion and zonal area using limited data.
Capsule Network (CapsNet) [
25] helps mitigate data starvation in deep learning-based medical image analysis due to its promising equivariance properties, representing the spatial/viewpoint variability of an object in a capsule (i.e., vector) format [
26]. The basic idea of CapsNet is to encode the part-whole relationships (e.g., scale, locations, orientations, brightnesses) between various entities, i.e., objects, and parts of an object, to achieve viewpoint equivariance [
25]. Unlike CNN models that learn all partial features of an object, CapsNet understands the relationship between these features through weights that are dynamically computed in each forward pass [
25]. This optimization mechanism, dynamic routing, allows the contribution of parts to the whole object to be weighted differently during training and inference [
25]. CapsNet has been applied to medical image segmentation in recent studies [
27,
28], demonstrating the prominence of hybrid architecture between Capsule-based and traditional neural networks in medical image analysis [
27].
For PI-RADS, the categorization depends on not only the dimension, edge morphology, and signal intensity, but also the positional relations of the lesion (e.g., extraprostatic extension/invasion) and its zonal location relative to the transition zone (TZ) and peripheral zone (PZ) [
5]. Specifically, each lesion can be scored 1–5 on diffusion-weighted imaging (DWI) and T2-weighted (T2W) MRI, as well as by the presence or absence of dynamic contrast enhancement. The contribution of these scores to the overall PI-RADS assessment differs depending on whether the lesion is located in the TZ or PZ of the prostate. For the TZ lesion, the PI-RADS assessment is primarily determined by the T2W score and sometimes modified by the DWI score. For the PZ lesion, the PI-RADS assessment is determined mainly by the DWI score and modulated by the presence of dynamic contrast enhancement [
5]. Such spatial relationships and other lesion properties (location, scale, dimension, etc.) can be encoded and represented by CapsNet in a single capsule vector, which is helpful for prostate cancer detection and classification.
Due to our relatively small database, the model in this study was based on a multi-task network with MiniSeg [
29] as the backbone for prostate cancer segmentation and PI-RADS classification. Our model, named MiniSegCaps, is built upon a 2D CapsuleNet block, which considers positional relations between the lesion, TZ, and PZ, and 2D convolutional encoder and decoder. Previous studies for PI-RADS classification based on convolutional blocks mainly used one-hot encoding for multi-class classification [
23,
24]. Different classes were assumed to be equally distanced, ignoring that cancer is a progressive disease. Inspired by Gleason Score prediction in [
29], we adopt the ordinal encoding for different PI-RADS categories to encode the lesion progression into vectors. Ordinal encoded vectors are not mutually orthogonal and can suggest the similarities and differences between PI-RADS categories compared with one-hot encoding [
29]. In our work, MiniSegCaps encodes five labels, i.e., four PI-RADS categories plus a normal issue type, into ordinal encoded vectors, predicting the ordinal encoded vector for each pixel using mpMRI. Mini-SegCaps can predict lesion masks, the scope (i.e., ordinal encoding) of PI-RADS categories, benign prostatic hyperplasia (BPH), and lesion malignancy. Inspired by a recurrent fully convolutional network (RFCN) [
30], a gated recurrent units (GRU) module [
31] leveraging inter-slice spatial dependences is also integrated into MiniSegCaps, to exploit the spatial information across adjacent slices, which are represented by capsule vectors, from the entire volume.
The contributions of our work are summarized as follows. Firstly, we proposed a multi-task network to segment and classify prostate cancer on mpMRI jointly. MiniSegCaps inherits the merits of both the 2D CapsuleNet to exploit spatial information and the 2D convolutional blocks to learn better visual representation. Secondly, for MiniSegCaps, we adopted the ordinal encoding to characterize PI-RADS score and the GRU on capsules to exploit spatial knowledge across slices in the entire volume.
4. Discussion
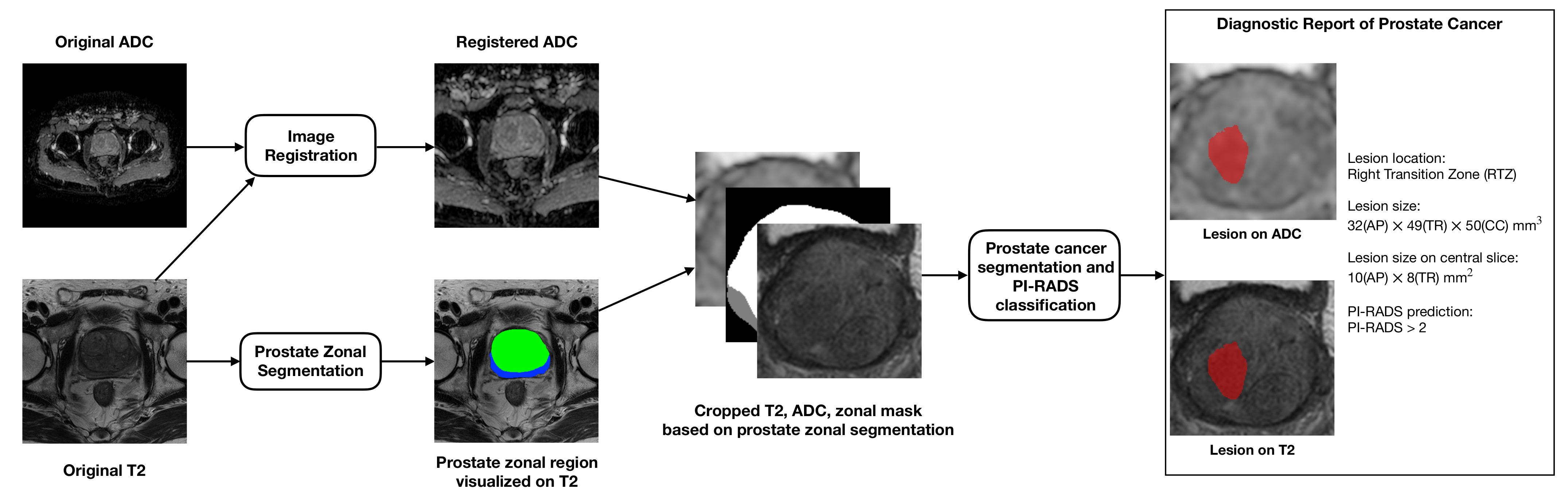
In this study, we presented a pipeline for automatic diagnosis of prostate cancer and a novel deep learning method, MiniSegCaps, for prostate cancer segmentation and PI-RADS classification on mpMRI. Our MiniSegCaps, a multi-branch network consisting of capsule predictive layers, exploited the spatial relationships between objects on mpMRI, and a CapsGRU to utilize spatial information across adjacent slices, predicting lesion segmentation and PI-RADS classifications jointly. We trained and validated MiniSegCaps under fivefold cross-validation using 462 pre-operative mpMRIs with annotations of all MRI-visible prostate cancer lesions and benign nodules (e.g., BPH). Experimental results show that our MiniSegCaps outperformed all six CNN-based baseline methods in PI-RADS classification, especially for PI-RADS ≥ 4, which is of great value for diagnosing clinically significant prostate cancer. For lesion segmentation, MiniSegCaps also achieved better performance than baseline methods. We also deployed a structured report GUI integrated into the overall workflow to automatically produce a prostate MRI report, which contained the predicted lesion mask, lesion visualization on T2 and ADC, and predicted probability of each PI-RADS category, position, and the dimension of each lesion, etc.
Previous studies for prostate cancer diagnosis on mpMRI mainly focused on prostate cancer detection based on classic segmentation networks such as U-Net [
14,
15,
16,
17,
19,
20,
21]. They showed reasonable performance in distinguishing prostate cancer from normal tissues [
14,
15,
16,
17,
19,
20,
21]. However, few considered the relative spatial information of prostate cancer to different anatomical structures to help identify prostate cancer from other anatomical tissues. Furthermore, most of them require a large amount of annotated data which are costly and difficult to acquire in practice. Instead, our MiniSegCaps can integrate anatomical knowledge by exploiting the spatial relationship between objects learned by the capsule branch. It can also be practicable on a small database due to the promising equivariance properties of capsule layers modeling the spatial/viewpoint variability of an object in the image and a lightweight MiniSeg backbone. Furthermore, the CapsGRU in our model is designed to utilize spatial information across adjacent slices, which could reduce flaws in the 2D model when dealing with a series of slices in volume. The experimental results in this study demonstrate that our MiniSegCaps achieved the best performance on prostate cancer detection compared with those classic segmentation networks.
The previous algorithms for PI-RADS classification did not address prostate lesion detection and required manual lesion contouring by radiologists [
22]. However, recent work [
21,
24] comparing prostate cancer detection and PI-RADS classification between deep learning methods and radiologists showed comparable performance between classic CNNs and radiologists. However, the trained models in these studies achieved prostate cancer detection in separate steps. They cannot predict specific lesion segmentations [
21], and mainly achieved good performance at a PI-RADS cutoff value ≥ 4. Furthermore, those studies only achieved classification on PI-RADS 3, 4, and 5, not including PI-RADS 1/2. Instead, our multi-branch MiniSegCaps can simultaneously produce prostate cancer masks by the decoder branch and the binary high-grade/low-grade PI-RADS categories (PI-RADS 1/2/3, 4/5) by the Capsule-predictive branch in an end-to-end diagnosis pipeline. Our MiniSegCaps also considered the anatomical priors by learning spatial relationships between objects and achieved the best performance on PI-RADS scoping classification compared with those existing deep neural networks. FocalNet [
29] was a multi-class segmentation network for prostate cancer detection and Gleason scores prediction on mpMRIs with focal loss and mutual finding loss. We also applied this method to our prostate cancer segmentation and PI-RADS classification tasks for comparison. The experimental results demonstrate that our MiniSegCaps outperformed the FocalNet in lesion segmentation and PI-RADS classification due to exploiting the spatial relationship between objects for PI-RADS prediction by capsule predictive layers in comparison with FocalNet. A more recent study [
23] used 3D cascaded U-Net, residual network architecture for prostate cancer detection, and PI-RADS classification, which required more training data than the 2D networks. Although it achieved acceptable performance in lesion segmentation (0.359 dice coefficient), the overall performance in the PI-RADS classification was unsatisfactory (30.8% accuracy). We tried a residual network (ResNet18 [
41]) for PI-RADS classification based on segmented lesions. According to our experiments, the trained model was always prone to over-fitting during the training process, and the corresponding results on the testing cohort were unsatisfactory (30.56% accuracy). Instead, our MiniSegCaps showed prominence in dealing with a small database and achieved better performance in both lesion segmentation (0.712 dice coefficient) and PI-RADS classification (71.56% accuracy) in patient-level evaluation.
Our MiniSegCaps achieved satisfactory prostate cancer detection and PI-RADS classification compared with state-of-the-art methods, especially for cutoff at PI-RADS 3, with clinical importance in disease management. Distinguishing PI-RADS 2 and 3 is challenging for radiologists due to the insignificant difference in hypointense and homogeneous signal intensity on mpMRI. Meanwhile, determining PI-RADS 2 and 3 plays a pivotal role in the differential diagnosis of prostate cancer as it directly affects the clinical decision-making, i.e., biopsy or not. Specifically, prostate cancer with PI-RADS ≥ 3 usually requires a further biopsy to assess lesion aggressiveness by giving a histologically assigned Gleason score (GS) in clinical practice [
2]. Therefore, accurate differentiation of PI-RADS 2/3 based on mpMRI reduces unnecessary biopsies [
3].
Our multi-task MiniSegCaps can jointly predict prostate cancer masks and PI-RADS categories and achieve satisfactory performance by exploiting spatial relationship between objects. The proposed framework could assist inexperienced readers or non-experts in providing consultations about the prostate cancer contour and PI-RADS categorical probabilities. However, there are also some limitations to this study: (1) We only achieved satisfactory results on PI-RADS scoping and binary high-grade/low-grade classification, not including specific PI-RADS categories due to the sample size limitation; (2) The performance of lesion segmentation and PI-RADS classification on low scores needs further improvement; (3) This study only conducted experiments on local data from one imaging center, not including data from multiple centers. These problems are expected to be solved by incorporating more cases of low PI-RADS categories and enlarging the database from multiple centers. Incorporating the public data from different sites into our database, e.g., those from PROSTATEx [
32] and NIH cancer image archive [
42], to enlarge the database for PI-RADS classification is currently underway in our lab. In the future, we plan to extend our work to multi-center datasets, further improving the performance of our model on multi-center datasets by incorporating meta learning [
43] or few-shot learning [
44].










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}