
Optical Coherence Tomography Angiography (OCT-A) in Uveitis: A Literature Review and a Reassessment of Its Real Role
 , , , , , and
, , , , , and
Abstract
:1. Introduction and Brief Overview of the Development of Imaging in Uveitis
1.1. Dual Fluorescein (FA) and Indocyanine Green Angiography (ICGA)
1.2. Optical Coherence Tomography (OCT)
1.3. Enhanced Depth Imaging OCT (EDI-OCT)
1.4. Blue Light Fundus Autofluorescence (BAF)
2. Optical Coherence Tomography Angiography (OCT-A)
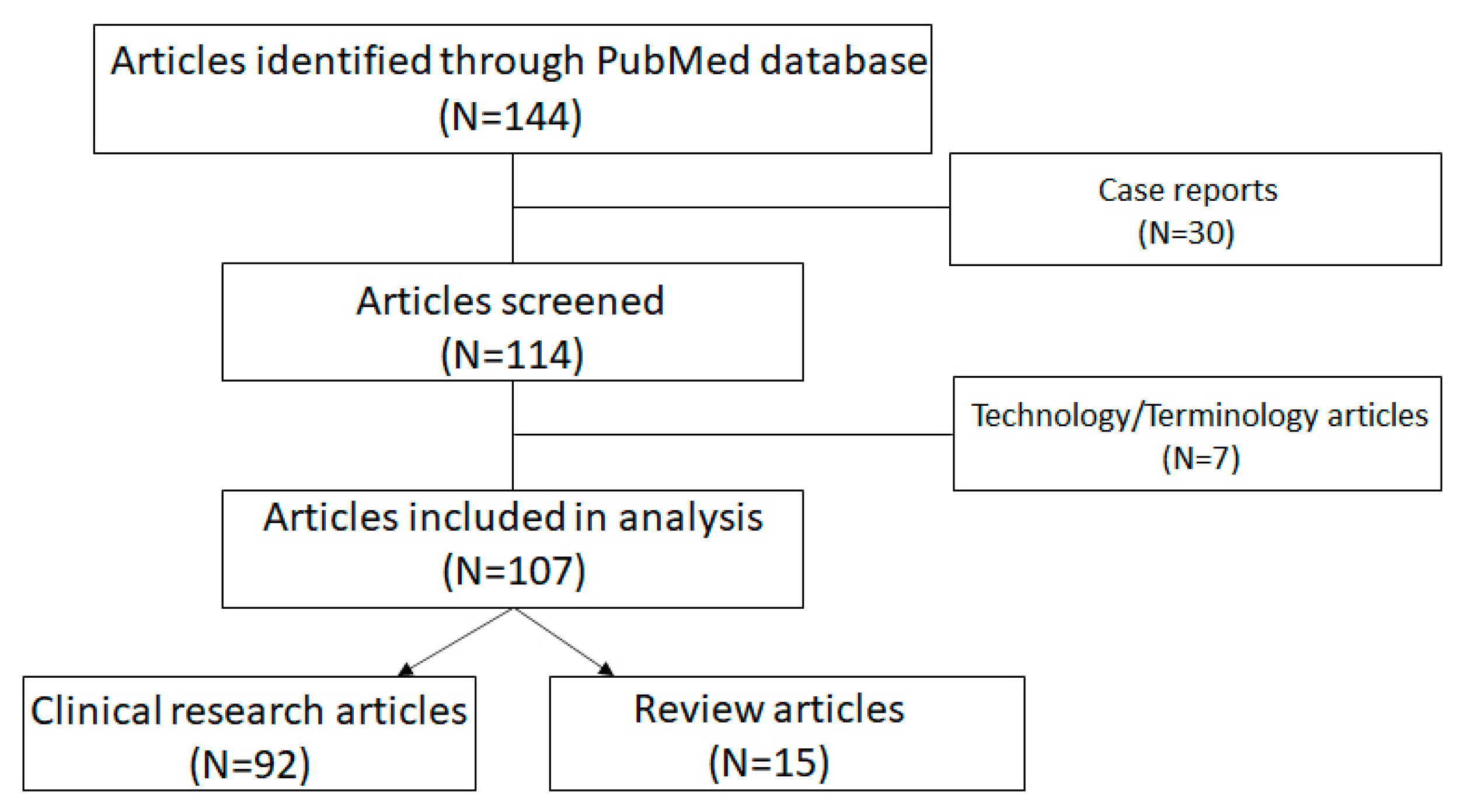
3. Methods
4. Results
4.1. Number of Articles (2016–2022)
4.2. Clinical Research Articles
4.3. Review Articles
4.4. Significant Contribution of OCT-A to Uveitis
5. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Novotny, H.R.; Alvis, D.L. A method of photographing fluorescence in circulating blood in the human retina. Circulation 1961, 24, 82–86. [Google Scholar] [CrossRef] [PubMed]
- Herbort, C.P.; LeHoang, P.; Guex-Crosier, Y. Schematic interpretation of indocyanine green angiography in posterior uveitis using a standard angiographic protocol. Ophthalmology 1998, 105, 432–440. [Google Scholar] [CrossRef] [PubMed]
- Altan-Yaycioglu, R.; Akova, Y.A.; Akca, S.; Yilmaz, G. Inflammation of the posterior uvea: Findings on fundus fluorescein and indocyanine green angiography. Ocul. Immunol. Inflamm. 2006, 14, 171–179. [Google Scholar] [CrossRef]
- Fardeau, C.; Tran, T.H.; Gharbi, B.; Cassoux, N.; Bodaghi, B.; LeHoang, P. Retinal fluorescein and indocyanine green angiography and optical coherence tomography in successive stages of Vogt-Koyanagi-Harada disease. Int. Ophthalmol. 2007, 27, 163–172. [Google Scholar] [CrossRef]
- Herbort, C.P. Fluorescein and indocyanine green angiography for uveitis. Middle East Afr. J. Ophthalmol. 2009, 16, 168–187. [Google Scholar] [CrossRef]
- El Ameen, A.; Herbort, C.P. Comparison of Retinal and Choroidal Involvement in Sarcoidosis-related Chorioretinitis Using Fluorescein and Indocyanine Green Angiography. J. Ophthalmic Vis. Res. 2018, 13, 426–432. [Google Scholar] [CrossRef] [PubMed]
- Tugal-Tutkun, I.; Herbort, C.P.; Khairallah, M. Angiography Scoring for Uveitis Working Group (ASUWOG). Scoring of dual fluorescein and ICG inflammatory angiographic signs for the grading of posterior segment inflammation (dual fluorescein and ICG angiographic scoring system for uveitis). Int. Ophthalmol. 2010, 30, 539–552. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, R.; Kaburaki, T.; Yoshida, A.; Takamoto, M.; Miyaji, T.; Yamaguchi, T. Fluorescein Angiography Scoring System Using Ultra-Wide-Field Fluorescein Angiography Versus Standard Fluorescein Angiography in Patients with Sarcoid Uveitis. Ocul. Immunol. Inflamm. 2021, 29, 1398–1402. [Google Scholar] [CrossRef]
- Sadiq, M.A.; Hassan, M.; Afridi, R.; Halim, M.S.; Do, D.V.; Sepah, Y.J.; Nguyen, Q.D.; STOP-UVEITIS Investigators. Posterior segment inflammatory outcomes assessed using fluorescein angiography in the STOP-UVEITIS study. Int. J. Retin. Vitr. 2020, 6, 47. [Google Scholar] [CrossRef]
- Antcliff, R.J.; Stanford, M.R.; Chauhan, D.S.; Graham, E.M.; Spalton, D.J.; Shilling, J.S.; Ffytche, T.J.; Marshall, J. Comparison between optical coherence tomography and fundus fluorescein angiography for the detection of cystoid macular edema in patients with uveitis. Ophthalmology 2000, 107, 593–599. [Google Scholar] [CrossRef]
- Papasavvas, I.; Mantovani, A.; Herbort, C.P., Jr. Acute Posterior Multifocal Placoid Pigment Epitheliopathy (APMPPE): A Comprehensive Approach and Case Series: Systemic Corticosteroid Therapy is Necessary in a Large Proportion of Cases. Medicina 2022, 58, 1070. [Google Scholar] [CrossRef] [PubMed]
- Papasavvas, I.; Herbort, C.P., Jr. Diagnosis and Treatment of Primary Inflammatory Choriocapillaropathies (PICCPs): A Comprehensive Overview. Medicina 2022, 58, 165. [Google Scholar] [CrossRef] [PubMed]
- Zicarelli, F.; Staurenghi, G.; Invernizzi, A. Anterior Segment Optical Coherence Tomography (AS-OCT) Visualization of Anterior Vitritis. Ocul. Immunol. Inflamm 2022, 1–2, ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Spaide, R.F.; Koizumi, H.; Pozzoni, M.C. Enhanced depth imaging spectral-domain optical coherence tomography. Am. J. Ophthalmol. 2008, 146, 496–500, Erratum in Am. J. Ophthalmol. 2009, 148, 325. [Google Scholar] [CrossRef]
- Balci, O.; Gasc, A.; Jeannin, B.; Herbort, C.P., Jr. Enhanced depth imaging is less suited than indocyanine green angiography for close monitoring of primary stromal choroiditis: A pilot report. Int. Ophthalmol. 2017, 37, 737–748. [Google Scholar] [CrossRef]
- Papasavvas, I.; Neri, P.; Mantovani, A.; Herbort, C.P., Jr. Idiopathic multifocal choroiditis (MFC): Aggressive and prolonged therapy with multiple immunosuppressive agents is needed to halt the progression of active disease. An offbeat review and a case series. J. Ophthalmic Inflamm. Infect. 2022, 12, 2. [Google Scholar] [CrossRef]
- Kramer, M.; Priel, E. Fundus autofluorescence imaging in multifocal choroiditis: Beyond the spots. Ocul. Immunol. Inflamm. 2014, 22, 349–355. [Google Scholar] [CrossRef]
- Spaide, R.F.; Fujimoto, J.G.; Waheed, N.K.; Sadda, S.R.; Staurenghi, G. Optical coherence tomography angiography. Prog Retin Eye Res. 2018, 64, 1–55. [Google Scholar] [CrossRef]
- Rocholz, R.; Corvi, F.; Weichsel, J.; Schmidt, S.; Staurenghi, G. OCT Angiography (OCTA) in Retinal Diagnostics. In High Resolution Imaging in Microscopy and Ophthalmology: New Frontiers in Biomedical Optics [Internet]; Bille, J.F., Ed.; Springer: Cham, Switzerland, 2019; Chapter 6. [Google Scholar]
- Reich, M.; Boehringer, D.; Rothaus, K.; Cakir, B.; Bucher, F.; Daniel, M.; Lang, S.J.; Lagrèze, W.A.; Agostini, H.; Lange, C. Swept-source optical coherence tomography angiography alleviates shadowing artifacts caused by subretinal fluid. Int. Ophthalmol. 2020, 40, 2007–2016. [Google Scholar] [CrossRef]
- Ashraf, M.; Sampani, K.; Abu-Qamar, O.; Cavallerano, J.; Silva, P.S.; Aiello, L.P.; Sun, J.K. Optical Coherence Tomography Angiography Projection Artifact Removal: Impact on Capillary Density and Interaction with Diabetic Retinopathy Severity. Transl. Vis. Sci. Technol. 2020, 9, 10. [Google Scholar] [CrossRef]
- Ripa, M.; Motta, L.; Florit, T.; Sahyoun, J.Y.; Matello, V.; Parolini, B. The Role of Widefield and Ultra Widefield Optical Coherence Tomography in the Diagnosis and Management of Vitreoretinal Diseases. Diagnostics 2022, 12, 2247. [Google Scholar] [CrossRef]
- Herbort, C.P., Jr.; Papasavvas, I.; Tugal-Tutkun, I. Benefits and Limitations of OCT-A in the Diagnosis and Follow-Up of Posterior Intraocular Inflammation in Current Clinical Practice: A Valuable Tool or a Deceiver? Diagnostics 2022, 12, 2384. [Google Scholar] [CrossRef] [PubMed]
- Pichi, F.; Sarraf, D.; Morara, M.; Mazumdar, S.; Neri, P.; Gupta, V. Pearls and pitfalls of optical coherence tomography angiography in the multimodal evaluation of uveitis. J. Ophthalmic Inflamm. Infect. 2017, 7, 20. [Google Scholar] [CrossRef]
- Camino, A.; Jia, Y.; Yu, J.; Wang, J.; Liu, L.; Huang, D. Automated detection of shadow artifacts in optical coherence tomography angiography. Biomed. Opt. Express. 2019, 10, 1514–1531. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.C.; Miller, J.B. Optical Coherence Tomography Angiography: Review of Current Technical Aspects and Applications in Chorioretinal Disease. Semin. Ophthalmol. 2019, 34, 211–217. [Google Scholar] [CrossRef]
- Caplash, S.; Kodati, S.; Cheng, S.K.; Akanda, M.; Vitale, S.; Thompson, I.; Gangaputra, S.; Sen, H.N. Repeatability of Optical Coherence Tomography Angiography in Uveitic Eyes. Transl. Vis. Sci. Technol. 2019, 8, 17. [Google Scholar] [CrossRef] [PubMed]
- Pichi, F.; Salas, E.C.; D de Smet, M.; Gupta, V.; Zierhut, M.; Munk, M.R. Standardisation of optical coherence tomography angiography nomenclature in uveitis: First survey results. Br. J. Ophthalmol. 2021, 105, 941–947. [Google Scholar] [CrossRef]
- Pichi, F.; Carreño, E.; Pavesio, C.; Denniston, A.K.; Grewal, D.S.; Deak, G.; Khairallah, M.; Ruiz-Cruz, M.; de Oliveira Dias, J.R.; Adan, A.; et al. Consensus-based recommendations for optical coherence tomography angiography reporting in uveitis. Br. J. Ophthalmol 2022. Online ahead of print. [Google Scholar] [CrossRef]
- Pohlmann, D.; Berlin, M.; Reidl, F.; Künzel, S.E.; Pleyer, U.; Joussen, A.M.; Winterhalter, S. Longitudinal Comparison of Constant Artifacts in Optical Coherence Tomography Angiography in Patients with Posterior Uveitis Compared to Healthy Subjects. J. Clin. Med. 2022, 11, 5376. [Google Scholar] [CrossRef]
- Tang, W.; Guo, J.; Liu, W.; Xu, G. Optical Coherence Tomography Angiography of Inflammatory Choroidal Neovascularization Early Response after Anti-VEGF Treatment. Curr. Eye Res. 2020, 45, 1556–1562. [Google Scholar] [CrossRef]
- Kim, E.L.; Thanos, A.; Yonekawa, Y.; Todorich, B.; Wolfe, J.; Randhawa, S.; Faia, L.J. Optical Coherence Tomography Angiography Findings in Punctate Inner Choroidopathy. Ophthalmic Surg. Lasers Imaging Retina. 2017, 48, 786–792. [Google Scholar] [CrossRef]
- Perente, A.; Kotsiliti, D.; Taliantzis, S.; Panagiotopoulou, E.K.; Gkika, M.; Perente, I.; Dardabounis, D.; Labiris, G. Serpiginous Choroiditis Complicated with Choroidal Neovascular Membrane Detected using Optical Coherence Tomography Angiography: A Case Series and Literature Review. Turk. J. Ophthalmol. 2021, 51, 326–333. [Google Scholar] [CrossRef]
- Kongwattananon, W.; Grasic, D.; Lin, H.; Oyeniran, E.; Sen, H.N.; Kodati, S. Role of optical coherence tomography angiography in detecting and monitoring inflammatory choroidal neovascularization. Retina 2022, 42, 1047–1056. [Google Scholar] [CrossRef]
- Arias, J.D.; Parra, M.M.; Arango, F.J.; Hoyos, A.T.; Rangel, C.M.; Sánchez-Ávila, R.M. Differentiation of Features of Inflammatory Neovascular Membrane Versus Active Posterior Uveitis by SS-OCTA. Ophthalmic Surg. Lasers Imaging Retina. 2021, 52, 129–137. [Google Scholar] [CrossRef]
- Levison, A.L.; Baynes, K.M.; Lowder, C.Y.; Kaiser, P.K.; Srivastava, S.K. Choroidal neovascularisation on optical coherence tomography angiography in punctate inner choroidopathy and multifocal choroiditis. Br. J. Ophthalmol. 2017, 101, 616–622. [Google Scholar] [CrossRef]
- Dutheil, C.; Korobelnik, J.F.; Delyfer, M.N.; Rougier, M.B. Optical coherence tomography angiography and choroidal neovascularization in multifocal choroiditis: A descriptive study. Eur. J. Ophthalmol. 2018, 28, 614–621. [Google Scholar] [CrossRef]
- Astroz, P.; Miere, A.; Mrejen, S.; Sekfali, R.; Souied, E.H.; Jung, C.; Nghiem-Buffet, S.; Cohen, S.Y. Optical coherence tomography angiography to distinguish choroidal neovascularization from macular inflammatory lesions in multifocal choroiditis. Retina 2018, 38, 299–309. [Google Scholar] [CrossRef]
- Gan, Y.; Zhang, X.; Su, Y.; Shen, M.; Peng, Y.; Wen, F. OCTA versus dye angiography for the diagnosis and evaluation of neovascularisation in punctate inner choroidopathy. Br. J. Ophthalmol. 2022, 106, 547–552. [Google Scholar] [CrossRef]
- Pichi, F.; Hay, S. Use of optical coherence tomography angiography in the uveitis clinic. Graefes Arch. Clin. Exp. Ophthalmol. 2022, 261, 23–36. [Google Scholar] [CrossRef]
- Invernizzi, A.; Carreño, E.; Pichi, F.; Munk, M.R.; Agarwal, A.; Zierhut, M.; Pavesio, C. Experts Opinion: OCTA vs. FFA/ICG in Uveitis-Which Will Survive? Ocul. Immunol. Inflamm 2022, 1–8, ahead of print. [Google Scholar] [CrossRef]
- Tian, M.; Zeng, G.; Tappeiner, C.; Zinkernagel, M.S.; Wolf, S.; Munk, M.R. Comparison of Indocyanine Green Angiography and Swept-Source Wide-Field Optical Coherence Tomography Angiography in Posterior Uveitis. Front. Med. 2022, 9, 853315. [Google Scholar] [CrossRef] [PubMed]
- Mebsout-Pallado, C.; Orès, R.; Terrada, C.; Dansingani, K.K.; Chhablani, J.; Eller, A.W.; Martel, J.N.; Anetakis, A.; Harwick, J.C.; Waxman, E.L.; et al. Review of the Current Literature and Our Experience on the Value of OCT-angiography in White Dot Syndromes. Ocul. Immunol. Inflamm. 2022, 30, 364–378. [Google Scholar] [CrossRef] [PubMed]
- Invernizzi, A.; Pellegrini, M.; Cornish, E.; Yi Chong Teo, K.; Cereda, M.; Chabblani, J. Imaging the Choroid: From Indocyanine Green Angiography to Optical Coherence Tomography Angiography. Asia Pac. J. Ophthalmol. 2020, 9, 335–348. [Google Scholar] [CrossRef]
- Tranos, P.; Karasavvidou, E.M.; Gkorou, O.; Pavesio, C. Optical coherence tomography angiography in uveitis. J. Ophthalmic Inflamm. Infect. 2019, 9, 21. [Google Scholar] [CrossRef]
- Dingerkus, V.L.S.; Munk, M.R.; Brinkmann, M.P.; Freiberg, F.J.; Heussen, F.M.A.; Kinzl, S.; Lortz, S.; Orgül, S.; Becker, M. Optical coherence tomography angiography (OCTA) as a new diagnostic tool in uveitis. J. Ophthalmic Inflamm. Infect. 2019, 9, 10. [Google Scholar] [CrossRef]
- Invernizzi, A.; Cozzi, M.; Staurenghi, G. Optical coherence tomography and optical coherence tomography angiography in uveitis: A review. Clin. Exp. Ophthalmol. 2019, 47, 357–371. [Google Scholar] [CrossRef]
- Kashani, A.H.; Chen, C.L.; Gahm, J.K.; Zheng, F.; Richter, G.M.; Rosenfeld, P.J.; Shi, Y.; Wang, R.K. Optical coherence tomography angiography: A comprehensive review of current methods and clinical applications. Prog. Retin. Eye Res. 2017, 60, 66–100. [Google Scholar] [CrossRef]
- Pichi, F.; Sarraf, D.; Arepalli, S.; Lowder, C.Y.; Cunningham, E.T., Jr.; Neri, P.; Albini, T.A.; Gupta, V.; Baynes, K.; Srivastava, S.K. The application of optical coherence tomography angiography in uveitis and inflammatory eye diseases. Prog. Retin. Eye Res. 2017, 59, 178–201. [Google Scholar] [CrossRef]
- Smid, L.M.; Vermeer, K.A.; Missotten, T.O.A.R.; van Laar, J.A.M.; van Velthoven, M.E.J. Parafoveal Microvascular Alterations in Ocular and Non-Ocular Behçet’s Disease Evaluated With Optical Coherence Tomography Angiography. Investig. Ophthalmol. Vis. Sci. 2021, 62, 8. [Google Scholar] [CrossRef]
- Furino, C.; Shalchi, Z.; Grassi, M.O.; Cardoso, J.N.; Keane, P.A.; Niro, A.; Cicinelli, M.V.; Reibaldi, M.; Boscia, F.; Alessio, G.; et al. OCT Angiography in Acute Posterior Multifocal Placoid Pigment Epitheliopathy. Ophthalmic Surg. Lasers Imaging Retin. 2019, 50, 428–436. [Google Scholar] [CrossRef]
- Papasavvas, I.; Mantovani, A.; Tugal-Tutkun, I.; Herbort, C.P., Jr. Multiple evanescent white dot syndrome (MEWDS): Update on practical appraisal, diagnosis and clinicopathology; a review and an alternative comprehensive perspective. J. Ophthalmic Inflamm. Infect. 2021, 11, 45. [Google Scholar] [CrossRef] [PubMed]
- Abucham-Neto, J.Z.; Torricelli, A.A.M.; Lui, A.C.F.; Guimarães, S.N.; Nascimento, H.; Regatieri, C.V. Comparison between optical coherence tomography angiography and fluorescein angiography findings in retinal vasculitis. Int. J. Retin. Vitr. 2018, 4, 15. [Google Scholar] [CrossRef] [PubMed]
- Usui, Y.; Goto, H. Granuloma-like formation in deeper retinal plexus in ocular sarcoidosis. Clin. Ophthalmol. 2019, 13, 895–896. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Fluorescein Angiography | ICG Angiography | OCT-Angiography |
|---|---|---|
| Invasive | Invasive | Non-invasive |
| Widefield analysis | Widefield analysis | Current technology offers limited field of view in commercially available machines |
| Kinetic analysis of blood flow and flow of liquids | Kinetic analysis of blood flow and flow of liquids | Static blood vessel imaging (sufficient flow necessary to detect vessels) |
| Information on the retina (choriocapillaris on the first 40–60 s) | Information on the choroid (some vascular information about the retina) | Information on the retina and choriocapillaris |
| Side effect from dye (rare) | Side effect from dye (very rare) | No dye needed |
| Non-repeatable at short interval, ±10 min exam duration | Non-repeatable at short interval, ±30 min exam duration | Repeatable, <5 min capture |
| Should be avoided in pregnancy or renal dysfunction (or performed with caution) | Should be avoided in pregnancy or hepatic dysfunction (or performed with caution) | No limitations |
| Information on retinal vascular leakage | Information on choroidal vascular leakage | No information on vascular leakage |
| Information on active iCNV | Information on active iCNV | Detection of iCNV (distinction between active/non-active not always available) |
| Dual FA/ICGA ➔ Global information on all inflammatory diseases two-dimensional | Dual FA/ICGA ➔ Global information on all inflammatory diseases two-dimensional | Limited information on limited disease entities three-dimensional |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Herbort, C.P., Jr.; Takeuchi, M.; Papasavvas, I.; Tugal-Tutkun, I.; Hedayatfar, A.; Usui, Y.; Ozdal, P.C.; Urzua, C.A. Optical Coherence Tomography Angiography (OCT-A) in Uveitis: A Literature Review and a Reassessment of Its Real Role. Diagnostics 2023, 13, 601. https://doi.org/10.3390/diagnostics13040601
Herbort CP Jr., Takeuchi M, Papasavvas I, Tugal-Tutkun I, Hedayatfar A, Usui Y, Ozdal PC, Urzua CA. Optical Coherence Tomography Angiography (OCT-A) in Uveitis: A Literature Review and a Reassessment of Its Real Role. Diagnostics. 2023; 13(4):601. https://doi.org/10.3390/diagnostics13040601
Chicago/Turabian StyleHerbort, Carl P., Jr., Masaru Takeuchi, Ioannis Papasavvas, Ilknur Tugal-Tutkun, Alireza Hedayatfar, Yoshihiko Usui, Pinar C. Ozdal, and Cristhian A. Urzua. 2023. "Optical Coherence Tomography Angiography (OCT-A) in Uveitis: A Literature Review and a Reassessment of Its Real Role" Diagnostics 13, no. 4: 601. https://doi.org/10.3390/diagnostics13040601