
Potential Role of PSMA-Targeted PET in Thyroid Malignant Disease: A Systematic Review
 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol
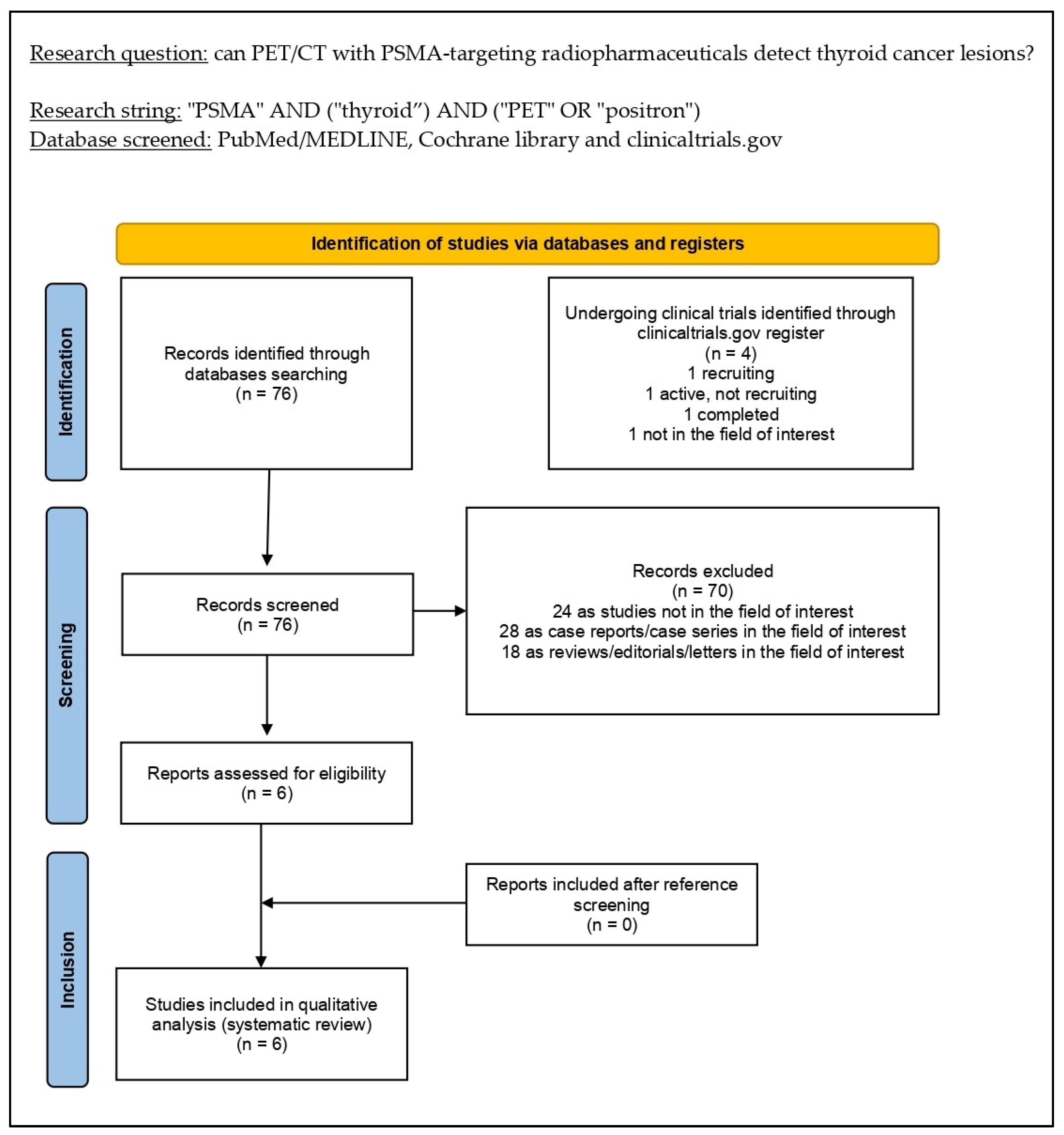
2.2. Literature Search Strategy and Information Sources
2.3. Eligibility Criteria
2.4. Selection Process
2.5. Data Collection Process and Data Extraction
2.6. Quality Assessment (Risk of Bias Assessment)
3. Results
3.1. Literature Search and Study Selection
3.2. Study Characteristics
3.3. Risk of Bias and Applicability
3.4. Results of Individual Studies (Qualitative Synthesis)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McLeod, D.S.A.; Zhang, L.; Durante, C.; Cooper, D.S. Contemporary Debates in Adult Papillary Thyroid Cancer Management. Endocr. Rev. 2019, 40, 1481–1499. [Google Scholar] [CrossRef] [PubMed]
- Enewold, L.; Zhu, K.; Ron, E.; Marrogi, A.J.; Stojadinovic, A.; Peoples, G.E.; Devesa, S.S. Rising thyroid cancer incidence in the United States by demographic and tumor characteristics, 1980–2005. Cancer Epidemiol. Biomark. Prev. 2009, 18, 784–791. [Google Scholar] [CrossRef]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [PubMed]
- Fugazzola, L.; Elisei, R.; Fuhrer, D.; Jarzab, B.; Leboulleux, S.; Newbold, K.; Smit, J. 2019 European Thyroid Association Guidelines for the Treatment and Follow-Up of Advanced Radioiodine-Refractory Thyroid Cancer. Eur. Thyroid J. 2019, 8, 227–245. [Google Scholar] [CrossRef] [PubMed]
- Tuttle, R.M.; Ahuja, S.; Avram, A.M.; Bernet, V.J.; Bourguet, P.; Daniels, G.H.; Dillehay, G.; Draganescu, C.; Flux, G.; Führer, D.; et al. Controversies, Consensus, and Collaboration in the Use of 131I Therapy in Differentiated Thyroid Cancer: A Joint Statement from the American Thyroid Association, the European Association of Nuclear Medicine, the Society of Nuclear Medicine and Molecular Imaging, and the European Thyroid Association. Thyroid 2019, 29, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Treglia, G.; Goichot, B.; Giovanella, L.; Hindié, E.; Jha, A.; Pacak, K.; Taïeb, D.; Walter, T.; Imperiale, A. Prognostic and predictive value of nuclear imaging in endocrine oncology. Endocrine 2020, 67, 9–19. [Google Scholar] [CrossRef]
- Piccardo, A.; Trimboli, P.; Foppiani, L.; Treglia, G.; Ferrarazzo, G.; Massollo, M.; Bottoni, G.; Giovanella, L. PET/CT in thyroid nodule and differentiated thyroid cancer patients. The evidence-based state of the art. Rev. Endocr. Metab. Disord. 2019, 20, 47–64. [Google Scholar] [CrossRef]
- Israeli, R.S.; Powell, C.T.; Fair, W.R.; Heston, W.D. Molecular cloning of a complementary DNA encoding a prostate-specific membrane antigen. Cancer Res. 1993, 53, 227–230. [Google Scholar]
- Horoszewicz, J.S.; Kawinski, E.; Murphy, G.P. Monoclonal antibodies to a new antigenic marker in epithelial prostatic cells and serum of prostatic cancer patients. Anticancer. Res. 1987, 7, 927–935. [Google Scholar]
- Sartor, O.; de Bono, J.; Chi, K.N.; Fizazi, K.; Herrmann, K.; Rahbar, K.; Tagawa, S.T.; Nordquist, L.T.; Vaishampayan, N.; El-Haddad, G.; et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2021, 385, 1091–1103. [Google Scholar] [CrossRef] [PubMed]
- Jadvar, H.; Calais, J.; Fanti, S.; Feng, F.; Greene, K.L.; Gulley, J.L.; Hofman, M.; Koontz, B.F.; Lin, D.W.; Morris, M.J.; et al. Appropriate Use Criteria for Prostate-Specific Membrane Antigen PET Imaging. J. Nucl. Med. 2022, 63, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Wester, H.-J.; Schottelius, M. PSMA-Targeted Radiopharmaceuticals for Imaging and Therapy. Semin. Nucl. Med. 2019, 49, 302–312. [Google Scholar] [CrossRef]
- Sadeghi, R.; Treglia, G. Systematic reviews and meta-analyses of diagnostic studies: A practical guideline. Clin. Transl. Imaging 2017, 5, 83–87. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Whiting Penny, F.; Rutjes Anne, W.S.; Westwood Marie, E.; Mallett Susan, D.J.J.; Reitsma Johannes, B.; Lee ang Mariska, M.G.; Bossuyt Patrick, M.M. QUADAS-2: A Revised Tool for the Quality Assessment of Diagnostic Accuracy Studies. Ann. Intern. Med. 2011, 155, 529–536. Available online: https://www.acpjournals.org/doi/10.7326/0003-4819-155-8-201110180-00009 (accessed on 21 August 2022). [CrossRef]
- Lütje, S.; Gomez, B.; Cohnen, J.; Umutlu, L.; Gotthardt, M.; Poeppel, T.D.; Bockisch, A.; Rosenbaum-Krumme, S. Imaging of Prostate-Specific Membrane Antigen Expression in Metastatic Differentiated Thyroid Cancer Using 68Ga-HBED-CC-PSMA PET/CT. Clin. Nucl. Med. 2017, 42, 20–25. [Google Scholar] [CrossRef]
- de Vries, L.H.; Lodewijk, L.; Braat, A.J.A.T.; Krijger, G.C.; Valk, G.D.; Lam, M.G.E.H.; Borel Rinkes, I.H.M.; Vriens, M.R.; de Keizer, B. 68Ga-PSMA PET/CT in radioactive iodine-refractory differentiated thyroid cancer and first treatment results with 177Lu-PSMA-617. EJNMMI Res. 2020, 10, 18. [Google Scholar] [CrossRef]
- Lawhn-Heath, C.; Yom, S.S.; Liu, C.; Villanueva-Meyer, J.E.; Aslam, M.; Smith, R.; Narwal, M.; Juarez, R.; Behr, S.C.; Pampaloni, M.H.; et al. Gallium-68 prostate-specific membrane antigen ([68Ga]Ga-PSMA-11) PET for imaging of thyroid cancer: A feasibility study. EJNMMI Res. 2020, 10, 128. [Google Scholar] [CrossRef]
- Verma, P.; Malhotra, G.; Meshram, V.; Chandak, A.; Sonavane, S.; Lila, A.R.; Bandgar, T.R.; Asopa, R.V. Prostate-Specific Membrane Antigen Expression in Patients With Differentiated Thyroid Cancer With Thyroglobulin Elevation and Negative Iodine Scintigraphy Using 68Ga-PSMA-HBED-CC PET/CT. Clin. Nucl. Med. 2021, 46, e406–e409. [Google Scholar] [CrossRef]
- Pitalua-Cortes, Q.; García-Perez, F.O.; Vargas-Ahumada, J.; Gonzalez-Rueda, S.; Gomez-Argumosa, E.; Ignacio-Alvarez, E.; Soldevilla-Gallardo, I.; Torres-Agredo, L. Head-to-Head Comparison of 68Ga-PSMA-11 and 131I in the Follow-Up of Well-Differentiated Metastatic Thyroid Cancer: A New Potential Theragnostic Agent. Front. Endocrinol. 2021, 12, 794759. [Google Scholar] [CrossRef] [PubMed]
- Wächter, S.; Di Fazio, P.; Maurer, E.; Manoharan, J.; Keber, C.; Pfestroff, A.; Librizzi, D.; Bartsch, D.K.; Luster, M.; Eilsberger, F. Prostate-Specific Membrane Antigen in Anaplastic and Poorly Differentiated Thyroid Cancer—A New Diagnostic and Therapeutic Target? Cancers 2021, 13, 5688. [Google Scholar] [CrossRef] [PubMed]
- Farolfi, A.; Fendler, W.; Iravani, A.; Haberkorn, U.; Hicks, R.; Herrmann, K.; Walz, J.; Fanti, S. Theranostics for Advanced Prostate Cancer: Current Indications and Future Developments. Eur. Urol. Oncol. 2019, 2, 152–162. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, A.; Dall’Armellina, S.; Pizzuto, D.A.; Perotti, G.; Zagaria, L.; Lanni, V.; Treglia, G.; Racca, M.; Annunziata, S. PSMA Radioligand Uptake as a Biomarker of Neoangiogenesis in Solid Tumours: Diagnostic or Theragnostic Factor? Cancers 2022, 14, 4039. [Google Scholar] [CrossRef]
- Moore, M.; Panjwani, S.; Mathew, R.; Crowley, M.; Liu, Y.-F.; Aronova, A.; Finnerty, B.; Zarnegar, R.; Fahey, T.J.; Scognamiglio, T. Well-Differentiated Thyroid Cancer Neovasculature Expresses Prostate-Specific Membrane Antigen-a Possible Novel Therapeutic Target. Endocr. Pathol. 2017, 28, 339–344. [Google Scholar] [CrossRef]
- Sollini, M.; di Tommaso, L.; Kirienko, M.; Piombo, C.; Erreni, M.; Lania, A.G.; Chiti, A. PSMA expression level predicts differentiated thyroid cancer aggressiveness and patient outcome. EJNMMI Res. 2019, 9, 93. [Google Scholar] [CrossRef]
- Heitkötter, B.; Steinestel, K.; Trautmann, M.; Grünewald, I.; Barth, P.; Gevensleben, H.; Bögemann, M.; Wardelmann, E.; Hartmann, W.; Rahbar, K.; et al. Neovascular PSMA expression is a common feature in malignant neoplasms of the thyroid. Oncotarget 2018, 9, 9867–9874. [Google Scholar] [CrossRef]
- Herrmann, G.; Schumm-Draeger, P.M.; Müller, C.; Atai, E.; Wenzel, B.; Fabian, T.; Usadel, K.H.; Hübner, K. T lymphocytes, CD68-positive cells and vascularisation in thyroid carcinomas. J. Cancer Res. Clin. Oncol. 1994, 120, 651–656. [Google Scholar] [CrossRef]
- Godê, K.K.S.; Mourato, F.A.; Sales, A.F.d.F.; de Almeida Filho, P.J.; Brandão, S.C.S.; Wichert-Ana, L. Thyroid incidentalomas in PSMA PET/CT: A systematic review and meta-analysis. Clin. Transl. Imaging 2022. [Google Scholar] [CrossRef]
- Bertagna, F.; Albano, D.; Giovanella, L.; Bonacina, M.; Durmo, R.; Giubbini, R.; Treglia, G. 68Ga-PSMA PET thyroid incidentalomas. Hormones 2019, 18, 145–149. [Google Scholar] [CrossRef]
- Bychkov, A.; Vutrapongwatana, U.; Tepmongkol, S.; Keelawat, S. PSMA expression by microvasculature of thyroid tumors—Potential implications for PSMA theranostics. Sci. Rep. 2017, 7, 5202. [Google Scholar] [CrossRef] [PubMed]
- Gossili, F.; Petersen, L.J.; Zacho, H.D. The frequency of thyroid incidental findings and risk of malignancy detected by 68Ga-labeled prostate-specific membrane antigen PET/CT in prostate cancer. Hell. J. Nucl. Med. 2020, 23, 240–245. [Google Scholar] [CrossRef]
- Boellaard, R.; Delgado-Bolton, R.; Oyen, W.J.G.; Giammarile, F.; Tatsch, K.; Eschner, W.; Verzijlbergen, F.J.; Barrington, S.F.; Pike, L.C.; Weber, W.A.; et al. FDG PET/CT: EANM procedure guidelines for tumour imaging: Version 2.0. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 328–354. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, A.; Racca, M.; Dall’Armellina, S.; Rescigno, P.; Banna, G.L.; Albano, D.; Dondi, F.; Bertagna, F.; Annunziata, S.; Treglia, G. The Emerging Role of PET/CT with PSMA-Targeting Radiopharmaceuticals in Clear Cell Renal Cancer: An Updated Systematic Review. Cancers 2023, 15, 355. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, A.; Racca, M.; Albano, D.; Dondi, F.; Bertagna, F.; Annunziata, S.; Treglia, G. Can PSMA-Targeting Radiopharmaceuticals Be Useful for Detecting Hepatocellular Carcinoma Using Positron Emission Tomography? An Updated Systematic Review and Meta-Analysis. Pharmaceuticals 2022, 15, 1368. [Google Scholar] [CrossRef]
- Muoio, B.; Albano, D.; Dondi, F.; Bertagna, F.; Garibotto, V.; Kunikowska, J.; Piccardo, A.; Annunziata, S.; Espeli, V.; Migliorini, D.; et al. Diagnostic Accuracy of PET/CT or PET/MRI Using PSMA-Targeting Radiopharmaceuticals in High-Grade Gliomas: A Systematic Review and a Bivariate Meta-Analysis. Diagnostics 2022, 12, 1665. [Google Scholar] [CrossRef]
- Cabanillas, M.E.; Ryder, M.; Jimenez, C. Targeted Therapy for Advanced Thyroid Cancer: Kinase Inhibitors and Beyond. Endocr. Rev. 2019, 40, 1573–1604. [Google Scholar] [CrossRef]
- Haddad, R.I.; Nasr, C.; Bischoff, L.; Busaidy, N.L.; Byrd, D.; Callender, G.; Dickson, P.; Duh, Q.-Y.; Ehya, H.; Goldner, W.; et al. NCCN Guidelines Insights: Thyroid Carcinoma, Version 2.2018. J. Natl. Compr. Cancer Netw. 2018, 16, 1429–1440. [Google Scholar] [CrossRef]
- Elia, G.; Patrizio, A.; Ragusa, F.; Paparo, S.R.; Mazzi, V.; Balestri, E.; Botrini, C.; Rugani, L.; Benvenga, S.; Materazzi, G.; et al. Molecular features of aggressive thyroid cancer. Front. Oncol. 2022, 12, 1099280. [Google Scholar] [CrossRef]
- Schlumberger, M.; Tahara, M.; Wirth, L.J.; Robinson, B.; Brose, M.S.; Elisei, R.; Habra, M.A.; Newbold, K.; Shah, M.H.; Hoff, A.O.; et al. Lenvatinib versus placebo in radioiodine-refractory thyroid cancer. N. Engl. J. Med. 2015, 372, 621–630. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Authors [Ref.] | Year | Country | Study Design/Number of Involved Centers | Funding Sources |
|---|---|---|---|---|
| Lütje et al. [17] | 2017 | Germany | Prospective/Monocentric | None declared |
| De Vries et al. [18] | 2020 | The Netherlands | Retrospective/Monocentric | None declared |
| Lawhn-Heath et al. [19] | 2020 | USA | Prospective/Monocentric | Several grants declared |
| Verma et al. [20] | 2021 | India | Prospective/Monocentric | None declared |
| Pitalua-Cortes et al. [21] | 2021 | Mexico | Retrospective/Monocentric | None declared |
| Wächter et al. [22] | 2022 | Germany | Retrospective/Monocentric | Several grants declared |
| Authors [Ref.] | Sample Size | Median Age (Years) | Gender (Male %) | Clinical Setting (No. Patients) | Histopathological TC Subtypes (No. Patients) | Median Thyroglobulin (ng/mL) | Comparative Imaging |
|---|---|---|---|---|---|---|---|
| Lütje et al. [17] | 6 | 72 | n.a. | RI-refractory TC | 2 papillary 4 follicular | 2482 | [18F]F-FDG PET/CT |
| De Vries et al. [18] | 5 | 50 | 20% | RI-refractory TC | 5 papillary | n.a. | [18F]F-FDG PET/CT (4 patients) |
| Lawhn-Heath et al. [19] | 11 | 65 | 45% | RI-refractory TC | 5 papillary 2 follicular 2 Hürtle cell 2 anaplastic | 22 | [18F]F-FDG PET/CT; [123I]I/[131I]I scan |
| Verma et al. [20] | 9 | 49 | 66.6% | RI-refractory TC | 9 papillary | 225 | [18F]F-FDG PET/CT |
| Pitalua-Cortes et al. [21] | 10 | 58 | 20% | RI-refractory TC | 7 papillary 3 follicular | 773 | [131I]I scan |
| Wächter et al. [22] | 8 | 59 | 75% | Anaplastic or dedifferentiated TC | 6 poorly differentiated 2 anaplastic | n.a. | [18F]F-FDG PET/CT |
| Authors [Ref.] | Tracer | Hybrid Imaging | Tomograph | Administered Activity | Uptake Time (Minutes) | Image Analysis |
|---|---|---|---|---|---|---|
| Lütje et al. [17] | [68Ga]Ga-PSMA-11 | PET/CT | Biograph mCT (Siemens®) | Range: 91–93 MBq | 62 ± 7 | Qualitative and semiquantitative (SUVmax and SUVmean) |
| De Vries et al. [18] | [68Ga]Ga-PSMA-11 [177Lu]Lu-PSMA-617 | PET/CT | TruePoint Biograph mCT40 (Siemens®) | Range: 1.5–2 MBq/kg | 60 | Qualitative and semiquantitative (SUVmax) |
| Lawhn-Heath et al. [19] | [68Ga]Ga-PSMA-11 | PET/MRI | Time-of-fight Signa (GE ®) | Median: 207.2 MBq | 73 | Qualitative and semiquantitative (SUVmax) |
| Verma et al. [20] | [68Ga]Ga-PSMA-11 | PET/CT | Unspecified time-of-flight tomograph (Philips ®) | Mean: 83 MBq | 60 | Qualitative and semiquantitative (SUVmax) |
| Pitalua-Cortes et al. [21] | [68Ga]Ga-PSMA-11 | PET/CT | Biograph mCT20 (Siemens®) | Range: 148–185 MBq | 60 | Qualitative and semiquantitative (SUVmax and TBR) |
| Wächter et al. [22] | [68Ga]Ga-PSMA (not further specified) [177Lu]Lu-PSMA-617 | PET/CT | n.a. | Range: 140–212 MBq | 60 | Qualitative and semiquantitative (SUVmax) |
| Authors [Ref.] | Lesions SUVmax | Lesions Site | Detection Rate |
|---|---|---|---|
| Lütje et al. [17] | Range: 3.3–39.7 | local recurrence lymph node bone soft tissue | Per patient: 83.3% |
| De Vries et al. [18] | Range: 0.85–10.56 | lymph nodes lungs liver leptomeningeal | Per patient: 100% |
| Lawhn-Heath et al. [19] | Range: 1.0–27.8 | local recurrence lymph node lungs bone | Per patient: 72.7% Per lesion: 65.1% |
| Verma et al. [20] | Range: 10.1–45.67 | Lungs bone | Per patient: 55% Per lesion: 64% |
| Pitalua-Cortes et al. [21] | Range: 1.8–70.5 | lymph nodes lung bone brain | Per patient: 100% |
| Wächter et al. [22] | Range: 1.3–6.3 | local recurrence lymph node lung bone | Per patient: 25% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rizzo, A.; Racca, M.; Dall’Armellina, S.; Delgado Bolton, R.C.; Albano, D.; Dondi, F.; Bertagna, F.; Annunziata, S.; Treglia, G. Potential Role of PSMA-Targeted PET in Thyroid Malignant Disease: A Systematic Review. Diagnostics 2023, 13, 564. https://doi.org/10.3390/diagnostics13030564
Rizzo A, Racca M, Dall’Armellina S, Delgado Bolton RC, Albano D, Dondi F, Bertagna F, Annunziata S, Treglia G. Potential Role of PSMA-Targeted PET in Thyroid Malignant Disease: A Systematic Review. Diagnostics. 2023; 13(3):564. https://doi.org/10.3390/diagnostics13030564
Chicago/Turabian StyleRizzo, Alessio, Manuela Racca, Sara Dall’Armellina, Roberto C. Delgado Bolton, Domenico Albano, Francesco Dondi, Francesco Bertagna, Salvatore Annunziata, and Giorgio Treglia. 2023. "Potential Role of PSMA-Targeted PET in Thyroid Malignant Disease: A Systematic Review" Diagnostics 13, no. 3: 564. https://doi.org/10.3390/diagnostics13030564