
Brain Tumor at Diagnosis: From Cognition and Behavior to Quality of Life
 and
and 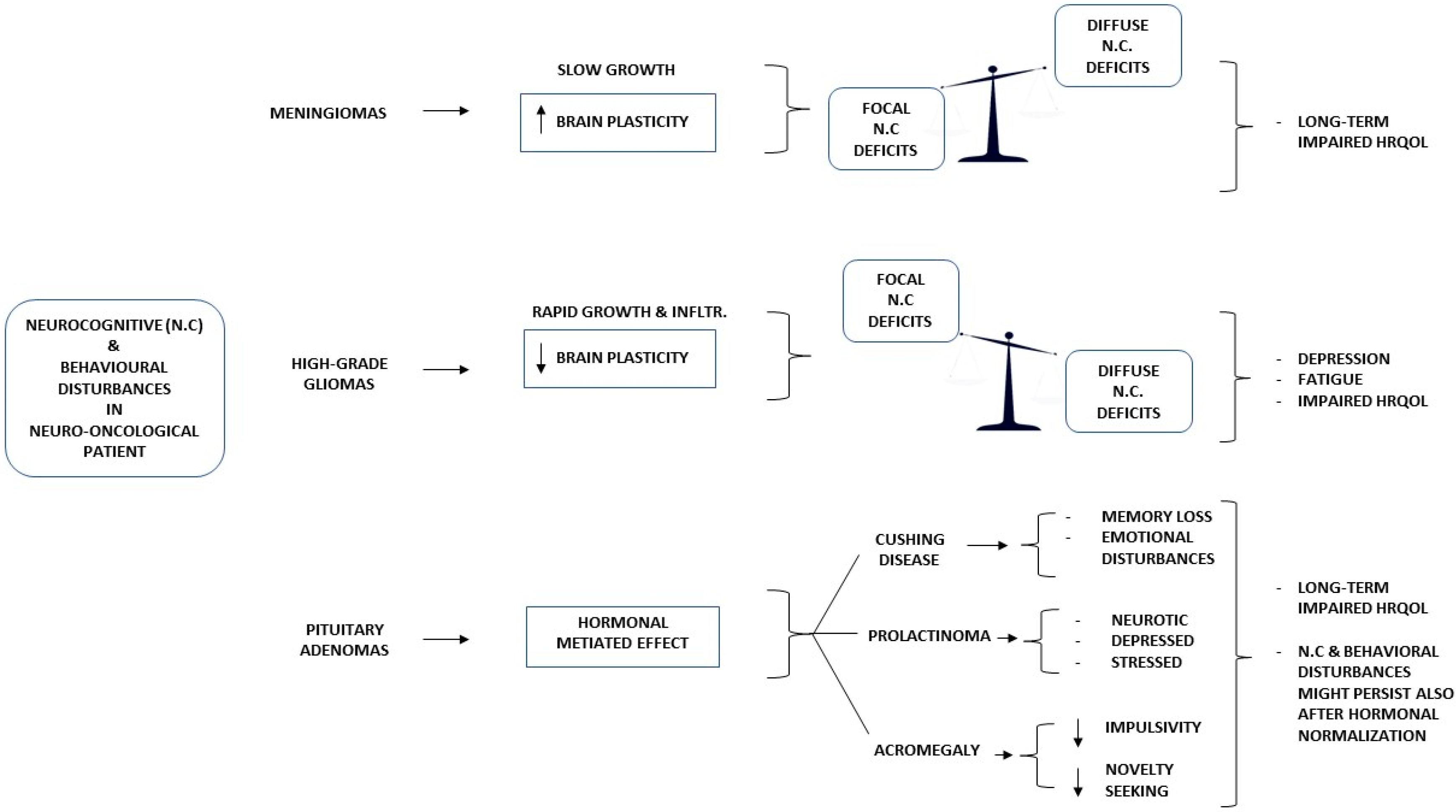{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
3. Symptoms at Diagnosis
4. Meningioma
5. Glioma
6. Pituitary Adenoma
7. Communication of Diagnosis
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.M.; Parney, I.F.; Huang, W.; Anderson, F.A., Jr.; Asher, A.L.; Bernstein, M.; Lillehei, K.O.; Brem, H.; Berger, M.S.; Laws, E.R. Glioma Outcomes Project Investigators. Patterns of care for adults with newly diagnosed malignant glioma. JAMA 2005, 293, 557–564. [Google Scholar] [CrossRef] [PubMed]
- Lageman, S.K.; Cerhan, J.H.; Locke, D.E.; Anderson, S.K.; Wu, W.; Brown, P.D. Comparing neuropsychological tasks to optimize brief cognitive batteries for brain tumor clinical trials. J. Neurooncol. 2010, 96, 271–276. [Google Scholar] [CrossRef] [PubMed]
- Schiavolin, S.; Raggi, A.; Scaratti, C.; Toppo, C.; Silvaggi, F.; Sattin, D.; Broggi, M.; Ferroli, P.; Leonardi, M. Outcome prediction in brain tumor surgery: A literature review on the influence of nonmedical factors. Neurosurg. Rev. 2021, 44, 807–819. [Google Scholar] [CrossRef] [PubMed]
- Bunevicius, A.; Deltuva, V.P.; Tamasauskas, A. Association of pre-operative depressive and anxiety symptoms with five-year survival of glioma and meningioma patients: A prospective cohort study. Oncotarget 2017, 8, 57543–57551. [Google Scholar] [CrossRef]
- Thong, M.S.Y.; van Noorden, C.J.F.; Steindorf, K.; Arndt, V. Cancer-Related Fatigue: Causes and Current Treatment Options. Curr. Treat Options Oncol. 2020, 21, 17. [Google Scholar] [CrossRef]
- van der Linden, S.D.; Gehring, K.; Rutten, G.M.; Kop, W.J.; Sitskoorn, M.M. Prevalence and correlates of fatigue in patients with meningioma before and after surgery. Neurooncol. Pract. 2020, 7, 77–85. [Google Scholar] [CrossRef]
- Cheng, J.X.; Liu, B.L.; Zhang, X.; Lin, W.; Zhang, Y.Q.; Liu, W.P.; Zhang, J.N.; Lin, H.; Wang, R.; Yin, H. Health-related quality of life in glioma patients in China. BMC Cancer 2010, 10, 305. [Google Scholar] [CrossRef]
- Armstrong, T.S.; Vera-Bolanos, E.; Acquaye, A.A.; Gilbert, M.R.; Ladha, H.; Mendoza, T. The symptom burden of primary brain tumors: Evidence for a core set of tumor- and treatment-related symptoms. Neuro Oncol. 2016, 18, 252–260. [Google Scholar] [CrossRef]
- Rockhill, J.; Mrugala, M.; Chamberlain, M.C. Intracranial meningiomas: An overview of diagnosis and treatment. Neurosurg. Focus. 2007, 23, E1. [Google Scholar] [CrossRef]
- Whittle, I.R.; Smith, C.; Navoo, P.; Collie, D. Meningiomas. Lancet 2004, 363, 1535–1543. [Google Scholar] [CrossRef] [PubMed]
- Tucha, O.; Smely, C.; Preier, M.; Becker, G.; Paul, G.M.; Lange, K.W. Preoperative and postoperative cognitive functioning in patients with frontal meningiomas. J. Neurosurg. 2003, 98, 21–31. [Google Scholar] [CrossRef]
- Meskal, I.; Gehring, K.; van der Linden, S.D.; Rutten, G.J.; Sitskoorn, M.M. Cognitive improvement in meningioma patients after surgery: Clinical relevance of computerized testing. J. Neurooncol. 2015, 121, 617–625. [Google Scholar] [CrossRef] [PubMed]
- Yoshii, Y.; Tominaga, D.; Sugimoto, K.; Tsuchida, Y.; Hyodo, A.; Yonaha, H.; Kushi, S. Cognitive function of patients with brain tumor in pre- and postoperative stage. Surg. Neurol. 2008, 69, 51–61. [Google Scholar] [CrossRef] [PubMed]
- Van Nieuwenhuizen, D.; Ambachtsheer, N.; Heimans, J.J.; Reijneveld, J.C.; Peerdeman, S.M.; Klein, M. Neurocognitive functioning and health-related quality of life in patients with radiologically suspected meningiomas. J. Neurooncol. 2013, 113, 433–440. [Google Scholar] [CrossRef]
- Abel, T.J.; Manzel, K.; Bruss, J.; Belfi, A.M.; Howard, M.A., 3rd; Tranel, D. The cognitive and behavioral effects of meningioma lesions involving the ventromedial prefrontal cortex. J. Neurosurg. 2016, 124, 1568–1577. [Google Scholar] [CrossRef]
- Pranckeviciene, A.; Deltuva, V.P.; Tamasauskas, A.; Bunevicius, A. Association between psychological distress, subjective cognitive complaints and objective neuropsychological functioning in brain tumor patients. Clin. Neurol. Neurosurg. 2017, 163, 18–23. [Google Scholar] [CrossRef]
- Van Lonkhuizen, P.J.C.; Rijnen, S.J.M.; van der Linden, S.D.; Rutten, G.M.; Gehring, K.; Sitskoorn, M.M. Subjective cognitive functioning in patients with a meningioma: Its course and association with objective cognitive functioning and psychological symptoms. Psychooncology 2019, 28, 1654–1662. [Google Scholar] [CrossRef]
- Merckelbach, H.; Muris, P.; Nijman, H.; de Jong, P. Self-reported cognitive failures and neurotic symptomatology. Pers. Individ. Differ. 1996, 20, 715–724. [Google Scholar] [CrossRef]
- Zamanipoor Najafabadi, A.H.; Peeters, M.C.M.; Dirven, L.; Lobatto, D.J.; Groen, J.L.; Broekman, M.L.D.; Peerdeman, S.M.; Peul, W.C.; Taphoorn, M.J.B.; van Furth, W.R. Impaired health-related quality of life in meningioma patients-a systematic review. Neuro Oncol. 2017, 19, 897–907. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Feeny, D.H.; Patrick, D.L. Measuring health-related quality of life. Ann. Intern. Med. 1993, 118, 622–629. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Zhang, H.; Wu, J.; Yu, Z.; Chen, X.; Rekik, I.; Wang, Q.; Lu, J.; Shen, D. Overall survival time prediction for high-grade glioma patients based on large-scale brain functional networks. Brain Imaging Behav. 2019, 13, 1333–1351. [Google Scholar] [CrossRef] [PubMed]
- Acevedo-Vergara, K.; Perez-Florez, M.; Ramirez, A.; Torres-Bayona, S.; Dau, A.; Salva, S.; Maloof, D.; Garcia, C.; Luque, M.; Guillen-Burgos, H.F. Cognitive deficits in adult patients with high-grade glioma: A systematic review. Clin. Neurol Neurosurg. 2022, 219, 107296. [Google Scholar] [CrossRef] [PubMed]
- Yu, Z.; Tao, L.; Qian, Z.; Wu, J.; Liu, H.; Yu, Y.; Song, J.; Wang, S.; Sun, J. Altered brain anatomical networks and disturbed connection density in brain tumor patients revealed by diffusion tensor tractography. Int. J. Comput. Assist. Radiol. Surg. 2016, 11, 2007–2019. [Google Scholar] [CrossRef] [PubMed]
- Marin, D.; Madotto, E.; Fabbro, F.; Skrap, M.; Tomasino, B. Design fluency and neuroan-atomical correlates in 54 neurosurgical patients with lesions to the right hemi-sphere. J. Neurooncol. 2017, 135, 141–150. [Google Scholar] [CrossRef]
- Habets, E.J.J.; Hendriks, E.J.; Taphoorn, M.J.B.; Douw, L.; Zwinderman, A.H.; Vandertop, W.P.; Barkhof, F.; De Witt Hamer, P.C.; Klein, M. Association between tumor location and neurocognitive functioning using tumor localization maps. J. Neurooncol. 2019, 144, 573–582. [Google Scholar] [CrossRef]
- Papagno, C.; Casarotti, A.; Comi, A.; Pisoni, A.; Lucchelli, F.; Bizzi, A.; Riva, M.; Bello, L. Long-term proper name anomia after removal of the uncinate fasciculus. Brain Struct Funct. 2016, 221, 687–694. [Google Scholar] [CrossRef]
- Zacharia, T.T.; Eslinger, P.J. Functional MRI activation patterns of cerebellum in patients with epilepsy and brain tumors. Clin. Anat. 2019, 32, 1053–1060. [Google Scholar] [CrossRef]
- Ahmadian, N.; van Baarsen, K.; van Zandvoort, M.; Robe, P.A. The Cerebellar Cognitive Affective Syndrome-a Meta-analysis. Cerebellum 2019, 18, 941–950. [Google Scholar] [CrossRef]
- Schmahmann, J.D.; Sherman, J.C. The cerebellar cognitive affective syndrome. Brain 1998, 121 Pt 4, 561–579. [Google Scholar] [CrossRef]
- Sagberg, L.M.; Iversen, D.H.; Fyllingen, E.H.; Jakola, A.S.; Reinertsen, I.; Solheim, O. Brain atlas for assessing the impact of tumor location on perioperative quality of life in patients with high-grade glioma: A prospective population-based cohort study. Neuroimage Clin. 2019, 21, 101658. [Google Scholar] [CrossRef] [PubMed]
- Mugge, L.; Mansour, T.R.; Crippen, M.; Alam, Y.; Schroeder, J. Depression and glioblastoma, complicated concomitant diseases: A systemic review of published literature. Neurosurg. Rev. 2020, 43, 497–511. [Google Scholar] [CrossRef] [PubMed]
- Bunevicius, A. Personality traits, patient-centered health status and prognosis of brain tumor patients. J. Neurooncol. 2018, 137, 593–600. [Google Scholar] [CrossRef] [PubMed]
- Fabi, A.; Bhargava, R.; Fatigoni, S.; Guglielmo, M.; Horneber, M.; Roila, F.; Weis, J.; Jordan, K.; Ripamonti, C.I. ESMO Guidelines Committee. Electronic address: Clinicalguidelines@esmo.org. Cancer-related fatigue: ESMO Clinical Practice Guidelines for diagnosis and treatment. Ann. Oncol. 2020, 31, 713–723. [Google Scholar] [CrossRef] [PubMed]
- Coomans, M.B.; Dirven, L.; Aaronson, N.K.; Baumert, B.G.; Van Den Bent, M.; Bottomley, A.; Brandes, A.A.; Chinot, O.; Coens, C.; Gorlia, T.; et al. Symptom clusters in newly diagnosed glioma patients: Which symptom clusters are independently associated with functioning and global health status? Neuro Oncol. 2019, 21, 1447–1457. [Google Scholar] [CrossRef] [PubMed]
- Molassiotis, A.; Wilson, B.; Brunton, L.; Chaudhary, H.; Gattamaneni, R.; McBain, C. Symptom experience in patients with primary brain tumours: A longitudinal exploratory study. Eur. J. Oncol. Nurs. 2010, 14, 410–416. [Google Scholar] [CrossRef] [PubMed]
- de Dreu, M.J.; Schouwenaars, I.T.; Rutten, G.J.M.; Ramsey, N.F.; Jansma, J.M. Fatigue in brain tumor patients, towards a neuronal biomarker. Neuroimage Clin. 2020, 28, 102406. [Google Scholar] [CrossRef] [PubMed]
- Röttgering, J.G.; Douw, L.; de Witt Hamer, P.C.; Kouwenhoven, M.C.M.; Würdinger, T.; van de Ven, P.M.; Sharpe, L.; Knoop, H.; Klein, M. Reducing severe fatigue in patients with diffuse glioma: A study protocol for an RCT on the effect of blended cognitive behavioural therapy. Trials 2022, 23, 568. [Google Scholar] [CrossRef]
- Song, L.; Quan, X.; Su, L.; Wang, K.; Wang, H.; Wu, L.; Chen, C.; Li, S.; Xiang, W.; Chen, L.; et al. Inflammation and behavioral symptoms in preoperational glioma patients: Is depression, anxiety, and cognitive impairment related to markers of systemic inflammation? Brain Behav. 2020, 10, e01771. [Google Scholar] [CrossRef]
- Alsumali, A.; Cote, D.J.; Regestein, Q.R.; Crocker, E.; Alzarea, A.; Zaidi, H.A.; Bi, W.L.; Dawood, H.Y.; Broekman, M.L.; van Zandvoort, M.J.E.; et al. The impact of transsphenoidal surgery on neurocognitive function: A systematic review. J. Clin. Neurosci. 2017, 42, 1–6. [Google Scholar] [CrossRef]
- Hendrix, P.; Hans, E.; Griessenauer, C.J.; Simgen, A.; Oertel, J.; Karbach, J. Neurocognitive status in patients with newly-diagnosed brain tumors in good neurological condition: The impact of tumor type, volume, and location. Clin. Neurol Neurosurg. 2017, 156, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Tiemensma, J.; Kaptein, A.A.; Pereira, A.M.; Smit, J.W.; Romijn, J.A.; Biermasz, N.R. Coping strategies in patients after treatment for functioning or nonfunctioning pituitary adenomas. J. Clin. Endocrinol. Metab. 2011, 96, 964–971. [Google Scholar] [CrossRef] [PubMed]
- Pertichetti, M.; Serioli, S.; Belotti, F.; Mattavelli, D.; Schreiber, A.; Cappelli, C.; Padovani, A.; Gasparotti, R.; Nicolai, P.; Fontanella, M.M.; et al. Pituitary adenomas and neuropsychological status: A systematic literature review. Neurosurg Rev. 2020, 43, 1065–1078. [Google Scholar] [CrossRef]
- Wang, X.; Tong, X.; Zou, Y.; Tian, X.; Mao, Z.; Sun, Z. The impact on cognitive functions of patients with pituitary adenoma before and after surgery. Neurol Sci. 2017, 38, 1315–1321. [Google Scholar] [CrossRef]
- Mauri, M.; Sinforiani, E.; Bono, G.; Vignati, F.; Berselli, M.E.; Attanasio, R.; Nappi, G. Memory impairment in Cushing’s disease. Acta Neurol Scand. 1993, 87, 52–55. [Google Scholar] [CrossRef] [PubMed]
- Santos, A.; Resmini, E.; Pascual, J.C.; Crespo, I.; Webb, S.M. Psychiatric Symptoms in Patients with Cushing’s Syndrome: Prevalence, Diagnosis and Management. Drugs 2017, 77, 829–842. [Google Scholar] [CrossRef]
- Feelders, R.A.; Pulgar, S.J.; Kempel, A.; Pereira, A.M. The burden of Cushing’s disease: Clinical and health-related quality of life aspects. Eur. J. Endocrinol. 2012, 167, 311–326. [Google Scholar] [CrossRef]
- Sievers, C.; Ising, M.; Pfister, H.; Dimopoulou, C.; Schneider, H.J.; Roemmler, J.; Schopohl, J.; Stalla, G.K. Personality in patients with pituitary adenomas is characterized by increased anxiety-related traits: Comparison of 70 acromegalic patients with patients with non-functioning pituitary adenomas and age- and gender-matched controls. Eur. J. Endocrinol. 2009, 160, 367–373. [Google Scholar] [CrossRef]
- Wagenmakers, M.A.; Netea-Maier, R.T.; Prins, J.B.; Dekkers, T.; den Heijer, M.; Hermus, A.R. Impaired quality of life in patients in long-term remission of Cushing’s syndrome of both adrenal and pituitary origin: A remaining effect of long-standing hypercortisolism? Eur. J. Endocrinol. 2012, 167, 687–695. [Google Scholar] [CrossRef]
- Pereira, A.M.; Tiemensma, J.; Romijn, J.A. Neuropsychiatric disorders in Cushing’s syndrome. Neuroendocrinology 2010, 92 (Suppl. 1), 65–70. [Google Scholar] [CrossRef]
- Kindratt, T.B.; Atem, F.; Dallo, F.J.; Allicock, M.; Balasubramanian, B.A. The Influence of Patient-Provider Communication on Cancer Screening. J. Patient Exp. 2020, 7, 1648–1657. [Google Scholar] [CrossRef] [PubMed]
- Peterson, E.B.; Ostroff, J.S.; DuHamel, K.N.; D’Agostino, T.A.; Hernandez, M.; Canzona, M.R.; Bylund, C.L. Impact of provider-patient communication on cancer screening adherence: A systematic review. Prev. Med. 2016, 93, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Baccolini, V.; Isonne, C.; Salerno, C.; Giffi, M.; Migliara, G.; Mazzalai, E.; Turatto, F.; Sinopoli, A.; Rosso, A.; De Vito, C.; et al. The association between adherence to cancer screening programs and health literacy: A systematic review and meta-analysis. Prev. Med. 2022, 155, 106927. [Google Scholar] [CrossRef] [PubMed]
- Berkman, N.D.; Davis, T.C.; McCormack, L. Health literacy: What is it? J. Health Commun. 2010, 15 (Suppl. 2), 9–19. [Google Scholar] [CrossRef]
- Papadakos, J.K.; Hasan, S.M.; Barnsley, J.; Berta, W.; Fazelzad, R.; Papadakos, C.J.; Giuliani, M.E.; Howell, D. Health literacy and cancer self-management behaviors: A scoping review. Cancer 2018, 124, 4202–4210. [Google Scholar] [CrossRef]
- Housten, A.J.; Gunn, C.M.; Paasche-Orlow, M.K.; Basen-Engquist, K.M. Health Literacy Interventions in Cancer: A Systematic Review. J. Cancer Educ. 2021, 36, 240–252. [Google Scholar] [CrossRef]
- Hasannejadasl, H.; Roumen, C.; Smit, Y.; Dekker, A.; Fijten, R. Health Literacy and eHealth: Challenges and Strategies. JCO Clin. Cancer Inform. 2022, 6, e2200005. [Google Scholar] [CrossRef]
- Koay, K.; Schofield, P.; Jefford, M. Importance of health literacy in oncology. Asia Pac. J. Clin. Oncol. 2012, 8, 14–23. [Google Scholar] [CrossRef]
- Petersen, G.S.; Laursen, S.G.W.; Jensen, H.; Maindal, H.T.; Pedersen, A.F.; Vedsted, P.; Virgilsen, L.F. Patients’ health literacy is associated with timely diagnosis of cancer-A cross-sectional study in Denmark. Eur. J. Cancer Care 2022, 31, e13532. [Google Scholar] [CrossRef]
- Moore, C.; Hassett, D.; Dunne, S. Health literacy in cancer caregivers: A systematic review. J. Cancer Surviv. 2021, 15, 825–836. [Google Scholar] [CrossRef]
- Buyens, G.; van Balken, M.; Oliver, K.; Price, R.; Venegoni, E.; Lawler, M.; Battisti, N.M.L.; Van Poppel, H. Cancer literacy—Informing patients and implementing shared decision making. J. Cancer Policy 2022, 35, 100375. [Google Scholar] [CrossRef]
- Kim, H.; Goldsmith, J.V.; Sengupta, S.; Mahmood, A.; Powell, M.P.; Bhatt, J.; Chang, C.F.; Bhuyan, S.S. Mobile Health Application and e-Health Literacy: Opportunities and Concerns for Cancer Patients and Caregivers. J. Cancer Educ. 2019, 34, 3–8. [Google Scholar] [CrossRef]
- Chawla, N.; Blanch-Hartigan, D.; Virgo, K.S.; Ekwueme, D.U.; Han, X.; Forsythe, L.; Rodriguez, J.; McNeel, T.S.; Yabroff, K.R. Quality of Patient-Provider Communication Among Cancer Survivors: Findings From a Nationally Representative Sample. J. Oncol. Pract. 2016, 12, e964–e973. [Google Scholar] [CrossRef]
- Lobb, E.A.; Halkett, G.K.; Nowak, A.K. Patient and caregiver perceptions of communication of prognosis in high grade glioma. J. Neurooncol. 2011, 104, 315–322. [Google Scholar] [CrossRef]
- Gilligan, T.; Salmi, L.; Enzinger, A. Patient-Clinician Communication Is a Joint Creation: Working Together Toward Well-Being. Am. Soc. Clin. Oncol. Educ. Book 2018, 38, 532–539. [Google Scholar] [CrossRef]
- Comelli, I.; Lippi, G.; Campana, V.; Servadei, F.; Cervellin, G. Clinical presentation and epidemiology of brain tumors firstly diagnosed in adults in the Emergency Department: A 10-year, single center retrospective study. Ann. Transl. Med. 2017, 5, 269. [Google Scholar] [CrossRef]
- van de Belt, T.H.; Nijmeijer, H.; Grim, D.; Engelen, L.J.L.P.G.; Vreeken, R.; van Gelder, M.M.H.J.; Ter Laan, M. Patient-Specific Actual-Size Three-Dimensional Printed Models for Patient Education in Glioma Treatment: First Experiences. World Neurosurg. 2018, 117, e99–e105. [Google Scholar] [CrossRef]
- Bragard, I.; Razavi, D.; Marchal, S.; Merckaert, I.; Delvaux, N.; Libert, Y.; Reynaert, C.; Boniver, J.; Klastersky, J.; Scalliet, P.; et al. Teaching communication and stress management skills to junior physicians dealing with cancer patients: A Belgian Interuniversity Curriculum. Support Care Cancer 2006, 14, 454–461. [Google Scholar] [CrossRef]
- Ley, A.; Kamp, M.; von Sass, C.; Hänggi, D.; Sabel, M.; Rapp, M. Psychooncological distress in low-grade glioma patients-a monocentric study. Acta Neurochir. 2022, 164, 713–722. [Google Scholar] [CrossRef]
- Hartung, T.J.; Brähler, E.; Faller, H.; Härter, M.; Hinz, A.; Johansen, C.; Keller, M.; Koch, U.; Schulz, H.; Weis, J.; et al. The risk of being depressed is significantly higher in cancer patients than in the general population: Prevalence and severity of depressive symptoms across major cancer types. Eur. J. Cancer 2017, 72, 46–53. [Google Scholar] [CrossRef]
- Adduci, A.; Jankovic, M.; Strazzer, S.; Massimino, M.; Clerici, C.; Poggi, G. Parent-child communication and psychological adjustment in children with a brain tumor. Pediatr. Blood Cancer 2012, 59, 290–294. [Google Scholar] [CrossRef]
- Stein, A.; Dalton, L.; Rapa, E.; Bluebond-Langner, M.; Hanington, L.; Stein, K.F.; Ziebland, S.; Rochat, T.; Harrop, E.; Kelly, B.; et al. Communication with children and adolescents about the diagnosis of their own life-threatening condition. Lancet 2019, 393, 1150–1163. [Google Scholar] [CrossRef]
- The Lancet. Let’s talk with children about life-threatening diseases. Lancet 2019, 393, 1072. [Google Scholar] [CrossRef]
- Back, A.L.; Arnold, R.M.; Baile, W.F.; Fryer-Edwards, K.A.; Alexander, S.C.; Barley, G.E.; Gooley, T.A.; Tulsky, J.A. Efficacy of communication skills training for giving bad news and discussing transitions to palliative care. Arch. Intern. Med. 2007, 167, 453–460. [Google Scholar] [CrossRef]
- Brandes, K.; Butow, P.N.; Tattersall, M.H.; Clayton, J.M.; Davidson, P.M.; Young, J.; Epstein, R.M.; Walczak, A. Advanced cancer patients’ and caregivers’ use of a Question Prompt List. Patient Educ. Couns. 2014, 97, 30–37. [Google Scholar] [CrossRef]
- Sacks, P.; Rahman, M. Epidemiology of Brain Metastases. Neurosurg. Clin. N. Am. 2020, 31, 481–488. [Google Scholar] [CrossRef]
- Mela, A.; Poniatowski, Ł.A.; Drop, B.; Furtak-Niczyporuk, M.; Jaroszyński, J.; Wrona, W.; Staniszewska, A.; Dąbrowski, J.; Czajka, A.; Jagielska, B.; et al. Overview and Analysis of the Cost of Drug Programs in Poland: Public Payer Expenditures and Coverage of Cancer and Non-Neoplastic Diseases Related Drug Therapies from 2015–2018 Years. Front. Pharmacol. 2020, 11, 1123. [Google Scholar] [CrossRef]
- Mela, A.; Rdzanek, E.; Tysarowski, A.; Sakowicz, M.; Jaroszyński, J.; Furtak-Niczyporuk, M.; Żurek, G.; Poniatowski, Ł.A.; Jagielska, B. The impact of changing the funding model for genetic diagnostics and improved access to personalized medicine in oncology. Expert Rev. Pharmacoecon. Outcomes Res. 2023, 23, 43–54. [Google Scholar] [CrossRef]
- Walker, E.V.; Ross, J.; Yuan, Y.; Smith, T.R.; Davis, F.G. Brain cancer survival in Canada 1996–2008: Effects of sociodemographic characteristics. Curr. Oncol. 2019, 26, e292–e299. [Google Scholar] [CrossRef] [Green Version]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chieffo, D.P.R.; Lino, F.; Ferrarese, D.; Belella, D.; Della Pepa, G.M.; Doglietto, F. Brain Tumor at Diagnosis: From Cognition and Behavior to Quality of Life. Diagnostics 2023, 13, 541. https://doi.org/10.3390/diagnostics13030541
Chieffo DPR, Lino F, Ferrarese D, Belella D, Della Pepa GM, Doglietto F. Brain Tumor at Diagnosis: From Cognition and Behavior to Quality of Life. Diagnostics. 2023; 13(3):541. https://doi.org/10.3390/diagnostics13030541
Chicago/Turabian StyleChieffo, Daniela Pia Rosaria, Federica Lino, Daniele Ferrarese, Daniela Belella, Giuseppe Maria Della Pepa, and Francesco Doglietto. 2023. "Brain Tumor at Diagnosis: From Cognition and Behavior to Quality of Life" Diagnostics 13, no. 3: 541. https://doi.org/10.3390/diagnostics13030541