

Incremental Detection Rate of Dysplasia and Sessile Serrated Polyps/Adenomas Using Narrow-Band Imaging and Dye Spray Chromoendoscopy in Addition to High-Definition Endoscopy in Patients with Long-Standing Extensive Ulcerative Colitis: Segmental Tandem Endoscopic Study
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Segmental Tandem Colonoscopy
2.3. Pathologic Interpretation
2.4. Outcome Measures
2.5. Sample Size Calculation
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
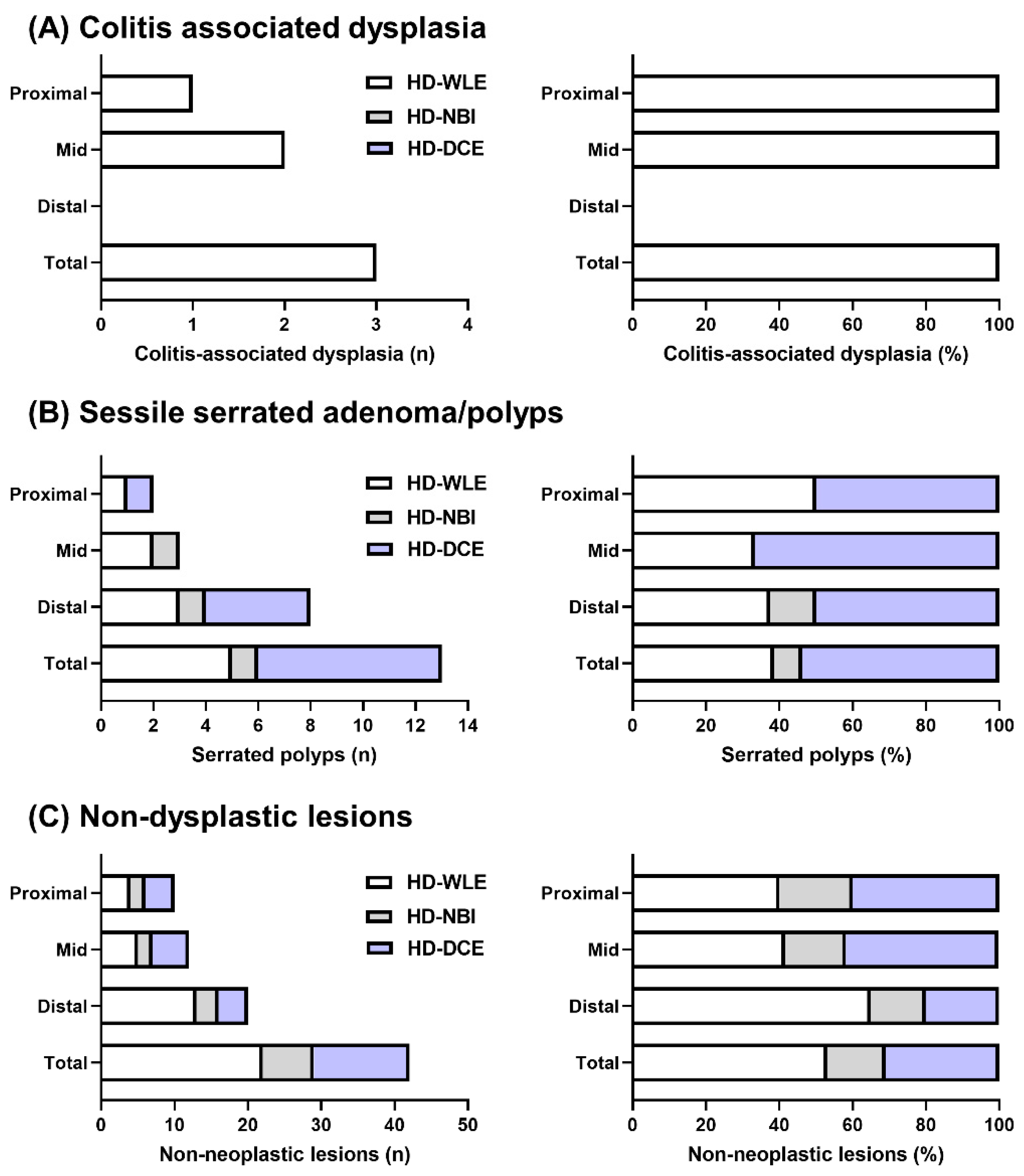
3.2. Per-Polyp Analysis of Dysplasia, SSAs/Ps, and Non-Dysplastic Lesions Detected by HD-WLE, HD-NBI, and HD-DCE
3.3. Per-Patient Analysis of Dysplasia, SSAs/Ps, and Non-Dysplastic Lesions Detected by HD-WLE, HD-NBI, and HD-DCE
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ananthakrishnan, A.N.; Cagan, A.; Cai, T.; Gainer, V.S.; Shaw, S.Y.; Churchill, S.; Karlson, E.W.; Murphy, S.N.; Kohane, I.; Liao, K.P. Colonoscopy is associated with a reduced risk for colon cancer and mortality in patients with inflammatory bowel diseases. Clin. Gastroenterol. Hepatol. 2015, 13, 322–329.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Annese, V.; Beaugerie, L.; Egan, L.; Biancone, L.; Bolling, C.; Brandts, C.; Dierickx, D.; Dummer, R.; Fiorino, G.; Gornet, J.M.; et al. European Evidence-based Consensus: Inflammatory Bowel Disease and Malignancies. J. Crohns. Colitis. 2015, 9, 945–965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shergill, A.K.; Lightdale, J.R.; Bruining, D.H.; Acosta, R.D.; Chandrasekhara, V.; Chathadi, K.V.; Decker, G.A.; Early, D.S.; Evans, J.A.; Fanelli, R.D.; et al. The role of endoscopy in inflammatory bowel disease. Gastrointest. Endosc. 2015, 81, 1101–1121. [Google Scholar] [CrossRef] [PubMed]
- Laine, L.; Kaltenbach, T.; Barkun, A.; McQuaid, K.R.; Subramanian, V.; Soetikno, R. SCENIC international consensus statement on surveillance and management of dysplasia in inflammatory bowel disease. Gastroenterology 2015, 148, 639–651.e28. [Google Scholar] [CrossRef] [PubMed]
- Cairns, S.R.; Scholefield, J.H.; Steele, R.J.; Dunlop, M.G.; Thomas, H.J.; Evans, G.D.; Eaden, J.A.; Rutter, M.D.; Atkin, W.P.; Saunders, B.P.; et al. Guidelines for colorectal cancer screening and surveillance in moderate and high risk groups (update from 2002). Gut 2010, 59, 666–689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamb, C.A.; Kennedy, N.A.; Raine, T.; Hendy, P.A.; Smith, P.J.; Limdi, J.K.; Hayee, B.; Lomer, M.C.E.; Parkes, G.C.; Selinger, C.; et al. British Society of Gastroenterology consensus guidelines on the management of inflammatory bowel disease in adults. Gut 2019, 68, s1–s106. [Google Scholar] [CrossRef] [Green Version]
- Murthy, S.K.; Feuerstein, J.D.; Nguyen, G.C.; Velayos, F.S. AGA Clinical Practice Update on Endoscopic Surveillance and Management of Colorectal Dysplasia in Inflammatory Bowel Diseases: Expert Review. Gastroenterology 2021, 161, 1043–1051.e4. [Google Scholar] [CrossRef]
- Magro, F.; Gionchetti, P.; Eliakim, R.; Ardizzone, S.; Armuzzi, A.; Barreiro-de Acosta, M.; Burisch, J.; Gecse, K.B.; Hart, A.L.; Hindryckx, P.; et al. Third European Evidence-based Consensus on Diagnosis and Management of Ulcerative Colitis. Part 1: Definitions, Diagnosis, Extra-intestinal Manifestations, Pregnancy, Cancer Surveillance, Surgery, and Ileo-anal Pouch Disorders. J. Crohns. Colitis. 2017, 11, 649–670. [Google Scholar] [CrossRef] [Green Version]
- Kiesslich, R. SCENIC update 2021: Is chromoendoscopy still standard of care for inflammatory bowel disease surveillance? Gastrointest. Endosc. 2022, 95, 38–41. [Google Scholar] [CrossRef]
- Santi, G.; Michetti, P.; Froehlich, F.; Rossel, J.B.; Pittet, V.; Maillard, M.H. Adherence to Recommendations and Quality of Endoscopic Colorectal Cancer Surveillance in Long-Standing Ulcerative Colitis. Inflamm. Intest. Dis. 2021, 6, 25–31. [Google Scholar] [CrossRef]
- Shinozaki, M.; Kobayashi, K.; Kunisaki, R.; Hisamatsu, T.; Naganuma, M.; Takahashi, K.I.; Iwao, Y.; Suzuki, Y.; Watanabe, M.; Itabashi, M.; et al. Surveillance for dysplasia in patients with ulcerative colitis: Discrepancy between guidelines and practice. Dig. Endosc. 2017, 29, 584–593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feuerstein, J.D.; Rakowsky, S.; Sattler, L.; Yadav, A.; Foromera, J.; Grossberg, L.; Cheifetz, A.S. Meta-analysis of dye-based chromoendoscopy compared with standard- and high-definition white-light endoscopy in patients with inflammatory bowel disease at increased risk of colon cancer. Gastrointest. Endosc. 2019, 90, 186–195.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parian, A.M.; Lazarev, M.G. Serrated Colorectal Lesions in Patients With Inflammatory Bowel Disease. Gastroenterol. Hepatol. 2018, 14, 19–25. [Google Scholar]
- Hurt, C.; Ramaraj, R.; Farr, A.; Morgan, M.; Williams, N.; Philips, C.J.; Williams, G.T.; Gardner, G.; Porter, C.; Sampson, J.; et al. Feasibility and economic assessment of chromocolonoscopy for detection of proximal serrated neoplasia within a population-based colorectal cancer screening programme (CONSCOP): An open-label, randomised controlled non-inferiority trial. Lancet Gastroenterol. Hepatol. 2019, 4, 364–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, E.J.; Calderwood, A.H.; Doros, G.; Fix, O.K.; Jacobson, B.C. The Boston bowel preparation scale: A valid and reliable instrument for colonoscopy-oriented research. Gastrointest. Endosc. 2009, 69, 620–625. [Google Scholar] [CrossRef] [Green Version]
- Rutgeerts, P.; Sandborn, W.J.; Feagan, B.G.; Reinisch, W.; Olson, A.; Johanns, J.; Travers, S.; Rachmilewitz, D.; Hanauer, S.B.; Lichtenstein, G.R.; et al. Infliximab for induction and maintenance therapy for ulcerative colitis. N. Engl. J. Med. 2005, 353, 2462–2476. [Google Scholar] [CrossRef] [Green Version]
- Rutter, M.; Bernstein, C.; Matsumoto, T.; Kiesslich, R.; Neurath, M. Endoscopic appearance of dysplasia in ulcerative colitis and the role of staining. Endoscopy 2004, 36, 1109–1114. [Google Scholar] [CrossRef]
- Kim, B.H.; Kim, J.M.; Kang, G.H.; Chang, H.J.; Kang, D.W.; Kim, J.H.; Bae, J.M.; Seo, A.N.; Park, H.S.; Kang, Y.K.; et al. Standardized Pathology Report for Colorectal Cancer, 2nd Edition. J. Pathol. Transl. Med. 2020, 54, 1–19. [Google Scholar] [CrossRef] [Green Version]
- WHO Classification of Tumours Editorial Board. WHO Classification of Tumours: Digestive System Tumours, 5th ed.; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Kiesslich, R.; Fritsch, J.; Holtmann, M.; Koehler, H.H.; Stolte, M.; Kanzler, S.; Nafe, B.; Jung, M.; Galle, P.R.; Neurath, M.F. Methylene blue-aided chromoendoscopy for the detection of intraepithelial neoplasia and colon cancer in ulcerative colitis. Gastroenterology 2003, 124, 880–888. [Google Scholar] [CrossRef]
- Rutter, M.D.; Saunders, B.P.; Schofield, G.; Forbes, A.; Price, A.B.; Talbot, I.C. Pancolonic indigo carmine dye spraying for the detection of dysplasia in ulcerative colitis. Gut 2004, 53, 256–260. [Google Scholar] [CrossRef]
- Marion, J.F.; Waye, J.D.; Present, D.H.; Israel, Y.; Bodian, C.; Harpaz, N.; Chapman, M.; Itzkowitz, S.; Steinlauf, A.F.; Abreu, M.T.; et al. Chromoendoscopy-targeted biopsies are superior to standard colonoscopic surveillance for detecting dysplasia in inflammatory bowel disease patients: A prospective endoscopic trial. Am. J. Gastroenterol. 2008, 103, 2342–2349. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, T.; Nakamura, S.; Jo, Y.; Yao, T.; Iida, M. Chromoscopy might improve diagnostic accuracy in cancer surveillance for ulcerative colitis. Am. J. Gastroenterol. 2003, 98, 1827–1833. [Google Scholar] [CrossRef] [PubMed]
- Picco, M.F.; Pasha, S.; Leighton, J.A.; Bruining, D.; Loftus, E.V., Jr.; Thomas, C.S.; Crook, J.E.; Krishna, M.; Wallace, M. Procedure time and the determination of polypoid abnormalities with experience: Implementation of a chromoendoscopy program for surveillance colonoscopy for ulcerative colitis. Inflamm. Bowel. Dis. 2013, 19, 1913–1920. [Google Scholar] [CrossRef]
- Hlavaty, T.; Huorka, M.; Koller, T.; Zita, P.; Kresanova, E.; Rychly, B.; Toth, J. Colorectal cancer screening in patients with ulcerative and Crohn’s colitis with use of colonoscopy, chromoendoscopy and confocal endomicroscopy. Eur. J. Gastroenterol. Hepatol 2011, 23, 680–689. [Google Scholar] [CrossRef] [PubMed]
- Yang, D.H.; Park, S.J.; Kim, H.S.; Park, Y.S.; Park, D.I.; Lee, K.M.; Jung, S.A.; Choi, C.H.; Koo, J.S.; Cheon, J.H.; et al. High-Definition Chromoendoscopy Versus High-Definition White Light Colonoscopy for Neoplasia Surveillance in Ulcerative Colitis: A Randomized Controlled Trial. Am. J. Gastroenterol. 2019, 114, 1642–1648. [Google Scholar] [CrossRef] [PubMed]
- Schønfeldt Troelsen, F.; Sørensen, H.T.; Pedersen, L.; Erichsen, R. Risk of a post-colonoscopy colorectal cancer diagnosis in patients with inflammatory bowel disease: A population-based cohort study. Endoscopy 2021, 53, 1023–1033. [Google Scholar] [CrossRef]
- Matkowskyj, K.A.; Chen, Z.E.; Rao, M.S.; Yang, G.Y. Dysplastic lesions in inflammatory bowel disease: Molecular pathogenesis to morphology. Arch. Pathol. Lab. Med. 2013, 137, 338–350. [Google Scholar] [CrossRef]
- Carballal, S.; Maisterra, S.; López-Serrano, A.; Gimeno-García, A.Z.; Vera, M.I.; Marín-Garbriel, J.C.; Díaz-Tasende, J.; Márquez, L.; Álvarez, M.A.; Hernández, L.; et al. Real-life chromoendoscopy for neoplasia detection and characterisation in long-standing IBD. Gut 2018, 67, 70–78. [Google Scholar] [CrossRef] [Green Version]
- Jackson, W.E.; Achkar, J.P.; Macaron, C.; Lee, L.; Liu, X.; Pai, R.K.; Lopez, R.; Burke, C.A.; Allende, D.S. The Significance of Sessile Serrated Polyps in Inflammatory Bowel Disease. Inflamm. Bowel. Dis. 2016, 22, 2213–2220. [Google Scholar] [CrossRef]
- Ko, H.M.; Harpaz, N.; McBride, R.B.; Cui, M.; Ye, F.; Zhang, D.; Ullman, T.A.; Polydorides, A.D. Serrated colorectal polyps in inflammatory bowel disease. Mod. Pathol. 2015, 28, 1584–1593. [Google Scholar] [CrossRef] [Green Version]
- de Jong, M.E.; Nagtegaal, I.D.; Vos, S.; van der Post, R.S.; van Herwaarden, Y.; Derikx, L.; Hoentjen, F. Increased Colorectal Neoplasia Risk in Patients with Inflammatory Bowel Disease and Serrated Polyps with Dysplasia. Dig. Dis. Sci. 2022, 67, 5647–5656. [Google Scholar] [CrossRef] [PubMed]
- Alexandersson, B.; Hamad, Y.; Andreasson, A.; Rubio, C.A.; Ando, Y.; Tanaka, K.; Ichiya, T.; Rezaie, R.; Schmidt, P.T. High-Definition Chromoendoscopy Superior to High-Definition White-Light Endoscopy in Surveillance of Inflammatory Bowel Diseases in a Randomized Trial. Clin. Gastroenterol. Hepatol. 2020, 18, 2101–2107. [Google Scholar] [CrossRef] [PubMed]
- Shukla, R.; Salem, M.; Hou, J.K. Use and barriers to chromoendoscopy for dysplasia surveillance in inflammatory bowel disease. World J. Gastrointest. Endosc. 2017, 9, 359–367. [Google Scholar] [CrossRef]
- Subramanian, V.; Mannath, J.; Ragunath, K.; Hawkey, C.J. Meta-analysis: The diagnostic yield of chromoendoscopy for detecting dysplasia in patients with colonic inflammatory bowel disease. Aliment. Pharmacol. Ther. 2011, 33, 304–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, S.N.; Choe, W.H.; Lee, J.H.; Kim, S.I.; Kim, J.H.; Lee, T.Y.; Kim, J.H.; Lee, S.Y.; Cheon, Y.K.; Sung, I.K.; et al. Prospective, randomized, back-to-back trial evaluating the usefulness of i-SCAN in screening colonoscopy. Gastrointest. Endosc. 2012, 75, 1011–1021.e2. [Google Scholar] [CrossRef]
- Bisschops, R.; Bessissow, T.; Joseph, J.A.; Baert, F.; Ferrante, M.; Ballet, V.; Willekens, H.; Demedts, I.; Geboes, K.; De Hertogh, G.; et al. Chromoendoscopy versus narrow band imaging in UC: A prospective randomised controlled trial. Gut 2018, 67, 1087–1094. [Google Scholar] [CrossRef]
- Iacucci, M.; Kaplan, G.G.; Panaccione, R.; Akinola, O.; Lethebe, B.C.; Lowerison, M.; Leung, Y.; Novak, K.L.; Seow, C.H.; Urbanski, S.; et al. A Randomized Trial Comparing High Definition Colonoscopy Alone With High Definition Dye Spraying and Electronic Virtual Chromoendoscopy for Detection of Colonic Neoplastic Lesions During IBD Surveillance Colonoscopy. Am. J. Gastroenterol. 2018, 113, 225–234. [Google Scholar] [CrossRef]
- Ullman, T. Surveillance of Inflammatory Bowel Disease. Gastroenterol. Hepatol. 2014, 10, 827–829. [Google Scholar]
- Dekker, E.; van den Broek, F.J.; Reitsma, J.B.; Hardwick, J.C.; Offerhaus, G.J.; van Deventer, S.J.; Hommes, D.W.; Fockens, P. Narrow-band imaging compared with conventional colonoscopy for the detection of dysplasia in patients with longstanding ulcerative colitis. Endoscopy 2007, 39, 216–221. [Google Scholar] [CrossRef]
- Ignjatovic, A.; East, J.E.; Subramanian, V.; Suzuki, N.; Guenther, T.; Palmer, N.; Bassett, P.; Ragunath, K.; Saunders, B.P. Narrow band imaging for detection of dysplasia in colitis: A randomized controlled trial. Am. J. Gastroenterol. 2012, 107, 885–890. [Google Scholar] [CrossRef]
- Pellisé, M.; López-Cerón, M.; Rodríguez de Miguel, C.; Jimeno, M.; Zabalza, M.; Ricart, E.; Aceituno, M.; Fernández-Esparrach, G.; Ginès, A.; Sendino, O.; et al. Narrow-band imaging as an alternative to chromoendoscopy for the detection of dysplasia in long-standing inflammatory bowel disease: A prospective, randomized, crossover study. Gastrointest. Endosc. 2011, 74, 840–848. [Google Scholar] [CrossRef]
- Buchner, A.M. The Role of Chromoendoscopy in Evaluating Colorectal Dysplasia. Gastroenterol. Hepatol. 2017, 13, 336–347. [Google Scholar]
- Tontini, G.E.; Vecchi, M.; Neurath, M.F.; Neumann, H. Review article: Newer optical and digital chromoendoscopy techniques vs. dye-based chromoendoscopy for diagnosis and surveillance in inflammatory bowel disease. Aliment. Pharmacol. Ther. 2013, 38, 1198–1208. [Google Scholar] [CrossRef] [PubMed]
- Imperatore, N.; Castiglione, F.; Testa, A.; De Palma, G.D.; Caporaso, N.; Cassese, G.; Rispo, A. Augmented Endoscopy for Surveillance of Colonic Inflammatory Bowel Disease: Systematic Review With Network Meta-analysis. J. Crohns. Colitis. 2019, 13, 714–724. [Google Scholar] [CrossRef]
- Gabbani, T.; Manetti, N.; Bonanomi, A.G.; Annese, A.L.; Annese, V. New endoscopic imaging techniques in surveillance of inflammatory bowel disease. World J. Gastrointest. Endosc. 2015, 7, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Štefănescu, D.; Pereira, S.P.; Filip, M.M.; Săftoiu, A.; Cazacu, S. Advanced Endoscopic Imaging Techniques for the Study of Colonic Mucosa in Patients with Inflammatory Bowel Disease. Rom. J. Intern. Med. 2016, 54, 11–23. [Google Scholar] [CrossRef] [Green Version]
- Huguet, J.M.; Ferrer-Barceló, L.; Suárez, P.; Sanchez, E.; Prieto, J.D.; Garcia, V.; Sempere, J. Colorectal cancer screening and surveillance in patients with inflammatory bowel disease in 2021. World J. Gastroenterol. 2022, 28, 502–516. [Google Scholar] [CrossRef]
- Buchner, A.M.; Lichtenstein, G.R. Evaluation and Detection of Dysplasia in IBD: The Role of Chromoendoscopy and Enhanced Imaging Techniques. Curr. Treat. Options Gastroenterol. 2016, 14, 73–82. [Google Scholar] [CrossRef] [PubMed]
- van Doorn, S.C.; van der Vlugt, M.; Depla, A.; Wientjes, C.A.; Mallant-Hent, R.C.; Siersema, P.D.; Tytgat, K.; Tuynman, H.; Kuiken, S.D.; Houben, G.; et al. Adenoma detection with Endocuff colonoscopy versus conventional colonoscopy: A multicentre randomised controlled trial. Gut 2017, 66, 438–445. [Google Scholar] [CrossRef]
- Wang, P.; Liu, P.; Glissen Brown, J.R.; Berzin, T.M.; Zhou, G.; Lei, S.; Liu, X.; Li, L.; Xiao, X. Lower Adenoma Miss Rate of Computer-Aided Detection-Assisted Colonoscopy vs Routine White-Light Colonoscopy in a Prospective Tandem Study. Gastroenterology 2020, 159, 1252–1261.e5. [Google Scholar] [CrossRef]
- Wan, J.; Zhang, Q.; Liang, S.H.; Zhong, J.; Li, J.N.; Ran, Z.H.; Zhi, F.C.; Wang, X.D.; Zhang, X.L.; Wen, Z.H.; et al. Chromoendoscopy with targeted biopsies is superior to white-light endoscopy for the long-term follow-up detection of dysplasia in ulcerative colitis patients: A multicenter randomized-controlled trial. Gastroenterol. Rep. 2021, 9, 14–21. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Value | Variables | Value | |
|---|---|---|---|---|
| Age at UC onset, years (mean ± SD) | 44.1 ± 16.3 | UC extension, n (%) | ||
| Age at surveillance, years (mean ± SD) | 58.7 ± 13.5 | Cecum | 5 (15.2) | |
| Male, n (%) | 23 (67) | Transverse colon | 11 (33.3) | |
| Disease duration, years (mean ± SD) | 14.6 ± 5.9 | Hepatic flexure | 3 (9.1) | |
| Partial Mayo score, n (%) | Ascending colon | 14 (42.4) | ||
| 0 | 19 (57.6) | Mayo endoscopic sub-score, n (%) | ||
| 1 | 14 (42.4) | 0 | 15 (45.5) | |
| Hemoglobin, g/dL (mean ± SD) | 14.1 ± 1.3 | 1 | 18 (54.5) | |
| Albumin, g/dL (mean ± SD) | 4.4 ± 0.3 | UCEIS, point (mean ± SD) | 2.1 ± 2.1 | |
| C-reactive protein, mg/dL (mean ± SD) | 0.23 ± 0.5 | Boston bowel preparation scale | 8.9 ± 0.3 | |
| Medication, n (%) | ||||
| 5-Aminosalicylates | 31 (93.9) | Withdrawal time, min (mean ± SD) | ||
| Azathioprine | 11 (33.3) | Proximal colon | HD-WLE | 2.6 ± 0.8 |
| Infliximab | 10 (30.3) | HD-NBI | 2.4 ± 2.0 | |
| Adalimumab | 2 (6.1) | HD-DCE | 3.6 ± 2.6 | |
| Vedolizumab | 3 (9.1) | Mid colon | HD-WLE | 1.9 ± 0.6 |
| Primary sclerosing cholangitis, n (%) | 1 (3.0) | HD-NBI | 2.2 ± 0.7 | |
| CRC history in 1st degree relative, n (%) | 0 | HD-DCE | 2.4 ± 1.1 | |
| No. of surveillance colonoscopies, n (mean ± SD) | 5.7 ± 4.0 | Distal colon | HD-WLE | 2.0 ± 1.4 |
| Interval from prior colonoscopy, months (mean ± SD) | 18.4 ± 10.7 | HD-NBI | 1.6 ± 2.1 | |
| Previous history of dysplasia and CRC, n (%) | 5 (15.2) | HD-DCE | 3.5 ± 2.7 | |
| Overall | Proximal colon | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HD-WLE | HD-NBI | HD-DCE | Total | HD-WLE | HD-NBI | HD-DCE | Total | |||||
| n | n | IDR | n | IDR | n | n | n | IDR | n | IDR | n | |
| Dysplasia | 3 | 0 | 0% | 0 | 0% | 3 | 1 | 0 | 0% | 0 | 0% | 1 |
| SSAs/Ps | 5 | 1 | 8% | 7 | 54% | 13 | 1 | 0 | 0% | 1 | 50% | 2 |
| Non-dysplastic lesions | 21 | 6 | 15% | 13 | 33% | 40 | 3 | 1 | 13% | 4 | 50% | 8 |
| Mid-colon | Distal colon | |||||||||||
| HD-WLE | HD-NBI | HD-DCE | Total | HD-WLE | HD-NBI | HD-DCE | Total | |||||
| n | n | IDR | n | IDR | n | n | n | IDR | n | IDR | n | |
| Dysplasia | 2 | 0 | 0% | 0 | 0% | 2 | 0 | 0 | - | 0 | - | 0 |
| SSAs/Ps | 1 | 0 | 0% | 2 | 67% | 3 | 3 | 1 | 13% | 4 | 50% | 8 |
| Non-dysplastic lesions | 5 | 2 | 17% | 5 | 42% | 12 | 13 | 3 | 15% | 4 | 20% | 20 |
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p | OR | 95% CI | p | |
| Dysplasia | 0.23 | 0.01–5.09 | 0.35 | 0.17 | 0.01–3.01 | 0.22 |
| Sessile serrated adenoma/polyp | 2.69 | 0.75–9.58 | 0.12 | 3.16 | 0.83–11.92 | 0.08 |
| Non-dysplastic lesion | 0.61 | 0.18–2.03 | 0.42 | 0.61 | 0.18–2.03 | 0.42 |
| Overall | Proximal colon | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HD-WLE | HD-NBI | HD-DCE | Total | HD-WLE | HD-NBI | HD-DCE | Total | |||||
| n | n | IDR | n | IDR | n | n | n | IDR | n | IDR | n | |
| Dysplasia | 3 | 0 | 0% | 0 | 0% | 3 | 1 | 0 | 0% | 0 | 0% | 1 |
| SSAs/Ps | 4 | 1 | 9% | 7 | 64% | 11 | 1 | 0 | 0% | 1 | 50% | 2 |
| Non-dysplastic lesions | 10 | 5 | 26% | 9 | 47% | 19 | 3 | 1 | 25% | 2 | 50% | 4 |
| Mid-colon | Distal colon | |||||||||||
| HD-WLE | HD-NBI | HD-DCE | Total | HD-WLE | HD-NBI | HD-DCE | Total | |||||
| n | n | IDR | n | IDR | n | n | n | IDR | n | IDR | n | |
| Dysplasia | 2 | 0 | 0% | 0 | 0% | 2 | 0 | 0 | - | 0 | - | 0 |
| SSAs/Ps | 1 | 0 | 0% | 2 | 67% | 3 | 3 | 1 | 14% | 4 | 57% | 7 |
| Non-dysplastic lesions | 3 | 1 | 11% | 5 | 56% | 9 | 6 | 3 | 38% | 2 | 25% | 8 |
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Age (+1 year) | 1.01 | 0.95–1.06 | 0.81 | |||
| Male (vs. Female) | 2.23 | 0.41–12.11 | 0.35 | |||
| No. of prior surveillance conolonoscopies | 0.99 | 0.81–0.19 | 0.89 | |||
| Interval from prior colonoscopy (+1 month) | 0.98 | 0.91–1.06 | 0.65 | |||
| 5-Aminosalicylates | 2.44 | 0.06–108.35 | 0.64 | |||
| Azathioprine | 0.85 | 0.18–4.12 | 0.84 | |||
| Infliximab | 1.03 | 0.21–5.07 | 0.97 | |||
| Adalimumab/vedolizumab | 0.17 | 0.02–1.23 | 0.079 | 0.12 | 0.01–2.04 | 0.14 |
| Withdrawal time (+1 min) | 1.08 | 0.95–1.24 | 0.24 | |||
| Large SSA/P (>1 cm) | 7.00 | 0.70–69.68 | 0.097 | 10.28 | 0.21–496.67 | 0.24 |
| Multiple SSAs/Ps (≥2) | 14.99 | 1.72–131.21 | 0.014 | 4.07 | 0.35–47.27 | 0.26 |
| Previous dysplasia | 4.01 | 0.56–28.74 | 0.17 | 2.81 | 0.24–32.80 | 0.41 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.E.; Choi, C.W.; Hong, S.N.; Song, J.H.; Kim, E.R.; Chang, D.K.; Kim, Y.-H. Incremental Detection Rate of Dysplasia and Sessile Serrated Polyps/Adenomas Using Narrow-Band Imaging and Dye Spray Chromoendoscopy in Addition to High-Definition Endoscopy in Patients with Long-Standing Extensive Ulcerative Colitis: Segmental Tandem Endoscopic Study. Diagnostics 2023, 13, 516. https://doi.org/10.3390/diagnostics13030516
Kim JE, Choi CW, Hong SN, Song JH, Kim ER, Chang DK, Kim Y-H. Incremental Detection Rate of Dysplasia and Sessile Serrated Polyps/Adenomas Using Narrow-Band Imaging and Dye Spray Chromoendoscopy in Addition to High-Definition Endoscopy in Patients with Long-Standing Extensive Ulcerative Colitis: Segmental Tandem Endoscopic Study. Diagnostics. 2023; 13(3):516. https://doi.org/10.3390/diagnostics13030516
Chicago/Turabian StyleKim, Ji Eun, Chang Wan Choi, Sung Noh Hong, Joo Hye Song, Eun Ran Kim, Dong Kyung Chang, and Young-Ho Kim. 2023. "Incremental Detection Rate of Dysplasia and Sessile Serrated Polyps/Adenomas Using Narrow-Band Imaging and Dye Spray Chromoendoscopy in Addition to High-Definition Endoscopy in Patients with Long-Standing Extensive Ulcerative Colitis: Segmental Tandem Endoscopic Study" Diagnostics 13, no. 3: 516. https://doi.org/10.3390/diagnostics13030516