
Clinical Applications of B-Flow Ultrasound: A Scoping Review of the Literature

Abstract
:1. Introduction
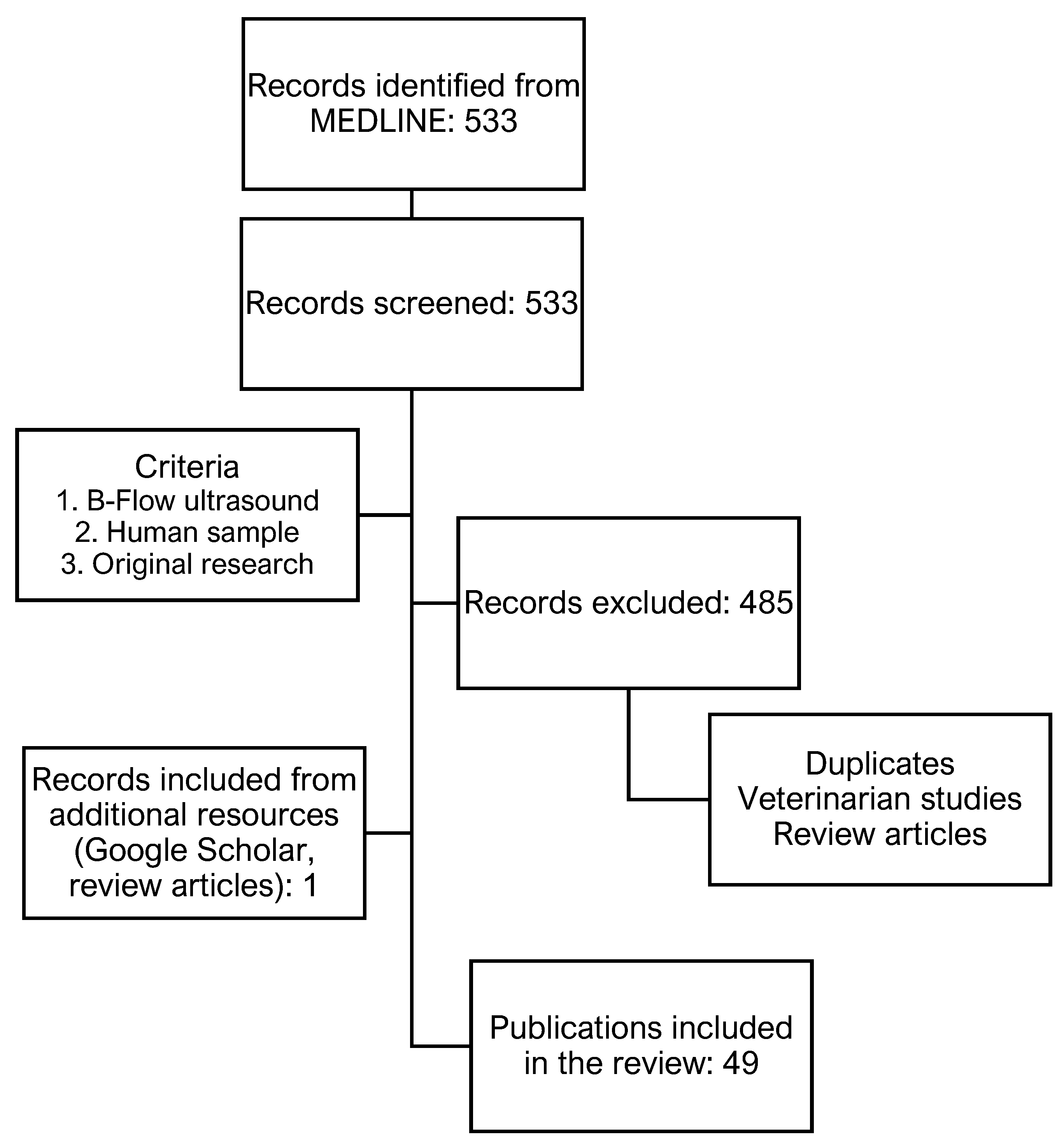
2. Methods
2.1. Abdominal Ultrasound
2.2. Obstetrics and Gynecology
2.3. Vascular Medicine
2.3.1. Extracranial Arteries
2.3.2. Vascular Access Care
2.3.3. Phlebology
2.3.4. Endovascular Interventions
2.3.5. Peripheral Artery Occlusive Disease
2.4. Further Applications
3. Discussion
3.1. Research in Context
3.2. Limitations of Current Evidence
3.3. Future Perspectives
Funding
Conflicts of Interest
References
- Jibiki, T. Coded excitation medical ultrasound imaging. Igaku Butsuri Nihon Igaku Butsuri Gakkai Kikanshi Jpn. J. Med. Phys. Off. J. Jpn. Soc. Med. Phys. 2001, 21, 136–141. [Google Scholar]
- Chiao, R.; Hao, X. Coded excitation for diagnostic ultrasound: A system developer’s perspective. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2005, 52, 160–170. [Google Scholar] [CrossRef] [PubMed]
- Lahav, A.; Ben-Shalom, Y.; Chernyakova, T.; Eldar, Y.C. Coded excitation ultrasound: Efficient implementation via frequency domain processing. In Proceedings of the 2016 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), Shanghai, China, 20–25 March 2016; IEEE: Las Vegas, NV, USA, 2016; pp. 674–678. [Google Scholar]
- O’Donnell, M.; Wang, Y. Coded excitation for synthetic aperture ultrasound imaging. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2005, 52, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Yang, J.; Ji, J.; Zhang, Y.; Zhou, S. Research on Golay-coded excitation in real-time imaging of high frequency ultrasound biomicroscopy. Sci. Rep. 2021, 11, 1848. [Google Scholar] [CrossRef] [PubMed]
- Mamou, J.; Ketterling, J.A.; Silverman, R.H. Chirp-coded excitation imaging with a high-frequency ultrasound annular array. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2008, 55, 508–513. [Google Scholar] [CrossRef] [Green Version]
- Yoon, C.; Lee, W.; Chang, J.H.; Song, T.-K.; Yoo, Y. An efficient pulse compression method of chirp-coded excitation in medical ultrasound imaging. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2013, 60, 2225–2229. [Google Scholar] [CrossRef]
- Kang, J.; Kim, Y.; Lee, W.; Yoo, Y. A New Dynamic Complex Baseband Pulse Compression Method for Chirp-Coded Excitation in Medical Ultrasound Imaging. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2017, 64, 1698–1710. [Google Scholar] [CrossRef]
- Misaridis, T.; Jensen, J. Use of modulated excitation signals in medical ultrasound. Part I: Basic concepts and expected benefits. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2005, 52, 177–191. [Google Scholar] [CrossRef]
- Peng, Q.; Gao, S. Coded excitation and its applications in medical ultrasound imaging. Sheng Wu Yi Xue Gong Cheng Xue Za Zhi J. Biomed. Eng. Shengwu Yixue Gongchengxue Zazhi 2005, 22, 175–180. [Google Scholar]
- Lamboul, B.; Bennett, M.; Anderson, T.; McDicken, N. Basic considerations in the use of coded excitation for color flow imaging applications. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2009, 56, 727–737. [Google Scholar] [CrossRef]
- Zhao, H.; Mo, L.Y.L.; Gao, S. Barker-coded ultrasound color flow imaging: Theoretical and practical design considerations. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2007, 54, 319–331. [Google Scholar] [CrossRef] [PubMed]
- Nowicki, A.; Tasinkiewicz, J.; Trots, I. Flow imaging using differential Golay encoded ultrasound. Ultrasonics 2022, 126, 106825. [Google Scholar] [CrossRef] [PubMed]
- Deane, C. Extended field-of-view and B-flow ultrasound: Fashion or future? Ultrasound Obstet. Gynecol. 2000, 15, 96–97. [Google Scholar] [CrossRef] [PubMed]
- Weskott, H.-P. B-flow—A new method for detecting blood flow. Ultraschall Med. 2000, 21, 59–65. [Google Scholar] [CrossRef]
- Henri, P.; Tranquart, F. B-flow ultrasonographic imaging of circulating blood. J. Radiol. 2000, 81, 465–467. [Google Scholar]
- Tochio, H.; Iwasaki, N.; Nakamura, H.; Nakayama, K.; Soga, T.; Nishiuma, S.; Fukunaga, T.; Okabe, Y.; Kashida, H.; Hirasa, M.; et al. Proximal bifurcation of hepatic artery: Novel findings on hepatic arteries demonstrated by ultrasound Doppler imaging, B-flow, and US angiography. J. Med. Ultrason. 2002, 29, 11–17. [Google Scholar] [CrossRef]
- Furuse, J.; Maru, Y.; Mera, K.; Sumi, H.; Yoshino, M.; Yokoyama, Y.; Ms, H.H.; Ejiri, A. Visualization of blood flow in hepatic vessels and hepatocellular carcinoma using B-flow sonography. J. Clin. Ultrasound 2001, 29, 1–6. [Google Scholar] [CrossRef]
- Ono, N.; Ijuin, H.; Suga, H.; Okabe, Y.; Yakushiji, K.; Hashiguchi, M.; Kurohiji, T.; Koga, N.; Kumashiro, R.; Sata, M. B-Flow contrast US with Levovist in hepatic tumors: Preliminary results. Kurume Med. J. 2003, 50, 21–25. [Google Scholar] [CrossRef]
- Jung, E.M.; Kubale, R.; Jungius, K.-P.; Jung, W.; Lenhart, M.; Clevert, D.A. Vascularization of liver tumors—Preliminary results with Coded Harmonic Angio (CHA), phase inversion imaging, 3D power Doppler and contrast medium-enhanced B-flow with second generation contrast agent (Optison). Clin. Hemorheol. Microcirc. 2006, 34, 483–497. [Google Scholar]
- Wachsberg, R.H. B-flow imaging of the hepatic vasculature: Correlation with color doppler sonography. Am. J. Roentgenol. 2007, 188, W522–W533. [Google Scholar] [CrossRef]
- Wang, F.; Numata, K.; Nihonmatsu, H.; Chuma, M.; Ideno, N.; Nozaki, A.; Ogushi, K.; Tanab, M.; Okada, M.; Luo, W.; et al. Added Value of Ultrasound-Based Multimodal Imaging to Diagnose Hepatic Sclerosed Hemangioma before Biopsy and Resection. Diagnostics 2022, 12, 2818. [Google Scholar] [CrossRef] [PubMed]
- Wachsberg, R.H. B-flow, a non-doppler technology for flow mapping: Early experience in the abdomen. Ultrasound Q. 2003, 19, 114–122. [Google Scholar] [CrossRef] [PubMed]
- Tola, M.; Yurdakul, M.; Ozbulbul, N.I. B-flow imaging for the measurement of residual lumen diameter of renal artery stenosis. J. Clin. Ultrasound 2012, 40, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Russo, E.; Cerbone, V.; Sciano, D.; Valeriani, G.; De Rosa, P. Posttransplant renal monitoring with B-flow ultrasonography. Transplant. Proc. 2010, 42, 1127–1129. [Google Scholar] [CrossRef]
- Dammann, E.; Groth, M.; Schild, R.-S.; Lemke, A.; Oh, J.; Adam, G.; Herrmann, J. B-Flow Sonography vs. Color Doppler Sonography for the Assessment of Vascularity in Pediatric Kidney Transplantation. In RöFo-Fortschritte auf dem Gebiet der Röntgenstrahlen und der Bildgebenden Verfahr; Georg Thieme Verlag KG: New York, NY, USA, 2021; Volume 193, pp. 49–60. [Google Scholar] [CrossRef]
- Ahmed, B.I. The new 3D/4D based spatio-temporal imaging correlation (STIC) in fetal echocardiography: A promising tool for the future. J. Matern.-Fetal Neonatal Med. 2014, 27, 1163–1168. [Google Scholar] [CrossRef]
- Lei, W.; Ying, Z.; Ailu, C.; Xiaoguang, W. Evaluation of normal fetal ductus venosus using b-flow imaging with spatiotemporal image correlation and traditional color doppler echocardiography. Echocardiography 2015, 32, 325–331. [Google Scholar] [CrossRef]
- Volpe, P.; Campobasso, G.; Stanziano, A.; De Robertis, V.; Di Paolo, S.; Caruso, G.; Volpe, N.; Gentile, M. Novel application of 4D sonography with B-flow imaging and spatio-temporal image correlation (STIC) in the assessment of the anatomy of pulmonary arteries in fetuses with pulmonary atresia and ventricular septal defect. Ultrasound Obstet. Gynecol. 2006, 28, 40–46. [Google Scholar] [CrossRef]
- Volpe, P.; Campobasso, G.; De Robertis, V.; Di Paolo, S.; Caruso, G.; Stanziano, A.; Volpe, N.; Gentile, M. Two- and four-dimensional echocardiography with B-flow imaging and spatiotemporal image correlation in prenatal diagnosis of isolated total anomalous pulmonary venous connection. Ultrasound Obstet. Gynecol. 2007, 30, 830–837. [Google Scholar] [CrossRef]
- Lee, W.; Espinoza, J.; Cutler, N.; Bronsteen, R.A.; Yeo, L.; Romero, R. The “starfish” sign: A novel sonographic finding with B-flow imaging and spatiotemporal image correlation in a fetus with total anomalous pulmonary venous return. Ultrasound Obstet. Gynecol. 2010, 35, 124–125. [Google Scholar] [CrossRef] [Green Version]
- Volpe, P.; Tuo, G.; De Robertis, V.; Campobasso, G.; Marasini, M.; Tempesta, A.; Gentile, M.; Rembouskos, G. Fetal interrupted aortic arch: 2D-4D echocardiography, associations and outcome. Ultrasound Obstet. Gynecol. 2010, 35, 302–309. [Google Scholar] [CrossRef]
- Pooh, R.K.; Korai, A. B-flow and B-flow spatio-temporal image correlation in visualizing fetal cardiac blood flow. Croat. Med. J. 2005, 46, 808–811. [Google Scholar] [PubMed]
- Pooh, R.K. New application of B-flow sono-angiography in perinatology. Ultrasound Obstet. Gynecol. 2000, 15, 163. [Google Scholar] [CrossRef] [PubMed]
- Groth, M.; Ernst, M.; Deindl, P.; Herrmann, J. B-Flow Sonography for Evaluation of Basal Cerebral Arteries in Newborns. Clin. Neuroradiol. 2019, 29, 95–100. [Google Scholar] [CrossRef]
- Dighe, M.K.; Moshiri, M.; Jolley, J.; Thiel, J.; Hippe, D. B-Flow imaging of the placenta: A feasibility study. Ultrasound 2018, 26, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Sladkevicius, P.; Zannoni, L.; Valentin, L. B-flow ultrasound facilitates visualization of contrast medium during hysterosalpingo-contrast sonography. Ultrasound Obstet. Gynecol. 2014, 44, 221–227. [Google Scholar] [CrossRef]
- Mikami, T.; Takahashi, A.; Houkin, K. Evaluation of blood flow in carotid artery stenosis using B-flow sonography. Neurol. Medico-Chir. 2003, 43, 528–532; discussion 533. [Google Scholar] [CrossRef] [Green Version]
- Jung, E.M.; Clevert, D.-A.; Rupp, N. B-flow and color-coded B-flow in sonographic diagnosis of filiform stenosis of the internal carotid artery. Rofo Fortschr. Geb. Rontgenstrahlen Nukl. 2003, 175, 1251–1258. [Google Scholar] [CrossRef]
- Umemura, A.; Yamada, K.; Yoshimoto, Y.; Tanaka, Y.; Hoya, K. B-mode flow imaging of the carotid artery. Stroke 2001, 32, 2055–2057. [Google Scholar] [CrossRef] [Green Version]
- Jung, E.M.; Kubale, R.; Clevert, D.A.; Weskott, H.-P.; Prantl, L.; Herold, T.; Renz, M.; Rupp, N.; Tacke, J. B-flow and B-flow with 3D and SRI postprocessing before intervention and monitoring after stenting of the internal carotid artery. Clin. Hemorheol. Microcirc. 2007, 36, 35–46. [Google Scholar]
- Jung, E.M.; Kubale, R.; Ritter, G.; Gallegos, M.T.; Jungius, K.-P.; Rupp, N.; Clevert, D.-A. Diagnostics and characterisation of preocclusive stenoses and occlusions of the internal carotid artery with B-flow. Eur. Radiol. 2007, 17, 439–447. [Google Scholar] [CrossRef]
- Pfister, K.; Rennert, J.; Greiner, B.; Jung, W.; Stehr, A.; Gössmann, H.; Menzel, C.; Zorger, N.; Prantl, L.; Feuerbach, S.; et al. Pre-surgical evaluation of ICA-stenosis using 3D power Doppler, 3D color coded Doppler sonography, 3D B-flow and contrast enhanced B-flow in correlation to CTA/MRA: First clinical results. Clin. Hemorheol. Microcirc. 2009, 41, 103–116. [Google Scholar] [CrossRef] [PubMed]
- Clevert, D.-A.; Johnson, T.; Jung, E.M.; Flach, P.M.; Strautz, T.I.; Ritter, G.; Gallegos, M.T.; Kubale, R.; Becker, C.; Reiser, M. Color Doppler, power Doppler and B-flow ultrasound in the assessment of ICA stenosis: Comparison with 64-MD-CT angiography. Eur. Radiol. 2007, 17, 2149–2159. [Google Scholar] [CrossRef] [PubMed]
- Yurdakul, M.; Tola, M.; Cumhur, T. B-flow imaging of internal carotid artery stenosis: Comparison with power Doppler imaging and digital subtraction angiography. J. Clin. Ultrasound 2004, 32, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Bucek, R.A.; Reiter, M.; Koppensteiner, I.; Ahmadi, R.; Minar, E.; Lammer, J. B-flow evaluation of carotid arterial stenosis: Initial experience. Radiology 2002, 225, 295–299. [Google Scholar] [CrossRef] [PubMed]
- Tola, M.; Yurdakul, M.; Cumhur, T. combined use of color duplex ultrasonography and B-flow imaging for evaluation of patients with carotid artery stenosis. Am. J. Neuroradiol. 2004, 25, 1856–1860. [Google Scholar] [PubMed]
- Gong, H.-Y.; Shi, X.-K.; Zhu, H.-Q.; Chen, X.-Z.; Zhu, J.; Zhao, B.-W. Evaluation of carotid atherosclerosis and related risk factors using ultrasonic B-Flow technology in elderly patients. J. Int. Med. Res. 2020, 48, 300060520961224. [Google Scholar] [CrossRef]
- Clevert, D.-A.; Jung, E.M.; Johnson, T.; Kubale, R.; Rupp, N.; Schoenberg, S.O.; Reiser, M. Cervical artery dissection: Improved diagnosis by B-Flow ultrasound. Clin. Hemorheol. Microcirc. 2007, 36, 141–153. [Google Scholar]
- Clevert, D.A.; Rupp, N.; Reiser, M.; Jung, E.M. Improved diagnosis of vascular dissection by ultrasound B-flow: A comparison with color-coded Doppler and power Doppler sonography. Eur. Radiol. 2005, 15, 342–347. [Google Scholar] [CrossRef]
- Cutler, J.J.; Campo, N.; Koch, S. B-Flow and B-Mode Ultrasound Imaging in Carotid Fibromuscular Dysplasia. J. Neuroimaging 2018, 28, 269–272. [Google Scholar] [CrossRef]
- Jung, E.M.; Kubale, R.; Clevert, D.-A.; Rupp, N. Improved evaluation of stenoses of hemodialysis fistulas by B-flow ultrasound. Rofo Fortschr. Geb. Rontgenstrahlen Nukl. 2003, 175, 387–392. [Google Scholar] [CrossRef]
- Putz, F.J.; Pfister, K.; Bergler, T.; Banas, M.C.; Jung, E.M.; Banas, B.; Schierling, W. Sonographic 3-D Power Doppler Imaging Enhances Rapid Assessment of Morphologic and Pathologic Arteriovenous Fistula Variations. Ultrasound Med. Biol. 2021, 47, 1484–1494. [Google Scholar] [CrossRef] [PubMed]
- Lurie, F.; Kistner, R.L.; Eklof, B.; Kessler, D. Mechanism of venous valve closure and role of the valve in circulation: A new concept. J. Vasc. Surg. 2003, 38, 955–961. [Google Scholar] [CrossRef]
- Lugli, M.; Maleti, O.; Iabichella, M.L.; Perrin, M. Investigation of non-saphenous veins in C0S patients. Int. Angiol. 2018, 37, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Jung, E.M.; Lutz, R.; Clevert, D.-A.; Rupp, N. B-Flow: Sonographic assessment and therapy for femoral artery pseudoaneurysm. Rofo Fortschr. Auf Dem Geb. Rontgenstrahlen Nukl. 2001, 173, 805–809. [Google Scholar] [CrossRef]
- Li, L.; Deng, H.; Yuan, Y.; Ye, X. Thrombin injection under B-flow and ultrasound guidance: A safe and effective treatment of pseudoaneurysms. Vascular 2022, 17085381221124708. [Google Scholar] [CrossRef]
- Cai, D.; Wu, W.W.; Zhang, D.D.; Chi, M.Y.; Ma, Y.; Cheng, D.; Zhou, Y.; Zhao, Q.Y. Effects of two dimensional gray-scale blood flow imaging combined with color Doppler flow imaging in guiding arterial puncture and catheterization through wounds in patients with large burns. Zhonghua Shao Shang Za Zhi = Zhonghua Shaoshang Zazhi= Chin. J. Burn. 2020, 36, 440–445. [Google Scholar]
- D’Abate, F.; De Bruin, J.L. Additional value of B-flow imaging in arterial wall calcifications. J. Clin. Ultrasound 2018, 46, 136–139. [Google Scholar] [CrossRef] [PubMed]
- D’Abate, F.; Ramachandran, V.; Young, M.A.; Farrah, J.; Ahmed, M.H.; Jones, K.; Hinchliffe, R.J. B-Flow Imaging in Lower Limb Peripheral Arterial Disease and Bypass Graft Ultrasonography. Ultrasound Med. Biol. 2016, 42, 2345–2351. [Google Scholar] [CrossRef] [Green Version]
- Kehrer, A.; Heidekrueger, P.I.; Lonic, D.; Taeger, C.D.; Klein, S.; Lamby, P.; Sachanadani, N.S.; Jung, E.M.; Prantl, L.; Da Silva, N.P.B. High-Resolution Ultrasound-Guided Perforator Mapping and Characterization by the Microsurgeon in Lower Limb Reconstruction. J. Reconstr. Microsurg. 2021, 37, 75–82. [Google Scholar] [CrossRef]
- Heneweer, C.; Zirk, M.M.; Safi, A.M.; Smeets, R.M.; Malter, W.; Kröger, N.; Zöller, J.E.M.; Maintz, D.M.; Zinser, M.M. An Innovative Approach for Preoperative Perforator Flap Planning Using Contrast-enhanced B-flow Imaging. Plast. Reconstr. Surg. Glob. Open 2021, 9, e3547. [Google Scholar] [CrossRef]
- Volpe, A.; Caramaschi, P.; Marchetta, A.; Biasi, D.; Bambara, L.M.; Arcaro, G. B-flow ultrasound in a case of giant cell arteritis. Clin. Rheumatol. 2007, 26, 1955–1957. [Google Scholar] [CrossRef] [PubMed]
- Lottspeich, C.; Puhr-Westerheide, D.; Stana, J.; Hoffmann, U.; Czihal, M. The Flashlight-Sign: A Novel B-Flow Based Ultrasound Finding for Detection of Intraluminal, Wall-Adherent, Floating Structures of the Abdominal Aorta and Peripheral Arteries. Diagnostics 2022, 12, 1708. [Google Scholar] [CrossRef] [PubMed]
- Brunese, L.; Romeo, A.; Iorio, S.; Napolitano, G.; Fucili, S.; Zeppa, P.; Vallone, G.; Lombardi, G.; Bellastella, A.; Biondi, B.; et al. Thyroid B-flow twinkling sign: A new feature of papillary cancer. Eur. J. Endocrinol. 2008, 159, 447–451. [Google Scholar] [CrossRef] [Green Version]
- Ohyama, Y.; Naganuma, H.; Ishida, H.; Hoshino, T. Portal vein gas in a patient with acute cholangitis: Report of a case with emphasis on B-flow imaging. J. Med. Ultrason. 2022, 49, 107–108. [Google Scholar] [CrossRef]
- Dashe, J.S.; McIntire, D.D.; Twickler, D.M. Maternal obesity limits the ultrasound evaluation of fetal anatomy. J. Ultrasound Med. 2009, 28, 1025–1030. [Google Scholar] [CrossRef]
- Kornezos, I.; Chatziioannou, A.; Kokkonouzis, I.; Nebotakis, P.; Moschouris, H.; Yiarmenitis, S.; Mourikis, D.; Matsaidonis, D. Findings and limitations of focused ultrasound as a possible screening test in stable adult patients with blunt abdominal trauma: A Greek study. Eur. Radiol. 2010, 20, 234–238. [Google Scholar] [CrossRef] [PubMed]
- De Jong, M.D.F.; Dubelaar, I.J.M.; Fassaert, T.A.; Jager, G.J.; Mus, R.D.M.; Rutten, M.J.C.M. 3-D ultrasound of the breast: Less dependent on the investigator. Ned. Tijdschr. Geneeskd. 2011, 155, A3702. [Google Scholar]
- Sistrom, C.L.; McKay, N.L. Costs, charges, and revenues for hospital diagnostic imaging procedures: Differences by modality and hospital characteristics. J. Am. Coll. Radiol. 2005, 2, 511–519. [Google Scholar] [CrossRef]
- Jang, J.-Y.; Kim, S.-W.; Lee, S.E.; Hwang, D.W.; Kim, E.-J.; Lee, J.Y.; Kim, S.J.; Ryu, J.K.; Kim, Y.-T. Differential Diagnostic and Staging Accuracies of High Resolution Ultrasonography, Endoscopic Ultrasonography, and Multidetector Computed Tomography for Gallbladder Polypoid Lesions and Gallbladder Cancer. Ann. Surg. 2009, 250, 943–949. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.H.; Cha, J.G.; Hong, H.S.; Lee, J.S.; Park, S.J.; Paik, S.H.; Lee, H.K. Comparison of High-Resolution Ultrasonography and Computed Tomography in the Diagnosis of Nasal Fractures. J. Ultrasound Med. 2009, 28, 717–723. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Sackett, D.L.; Sinclair, J.C.; Hayward, R.; Cook, D.J.; Cook, R.J. Users’ guides to the medical literature. IX. A method for grading health care recommendations. Evidence-Based Medicine Working Group. JAMA 1995, 274, 1800–1804. [Google Scholar] [CrossRef] [PubMed]
- European Society of Radiology; Alberich-Bayarri, A.; Sourbron, S.; Golay, X.; Desouza, N.; Smits, M.; van der Lugt, A.; Boellard, R. ESR Statement on the Validation of Imaging Biomarkers. Insights Imaging 2020, 11, 76. [Google Scholar] [CrossRef] [PubMed]
- Ranschaert, E.R.; Morozov, S.; Algra, P.R. (Eds.) Artificial Intelligence in Medical Imaging: Opportunities, Applications and Risks; Springer: Cham, Switzerland, 2019; ISBN 978-3-319-94877-5. [Google Scholar]
- Koksalmis, G.H. Drivers to adopting B-flow ultrasonography:contextualizing the integrated technology acceptance model. BMC Med. Imaging 2019, 19, 56. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Anatomic Location | Pathologies | |||
|---|---|---|---|---|
| Head/Neck |
Carotid artery stenosis Thyroid papillary cancer |
Carotid artery stenting Carotid artery occlusion | Carotid/vertebral artery dissection | Refs. [38,39,40,41,42,43,44,45,46,47,48,49,50,51,65] |
| Abdomen |
Abdominal aorta Hepatic tumor vascularization Renal artery stenosis |
Visceral arteries Hepatic sclerosed hemangioma |
Hepatic arteries Kidney transplants | Refs. [17,18,19,20,21,22,23,24,25,26] |
| Fetus/Neonate |
Fetal ductus venosus Interrupted aortic arch |
PA-VSD Umbilical blood flow |
ITAPVC Basal cerebral artery | Refs. [28,29,30,31,32,33,34,35] |
| Female reproductive system | Placenta vascularization | Hysterosalpingo contrast-sonography | Refs. [36,37] | |
| Peripheral vascular system |
Arteriovenous fistulas Arterial puncture | (Pseudo-) Aneurysms | PAOD | Refs. [52,53,54,55,56,57,58,59,60] |
| Other | Perforator flap mapping | Giant cell arteritis | Refs. [61,62,63] | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hofmann, A.G.; Mlekusch, I.; Wickenhauser, G.; Assadian, A.; Taher, F. Clinical Applications of B-Flow Ultrasound: A Scoping Review of the Literature. Diagnostics 2023, 13, 397. https://doi.org/10.3390/diagnostics13030397
Hofmann AG, Mlekusch I, Wickenhauser G, Assadian A, Taher F. Clinical Applications of B-Flow Ultrasound: A Scoping Review of the Literature. Diagnostics. 2023; 13(3):397. https://doi.org/10.3390/diagnostics13030397
Chicago/Turabian StyleHofmann, Amun G., Irene Mlekusch, Georg Wickenhauser, Afshin Assadian, and Fadi Taher. 2023. "Clinical Applications of B-Flow Ultrasound: A Scoping Review of the Literature" Diagnostics 13, no. 3: 397. https://doi.org/10.3390/diagnostics13030397