
Immunometabolic Profiling of Chronic Subdural Hematoma through Untargeted Mass Spectrometry Analysis: Preliminary Findings of a Novel Approach
 , , and
, , and
Abstract
:1. Introduction
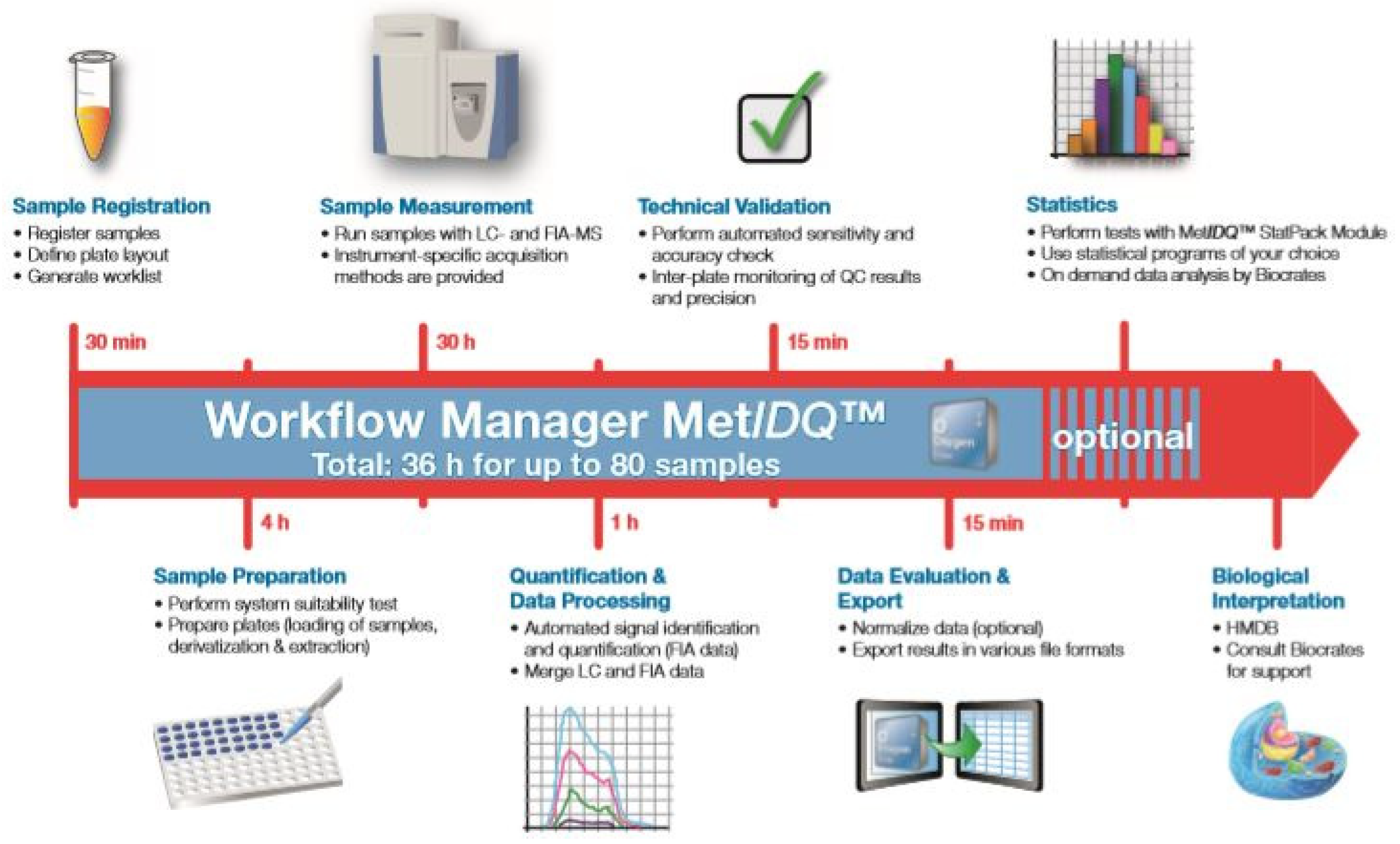
2. Materials and Methods
Study Design
3. Definition of Objectives
Statistical Analysis
4. Results
4.1. General Patient Demographics
4.2. Univariate Analysis
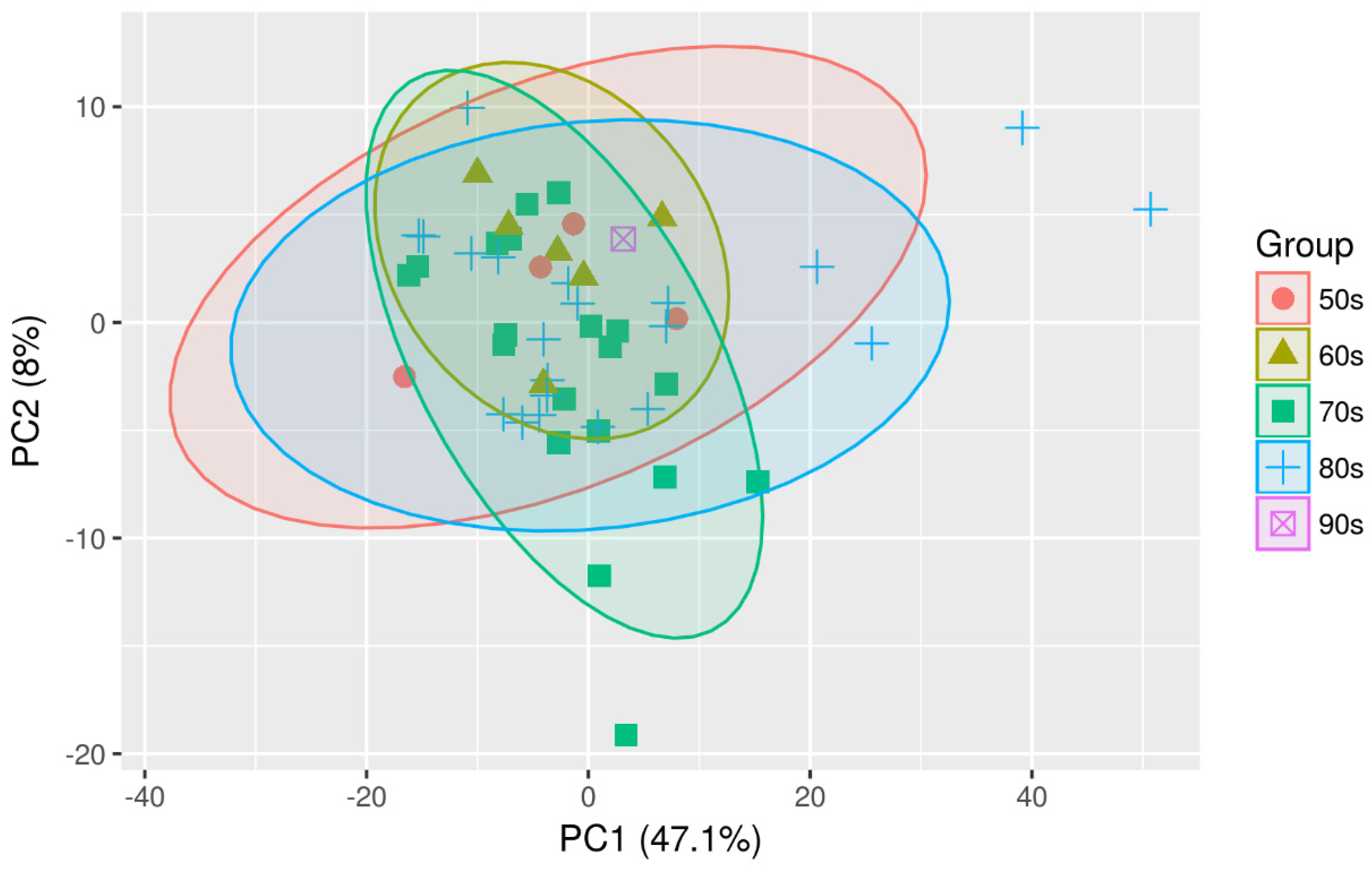
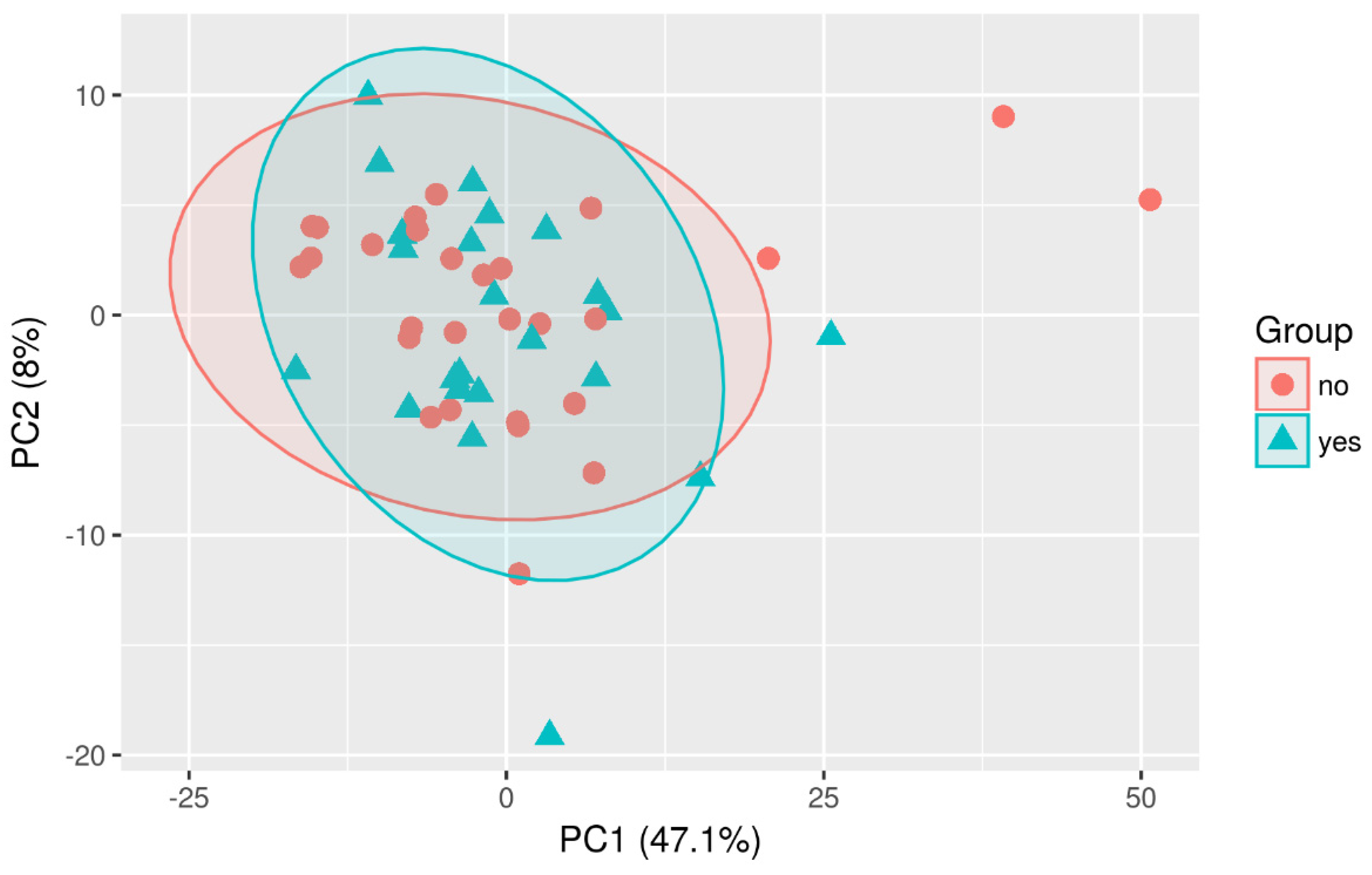
4.3. Multivariate Analysis
4.4. Metabolism Indicators
5. Discussion
6. Potential Drawbacks
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Jacob, W.J. Observationes Anatomicæ ex Cadaveribus Eorum, Quos Sustulit Apoplexia; National Library of the Netherlands: Amsterdam, The Netherlands, 1745; Available online: https://books.google.ro/books?hl=ro&lr=&id=ZslkAAAAcAAJ&oi=fnd&pg=PA1&dq=%3DJohan+Jacob+W.+Observationes+anatomic%C3%A6+ex+cadaveribus+eorum,+quos+sustulit+apoplexia+-+Johan+Jacob+Wepfer+-+Google+Books.+Published+1745.+Accessed+November+29,+2022.+h.&ots=VI7PryXsWJ&sig=8uT37ZSzjQxFchzgrSWVAauUYQg&redir_esc=y#v=onepage&q&f=false (accessed on 29 November 2022).
- Bayle, A.L.J. Traité des Maladies du Cerveau et de ses Membranes; Austrian National Library: Wien, Austria, 1826; Available online: https://books.google.ro/books?hl=ro&lr=&id=QzZbAAAAcAAJ&oi=fnd&pg=PR1&dq=%3DBayle+ALJ.+Trait%C3%A9+des+maladies+du+cerveau+et+de+ses+membranes+-+Antoine+Laurent+Jess%C3%A9+Bayle+-+Google+Books.+Published+1826.+Accessed+November+30,+2022.&ots=ZlYTvp5RKY&sig=IWjZIgDbgxxdKh6OfdCCLW3NZUA&redir_esc=y#v=onepage&q&f=false (accessed on 30 November 2022).
- Virchow, R.L.C. Virchow 1857. In Verhandlungen Der Physikalisch-Medizinischen Gesellschaft Zu Würzburg; Universitätsbibliothek Johann Christian Senckenberg: Vienna, Austria, 1857; pp. 134–142. [Google Scholar]
- Müller, M.; Biedermann, M.; Strecker, W. Komplikation im Rahmen der Kyphoplastie. Orthopade 2006, 35, 1183–1186. [Google Scholar] [CrossRef] [PubMed]
- Markwalder, T. Chronic subdural hematomas: A review. J. Neurosurg. 1981, 54, 637–645. [Google Scholar] [CrossRef] [PubMed]
- Fu, S.; Li, F.; Bie, L. Drug therapy for chronic subdural hematoma: Bench to bedside. J. Clin. Neurosci. 2018, 56, 16–20. [Google Scholar] [CrossRef] [PubMed]
- Edlmann, E.; Giorgi-Coll, S.; Whitfield, P.C.; Carpenter, K.L.H.; Hutchinson, P.J. Pathophysiology of chronic subdural haematoma: Inflammation, angiogenesis and implications for pharmacotherapy. J. Neuroinflammation 2017, 14, 108. [Google Scholar] [CrossRef]
- Holl, D.C.; Volovici, V.; Dirven, C.M.; Peul, W.C.; van Kooten, F.; Jellema, K.; van der Gaag, N.A.; Miah, I.P.; Kho, K.H.; Hertog, H.M.D.; et al. Pathophysiology and Nonsurgical Treatment of Chronic Subdural Hematoma: From Past to Present to Future. World Neurosurg. 2018, 116, 402–411.e2. [Google Scholar] [CrossRef]
- Kitazono, M.; Yokota, H.; Satoh, H.; Onda, H.; Matsumoto, G.; Fuse, A.; Teramoto, A. Measurement of Inflammatory Cytokines and Thrombomodulin in Chronic Subdural Hematoma. Neurol. Med. Chir. 2012, 52, 810–815. [Google Scholar] [CrossRef]
- Weigel, R.; Schilling, L.; Krauss, J.K. The pathophysiology of chronic subdural hematoma revisited: Emphasis on aging processes as key factor. GeroScience 2022, 44, 1353–1371. [Google Scholar] [CrossRef]
- Breslin, J.W.; Pappas, P.J.; Cerveira, J.J.; Hobson, R.W.; Durán, W.N. VEGF increases endothelial permeability by separate signaling pathways involving ERK-1/2 and nitric oxide. Am. J. Physiol. Heart Circ. Physiol. 2022, 1709, 92–100. [Google Scholar] [CrossRef]
- Nanko, N.; Tanikawa, M.; Mase, M.; Fujita, M.; Tateyama, H.; Miyati, T.; Yamada, K. Involvement of Hypoxia-Inducible Factor-1.α and Vascular Endothelial Growth Factor in the Mechanism of Development of Chronic Subdural Hematoma. Neurol. Med. Chir. 2009, 49, 379–385. [Google Scholar] [CrossRef]
- Hua, C.; Zhao, G.; Feng, Y.; Yuan, H.; Song, H.; Bie, L.; Katayama, K.; Matsuda, N.; Kakuta, K.; Naraoka, M.; et al. Role of Matrix Metalloproteinase-2, Matrix Metalloproteinase-9, and Vascular Endothelial Growth Factor in the Development of Chronic Subdural Hematoma. J. Neurotrauma 2016, 33, 65–70. [Google Scholar] [CrossRef]
- Kalamatianos, T.; Stavrinou, L.C.; Koutsarnakis, C.; Psachoulia, C.; Sakas, D.E.; Stranjalis, G. PlGF and sVEGFR-1 in chronic subdural hematoma: Implications for hematoma development. J. Neurosurg. 2013, 118, 353–357. [Google Scholar] [CrossRef]
- Heula, A.-L.; Ohlmeier, S.; Sajanti, J.; Majamaa, K. Characterization of chronic subdural hematoma fluid proteome. Neurosurgery 2013, 73, 317–331. [Google Scholar] [CrossRef]
- Stanisic, M.; Lyngstadaas, S.P.; Pripp, A.H.; Aasen, A.O.; Lindegaard, K.-F.; Ivanovic, J.; Ilstad, E.; Konglund, A.; Sandell, T.; Ellingsen, O.; et al. Chemokines as markers of local inflammation and angiogenesis in patients with chronic subdural hematoma: A prospective study. Acta Neurochir. 2012, 154, 113–120. [Google Scholar] [CrossRef]
- Hutchinson, P.J.; Edlmann, E.; Bulters, D.; Zolnourian, A.; Holton, P.; Suttner, N.; Agyemang, K.; Thomson, S.; Anderson, I.A.; Al-Tamimi, Y.Z.; et al. Trial of Dexamethasone for Chronic Subdural Hematoma. N. Engl. J. Med. 2020, 383, 2616–2627. [Google Scholar] [CrossRef] [PubMed]
- Soleman, J.; Nocera, F.; Mariani, L. The conservative and pharmacological management of chronic subdural haematoma. Swiss Med. Wkly. 2017, 147, w14398. [Google Scholar] [CrossRef] [PubMed]
- Qiu, S.; Zhuo, W.; Sun, C.; Su, Z.; Yan, A.; Shen, L. Effects of atorvastatin on chronic subdural hematoma: A systematic review. Medicine 2017, 96, e7290. [Google Scholar] [CrossRef] [PubMed]
- Zou, H.; Zhu, X.-X.; Ding, Y.-H.; Zhang, G.-B.; Geng, Y.; Huang, D.-S. Statins in conditions other than hypocholesterolemic effects for chronic subdural hematoma therapy, old drug, new tricks? Oncotarget 2017, 8, 27541–27546. [Google Scholar] [CrossRef] [PubMed]
- Hirashima, Y.; Nagahori, T.; Nishijima, M.; Endo, S.; Takaku, A.; Nakagawa, Y. Analysis of Plasma and Hematoma Lipids Related to Choline Glycerophospholipid in Patients with Chronic Subdural Hematoma. Neurol. Med. Chir. 1994, 34, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Vallejo, A.N.; Mroczkowski, H.J.; Michel, J.J.; Woolford, M.; Blair, H.C.; Griffin, P.; McCracken, E.; Mihalik, S.J.; Reyes-Mugica, M.; Vockley, J. Pervasive inflammatory activation in patients with deficiency in very-long-chain acyl-coA dehydrogenase (VLCADD). Clin. Transl. Immunol. 2021, 10, e1304. [Google Scholar] [CrossRef]
- Oerton, J.; Khalid, J.M.; Besley, G.; Dalton, R.N.; Downing, M.; Green, A.; Henderson, M.; Krywawych, S.; Leonard, J.; Andresen, B.S.; et al. Newborn screening for medium chain acyl-CoA dehydrogenase deficiency in England: Prevalence, predictive value and test validity based on 1.5 million screened babies. J. Med. Screen. 2011, 18, 173–181. [Google Scholar] [CrossRef]
- Singh, A.K.; Suryanarayanan, B.; Choudhary, A.; Prasad, A.; Singh, S.; Gupta, L.N. A prospective randomized study of use of drain versus no drain after burr-hole evacuation of chronic subdural hematoma. Neurol. India 2014, 62, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Kapoor, S. Metabolomics Wellcome Trust-Funded Monographs and Book Chapters; Wellcome Trust: London, UK, 2012. [Google Scholar]
- Murdoch, C.; Muthana, M.; Lewis, C.E. Hypoxia regulates macrophage functions in inflammation. J. Immunol. 2005, 175, 6257–6263. [Google Scholar] [CrossRef]
- Fuhrmann, D.C.; Olesch, C.; Kurrle, N.; Schnütgen, F.; Zukunft, S.; Fleming, I.; Brüne, B. Chronic Hypoxia Enhances β-Oxidation-Dependent Electron Transport via Electron Transferring Flavoproteins. Cells 2019, 8, 172. [Google Scholar] [CrossRef] [PubMed]
- Dambrova, M.; Makrecka-Kuka, M.; Kuka, J.; Vilskersts, R.; Nordberg, D.; Attwood, M.M.; Smesny, S.; Sen, Z.D.; Guo, A.C.; Oler, E.; et al. Acylcarnitines: Nomenclature, Biomarkers, Therapeutic Potential, Drug Targets, and Clinical Trials. Pharmacol. Rev. 2022, 74, 506–551. [Google Scholar] [CrossRef] [PubMed]
- Rutkowsky, J.M.; Knotts, T.A.; Ono-Moore, K.D.; McCoin, C.S.; Huang, S.; Schneider, D.; Singh, S.; Adams, S.H.; Hwang, D.H.; Shigiyama, F.; et al. Acylcarnitines activate proinflammatory signaling pathways. Am. J. Physiol. Metab. 2014, 306, E1378–E1387. [Google Scholar] [CrossRef] [PubMed]
- Dadej, D.; Szczepanek-Parulska, E.; Wrotkowska, E.; Ruchała, M. Cushing’s syndrome is associated with altered adipokine profile. Front. Endocrinol. 2022, 13, 1032329. [Google Scholar] [CrossRef]
- Lodewijkx, R.; Immenga, S.; Berg, R.v.D.; Post, R.; Westerink, L.G.; Nabuurs, R.J.A.; Can, A.; Vandertop, W.P.; Verbaan, D. Tranexamic acid for chronic subdural hematoma. Br. J. Neurosurg. 2021, 35, 564–569. [Google Scholar] [CrossRef]
- Federal, U.; Catarina, D.S.; Catarina, S. Adipokines and Metabolic Syndrome: Pluripotent Markers for a Complex Relationship? Am. J. Hypertens. 2022, 35, 306–308. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Signed written consent | Previous ipsilateral or infratentorial surgical procedure within the previous six months |
| Age > 18 | Age < 18 |
| Burr-hole craniostomy |
| Total Samples N = 59 | |||
|---|---|---|---|
| Missing metabolite N = 8 |  |  | |
| Complete metabolite profile N = 51 | |||
| cSDH without recurrence N = 39 |  |  | cSDH with recurrence N = 12 |
| Sex | Recurrence of cSDH | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | Total | Yes | No | ||||||
| Age | Freq | % | Freq | % | Freq | % | Freq | % | Freq | % |
| 51–60 | 3 | 5.9 | 2 | 3.9 | 5 | 9.8 | 1 | 2 | 4 | 7.8 |
| 61–70 | 5 | 9.8 | 0 | 0 | 5 | 9.8 | 2 | 3.9 | 3 | 5.9 |
| 71–80 | 12 | 23.5 | 10 | 19.6 | 22 | 43.1 | 5 | 9.8 | 17 | 33.3 |
| 81–90 | 9 | 17.7 | 9 | 17.7 | 18 | 35.3 | 4 | 7.8 | 14 | 27.5 |
| 91–100 | 0 | 0 | 1 | 2 | 1 | 2 | 0 | 0 | 1 | 2 |
| Total | 29 | 56.9 | 22 | 43.1 | 51 | 100 | 12 | 23.5 | 39 | 76.5 |
| Acylcarnitines | Ratio (Rec./No Rec.) | p-Value |
|---|---|---|
| AC(0:0) | 0.83 | 0.103 |
| AC(2:0) | 0.82 | 0.134 |
| AC(3:0) | 0.83 | 0.238 |
| AC(4:0) | 0.77 | 0.124 |
| AC(4:0-OH) | 0.75 | 0.286 |
| AC(5:0) | 0.80 | 0.332 |
| AC(6:0) | 0.53 | 0.001 |
| AC(8:0) | 0.58 | 0.018 |
| AC(8:1) | 0.69 | 0.106 |
| AC(10:0) | 0.58 | 0.012 |
| AC(10:1) | 0.69 | 0.081 |
| AC(12:0) | 0.47 | 0.010 |
| AC(12:1) | 0.56 | 0.007 |
| AC(14:0) | 0.42 | 0.006 |
| AC(14:1) | 0.40 | 0.002 |
| AC(14:2) | 0.51 | 0.017 |
| AC(16:0) | 0.76 | 0.323 |
| AC(16:1) | 0.50 | 0.012 |
| AC(16:2) | 0.56 | 0.049 |
| AC(18:0) | 0.70 | 0.234 |
| AC(18:1) | 0.75 | 0.259 |
| AC(18:2) | 0.86 | 0.599 |
| Metabolism Indicator | Ratio | p-Value |
|---|---|---|
| MCAD Deficiency (NBS) | 0.70 | 0.079 |
| VLCAD Deficiency (NBS) | 0.53 | 0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kipele, M.; Buchfelder, M.; Taudte, R.V.; Stadlbauer, A.; Kinfe, T.; Bozhkov, Y. Immunometabolic Profiling of Chronic Subdural Hematoma through Untargeted Mass Spectrometry Analysis: Preliminary Findings of a Novel Approach. Diagnostics 2023, 13, 3345. https://doi.org/10.3390/diagnostics13213345
Kipele M, Buchfelder M, Taudte RV, Stadlbauer A, Kinfe T, Bozhkov Y. Immunometabolic Profiling of Chronic Subdural Hematoma through Untargeted Mass Spectrometry Analysis: Preliminary Findings of a Novel Approach. Diagnostics. 2023; 13(21):3345. https://doi.org/10.3390/diagnostics13213345
Chicago/Turabian StyleKipele, Maria, Michael Buchfelder, R. Verena Taudte, Andreas Stadlbauer, Thomas Kinfe, and Yavor Bozhkov. 2023. "Immunometabolic Profiling of Chronic Subdural Hematoma through Untargeted Mass Spectrometry Analysis: Preliminary Findings of a Novel Approach" Diagnostics 13, no. 21: 3345. https://doi.org/10.3390/diagnostics13213345